
Abstract
Colonization of the upper respiratory tract by pneumococcus is important both as a determinant of disease and for transmission into the population. The immunological mechanisms that contain pneumococcus during colonization are well studied in mice but remain unclear in humans. Loss of this control of pneumococcus following infection with influenza virus is associated with secondary bacterial pneumonia. We used a human challenge model with type 6B pneumococcus to show that acquisition of pneumococcus induced early degranulation of resident neutrophils and recruitment of monocytes to the nose. Monocyte function was associated with the clearance of pneumococcus. Prior nasal infection with live attenuated influenza virus induced inflammation, impaired innate immune function and altered genome-wide nasal gene responses to the carriage of pneumococcus. Levels of the cytokine CXCL10, promoted by viral infection, at the time pneumococcus was encountered were positively associated with bacterial load.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$32.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout








Similar content being viewed by others


Data availability
Raw RNA sequencing data have been deposited in the Gene Expression Omnibus repository, accession number GSE117580. All other underlying data are provided in the manuscript.
References
Liu, L. et al. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet 388, 3027–3035 (2016).
Morens, D. M., Taubenberger, J. K. & Fauci, A. S. Predominant role of bacterial pneumonia as a cause of death in pandemic influenza: implications for pandemic influenza preparedness. J. Infect. Dis. 198, 962–970 (2008).
Goldblatt, D. et al. Antibody responses to nasopharyngeal carriage of Streptococcus pneumoniae in adults: a longitudinal household study. J. Infect. Dis. 192, 387–393 (2005).
Simell, B. et al. The fundamental link between pneumococcal carriage and disease. Expert Rev. Vaccines 11, 841–855 (2012).
Melegaro, A., Gay, N. J. & Medley, G. F. Estimating the transmission parameters of pneumococcal carriage in households. Epidemiol. Infect. 132, 433–441 (2004).
Ferreira, D. M. et al. Controlled human infection and rechallenge with Streptococcus pneumoniae reveals the protective efficacy of carriage in healthy adults. Am. J. Respir. Crit. Care Med. 187, 855–864 (2013).
McCool, T. L., Cate, T. R., Moy, G. & Weiser, J. N. The immune response to pneumococcal proteins during experimental human carriage. J. Exp. Med. 195, 359–365 (2002).
Mina, M. J. & Klugman, K. P. The role of influenza in the severity and transmission of respiratory bacterial disease. Lancet Respir. Med. 2, 750–763 (2014).
Alpkvist, H. et al. Clinical and microbiological factors associated with high nasopharyngeal pneumococcal density in patients with pneumococcal pneumonia. PLoS ONE 10, e0140112 (2015).
Wolter, N. et al. High nasopharyngeal pneumococcal density, increased by viral coinfection, is associated with invasive pneumococcal pneumonia. J. Infect. Dis. 210, 1649–1657 (2014).
Albrich, W. C. et al. Pneumococcal colonisation density: a new marker for disease severity in HIV-infected adults with pneumonia. BMJ Open 4, e005953 (2014).
Thors, V. et al. The effects of live attenuated influenza vaccine on nasopharyngeal bacteria in healthy 2 to 4 year olds. A randomized controlled trial. Am. J. Respir. Crit. Care Med. 193, 1401–1409 (2016).
Mina, M. J., McCullers, J. A. & Klugman, K. P. Live attenuated influenza vaccine enhances colonization of Streptococcus pneumoniae and Staphylococcus aureus in mice. mBio 5, e01040-13 (2014).
Rylance, J. et al. Effect of live attenuated influenza vaccine on pneumococcal carriage. bioRxiv https://doi.org/10.1101/343319 (2018).
Lu, Y. J. et al. Interleukin-17A mediates acquired immunity to pneumococcal colonization. PLoS Pathog. 4, e1000159 (2008).
Zhang, Z., Clarke, T. B. & Weiser, J. N. Cellular effectors mediating Th17-dependent clearance of pneumococcal colonization in mice. J. Clin. Investig. 119, 1899–1909 (2009).
Lu, Y. J. et al. GMP-grade pneumococcal whole-cell vaccine injected subcutaneously protects mice from nasopharyngeal colonization and fatal aspiration-sepsis. Vaccine 28, 7468–7475 (2010).
Nakamura, S., Davis, K. M. & Weiser, J. N. Synergistic stimulation of type I interferons during influenza virus coinfection promotes Streptococcus pneumoniae colonization in mice. J. Clin. Investig. 121, 3657–3665 (2011).
Sun, K. & Metzger, D. W. Inhibition of pulmonary antibacterial defense by interferon-γ during recovery from influenza infection. Nat. Med 14, 558–564 (2008).
Li, W., Moltedo, B. & Moran, T. M. Type I interferon induction during influenza virus infection increases susceptibility to secondary Streptococcus pneumoniae infection by negative regulation of γδ T cells. J. Virol. 86, 12304–12312 (2012).
Jochems, S. P., Weiser, J. N., Malley, R. & Ferreira, D. M. The immunological mechanisms that control pneumococcal carriage. PLoS Pathog. 13, e1006665 (2017).
Querec, T. D. et al. Systems biology approach predicts immunogenicity of the yellow fever vaccine in humans. Nat. Immunol. 10, 116–125 (2009).
Oh, J. Z. et al. TLR5-mediated sensing of gut microbiota is necessary for antibody responses to seasonal influenza vaccination. Immunity 41, 478–492 (2014).
Li, S. et al. Metabolic phenotypes of response to vaccination in humans. Cell 169, 862–877 (2017).
Kazmin, D. et al. Systems analysis of protective immune responses to RTS,S malaria vaccination in humans. Proc. Natl Acad. Sci. USA 114, 2425–2430 (2017).
Nakaya, H. I. et al. Systems biology of vaccination for seasonal influenza in humans. Nat. Immunol. 12, 786–795 (2011).
Nakaya, H. I. et al. Systems analysis of immunity to influenza vaccination across multiple years and in diverse populations reveals shared molecular signatures. Immunity 43, 1186–1198 (2015).
Li, S. et al. Molecular signatures of antibody responses derived from a systems biology study of five human vaccines. Nat. Immunol. 15, 195–204 (2014).
Glennie, S. et al. Modulation of nasopharyngeal innate defenses by viral coinfection predisposes individuals to experimental pneumococcal carriage. Mucosal Immunol 9, 56–67 (2015).
Karppinen, S. et al. Acquisition and transmission of Streptococcus pneumoniae are facilitated during rhinovirus infection in families with children. Am. J. Respir. Crit. Care Med. 196, 1172–1180 (2017).
Segal, A. W. How neutrophils kill microbes. Annu. Rev. Immunol. 23, 197–223 (2005).
Craft, A. W., Reid, M. M. & Low, W. T. Effect of virus infections on polymorph function in children. Br. Med. J. 1, 1570 (1976).
Yuasa, T., Ohno, S., Kehrl, J. H. & Kyriakis, J. M. Tumor necrosis factor signaling to stress-activated protein kinase (SAPK)/Jun NH2-terminal kinase (JNK) and p38. Germinal center kinase couples TRAF2 to mitogen-activated protein kinase/ERK kinase kinase 1 and SAPK while receptor interacting protein associates with a mitogen-activated protein kinase kinase kinase upstream of MKK6 and p38. J. Biol. Chem. 273, 22681–22692 (1998).
Anderson, A. C., Joller, N. & Kuchroo, V. K. Lag-3, Tim-3, and TIGIT: co-inhibitory receptors with specialized functions in immune regulation. Immunity 44, 989–1004 (2016).
Wu, W. et al. RIG-I and TLR3 are both required for maximum interferon induction by influenza virus in human lung alveolar epithelial cells. Virology 482, 181–188 (2015).
Malley, R. et al. Recognition of pneumolysin by Toll-like receptor 4 confers resistance to pneumococcal infection. Proc. Natl Acad. Sci. USA 100, 1966–1971 (2003).
Paixao, L. et al. Host glycan sugar-specific pathways in Streptococcus pneumonia: galactose as a key sugar in colonisation and infection. PLoS ONE 10, e0121042 (2015). correction 10, e0127483 (2015).
Siegel, S. J., Roche, A. M. & Weiser, J. N. Influenza promotes pneumococcal growth during coinfection by providing host sialylated substrates as a nutrient source. Cell Host Microbe 16, 55–67 (2014).
Russo, P. S. T. et al. CEMiTool: a Bioconductor package for performing comprehensive modular co-expression analyses. BMC Bioinformatics 19, 56 (2018).
Kwissa, M. et al. Dengue virus infection induces expansion of a CD14+CD16+ monocyte population that stimulates plasmablast differentiation. Cell Host Microbe 16, 115–127 (2014).
Parker, D. et al. Streptococcus pneumoniae DNA initiates type I interferon signaling in the respiratory tract. mBio 2, e00016-00011 (2011).
Gerszten, R. E. et al. MCP-1 and IL-8 trigger firm adhesion of monocytes to vascular endothelium under flow conditions. Nature 398, 718–723 (1999).
Weiser, J. N. The pneumococcus: why a commensal misbehaves. J. Mol. Med. 88, 97–102 (2010).
Rynda-Apple, A., Robinson, K. M. & Alcorn, J. F. Influenza and bacterial superinfection: illuminating the immunologic mechanisms of disease. Infect. Immun. 83, 3764–3770 (2015).
Cox, M. A., Nechanitzky, R. & Mak, T. W. Check point inhibitors as therapies for infectious diseases. Curr. Opin. Immunol. 48, 61–67 (2017).
Hoffmann, J. et al. Viral and bacterial co-infection in severe pneumonia triggers innate immune responses and specifically enhances IP-10: a translational study. Sci. Rep. 6, 38532 (2016).
Seyoum, B., Yano, M. & Pirofski, L. A. The innate immune response to Streptococcus pneumoniae in the lung depends on serotype and host response. Vaccine 29, 8002–8011 (2011).
Luo, H., Wang, D., Che, H. L., Zhao, Y. & Jin, H. Pathological observations of lung inflammation after administration of IP-10 in influenza virus- and respiratory syncytial virus-infected mice. Exp. Ther. Med. 3, 76–79 (2012).
Hogberg, L. et al. Age- and serogroup-related differences in observed durations of nasopharyngeal carriage of penicillin-resistant pneumococci. J. Clin. Microbiol. 45, 948–952 (2007).
Madhi, S. A., Klugman, K. P. & Vaccine Trialist Group. A role for Streptococcus pneumoniae in virus-associated pneumonia. Nat. Med. 10, 811–813 (2004).
Gritzfeld, J. F. et al. Experimental human pneumococcal carriage. J. Vis. Exp. 72, e50115 (2013).
Jochems, S. P. et al. Novel analysis of immune cells from nasal microbiopsy demonstrates reliable, reproducible data for immune populations, and superior cytokine detection compared to nasal wash. PLoS ONE 12, e0169805 (2017).
Gritzfeld, J. F. et al. Density and duration of experimental human pneumococcal carriage. Clin. Microbiol. Infect. 20, O1145–O1151 (2014).
Morton, B. et al. Augmented passive immunotherapy with P4 peptide improves phagocyte activity in severe sepsis. Shock 46, 635–641 (2016).
Dobin, A. et al. STAR: ultrafast universal RNA-seq aligner. Bioinformatics 29, 15–21 (2013).
Liao, Y., Smyth, G. K. & Shi, W. featureCounts: an efficient general purpose program for assigning sequence reads to genomic features. Bioinformatics 30, 923–930 (2014).
Yates, A. et al. Ensembl 2016. Nucleic Acids Res. 44, D710–D716 (2016).
Love, M. I., Huber, W. & Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 15, 550 (2014).
Acknowledgements
S.B.G. and D.M.F. are supported by the Medical Research Council (grant MR/M011569/1), the Bill and Melinda Gates Foundation (grant OPP1117728) and the National Institute for Health Research Local Comprehensive Research Network. Flow cytometric acquisition was performed on a BD LSR II funded by a Wellcome Trust Multi-User Equipment Grant (104936/Z/14/Z). S.P.J. received support from the Royal Society of Tropical Medicine and Hygiene for NanoString analysis. H.I.N. is supported by the São Paulo Research Foundation (FAPESP; grants 2013/08216-2 and 2012/19278-6). We thank all volunteers for participating in this study, and R. Robinson, C. Lowe, L. Lazarova, K. Piddock and I. Wheeler for clinical support. We also acknowledge M. Mina for his input in study design.
Author information
Authors and Affiliations
Contributions
S.P.J. contributed to conceiving, designing, performing and analyzing experiments and writing the paper. F.M. and H.I.N. contributed to analyzing experiments and writing the paper. B.F.C., M.H., E.M., E.S., J.F.G., C.S., J.Reiné, S.P., E.N., E.L.G., W.A.A.d.S.P. and D.B. contributed to conducting and analyzing experiments. A.H.-W., H.H., C.H., H.A., S.Z., V.C., J.Rylance and S.B.G. contributed to sample collection and/or designing the study. D.M.F. contributed to conceiving, designing and analyzing experiments, designing the study and writing the paper. All authors have read and approved the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Integrated supplementary information
Supplementary Figure 1 Pneumococcal load in the LAIV and control cohorts.
Mean and standard error of log-transformed carriage load (colony-forming units (CFU)/mL nasal wash) for carriage+ volunteers (defined by detection of S. pneumoniae at any timepoint) are shown for the control carriage+ group (green, n = 24 subjects) and LAIV carriage+ group (orange, n = 25). Load for samples with undetectable pneumococcal load was set at 0.1 CFU/mL nasal wash.
Supplementary Figure 2 CXCL10 concentrations are increased by virus infection.
(a), Concentrations of CXCL10 at day 0 in the LAIV cohort, measured by Luminex in nasosorption (n = 77). (b), Concentrations of CXCL10 at day 5 to S. pneumoniae inoculation in a cohort with known viral URT state measured by ELISA (n = 82). Oropharyngeal swabs collected 5 d before S. pneumoniae inoculation were assessed for a viral multiplex PCR panel for detection of influenza A and B (n = 0), respiratory syncytial virus (n = 2), human metapneumovirus (n = 0), human rhinovirus (n = 12), parainfluenza viruses 1–4 (n = 1), and coronaviruses OC43, NL63, 229E, and HKU1 (n = 5). Individual volunteers are shown and box plots depict median and interquartile ranges, with whiskers extending to 1.5 × interquartile range or maximum value, per group. *P = 0.017, **P = 6.2 × 10–5 by two-tailed Mann–Whitney test.
Supplementary Figure 3 Nasal granulocyte numbers over time and baseline immune cell composition.
(a), Numbers of granulocytes, predominantly neutrophils based on CD16 expression, at the nasal mucosa. Median and interquartile range are shown for cell numbers normalized to numbers of epithelial cells for control carriage+ (n = 24), control carriage– (n = 37), LAIV carriage+ (n = 25) and LAIV carriage– (n = 30) groups. The x axis shows days relative to inoculation. (b), Absolute numbers of cells observed per nasal sample (median and IQR are shown for 117 subjects at baseline).
Supplementary Figure 4 Flow cytometry gating strategy and longitudinal levels of nasal T cells and monocytes.
(a), Gating strategy of nasal cells for one representative volunteer. (b), Numbers of T cells at the nasal mucosa. Median and interquartile range are shown for cell numbers normalized to numbers of epithelial cells for control carriage+ (n = 24), control carriage– (n = 37), LAIV carriage+ (n = 25) and LAIV carriage– (n = 30) groups. The x axis shows days relative to inoculation. (c), Median and interquartile range of monocyte numbers in the control group over time with carriage detected by classical microbiology (carriage+, n = 24), molecular methods only (lytA+, n = 16) or not at all (carriage–, n = 22). *P = 0.038 at day 2 and P = 0.030 at day 29, **P = 0.002 by two-tailed Wilcoxon paired non-parametric test.
Supplementary Figure 5 Monocyte recruitment associates with CCL2 concentration and is reproducible in an independent volunteer cohort.
(a), Spearman’s correlation between the 30 measured cytokines and nasal monocyte numbers for each timepoint (n = 73). The length of the bar depicts the rho value, cyan bars represent cytokines that correlate significantly at all days, red bars associate for a specific day, and transparent red bars are not significantly associated for that day. (b), Monocyte numbers over time in those volunteers who most upregulate CCL2, IFN-γ, IL-6 or TNF at day 2 (top quartile FC induction, n = 17 versus below top quartile, n = 56) or not. *P = 0.028 by two-tailed Mann–Whitney test of monocyte number area under curve of inducers and non-inducers. (c), Numbers of monocytes and CCL2 in a second, independent cohort of seven carriers without any vaccination. Symbols represent individual subjects, with color corresponding to day relative to S. pneumoniae inoculation. The effects of CCL2 on monocyte numbers by generalized linear regression analysis are shown, correcting for repeated individual measurements.
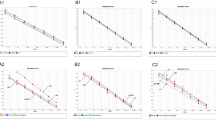
Supplementary Figure 6 Nasal cell responses to in vitro stimulation with pneumococcus.
Whole nasal cells were collected 29 d after S. pneumoniae inoculation and stimulated for 18 h with heat-killed pneumococcus (n = 48). Supernatant was collected and the concentrations of 30 cytokines were measured by Luminex. Four cytokines were not measured above the limit of detection (IL-2, IL-4, MIG and eotaxin), and these were excluded from analysis. (a), Responses for all measured cytokines for the four groups are shown. (b), Production in carriage– volunteers subdivided into those who had very low carriage loads, detectable only by molecular methods (lytA+, n = 9), or not at all (carriage–, n = 5). The dotted line indicates a twofold increase over the unstimulated control. The median and interquartile range of FC to unstimulated are shown An asterisk indicates significantly induced cytokines (shown in red) (FC > 2, q < 0.05, two-tailed paired Wilcoxon test followed by Benjamini–Hochberg correction).
Supplementary Figure 7 Immune mechanisms associating with control of S. pneumoniae carriage and their disruption by LAIV.
Carriage in the absence of influenza leads to quick degranulation of nasal neutrophils followed by recruitment of monocytes to the nose, associating with the start of clearance. Influenza infection leads to inflammation, impairing this innate control of carriage.
Supplementary information
Supplementary Text and Figures (download PDF )
Supplementary Figures 1–7 and Supplementary Tables 2 and 3
Supplementary Data 1
CEMiTool report of control group
Supplementary Data 2
CEMiTool report of LAIV group
Supplementary Table 1 (download XLSX )
Cytokine induction following LAIV or control vaccination
Supplementary Table 4 (download XLSX )
List of differentially expressed genes
Supplementary Table 5 (download XLSX )
List of pathways
Rights and permissions
About this article

Cite this article
Jochems, S.P., Marcon, F., Carniel, B.F. et al. Inflammation induced by influenza virus impairs human innate immune control of pneumococcus. Nat Immunol 19, 1299–1308 (2018). https://doi.org/10.1038/s41590-018-0231-y
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41590-018-0231-y
This article is cited by
-
Persistent pneumococcal colonisation in antiretroviral-treated HIV infection is associated with nasal inflammation
Nature Communications (2025)
-
Safety and efficacy of an intramuscular bivalent vaccine against influenza and Streptococcus pneumoniae infections in mice
Medical Microbiology and Immunology (2025)
-
Exploring the immune-inflammatory mechanism of Maxing Shigan Decoction in treating influenza virus A-induced pneumonia based on an integrated strategy of single-cell transcriptomics and systems biology
European Journal of Medical Research (2024)
-
NEDD4 Regulated Pyroptosis Occurred from Co-infection between Influenza A Virus and Streptococcus pneumoniae
Journal of Microbiology (2023)
-
A novel Streptococcus pneumoniae human challenge model demonstrates Treg lymphocyte recruitment to the infection site
Scientific Reports (2022)
