
Abstract
Obesity is a major public health challenge. Glucagon-like peptide-1 receptor agonists (GLP1-RA) and bariatric surgery (BS) are effective weight loss interventions; however, the genetic factors influencing treatment response remain largely unexplored. Moreover, most previous studies have focused on race and ethnicity rather than genetic ancestry. Here we analyzed 10,960 individuals from 9 multiancestry biobank studies across 6 countries to assess the impact of known genetic factors on weight loss. Between 6 and 12 months, GLP1-RA users had an average weight change of −3.93% or −6.00%, depending on the outcome definition, with modest ancestry-based differences. BS patients experienced −21.17% weight change between 6 and 48 months. We found no significant associations between GLP1-RA-induced weight loss and polygenic scores for body mass index or type 2 diabetes, nor with missense variants in GLP1R. A higher body mass index polygenic score was modestly linked to lower weight loss after BS (+0.7% per s.d., P = 1.24 × 10−4), but the effect attenuated in sensitivity analyses. Our findings suggest known genetic factors have limited impact on GLP1-RA effectiveness with respect to weight change and confirm treatment efficacy across ancestry groups.
Similar content being viewed by others
Main
The obesity epidemic presents a substantial public health burden, with 75% of adults with obesity attempting weight loss but few achieving lasting success1,2,3. Amid these challenges, GLP1-RA have emerged as a promising solution. Discovered in the 1980s, glucagon-like peptide-1 (GLP1) is linked to the incretin effect, promoting insulin release from pancreatic β cells, thus regulating blood sugar levels4. This led to approval of the first GLP1-RA for treatment of type 2 diabetes (T2D) in 2005, followed by approval for obesity treatment in 2014 after its association with reduced food intake was established5.
Clinical trials demonstrated weight loss effects of 6–16% with liraglutide and semaglutide, driving a global rise in GLP1-RA use6,7,8. Additional trials have revealed cardiovascular9,10 and renal benefits11, with ongoing trials underway12. By 2030, an estimated 30 million people in the United States (~9% of the population) are expected to use GLP1-RA drugs, highlighting their role in addressing obesity and expanding therapeutic applications13,14.
Meanwhile, BS remains a durable and effective treatment for individuals with severe obesity and metabolic comorbidities (body mass index (BMI) ≥ 35 kg m−2)15,16. Meta-analyses of randomized controlled trials and observational studies report an average weight loss of 26 kg, with one trial showing 25% total weight loss after 5 years for sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB)17,18. Although BS carries risks such as nutrient malabsorption, large-scale observational studies have demonstrated remarkable long-term benefits, including reduced cardiovascular outcomes, lower all-cause mortality and higher remission rates of T2D, hypertension and hyperlipidemia19,20,21,22.
Despite the robust weight loss effects observed with both GLP1-RA treatment and BS, there exists heterogeneity in their effectiveness. Up to 20% of BS patients may not achieve the desired weight loss in the first year or may regain weight in two years23,24. Variability in GLP1-RA’s glycemic effects has been linked to clinical factors like low β cell function, C-peptide levels and genetic variants25,26,27,28,29. However, aside from T2D, sex and baseline weight, factors driving differences in weight loss responses remain poorly understood30,31,32. In addition, differences in patient adherence may further contribute to this variability33.
Genetics has been considered a potential factor for heterogeneity in weight loss treatments, but its role remains largely unexplored30. A previous study of 57 women found a weak association between a common GLP1R missense variant and GLP1-RA response27,34. Although more well-powered studies have been conducted in BS patients35,36, no consistent genome-wide associations for weight loss have been identified. However, a polygenic score (PGS) for BMI was significantly linked to weight loss after biliopancreatic diversion with duodenal switch in 865 patients37.
Finally, there has been limited exploration into the effectiveness of these obesity treatments across different genetic ancestries and across various healthcare settings6,38.
In our study we seek to: (1) characterize the observed GLP1-RA and BS body weight-lowering effects using real-world data from 10,960 individuals across nine biobanks in six countries, with six major continental ancestry groups; (2) identify whether plausible genetic factors (PGS for BMI and T2D, and coding variants in GLP1R, PCSK1 and APOE genes) associate with heterogeneity in GLP1-RA and BS weight loss effects, and thus identify patient groups that will benefit most from such treatments; (3) compare the effects of GLP1-RA treatment and BS on weight loss across major continental ancestry groups.
Results
GLP1-RA and BS weight loss across ancestries
We investigated changes in body weight associated with GLP1-RA treatment and BS across nine biobank studies: Helsinki University Hospital (HUS, Finland; n = 633), Estonian Biobank (ESTBB; n = 464), UK Biobank (UKBB, United Kingdom; n = 810), All of Us (AoU, United States; n = 559), BioMe Biobank (BioMe, United States; n = 2,170), Mass General Brigham Biobank (MGBB, United States; n = 2,141), Atlas Biobank (UCLA-ATLAS, United States; n = 1,445), Qatar Biobank (QBB, Qatar; n = 2,383) and Bialystok Bariatric Surgery Study (BBSS, Poland, n = 355). We included individuals that were at least 18 years of age when starting a GLP1-RA treatment or undergoing BS. Individuals undergo GLP1-RA treatment for different medical reasons, not only for weight loss. We defined GLP1-RA usage based on prescription or purchase data (ATC codes starting with A10B*; including exenatide, liraglutide, lixisenatide, albiglutide, dulaglutide, semaglutide and beinaglutide) covering at least 12 months, and excluding individuals with indication of treatment discontinuation within this time window. For BS, we considered individuals undergoing the following procedures: RYGB, SG, adjustable gastric band, vertical banded gastroplasty or biliopancreatic diversion with duodenal switch. More information can be found in the Methods.
We included only individuals with an initial body weight measurement recorded in the 12 months before baseline (treatment initiation or surgery) and a follow-up measurement taken 6–12 months after baseline for GLP1-RA or within 48 months for BS. In case of multiple measurements in this time frame, we considered their median (Extended Data Fig. 1). We defined our main outcome of interest as the percentage change in body weight, calculated as the difference between the second body weight measurement (or median of multiple measurements) and the initial one, divided by the initial measurement.
Our study population included a total of 6,750 GLP1-RA users and 4,210 individuals undergoing BS (baseline characteristics are reported in Table 1). Overall, GLP1-RA users: (1) had a lower proportion of women (61.0% weighted average across studies) when compared with BS patients (73.1% weighted average across studies); (2) were on average older (57.30 versus 46.50 years); and (3) had a lower initial body weight (99.80 kg versus 116.96 kg). The proportion of individuals diagnosed with T2D at time of GLP1-RA initiation was ≥48% across all studies and major continental ancestry groups.
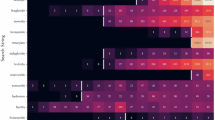
Among GLP1-RA users, we observed an average body weight change (Fig. 1) across studies of −3.93% (ranging from −1.08% to −7.07%), in line with results from observational studies39,40. Among BS patients, we observed an average change of −21.17% (−15.00% to −27.72%).

Bars represent the mean percentage change in body weight in each study and ancestry, and the overall combined weighted mean change. Error bars represent standard errors. Total n for GLP1-RA = 6,750, total n for BA = 4,210, sample size per each cohort or ancestry can be found in Table 1.
Demographic factors linked to GLP1-RA and BS weight change
We explored the effect of baseline characteristics on body weight changes associated with GLP1-RA treatment and BS. We fitted a multivariable linear model with percentage change in body weight as outcome and baseline body weight, sex, age at baseline, the first 20 principal genetic components and medication type (for GLP1-RA users only) as predictors. Each cohort was analyzed separately, stratifying by major continental ancestry group, and the effects were then meta-analyzed (Table 2). Baseline body weight was significantly associated with higher weight loss for both GLP1-RA and BS treatments (βGLP1-RA = −0.05% weight change compared with baseline, P = 1.63 × 10−35; βBS = −0.14% weight change compared with baseline, P = 5.49 × 10−69) and women had a significantly higher weight loss for both treatments (βGLP1-RA = −1.54% weight change compared with baseline, P = 2.47 × 10−16; βBS = −2.66% weight change compared with baseline, P = 6.83 × 10−10). Being older at treatment initiation was only associated with less weight loss for BS (βBS = 0.15% weight change compared with baseline, P = 2.54 × 10−15). The effects of baseline weight and sex on weight loss were highly heterogeneous across ancestries and studies (heterogeneity (I2) for GLP1-RA = 0.99 and 0.83 for baseline weight and sex, respectively) (Extended Data Figs. 2–4 and Supplementary Tables 1 and 2).
Ancestry has marginal impact on GLP1-RA and BS weight loss
We evaluated whether the effect of GLP1-RA- and BS-associated weight loss was significantly different across genetically defined continental ancestry groups after accounting for differences in weight at baseline, age, sex and, for GLP1-RA only, medication type (Table 3). Only multiancestry biobanks (AoU, BioMe, MGBB, UCLA-ATLAS) were included in this analysis (n = 6,315). Compared with individuals of European ancestry, all other ancestry groups had a lower change in body weight. However, this effect was statistically significant only among GLP1-RA users of African (β = 0.76% weight change from baseline weight, P = 0.02) and admixed American (β = 0.87% weight change from baseline weight, P = 3 × 10−3) ancestries.
Plausible genetic factors show no link to GLP1-RA weight loss
We investigated the effect of genetic exposures with plausible effects on body weight changes. Genetic exposures were selected upon discussion between authors and before initiating analyses. First, we considered PGS for BMI based on previous observation that a PGS was associated with BMI trajectories41,42. We also consider the only replicated genome-wide variant associated with BMI change in the largest study of BMI trajectories (rs429358 in APOE)41. Second, we considered a PGS for T2D based on the observation that biomarkers of T2D were associated with effectiveness of GLP1-RA26,43. We confirmed that both PGS for BMI and T2D were significantly associated with their respective traits across all major continental ancestry groups (Supplementary Table 3) although the effects were larger in individuals of European ancestry.
Third, we considered 13 single nucleotide polymorphisms (SNPs) in the GLP1R and PCSK1 genes. We considered all missense variants in the GLP1R gene with at least 1% minor allele frequency (MAF) in at least one of major continental ancestry group, as per gnomAD (v.4.1)44, three of which have been functionally characterized as gain or loss of function (Supplementary Table 4)45. We also considered two nonsynonymous variants in the PCSK1 gene that have been associated with BMI variation in the population46. Finally, we sought to replicate the effect of two variants associated with weight loss in one of the largest studies of BS36 (Methods). After analyses, two missense variants in the GLP1R genes rs2295006 and rs201672448 were too rare to be tested across studies and were not considered further.
We estimated the effect of each genetic exposure on weight change in each cohort and major continental ancestry groups separately, fitting a linear model adjusted for baseline body weight, sex, age at baseline, first 20 principal genetic components and medication type (for GLP1-RA users only), and we subsequently combined the effects through ancestry-specific and multiancestry meta-analyses (Fig. 2 and Supplementary Tables 5 and 6). We did not adjust for T2D diagnosis because we considered it a potential mediator between the genetic exposure and weight change outcome.

a, Ancestry-specific and multiancestry meta-analysis effect sizes for the association between percentage change in body weight and PGS for BMI and T2D. Dots represent the estimated percentage change in body weight per 1 s.d. change in PGS, error bars represent the 95% confidence interval (CI) for the estimate. b, Multiancestry meta-analysis effect sizes for the association between percentage change in body weight and genotype at each locus. Dots represent the estimated percentage change in body weight, error bars represent the 95% CI for the estimate. For a and b, coefficients are estimated from a linear regression model, separately for each genetic exposure. Full dots represent statistical significance at P < 0.004 (Bonferroni adjusted for 14 independent tests). P values are two-sided and were calculated by dividing the coefficient values by their standard errors and observing the probability mass corresponding to equal or more extreme values from both tails of Student’s t distribution. Exact P values can be found in Supplementary Tables 5 and 6. Total sample size is 6,750 for GLP1-RA and 4,210 for BS. Sample size per ancestry can be found in Table 1.
Among GLP1-RA users, we did not observe any significant genetic exposure associated with weight loss after multiple-testing correction (P < 0.004, Bonferroni correction for 13 exposures tested).
We further tested whether the lack of associations observed was possibly due to high effect-size heterogeneity across ancestries, or to a lack of statistical power. We did not observe any significant heterogeneity across ancestries for any of the genetic exposure (average I2 across genetic exposures for GLP1-RA was 0.06) (Supplementary Table 7). Moreover, given the current sample size for GLP1-RA users (n = 6,750) our power calculation showed we would have at least 80% power to detect a statistically significant effect (at P < 0.05) of at least a 0.3% change in body weight for 1 s.d. change in the PGS, or for SNPs with an MAF of at least 1% (Methods).
A higher BMI PGS associates with lower weight loss due to BS
Among BS patients, a higher PGS for BMI was significantly associated with lower weight loss (βBMI PGS = 0.70% weight change compared with baseline for 1 s.d. change in the PGS, P = 1.24 × 10−4) after multiple-testing correction (P < 0.01, Bonferroni correction for five exposures tested), in the opposite direction than observed for weight at baseline (Fig. 2 and Table 2). A higher PGS for T2D was nominally associated with lower weight loss (βT2D PGS = 0.45% weight change compared with baseline for 1 s.d. change in the PGS, P = 0.03).
We observed significant heterogeneity in the association between BMI PGS and weight loss across studies (I2 = 0.64) (Supplementary Table 8).
Sensitivity analyses
To assess the robustness of our findings, we conducted a series of sensitivity analyses (Supplementary Methods and Supplementary Results).
First, we consider different outcome definitions. We shortened the follow-up period for BS to 12 months to make it comparable with that of GLP1-RA. We considered only participants with weight measurements available at least 30 days before BS to account for the possibility of substantial weight loss due to preoperative low-calorie diets. We used minimum rather than median weight during the follow-up period to assess the impact of a different definition of weight loss. This latter definition resulted in significant higher weight loss for GLP1-RA (−6.00% compared with −3.93% when using the median) (Supplementary Tables 9 and 10 and Supplementary Figs. 1 and 2). All analyses confirmed the associations observed in the primary analysis (Supplementary Tables 11–21 and Supplementary Figs. 1–12), although the effect of BMI PGS on weight loss due to BS was slightly reduced when considering a shortened follow-up period (0.43% per 1 s.d. change in the PGS, P = 0.03 compared with 0.70% in the primary model) (Supplementary Table 11 and Supplementary Figs. 3 and 4).
Second, we considered different covariate adjustment and performed subgroup analyses. To evaluate whether a T2D diagnosis independently affects weight loss, we adjusted the analyses for T2D status and observed similar results to the primary analyses (for BMI PGS in BS, the only statistically significant result, 0.59% per 1 s.d. change, P = 6.6 × 10−4 compared with 0.70% in the primary model) (Supplementary Tables 12 and 13 and Supplementary Fig. 5). We considered only semaglutide and liraglutide as GLP1-RA treatments to capture their specific use for weight loss. Although we observed a higher weight loss than considering all GLP1-RA treatments (−4.69% versus −3.93%) (Supplementary Fig. 6), we confirmed the lack of effect of BMI and T2D PGS on weight loss observed in primary analyses (Supplementary Table 14 and Supplementary Fig. 7). We stratified the BS analysis by the two major surgery procedures, RYGB and SG, allowing us to assess whether the observed effects varied by surgery type. Although both procedures showed similar weight loss effects (−22.30% and −22.10%, for RYGB and SG respectively) (Supplementary Figs. 10 and 11), we observed a significant effect of BMI PGS on weight change only for RYGB (0.83% weight change compared with baseline per 1 s.d. change in the PGS, P = 1.49 × 10−4 ((Supplementary Tables 16 and 17).
Third, we considered different statistical models. Previous works have argued that using percentage changes in weight loss pre versus post therapy is statistically inappropriate and inefficient47,48,49. Thus, we considered a model using post-treatment weight as outcome, including the same predictors as in the main model and an additional term modeling the interaction between baseline weight and each genetic exposure. We observed similar results as in the primary model (Supplementary Tables 18 and 19). A second potential issue with the primary model relates to adjusting longitudinal change phenotypes for the baseline trait50,51. In particular, when testing for the effect of genetic exposure on drug response outcomes, adjusting phenotype changes (for example, weight loss) for baseline levels (for example, weight at treatment initiation) can result in a false-positive association when genetic variants are also associated with baseline levels52. Removing baseline weight from the model led to a reduction in the effect of the BMI PGS on weight loss due to BS (0.15% per 1 s.d. change in the PGS, P = 0.420, compared with 0.70% in the primary model) (Supplementary Tables 20 and 21 and Supplementary Fig. 12).
Discussion
In this study, we provide a comprehensive assessment of major demographic factors and plausible genetic factors on body weight changes associated with GLP1-RA use and BS. In line with previous work30,53,54,55,56, our main outcome of interest was the percentage change in body weight between 6 and 12 months after GLP1-RA treatment initiation as well as between 6 and 48 months after BS.
By considering studies from six different countries, we were able to highlight heterogeneity in the use of GLP1-RA across different healthcare systems. GLP1-RA users consisted mostly of individuals with T2D, reflecting their original use for treatment of this condition. Biobank studies covering Boston (MGBB), New York (BioMe), Los Angeles (UCLA-ATLAS) and Helsinki (HUS) had overall lower rates of T2D individuals compared with the other studies and lower weights at baseline, which, together with the availability of more updated electronic health records (EHR) data, suggest a larger number of individuals being prescribed GLP1-RA for weight loss. However, care should be taken in interpreting variation in the rate of T2D across biobanks because this might reflect different approaches used for capturing this diagnosis from the EHR as well as the different sampling strategies of biobanks.
The comparison between GLP1-RA and BS is informative because it highlights the younger age, higher weight and lower percentage of men undergoing BS compared with GLP1-RA users. The weight reduction was also approximately five times higher among BS patients compared with GLP1-RA users. The weight reduction among GLP1-RA users was also more heterogeneous across biobanks compared with BS, but in line with that reported previously in the literature using real-world data28 and lower than results from clinical trials7,57. The lower weight reduction observed among GLP1-RA users is partially influenced by use of the median postoperative or post-drug therapy weight, although we observed greater weight reduction when using minimum weight. However, our approach provides a more conservative and robust estimate, better accounting for the variability and potential uncertainty in clinical measurement data. Our findings also highlight a consistent effect of baseline body weight and sex on weight loss associated with both GLP1-RA treatment and BS, suggesting that individuals with higher weight at baseline, as well as women benefit more from both interventions. These findings underscore the importance of considering individual characteristics when designing weight loss interventions.
The main aim of this study was to evaluate the impact of genetic exposures on body weight changes induced by GLP1-RA or BS. At the current sample size, a genome-wide scan would have limited power to identify potential new signals. With 6,750 individuals, we would have at least 80% statistical power to identify, at a genome-wide significant threshold, a genetic variant with an allele frequency of ≥1% and an effect >0.3% weight change per s.d., being unlikely given previous effects of common variants on treatment response52. Instead, we tested hypotheses based on the largest genome-wide association studies of BMI and T2D and examined biologically plausible mutations in candidate genes. PGS represent the most powerful genetic predictors for BMI and T2D and we confirm their significant association with the corresponding trait across all major continental ancestry groups. Thus, lack of associations with these PGS would suggest that these interventions act independently of genetic predisposition to BMI or T2D, as explained by common genetic variants. Moreover, because the biological underpinning of weight change is partially distinct from weight at baseline, we also consider the few replicated genetic signals for BMI variability and BMI trajectories.
For BS, genetically higher BMI was associated with weight gain, opposite to the phenotypic association with initial body weight. This suggests that individuals with a stronger genetic predisposition to obesity may regain weight faster post surgery. Maintaining weight loss may require additional lifestyle modifications, behavioral therapy or adjunct pharmacologic treatments like GLP1-RA58,59.
By contrast, none of the genetic exposures were associated with weight loss among GLP1-RA users, after multiple-testing correction. These results were not attributable to high heterogeneity across studies or across major continental ancestry groups. Whether we directly tested the impact of genetic exposure on percentage body weight change or used post-treatment weight as outcome and tested the interaction between baseline weight and the genetic exposure, the results did not significantly change.
In addition, we conducted extensive sensitivity analyses to further examine the effect of BMI and T2D PGS on weight loss after BS and GLP1-RA treatment. These analyses included alternative definitions of weight outcomes, a shorter follow-up period and stricter inclusion criteria for BS, adjustments for T2D status, subgroup analysis for GLP1-RA medication and BS patients, and testing different statistical models. Across all these analyses, we did not observe a significant effect of BMI or T2D PGS on weight reduction following GLP1-RA treatment, in concordance with our primary analysis. Regarding the impact of BMI PGS on weight loss due to BS, we observed a reduction of effect in some of the sensitivity analyses, in particular when excluding baseline weight adjustment from the model. In this case, the directionality of the effect remained consistent; however, the association was no longer statistically significant. Further, no significant genetic effect was observed for SG. Notably, the QBB cohort contained only 23 individuals who underwent SG, resulting in a sample size too small to calculate standard errors for the estimates in the model. Consequently, the QBB cohort, and by extension, the Middle Eastern ancestry group, did not contribute to the SG subanalysis. The lack of separation between techniques and studies makes it difficult to discern whether the observed effects stem from surgical procedures, cohort characteristics or ancestry-related factors. Overall, our results showed that the considered genetic influence on weight loss in response to GLP1-RA treatment and BS may be too small to impact clinical decision-making or patient outcomes. Future studies should explore more powerful PGS or focus on individuals using GLP1-RA solely for weight loss.
Another aim was to compare GLP1-RA- and BS-associated weight loss across major continental ancestry groups. Ancestry can provide more useful information about population health than racial and ethnic categories because it is not directly influenced by geographic, cultural and sociopolitical forces60. Nonetheless, ancestry is also partially correlated with self-reported race and ethnicity and socioeconomic characteristics do differ across racial and ethnic groups. Overall, we found no large differences in GLP1-RA- and BS-associated weight loss between major continental ancestry groups. However, GLP1-RA users of African and admixed American ancestry showed significantly lower weight change than Europeans, after adjusting for sex, age, baseline weight and medication type. The effects were consistent in BioMe and UCLA-ATLAS for admixed American ancestry, and in AoU and MGBB for African ancestry. These differences may reflect socioeconomic factors, such as disparities in treatment access.
The main strength of our study is its size and diversity across countries, healthcare systems and ancestries. Yet, our study presents various limitations. First, we cannot be sure that all GLP1-RA users fulfilled their prescription, although this affects studies with prescription data more than those with purchase data. Nonetheless, weight loss was comparable across both study types. Moreover, to ensure weight changes reflected treatment effects, we included only measurements within one month of the last purchase or prescription. Second, we could not accurately estimate treatment adherence, but overcome this limitation by considering treatments of maximum 12 months’ duration, a period for which adherence has been observed to be around 65% (ref. 53). Third, we used ancestry labels based on major continental ancestry groups, while ancestry can be better characterized as a continuous quantity60. This discretization reflects pragmatic considerations to enable comparable analyses across the different studies. Fourth, the absence of a control group in the GLP1-RA analysis may limit distinguishing intentional from unintentional weight loss. However, large-scale real-world data and consistent sensitivity analysis support the robustness of our results. Fifth, although T2D medications like metformin can affect weight loss, our T2D-adjusted sensitivity analyses likely accounted for first-line treatments. Finally, we did not assess GLP1-RA dosing effects, because dose adjustments vary over time, higher doses do not consistently correlate with greater weight loss and inconsistent reporting across studies could introduce biases.
In conclusion, our study suggests that GLP1-RA treatments work equally well in individuals carrying common nonsynonymous mutations in the GLP1R gene and in individuals at high genetic risk for BMI and T2D. Although BS is slightly less effective in individuals with a higher BMI PGS, the effect (~0.7% lower weight loss per s.d. increase) may be not clinically substantial. Both interventions achieved sustained weight loss across ancestry groups, although socioeconomic factors linked to ancestry should be further studied to understand remaining differences.
Methods
Ethics statement
This study complies with all relevant ethical regulations and was conducted in accordance with the research permits and approvals granted by the respective institutions.
The INTERVENE Helsinki Biobank project was approved by the Helsinki University Central Hospital Ethics Board (HUS/230/2022 §69). The application meets the requirements for biobank research as defined by the Biobank Act (688/2012). The Bialystok Bariatric Surgery Study was approved by the Ethics Committee of the Medical University of Bialystok (approval number R-I-002/546/2015). This study was approved by the Institutional Review Board of the Icahn School of Medicine at Mount Sinai (23-00583). The Estonian Biobank (ESTBB) operates under the Human Genes Research Act, which has regulated its activities since 2000. Individual-level data analyses in ESTBB were conducted under ethical approvals 1.1-12/1409 and 1.1-12/2161 from the Estonian Committee on Bioethics and Human Research (Estonian Ministry of Social Affairs), using data according to release application 6-7/GI/18857 and 3-10/GI/11571 from the Estonian Biobank. The analysis in the Mass General Brigham Biobank (MGBB) was approved by the Mass General Brigham Institutional Review Board under protocol number 2018P001236. In Qatar Biobank all participants provided written informed consent for the biobank study and this study was approved by the Biobank Institutional Review Board number E-2024-QF-QBB-RES-QCC-00205-0280. UK Biobank data used in this study were obtained under approved application 78537.
For all other biobanks included in this study, additional ethical approval was not required as per their respective governance policies for secondary research using de-identified biobank data.
Study population
In the current study, we included samples from 10,960 individuals from the following nine biobanks: HUS (Finland; n = 633), ESTBB (Estonia; n = 464), UKBB (United Kingdom; n = 810), AoU (United States; n = 559), BioMe (United States; n = 2,170), MGBB (United States; n = 2,141), UCLA-ATLAS (United States; n = 1,445), QBB (Qatar; n = 2,383) and BBSS (Poland, N = 355). The biobank studies include samples from (hospital) biobanks, prospective epidemiological and disease-based cohorts. Follow-up covers a total of 20 years with the earliest study starting follow-up in 2004 (AoU) and the latest study ending follow-up in 2024 (BioMe). Below we provide a detailed description of the population selected and ancestry definitions in each study.
Inclusion and exclusion criteria for GLP1-RA analysis
For our GLP1-RA analysis we implemented the following inclusion and exclusion criteria. We required an initiation of a GLP1-RA treatment (ATC codes: A10BJ*, A10BX04, A10BX10, A10BX13, A10BX14) defined as the date of first medication purchase or medication prescription of GLP1-RA. Only first-time (GLP1-RA naive) users in the datasets were included. Individuals were required to be on a GLP1-RA treatment for at least 12 months. This was defined through prescription length, regular drug prescription refills or drug purchases, depending on the dataset and healthcare setting.
Individuals aged under 18 were excluded from the analysis. Furthermore, individuals were required to have at least one body weight measurement a maximum of 1 year before treatment initiation or within 14 days after initiation, if no measure before initiation was available. If we observed multiple weight measurements in this time frame, only the one closest to initiation was considered. This measurement defined our baseline weight variable. At least one body weight measurement between 26 and 52 weeks was necessary for each individual to be included in the analysis. Individuals were excluded if they underwent BS before or during the first year of GLP1-RA treatment.
Inclusion and exclusion criteria for BS analysis
For our BS analysis we implemented the following inclusion and exclusion criteria. Individuals were included if they underwent any type of BS. The respected code definitions for BS varied across countries and healthcare systems and can be found in Supplementary Table 22. The proportions of all procedures across cohorts can be found in Supplementary Table 23. Individuals aged under 18 years at baseline were excluded from the analysis. Analogously to the GLP1-RA analysis, individuals were required to have at least one body weight measurement a maximum of 1 year before surgery or within 14 days after it, if no measure before baseline was available. If we observed multiple weight measurements in this time frame, only the one closest to initiation was considered. This measurement defined our baseline weight variable. In addition, at least one body weight measurement between 26 and 208 weeks was necessary for each individual to be included in the analysis.
Outcome definitions
In our primary model, for both GLP1-RA and BS we defined the outcome to be the percentage change in body weight from baseline. The baseline body weight measured closest to T0 and between −52 weeks and +2 weeks from T0 was defined as W0. The second body weight (mW1) was defined as the median of body weight measurements between 26 and 52 weeks from T0 for the GLP1-RA analysis and between 180 and 1,460 days for the BS analysis. This was to enhance robustness against outlier measurements occurring in these intervals.
Therefore, the percentage change in body weight from baseline was calculated using
In our secondary model, we used mW1 as an outcome.
Genetic exposures
We identified 15 genetic variants (SNPs) and two PGS of interest for our analysis. Among the included SNPs, three are functionally characterized GLP1R variants (rs10305492, rs146868158, rs6923761) associated with random glucose levels that have shown a decreased or increased response to different endogenous and exogenous GLP1-RA45. Seven SNPs are GLP1R missense variants (rs1042044, rs10305420, rs3765467, rs10305421, rs2295006, rs10305510, rs201672448) with a frequency >1% in at least one ancestry group in gnomAD (v.4.1)44. One SNP is the only robustly replicated lead genome-wide significant variant (rs429358, ApoE) in a genome-wide association study of BMI change over time41,61. Two SNPs are PCSK1 missense variants (rs6232, rs6235) that have been found associated with BMI variations46. And two SNPs (rs728996, rs17702901) were associated with an effect on excess BMI loss among BS patients36. A list of all genetic exposures and their frequencies across all major continental ancestry groups can be found in Supplementary Table 4. The included PGS are for BMI and T2D62. The PGS weights were taken from ref. 62 and obtained from UK Biobank. The scores were computed in each study using PLINK 2.0 (ref. 63). Because the PGS scores were derived from UK Biobank, we could not use the same score in UK Biobank, instead we used ref. 64.
Statistical model
We used a linear regression model to investigate the effect of the chosen genetic exposures on weight change after initiation of GLP1-RA treatment and BS, respectively. In the primary model we adjusted for the baseline weight, sex, age at initiation of treatment or surgery in years, the first 20 genetic principal components (PCs) and study-specific covariates, such as the genotyping batch. In the GLP1-RA analysis we additionally adjusted for the medication type in the drug class.
We defined % weight change as the outcome variable in the primary model.
Primary model:
Meta-analyses
We conducted ancestry-specific and multiancestry fixed-effect meta-analyses for each of the genetic exposures. Effect sizes were combined using fixed-effect inverse-variance weighting, as implemented in the R package meta65. For each exposure we reported the unadjusted P values, but considered as threshold for statistical significance P < 0.004 for GLP1-RA (that is, P < \(\frac{0.05}{13}\), Bonferroni correction for 13 exposures tested) and P < 0.01 for BS (that is, P < \(\frac{0.05}{5}\), Bonferroni correction for 5 exposures tested). We tested for heterogeneity in effect sizes between ancestries using Cochran’s Q-test66 and by inspecting the I2 statistics67, which is defined as:
where d.f. is equal to the number of studies − 1.
Power calculation
To calculate the statistical power for the PGS effect sizes, we used a t-test for linear regression coefficient as implemented in the R package pwrs68 assuming a standard deviation for the outcome variable s.d.y = 7.8 (weighted combine s.d. across studies), a sample size of n = 6,750, a total number of predictors k = 25 and an adjusted r2 = 0.05 (coefficient of determination), to calculate power at P < 0.05 significance level.
For the coefficients of association with single variants, we estimated statistical power via the noncentrality parameter of the chi-squared distribution. We defined the noncentrality parameter as 2f (1 − f) n β2 where f is MAF, n is the effective sample size and β is the expected effect size69. We set a beta value of 0.3 (percent weight change from baseline) as the expected genetic effect on GLP1 response, based on findings from a recent large-scale study on genetic influences on drug response52.
Cohort descriptions and ancestry definitions
All of Us
The AoU Research Program is a longitudinal cohort study aiming to enroll at least one million individuals across a diverse population in the United States. More than 245,000 individuals have genotype data. The sensitivity for single nucleotide variants was >98.7% and the precision was >99.9%.
Ancestry categories were based on gnomAD and inferred using principal components analysis (PCA) data. The patterns of ancestry and admixture were compared with self-identified race and ethnicity, and continuous ancestry inference using genome-wide genotypes resulted in concordant estimates. We restricted participants to an unrelated subset. The participants were further filtered based on the criteria described in the analysis plan (for example, \(\frac{\mathrm{Per}\; \mathrm{ancestry}\; \mathrm{minimum}\; \mathrm{allele}\; \mathrm{count}}{\mathrm{Sample}\; \mathrm{size}}\) after filtering on availability of weight measurements and prescription and/or BS).
Bialystok Bariatric Surgery Study
The BBSS is a prospective cohort study of patients undergoing BS at the First Clinical Department of General and Endocrine Surgery at the Medical University of Bialystok. This is the primary receiving center for patients referred for BS in the province of Podlaskie Voivodeship and the largest center by number of bariatric surgeries performed in northeastern Poland. This center specializes in several bariatric surgical techniques including RYGB, gastric banding and SG. For this study, we selected only patients who underwent SG because it represents the vast majority (>90%) of all interventions performed at the center and to eliminate confounding variation in surgical technique. The BBSS began in 2015 and consisted of a battery of baseline tests established one month before the intervention and repeated at 1-, 3-, 6- and 12-month follow-up clinical visits. Subsequently, patients are examined every year after the first year. At each visit, all subjects underwent physical examination, body composition analysis and blood testing, as well as completed diet and physical activity questionnaires. All subjects give their informed consent for inclusion before participating in the study. The study is conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Medical University of Bialystok (Project identification code: R-I-002/546/2015).
Genetic ancestry in the BBSS cohort was determined using a combination of self-reported race or ethnicity and genotype-based analysis. Self-reported race or ethnicity information was collected during baseline assessments. Additionally, genetic ancestry was further refined through genotype clustering analyses using reference populations from the 1000 Genomes Project.
BioMe
The BioMe Biobank, founded in 2007, is an ongoing EHR-linked biorepository that enrolls participants nonselectively from across the Mountain Sinai Health System. More than 60,000 participants have been recruited from >26 outpatients sites located in Manhattan and Queens, and recruitment is ongoing. We restricted participants to an unrelated subset (based on second-degree or greater KING-derived kinship coefficients) who had been genotyped with either the Global Screening Array or Global Diversity Array. We then filtered this population to those adhering to the criteria described in the analysis plan (for example, \(\frac{\mathrm{Per}\;\mathrm{ancestry}\;\mathrm{minimum}\;\mathrm{allele}\;\mathrm{count}}{\mathrm{Sample}\;\mathrm{size}}\) after filtering on availability of weight measurements and prescription and/or BS).
Genetically determined ancestry group based on ADMIXTURE with K = 10 (where K refers to the number of ancestral clusters inferred in the ADMIXTURE analysis), with grouping based on which 1000 Genomes phase 3 reference samples (with superpopulation labels as reference) showed the highest proportion for a given class. The choice for K = 10 was based on a combination of minimizing cross-validation errors for admixture analysis, as well as minimizing the Frobenius distance of each ADMIXTURE matrix K with the matrix outputted by Genetic Relationship and Fingerprinting.
Estonian Biobank
ESTBB is a population-based biobank that involves more than 212,000 adult participants (about 20% of the Estonian adult population). The Estonian Biobank Project was initiated in 1999; data collection began in 2002. Initially, participants were recruited by general practitioners across Estonia from among individuals visiting general practitioners’ offices and hospitals. Consenting adults donated blood samples for DNA extraction, underwent anthropometric, blood pressure and resting heart rate measurement, and provided extensive information on demographic characteristics, genealogy, education, occupation and lifestyle, as well as health status and medical history70. From 2017 onward, the process of joining ESTBB was simplified: new joiners were required to sign an online consent form, visit a healthcare provider or pharmacy to provide a blood sample, and fill in an online questionnaire. Additional data are collected through linkage with various national databases and registries and through subsequent studies involving different subsets of participants.
Participants were genotyped using the Illumina Global Screening Array v.1.0, v.2.0 and v.2.0_EST. Samples were genotyped and PLINK format files created using Illumina GenomeStudio v.2.0.4. Individuals with call rates below 95% or whose sex in phenotype data did not match X chromosome heterozygosity were excluded. Before imputation, variants were filtered by call rate <95%, Hardy–Weinberg equilibrium P < 1 × 10−4 (autosomal variants only) and MAF < 1%. A population-specific imputation reference panel of 2,297 whole-genome sequencing (WGS) samples was used71.
We aligned participants to 21 major ancestry groups similarly to Privé72. We removed participants with nonEuropean assigned group ancestry, keeping Europeans, Finns and Italians.
Helsinki University Hospital/Helsinki Biobank
The Helsingin Biopankki (Helsinki Biobank) was founded in 2015 by HUS Helsinki University Hospital, University of Helsinki, the Joint Municipality for Health and Social Services in the Kymenlaakso Valley (Kymsote) and the South Karelia Social and Health Care District (Exote), and is the largest hospital biobank in Finland. Approximately 80,000 patients have given a blood sample based on biobank consent and used for research purposes. Diagnostic formalin-fixed paraffin-embedded tissue samples from approximately one million patients have been transferred to the biobank’s sample collection. The biobank’s samples were combined with clinical patient data from the hospital’s database (HUS Datapool) in accordance with the description in the research plan recommended by the ethics committee. Data that are run together can usually include the sampling date, the donor’s gender, histological and cytological examinations, diagnoses, care measures and laboratory examination results.
Mass General Brigham Biobank
Mass General Brigham is an integrated healthcare system located in Boston, Massachusetts for more than 1.5 million individuals per year. The MGBB has recruited more than 140,000 participants since 2008. More than 65,000 participants have genotype data sequenced using the Illumina Multi-Ethnic Genotyping assay or the Illumina Global Screening Array. All genotyped biospecimens had at least 99% call rate per array and were confirmed for sex concordance using sex in EHR and sex computed from array data.
Ancestry was defined using high-dimensional PCs, specifically top 30 genetic PCs and a network-based clustering approach. We restricted participants to an unrelated subset. The participants were further filtered based on the criteria described in the analysis plan (for example, \(\frac{\mathrm{Per}\;\mathrm{ancestry}\;\mathrm{minimum}\;\mathrm{allele}\;\mathrm{count}}{\mathrm{Sample}\;\mathrm{size}}\) after filtering on availability of weight measurements and prescription and/or BS).
UCLA-ATLAS (Atlas Biobank)
ATLAS is an EHR-linked biobank across multiple institutions in the UCLA Health System. After participants signed informed consent for participation to the UCLA-ATLAS Community Health Initiative, biological samples in the form of de-identified blood samples were collected and subsequently processed for DNA extraction and genotyping. The data analyzed in this manuscript draw from a ‘frozen snapshot’ of ATLAS data encompassing all available samples up to 15 February 2024, totaling n = 53,829. The corresponding EHR data for ATLAS participants were sourced from the UCLA Data Discovery Repository. This repository operates under the auspices of the UCLA Health Office of Health Informatics Analytics and the UCLA Institute of Precision Health. Patient Recruitment and Sample Collection for Precision Health Activities at UCLA is an approved study by the UCLA Institutional Review Board. Extensive details on ATLAS genotyping and quality control were previously reported in ref. 73. In short, participants in the ATLAS initiative were genotyped using a custom genotyping array constructed from the Global Screening Array with the Infinium Global Screening Array-24 Kit (Illumina), a multidisease drop-in panel aligned with the GRCh38 assembly. SNPs were subjected to removal if they were unmapped, strand-ambiguous, duplicates or exhibited >5% missingness. Samples with missingness exceeding >5% were excluded, as were duplicates (including identical twins or triplets) with preference given to individuals with the lowest missing rate in each pair. Imputation to the TOPMedFreeze5 was conducted using the Michigan Imputation Server74. After imputation, SNPs with a quality score (R2) below 0.90 were excluded, for PGS calculation SNPs with a MAF below 0.1% were filtered out.
The genetic ancestry of ATLAS individuals was estimated by assessing their proximity to 1000 Genome super populations on the PC space. We computed the top 20 PCs using bigsnpr R software with default parameters. Subsequently, leveraging the superpopulation label and PCs of the 1000 Genome individuals, we train a K-nearest neighbors model to assign genetic ancestry labels to each ATLAS individual. To optimize model performance, we used tenfold cross-validation to select the optimal hyperparameter (k) from a range of values (k = 5, 10, 15, 20). In instances in which an individual was assigned to multiple ancestries with probability >0.5 or was not assigned to any cluster, their ancestry was labeled as unknown. We clustered 94% of the ATLAS participants into one of the five 1000 Genome superpopulation (African (AFR), admixed American (AMR), East Asian (EAS), European (EUR), Middle Eastern (MID), South Asian (SAS)) while the remaining individuals’ ancestry could not be ascertained.
UK Biobank
The UKBB is a large-scale biomedical database and research resource containing in-depth genetic and health information from half a million UK participants. Upon signing informed consent, participants provided biological samples, including de-identified blood samples, which were processed for DNA extraction and genotyping. The dataset analyzed in this manuscript is derived from a ‘frozen snapshot’ of the UKBB data, encompassing all available samples up to 31 January 2024, totaling n = 502,536. Corresponding EHR data for UKBB participants were sourced from the UK Biobank Resource, which operates under the auspices of the UK Biobank Steering Committee and has received ethical approval from the North West Multi-centre Research Ethics Committee. Detailed information on UKBB genotyping and quality control has been previously reported75. Samples were genotyped at the Affymetrix Research Services Laboratory in Santa Clara, California, USA. Upon receipt of a 96-well plate containing 94 UK Biobank samples, Affymetrix added two control individuals (from 1000 Genomes) to the same well positions on each plate. Genotypes were then called from the resulting intensities in batches of ~4,700 samples (~4,800 including the controls) using Affymetrix Power Tools software and Affymetrix Best Practices Workflow. After genotype calling, Affymetrix performed quality control in each batch separately, to exclude SNPs with poor cluster properties. If an SNP did not meet the Affymetrix prescribed QC thresholds in a given batch, it was set to missing in all individuals from that batch. Affymetrix also checked sample quality (such as DNA concentration) and genotype calls were provided only for samples with sufficient DNA metrics.
The ancestry composition of UKBB participants was defined based on self-reported ethnicities and genetic PCA. Participants self-reported their ethnic backgrounds into categories such as White, Mixed, Asian or Asian British, Black or Black British, and Other ethnic groups, with the majority (~94%) identifying as White British. Genetic PCA was used to capture the underlying population structure and define genetic ancestry more precisely, categorizing participants into groups such as European, South Asian, African, East Asian and other ancestries. This approach ensured a nuanced understanding of the genetic and demographic diversity in the cohort, enabling robust and reliable biomedical research.
To capture population structure specific to the UKBB cohort, we performed principal component analysis of ~150,000 UKBB samples using ~100,000 SNPs. These PCs can be used to identify samples with similar ancestry or to control for population structure in association studies.
Qatar Biobank
This study was based on the second release of 14,060 Qatari participants (all from the same ancestry, MID) from the population-based Qatar Genome Program (QGP). Ethical approval was provided by the institutional review board of the QBB (Protocol no. QF-QBB-RES-ACC-00205). A detailed description of the recruitment process and collection of phenotypic data by the QGP and the QBB was previously reported76. A signed consent was obtained from all included participants by the QBB, and WGS data used in the current study were obtained from the QGP as previously described77. All samples were sequenced on Illumina HiSeq X instruments to obtain WGS with a target average depth of coverage of 30×. The read mapping, variant calling and joint variant calling were performed using Sentieon’s DNASeq pipeline v.201808.03, following the BWA-GATK Best Practice Workflow and using the GRCh38/hg38 reference genome. The produced gVCF were jointly called to produce one multisample VCF file for the whole cohort. Clinical data are extracted from the EMR of the Hamad Medical Corporation.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The Helsinki Biobank can provide access for research projects within the scope regulated by the Finnish Biobank Act, which is research utilizing the biobank samples or data for the purposes of promoting health, understanding the mechanisms of disease or developing products and treatment practices used in health and medical care. De-identified data of the MGBB that supports this study is available from the MGB Biobankportal at https://www.massgeneralbrigham.org/en/research-and-innovation/participate-in-research/biobank/for-researchers. Restrictions apply to the availability of these data, which are available to MGB-affiliated researchers via a formal application. UK Biobank data are available through a procedure described at http://www.ukbiobank.ac.uk/using-the-resource/. Registered researchers whose institutions have Data Use and Registration Agreements in place with All of Us that include the Controlled Tier can access genomic data. Clinical and genotype data from UCLA ATLAS Community Health Initiative patients, de-identified for research purposes, are accessible to UCLA-approved researchers through the Discovery Data Repository (DDR). BioMe data is available through a process described at https://icahn.mssm.edu/research/ipm/programs/biome-biobank/researcher-faqs. Pseudonymized data and/or biological samples can be accessed for research and development purposes in accordance with the Estonian Human Genome Research Act. To access data, the research proposal must be approved by the Scientific Advisory Committee of the Estonian Biobank as well as by the Estonian Committee on Bioethics and Human Research. For more details on data access and relevant documents, please see https://genomics.ut.ee/en/content/estonian-biobank#dataaccess. For access to the Bialystok Bariatric Surgery Study please refer to the Medical University of Bialystok. The data and biosamples collected or generated by QBB will be made available to researchers employed within or otherwise contractually bound to public and private institutions that conduct scientific research and that meet the requirements detailed in the Qatar Biobank Research Access policy. The PGS weights used in this study are available in refs. 62 and 64. Source data are provided with this paper.
Code availability
The study utilized previously published analysis tools as described in the Methods. Additional code used for these analyses is available at https://github.com/dsgelab/glp1-bs-genetics/.
References
Hruby, A. & Hu, F. B. The epidemiology of obesity: a big picture. Pharmacoeconomics 33, 673–689 (2015).
Boutari, C. & Mantzoros, C. S. A. 2022 update on the epidemiology of obesity and a call to action: as its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism 133, 155217 (2022).
European survey finds over three-quarters of adults with obesity have attempted to lose weight in the past year, but most have been unsuccessful. EASO Secretariat https://easo.org/european-survey-finds-over-three-quarters-of-adults-with-obesity-have-attempted-to-lose-weight-in-the-past-year-but-most-have-been-unsuccessful/ (2022).
Kreymann, B., Williams, G., Ghatei, M. A. & Bloom, S. R. Glucagon-like peptide-1 7-36: a physiological incretin in man. Lancet 2, 1300–1304 (1987).
Nauck, M. A. et al. Normalization of fasting glycaemia by intravenous GLP-1 ([7-36 amide] or [7-37]) in type 2 diabetic patients. Diabet. Med. 15, 937–945 (1998).
Ryan, D. H. et al. Long-term weight loss effects of semaglutide in obesity without diabetes in the SELECT trial. Nat. Med. 30, 2049–2057 (2024).
Wilding, J. P. H. et al. Once-weekly semaglutide in adults with overweight or obesity. N. Engl. J. Med. 384, 989–1002 (2021).
Rubino, D. M. et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body weight in adults with overweight or obesity without diabetes: the STEP 8 randomized clinical trial. JAMA 327, 138–150 (2022).
Marso, S. P. et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 375, 311–322 (2016).
Marso, S. P. et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 375, 1834–1844 (2016).
Perkovic, V. et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N. Engl. J. Med. 391, 109–121 (2024).
Sattar, N. et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 9, 653–662 (2021).
Watanabe, J. H., Kwon, J., Nan, B. & Reikes, A. Trends in glucagon-like peptide 1 receptor agonist use, 2014 to 2022. J. Am. Pharm. Assoc. 64, 133–138 (2024).
The increase in appetite for obesity drugs. J.P. Morgan https://www.jpmorgan.com/insights/global-research/current-events/obesity-drugs (2023).
Clapp, B. et al. American Society for Metabolic and Bariatric Surgery 2020 estimate of metabolic and bariatric procedures performed in the United States. Surg. Obes. Relat. Dis. 18, 1134–1140 (2022).
Centers for Medicare & Medicaid Services. Billing and Coding: Bariatric Surgery Coverage (A53028). https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleid=53028 (accessed March 2025).
Gloy, V. L. et al. Bariatric surgery versus non-surgical treatment for obesity: a systematic review and meta-analysis of randomised controlled trials. BMJ 347, f5934 (2013).
Salminen, P. et al. Effect of laparoscopic sleeve gastrectomy vs Roux-en-Y gastric bypass on weight loss, comorbidities, and reflux at 10 years in adult patients with obesity: the SLEEVEPASS randomized clinical trial. JAMA Surg. 157, 656–666 (2022).
Lim, R., Beekley, A., Johnson, D. C. & Davis, K. A. Early and late complications of bariatric operation. Trauma Surg. Acute Care Open 3, e000219 (2018).
Doumouras, A. G. et al. Bariatric surgery and cardiovascular outcomes in patients with obesity and cardiovascular disease: a population-based retrospective cohort study. Circulation 143, 1468–1480 (2021).
Elsaid, M. I. et al. Association of bariatric surgery with cardiovascular outcomes in adults with severe obesity and nonalcoholic fatty liver disease. JAMA Netw. Open 5, e2235003 (2022).
Adams, T. D. et al. Long-term all-cause and cause-specific mortality for four bariatric surgery procedures. Obesity (Silver Spring) 31, 574–585 (2023).
Cadena-Obando, D. et al. Are there really any predictive factors for a successful weight loss after bariatric surgery? BMC Endocr. Disord. 20, 20 (2020).
Çalık Başaran, N., Dotan, I. & Dicker, D. Post metabolic bariatric surgery weight regain: the importance of GLP-1 levels. Int. J. Obes. (Lond.) https://doi.org/10.1038/s41366-024-01461-2 (2024).
Young, K. G. et al. Treatment effect heterogeneity following type 2 diabetes treatment with GLP1-receptor agonists and SGLT2-inhibitors: a systematic review. Commun. Med. (Lond.) 3, 131 (2023).
Jones, A. G. et al. Markers of β-cell failure predict poor glycemic response to GLP-1 receptor agonist therapy in type 2 diabetes. Diabetes Care 39, 250–257 (2016).
Dawed, A. Y. et al. Pharmacogenomics of GLP-1 receptor agonists: a genome-wide analysis of observational data and large randomised controlled trials. Lancet Diabetes Endocrinol. 11, 33–41 (2023).
Brown, E., Wilding, J. P. H., Barber, T. M., Alam, U. & Cuthbertson, D. J. Weight loss variability with SGLT2 inhibitors and GLP-1 receptor agonists in type 2 diabetes mellitus and obesity: mechanistic possibilities. Obes. Rev. 20, 816–828 (2019).
Umapathysivam, M. M. et al. Type 2 diabetes risk alleles in peptidyl-glycine alpha-amidating monooxygenase influence GLP-1 levels and response to GLP-1 receptor agonists. Preprint at medRxiv https://doi.org/10.1101/2023.04.07.23288197 (2023).
Jensterle, M., Rizzo, M., Haluzík, M. & Janež, A. Efficacy of GLP-1 RA approved for weight management in patients with or without diabetes: a narrative review. Adv. Ther. 39, 2452–2467 (2022).
Nathan, B. M. et al. Predictors of weight-loss response with glucagon-like peptide-1 receptor agonist treatment among adolescents with severe obesity. Clin. Obes. 6, 73–78 (2016).
Vosoughi, K. et al. Association of glucagon-like peptide 1 analogs and agonists administered for obesity with weight loss and adverse events: a systematic review and network meta-analysis. EClinicalMedicine 42, 101213 (2021).
Segal, J. B. et al. Assessing heterogeneity of treatment effect in real-world data. Ann. Intern. Med. 176, 536–544 (2023).
Jensterle, M., Pirš, B., Goričar, K., Dolžan, V. & Janež, A. Genetic variability in GLP-1 receptor is associated with inter-individual differences in weight lowering potential of liraglutide in obese women with PCOS: a pilot study. Eur. J. Clin. Pharmacol. 71, 817–824 (2015).
van der Meer, R. et al. Genetic variants associated with weight loss and metabolic outcomes after bariatric surgery: a systematic review. Obes. Rev. 24, e13626 (2023).
Aasbrenn, M. et al. Genetic determinants of weight loss after bariatric surgery. Obes. Surg. 29, 2554–2561 (2019).
de Toro-Martín, J. et al. Polygenic risk score for predicting weight loss after bariatric surgery. JCI Insight 3, e122011 (2018).
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in underweight and obesity from 1990 to 2022: a pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet 403, 1027–1050 (2024).
White, G. E. et al. Real-world weight-loss effectiveness of glucagon-like peptide-1 agonists among patients with type 2 diabetes: a retrospective cohort study. Obesity 31, 537–544 (2023).
Inoue, K. et al. Long-term impact of liraglutide, a glucagon-like peptide-1 (GLP-1) analogue, on body weight and glycemic control in Japanese type 2 diabetes: an observational study. Diabetol. Metab. Syndr. 6, 95 (2014).
Venkatesh, S. S. et al. Characterising the genetic architecture of changes in adiposity during adulthood using electronic health records. Nat. Commun. 15, 5801 (2024).
Xu, J. et al. Exploring the clinical and genetic associations of adult weight trajectories using electronic health records in a racially diverse biobank: a phenome-wide and polygenic risk study. Lancet Digit. Health 4, e604–e614 (2022).
Cardoso, P. et al. Phenotype-based targeted treatment of SGLT2 inhibitors and GLP-1 receptor agonists in type 2 diabetes. Diabetologia 67, 822–836 (2024).
Karczewski, K. J. et al. The mutational constraint spectrum quantified from variation in 141,456 humans. Nature 581, 434–443 (2020).
Lagou, V. et al. GWAS of random glucose in 476,326 individuals provide insights into diabetes pathophysiology, complications and treatment stratification. Nat. Genet. 55, 1448–1461 (2023).
Nead, K. T. et al. Contribution of common non-synonymous variants in PCSK1 to body mass index variation and risk of obesity: a systematic review and meta-analysis with evidence from up to 331 175 individuals. Hum. Mol. Genet. 24, 3582–3594 (2015).
Vickers, A. J. The use of percentage change from baseline as an outcome in a controlled trial is statistically inefficient: a simulation study. BMC Med. Res. Methodol. 1, 6 (2001).
Curran-Everett, D. Explorations in statistics: the analysis of ratios and normalized data. Adv. Physiol. Educ. 37, 213–219 (2013).
Berry, D. A. & Ayers, G. D. Symmetrized percent change for treatment comparisons. Am. Stat. 60, 27–31 (2006).
Lepage, B., Lamy, S., Dedieu, D., Savy, N. & Lang, T. Estimating the causal effect of an exposure on change from baseline using directed acyclic graphs and path analysis. Epidemiology 26, 122–129 (2015).
Glymour, M. M., Weuve, J., Berkman, L. F., Kawachi, I. & Robins, J. M. When is baseline adjustment useful in analyses of change? An example with education and cognitive change. Am. J. Epidemiol. 162, 267–278 (2005).
Sadler, M. C. et al. Leveraging large-scale biobank EHRs to enhance pharmacogenetics of cardiometabolic disease medications. Nat. Commun. 16, 2913 (2025).
Weiss, T. et al. Real-world weight change, adherence, and discontinuation among patients with type 2 diabetes initiating glucagon-like peptide-1 receptor agonists in the UK. BMJ Open Diabetes Res. Care 10, e002517 (2022).
Ghusn, W. et al. Weight loss outcomes associated with semaglutide treatment for patients with overweight or obesity. JAMA Netw. Open 5, e2231982 (2022).
Xu, T. et al. Timing of maximal weight reduction following bariatric surgery: a study in Chinese patients. Front. Endocrinol. 11, 615 (2020).
Monpellier, V. M., Janssen, I. M. C., Antoniou, E. E. & Jansen, A. T. M. Weight change after Roux-en Y gastric bypass, physical activity and eating style: is there a relationship? Obes. Surg. 29, 526–533 (2019).
Knop, F. K. et al. Oral semaglutide 50 mg taken once per day in adults with overweight or obesity (OASIS 1): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 402, 705–719 (2023).
Hall, K. D. & Kahan, S. Maintenance of lost weight and long-term management of obesity. Med. Clin. North Am. 102, 183–197 (2018).
Mok, J. et al. Safety and efficacy of liraglutide, 3.0 mg, once daily vs placebo in patients with poor weight loss following metabolic surgery: the BARI-OPTIMISE randomized clinical trial. JAMA Surg. 158, 1003–1011 (2023).
Borrell, L. N. et al. Race and genetic ancestry in medicine – a time for reckoning with racism. N. Engl. J. Med. 384, 474–480 (2021).
Kemper, K. E. et al. Genetic influence on within-person longitudinal change in anthropometric traits in the UK Biobank. Nat. Commun. 15, 3776 (2024).
Weissbrod, O. et al. Leveraging fine-mapping and multipopulation training data to improve cross-population polygenic risk scores. Nat. Genet. 54, 450–458 (2022).
Chang, C. C. et al. Second-generation PLINK: rising to the challenge of larger and richer datasets. Gigascience 4, 7 (2015).
Thompson, D. J. et al. A systematic evaluation of the performance and properties of the UK Biobank Polygenic Risk Score (PRS) Release. PLoS One 19, e0307270 (2024).
Schwarzer, G., Carpenter, J. R. & Rücker, G. Meta-Analysis with R (Springer, 2015).
Cochran, W. G. The combination of estimates from different experiments. Biometrics 10, 101–129 (1954).
Higgins, J. P. T. & Thompson, S. G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 21, 1539–1558 (2002).
Bulus, M. A practical guide to statistical power and sample size calculations in R. https://cran.r-project.org/web/packages/pwrss/vignettes/examples.html (2023).
Kanai, M. et al. Insights from complex trait fine-mapping across diverse populations. Preprint at bioRxiv https://doi.org/10.1101/2021.09.03.21262975 (2021).
Leitsalu, L. et al. Cohort profile: Estonian Biobank of the Estonian Genome Center, University of Tartu. Int. J. Epidemiol. 44, 1137–1147 (2015).
Mitt, M. et al. Improved imputation accuracy of rare and low-frequency variants using population-specific high-coverage WGS-based imputation reference panel. Eur. J. Hum. Genet. 25, 869–876 (2017).
Privé, F. Using the UK Biobank as a global reference of worldwide populations: application to measuring ancestry diversity from GWAS summary statistics. Bioinformatics 38, 3477–3480 (2022).
Johnson, R. et al. The UCLA ATLAS Community Health Initiative: Promoting precision health research in a diverse biobank. Cell Genom. 3, 100243 (2023).
Das, S. et al. Next-generation genotype imputation service and methods. Nat. Genet. 48, 1284–1287 (2016).
Genotyping and quality control of UK Biobank, a large-scale, extensively phenotyped prospective resource. UKBiobank https://biobank.ctsu.ox.ac.uk/crystal/crystal/docs/genotyping_qc.pdf (2015).
Al Thani, A. et al. Qatar Biobank Cohort Study: study design and first results. Am. J. Epidemiol. https://doi.org/10.1093/aje/kwz084 (2019).
Mbarek, H., et al. Qatar genome: Insights on genomics from the Middle East. Hum. Mutat. https://doi.org/10.1002/humu.24336 (2022).
Acknowledgements
We gratefully acknowledge the resources provided by the Institute for Precision Health and participating patients from the UCLA ATLAS Community Health Initiative (https://www.uclahealth.org/international-services/consulting-services/clinical-research-consultation/ucla-atlas-community-health-initiative). The UCLA ATLAS Community Health Initiative in collaboration with UCLA ATLAS Precision Health Biobank is a program of the Institute for Precision Health, which directs and supports the biobanking and genotyping of biospecimen samples from participating patients from UCLA in collaboration with the David Geffen School of Medicine, UCLA Clinical and Translational Science Institute and UCLA Health. The ATLAS Community Health Initiative is supported by UCLA Health, the David Geffen School of Medicine and a grant from the UCLA Clinical and Translational Science Institute (UL1TR001881). This work was financially supported in part by National Institutes of Health awards U01HG011715, R01HG009120 and R01MH115676. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We thank all participants of HUS (https://www.helsinginbiopankki.fi/en/Helsinki-Biobank; https://www.hus.fi/en), ESTBB (https://genomics.ut.ee/en/content/estonian-biobank), BBSS (https://classic.clinicaltrials.gov/ct2/show/NCT04634591), QBB (https://www.qphi.org.qa/), BioMe (https://icahn.mssm.edu/research/ipm/programs/biome-biobank), UKBB (https://www.ukbiobank.ac.uk/), MGBB (https://www.massgeneralbrigham.org/en/research-and-innovation/participate-in-research/biobank) and AoU (https://allofus.nih.gov/) for their generous contribution. The Estonian Biobank Research Team responsible for data collection, genotyping, QC and imputation: A. Metspalu, T. Esko, R. Mägi, M. Nelis and G. Hudjashov. L.S. is supported by funds from the Ministry of Education and Science of Poland within the project 'Excellence Initiative - Research University', the Ministry of Health of Poland within the project 'Center of Artificial Intelligence in Medicine at the Medical University of Bialystok', the Medical Research Agency within the project 'Regional Center for Digital Medicine at the Medical University of Bialystok' (grant number 2023/ABM/02/00008), and the American Diabetes Association grant 11-22-PDFPM-03. A.J. is supported by funds from the Ministry of Education and Science of Poland within the project 'Excellence Initiative - Research University', the Ministry of Health of Poland within the project 'Center of Artificial Intelligence in Medicine at the Medical University of Bialystok', and the Medical Research Agency within the project 'Regional Center for Digital Medicine at the Medical University of Bialystok' (grant number 2023/ABM/02/00008). This work and J.G. were further supported in part by funding from the Eric and Wendy Schmidt Center at the Broad Institute of MIT and Harvard. U.V. and K.A. have been funded by Estonian Research Council’s personal research funding start-up grant no. PSG759 and European Research Council’s starting grant under the grant agreement no. 101117251 (OBECAUSE). J.H.L. is supported by NIDDK K23 DK131345. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Funding
Open Access funding provided by University of Helsinki (including Helsinki University Central Hospital).
Author information
Authors and Affiliations
Contributions
J.G., M.C., A.P., B.P., R.J.F.L., R.A.J.S., H.O.H., H.M., U.V. and A.G. conceptualized the study. J.G., M.C. and A.G. designed the analyses. J.G., M.C., V.T., S.U., K.A., R.A.J.S., J.L., J.H.L., A.J., Y.D., A.A., A.E., C.S., Y.A.-S. and Z.W. performed statistical analyses. J.G., V.T. and C.S. performed PGS-phenotype association analyses. Z.K. and A.C. provided statistical and methodological support for the statistical analyses. A.P., L.S., B.P. and R.J.F.L. provided methodological support. J.G., M.C., T.C. and A.G. mainly drafted and revised the manuscript. All authors provided interpretation.
Corresponding author
Ethics declarations
Competing interests
A.G. is the founder of Real World Genetics OY. P.N. reports research grants from Allelica, Amgen, Apple, Boston Scientific, Genentech/Roche and Novartis; personal fees from Allelica, Apple, AstraZeneca, Blackstone Life Sciences, Creative Education Concepts, CRISPR Therapeutics, Eli Lilly & Co, Foresite Labs, Genentech/Roche, GV, HeartFlow, Magnet Biomedicine, Merck and Novartis; scientific advisory board membership of Esperion Therapeutics, Preciseli, TenSixteen Bio and Tourmaline Bio; scientific co-founder of TenSixteen Bio; equity in MyOme, Preciseli and TenSixteen Bio; and spousal employment at Vertex Pharmaceuticals, all unrelated to the present work. A.P. is an employee of Alphabet Corporation. He has previously received research support from Microsoft, Alphabet, Intel, IBM and Bayer.
Peer review
Peer review information
Nature Medicine thanks Naveed Sattar and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editors: Liam Messin and Sonia Muliyil, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Study Design.
a, Eligibility criteria are displayed for the GLP1-RA analysis and the BS analysis. The axis represents time in weeks. The highlighted areas depict the time intervals for determining the baseline weight (W0) and final weight (mW1), defined as the median of body weight measurements in the given time interval. Detailed information on the eligibility criteria can be found in the Methods. b, Outcome definition for our primary model. Detailed information can be found in the Methods. Created in BioRender. German, J. (2025) https://BioRender.com/i42b370.
Extended Data Fig. 2 Effect sizes of baseline weight on weight loss amongst GLP1-RA users across studies by ancestries.
Points represent beta coefficients in Kg and error bars represent the 95% confidence intervals. Negative beta coefficients indicate that higher baseline weight is associated with greater weight loss, while positive beta coefficients indicate the opposite. Total N = 6 750, sample size per each cohort/ancestry can be found in Table 1. AoU: All of Us, ATLAS: UCLA-Atlas Biobank, BioMe: BioMe Biobank, ESTBB: Estonian Biobank, HUS: Helsinki University Hospital, MGBB: Mass General Brigham Biobank, QBB: Qatar Biobank, UKBB: UK Biobank, AFR: African, AMR: admixed American, EAS: East Asian, EUR: European, MID: Middle Eastern, SAS: South Asian.
Extended Data Fig. 3 Effect sizes of sex on weight loss amongst GLP1-RA users across studies by ancestries.
Points represent beta coefficients in Kg and error bars represent the 95% confidence intervals. Negative beta coefficients indicate that female sex is associated with greater weight loss, while positive beta coefficients indicate the opposite. Total N = 6 750, sample size per each cohort/ancestry can be found in Table 1. AoU: All of Us, ATLAS: UCLA-Atlas Biobank, BioMe: BioMe Biobank, ESTBB: Estonian Biobank, HUS: Helsinki University Hospital, MGBB: Mass General Brigham Biobank, QBB: Qatar Biobank, UKBB: UK Biobank, AFR: African, AMR: admixed American, EAS: East Asian, EUR: European, MID: Middle Eastern, SAS: South Asian.
Extended Data Fig. 4 Effect sizes of age at treatment initiation on weight loss amongst GLP1-RA users across studies by ancestries.
Points represent beta coefficients in Kg and error bars represent the 95% confidence intervals. Negative beta coefficients indicate that baseline age is associated with greater weight loss, while positive beta coefficients indicate the opposite. Total N = 6 750, sample size per each cohort/ancestry can be found in Table 1. AoU: All of Us, ATLAS: UCLA-Atlas Biobank, BioMe: BioMe Biobank, ESTBB: Estonian Biobank, HUS: Helsinki University Hospital, MGBB: Mass General Brigham Biobank, QBB: Qatar Biobank, UKBB: UK Biobank, AFR: African, AMR: admixed American, EAS: East Asian, EUR: European, MID: Middle Eastern, SAS: South Asian.
Supplementary information
Supplementary Information (download PDF )
Supplementary Methods, Results and Figs. 1–12.
Source data
Source Data Fig. 1, 2a, 2b and Extended Data Fig. 2–4. (download XLSX )
An Excel workbook containing the source data to generate Figs 1, 2a, 2b and Extended Data Figs 2–4.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
German, J., Cordioli, M., Tozzo, V. et al. Association between plausible genetic factors and weight loss from GLP1-RA and bariatric surgery. Nat Med 31, 2269–2276 (2025). https://doi.org/10.1038/s41591-025-03645-3
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41591-025-03645-3
This article is cited by
-
The expanding landscape of GLP-1 medicines
Nature Medicine (2026)
-
Glucagon-like peptide-1 medicines and cancer
Nature Cancer (2026)
-
In Vivo Gastric Expression of FTO and MC4R in Sleeve Gastrectomy Patients: Diagnostic Utility Without Predictive Value for Weight Loss
Obesity Surgery (2026)
-
Safety and Tolerability of Glucagon-Like Peptide-1 Receptor Agonists: A State-of-the-Art Narrative Review
Drugs (2026)
-
Bariatric Surgery in the Era of GLP1RA: A Narrative Review
Advances in Therapy (2026)
