
Abstract
Sodium glucose co-transporter 2 inhibitors (SGLT2i) reduce the risk of chronic kidney disease (CKD) progression in type 2 diabetes, but their effects in type 1 diabetes (T1D) are not completely understood. ATTEMPT (Adolescent Type 1 Diabetes Treatment with SGLT2i for Hyperglycemia and Hyperfiltration Trial) is a 22-week, double-blind, randomized, placebo-controlled trial to assess dapagliflozin, as an adjunct to insulin, in youth with T1D. Ninety-eight participants (12–21 years of age, 53% female) were randomly assigned to dapagliflozin 5 mg or placebo alongside ketone monitoring and diabetic ketoacidosis (DKA) risk mitigation education. The primary outcome was change in measured glomerular filtration rate (mGFR) using iohexol clearance. Dapagliflozin reduced mGFR by 8.8 ml min−1 1.73 m−2 when compared to placebo (95% confidence interval (CI): −12.7 to −4.8; P < 0.0001), and participants with higher baseline mGFR experienced greater attenuation with dapagliflozin (r: −0.58; P < 0.0001). HbA1c decreased by 0.47% (95% CI: −0.66 to −0.28), and time in range (glucose levels 70–180 mg dl−1, 4–10 mmol L−1) increased by 9.0% (95% CI: 3.8–14.3). Body weight decreased by 2.8 kg (95% CI: −3.7 to −2.0) with dapagliflozin. No differences were observed with respect to total daily insulin dose (U kg−1). Adverse events were similar between groups, with one mild DKA case in the dapagliflozin group. In youth with T1D, dapagliflozin as an adjunct-to-insulin treatment reduced mGFR, improved glycemic control and was safe when combined with ketone testing and risk mitigation strategies. ClinicalTrials.gov: NCT04333823.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$32.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


Data availability
Due to confidentiality reasons (that is, limitations of informed consent and ethics board approval), the datasets used in this study are not publicly available. Qualified researchers, however, can submit data requests for academic purposes only within 12 months after the publication date, and de-identified data and a data dictionary will be made accessible for up to 12 months. Proposals and statistical analysis plans should be directed to the corresponding author and principal investigator (F.H.M.). Upon proposal acceptance by the corresponding author and the Hospital for Sick Children Research Ethics Board, qualified researchers will be granted access to the data within a reasonable timeframe of approximately 3 months after signing a data-sharing agreement. Corresponding author contact: farid.mahmud@sickkids.ca. Source data are provided with this paper.
Code availability
The code used for data analysis is also available upon reasonable request to the corresponding author (F.H.M.) at farid.mahmud@sickkids.ca.
References
Apperloo, E. M. et al. Efficacy and safety of SGLT2 inhibitors with and without glucagon-like peptide 1 receptor agonists: a SMART-C collaborative meta-analysis of randomised controlled trials. Lancet Diabetes Endocrinol. 12, 545–557 (2024).
Seidu, S. et al. SGLT2 inhibitors—the new standard of care for cardiovascular, renal and metabolic protection in type 2 diabetes: a narrative review. Diabetes Ther. 15, 1099–1124 (2024).
Mosenzon, O. et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 7, 606–617 (2019).
Zinman, B. et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 373, 2117–2128 (2015).
Dekkers, C. C. J. et al. Effects of the SGLT-2 inhibitor dapagliflozin on glomerular and tubular injury markers. Diabetes Obes. Metab. 20, 1988–1993 (2018).
Heerspink, H. J., Perkins, B. A., Fitchett, D. H., Husain, M. & Cherney, D. Z. Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus: cardiovascular and kidney effects, potential mechanisms, and clinical applications. Circulation 134, 752–772 (2016).
Heerspink, H. J. L. et al. Kidney outcomes associated with use of SGLT2 inhibitors in real-world clinical practice (CVD-REAL 3): a multinational observational cohort study. Lancet Diabetes Endocrinol. 8, 27–35 (2020).
Palanca, A., van Nes, F., Pardo, F., Ampudia Blasco, F. J. & Mathieu, C. Real-world evidence of efficacy and safety of SGLT2 inhibitors as adjunctive therapy in adults with type 1 diabetes: a European two-center experience. Diabetes Care 45, 650–658 (2022).
Dandona, P. et al. Efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes (DEPICT-1): 24 week results from a multicentre, double-blind, phase 3, randomised controlled trial. Lancet Diabetes Endocrinol. 5, 864–876 (2017).
Mathieu, C. et al. Efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes (the DEPICT-2 study): 24-week results from a randomized controlled trial. Diabetes Care 41, 1938–1946 (2018).
Sridhar, V. S. et al. Chronic kidney disease in type 1 diabetes: translation of novel type 2 diabetes therapeutics to individuals with type 1 diabetes. Diabetologia 67, 3–18 (2024).
Costacou, T. & Orchard, T. J. Cumulative kidney complication risk by 50 years of type 1 diabetes: the effects of sex, age, and calendar year at onset. Diabetes Care 41, 426–433 (2018).
Bjornstad, P. et al. ISPAD Clinical Practice Consensus Guidelines 2022: microvascular and macrovascular complications in children and adolescents with diabetes. Pediatr. Diabetes 23, 1432–1450 (2022).
Minges, K. E. et al. Correlates of overweight and obesity in 5529 adolescents with type 1 diabetes: the T1D Exchange Clinic Registry. Diabetes Res. Clin. Pract. 126, 68–78 (2017).
Ebekozien, O. et al. Longitudinal trends in glycemic outcomes and technology use for over 48,000 people with type 1 diabetes (2016–2022) from the T1D Exchange Quality Improvement Collaborative. Diabetes Technol. Ther. 25, 765–773 (2023).
Cherney, D. Z. & Sochett, E. B. Evolution of renal hyperfiltration and arterial stiffness from adolescence into early adulthood in type 1 diabetes. Diabetes Care 34, 1821–1826 (2011).
Moriconi, D. et al. Glomerular hyperfiltration predicts kidney function decline and mortality in type 1 and type 2 diabetes: a 21-year longitudinal study. Diabetes Care 46, 845–853 (2023).
Groop, P. H. et al. The presence and severity of chronic kidney disease predicts all-cause mortality in type 1 diabetes. Diabetes 58, 1651–1658 (2009).
Goldenberg, R. M., Gilbert, J. D., Hramiak, I. M., Woo, V. C. & Zinman, B. Sodium-glucose co-transporter inhibitors, their role in type 1 diabetes treatment and a risk mitigation strategy for preventing diabetic ketoacidosis: the STOP DKA protocol. Diabetes Obes. Metab. 21, 2192–2202 (2019).
Garg, S. K., Peters, A. L., Buse, J. B. & Danne, T. Strategy for mitigating DKA risk in patients with type 1 diabetes on adjunctive treatment with SGLT inhibitors: a STICH protocol. Diabetes Technol. Ther. 20, 571–575 (2018).
Biester, T. et al. Effects of dapagliflozin on insulin-requirement, glucose excretion and β-hydroxybutyrate levels are not related to baseline HbA1c in youth with type 1 diabetes. Diabetes Obes. Metab. 19, 1635–1639 (2017).
Škrtić, M. & Cherney, D. Z. Sodium-glucose cotransporter-2 inhibition and the potential for renal protection in diabetic nephropathy. Curr. Opin. Nephrol. Hypertens. 24, 96–103 (2015).
Heerspink, H. J. L. et al. Effect of dapagliflozin on the rate of decline in kidney function in patients with chronic kidney disease with and without type 2 diabetes: a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 9, 743–754 (2021).
Amin, R. et al. The relationship between microalbuminuria and glomerular filtration rate in young type 1 diabetic subjects: the Oxford Regional Prospective Study. Kidney Int. 68, 1740–1749 (2005).
Bjornstad, P. et al. Rapid GFR decline is associated with renal hyperfiltration and impaired GFR in adults with type 1 diabetes. Nephrol. Dial. Transplant. 30, 1706–1711 (2015).
Hostetter, T. H., Olson, J. L., Rennke, H. G., Venkatachalam, M. A. & Brenner, B. M. Hyperfiltration in remnant nephrons: a potentially adverse response to renal ablation. Am. J. Physiol. 241, F85–F93 (1981).
Lovshin, J. A. et al. Hyperfiltration, urinary albumin excretion, and ambulatory blood pressure in adolescents with type 1 diabetes mellitus. Am. J. Physiol. 314, F667–F674 (2018).
Verma, S., Mudaliar, S. & Greasley, P. J. Potential underlying mechanisms explaining the cardiorenal benefits of sodium-glucose cotransporter 2 inhibitors. Adv. Ther. 41, 92–112 (2024).
Schaub, J. A. et al. SGLT2 inhibitors mitigate kidney tubular metabolic and mTORC1 perturbations in youth-onset type 2 diabetes. J. Clin. Invest. 133, e164486 (2023).
Drummond, K. & Mauer, M. The early natural history of nephropathy in type 1 diabetes: II. Early renal structural changes in type 1 diabetes. Diabetes 51, 1580–1587 (2002).
Phillip, M. et al. Long-term efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes: pooled 52-week outcomes from the DEPICT-1 and -2 studies. Diabetes Obes. Metab. 23, 549–560 (2021).
Rosenstock, J. et al. Empagliflozin as adjunctive to insulin therapy in type 1 diabetes: the EASE trials. Diabetes Care 41, 2560–2569 (2018).
Rodbard, H. W. et al. Sotagliflozin added to optimized insulin therapy leads to HbA1c reduction without weight gain in adults with type 1 diabetes: a pooled analysis of inTandem1 and inTandem2. Diabetes Obes. Metab. 22, 2089–2096 (2020).
Parkinson, J., Tang, W., Johansson, C. C., Boulton, D. W. & Hamren, B. Comparison of the exposure–response relationship of dapagliflozin in adult and paediatric patients with type 2 diabetes mellitus. Diabetes Obes. Metab. 18, 685–692 (2016).
Busse, D. et al. Comparison of pharmacokinetics and the exposure–response relationship of dapagliflozin between adolescent/young adult and adult patients with type 1 diabetes mellitus. Br. J. Clin. Pharmacol. 85, 1820–1828 (2019).
Tirucherai, G. S., LaCreta, F., Ismat, F. A., Tang, W. & Boulton, D. W. Pharmacokinetics and pharmacodynamics of dapagliflozin in children and adolescents with type 2 diabetes mellitus. Diabetes Obes. Metab. 18, 678–684 (2016).
Perkins, B. A. et al. Low-dose empagliflozin as adjunct-to-insulin therapy in type 1 diabetes: a valid modelling and simulation analysis to confirm efficacy. Diabetes Obes. Metab. 22, 427–433 (2020).
Danne, T. et al. Improved time in range and glycemic variability with sotagliflozin in combination with insulin in adults with type 1 diabetes: a pooled analysis of 24-week continuous glucose monitoring data from the inTandem program. Diabetes Care 42, 919–930 (2019).
DeSalvo, D. J. et al. Transatlantic comparison of pediatric continuous glucose monitoring use in the Diabetes-Patienten-Verlaufsdokumentation Initiative and Type 1 Diabetes Exchange Quality Improvement Collaborative. Diabetes Technol. Ther. 24, 920–924 (2022).
Purnell, J. Q., Zinman, B. & Brunzell, J. D. The effect of excess weight gain with intensive diabetes mellitus treatment on cardiovascular disease risk factors and atherosclerosis in type 1 diabetes mellitus: results from the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study (DCCT/EDIC) study. Circulation 127, 180–187 (2013).
Chen, J. et al. The efficacy and safety of SGLT2 inhibitors for adjunctive treatment of type 1 diabetes: a systematic review and meta-analysis. Sci. Rep. 7, 44128 (2017).
Pottel, H., Adebayo, O. C., Nkoy, A. B. & Delanaye, P. Glomerular hyperfiltration: part 1—defining the threshold—is the sky the limit? Pediatric Nephrol. 38, 2523–2527 (2023).
Urbano, F., Farella, I., Brunetti, G. & Faienza, M. F. Pediatric type 1 diabetes: mechanisms and impact of technologies on comorbidities and life expectancy. Int. J. Mol. Sci. 24, 11980 (2023).
Zabeen, B. et al. Insulin pump therapy is associated with lower rates of retinopathy and peripheral nerve abnormality. PLoS ONE 11, e0153033 (2016).
Wiseman, M. J., Saunders, A. J., Keen, H. & Viberti, G. Effect of blood glucose control on increased glomerular filtration rate and kidney size in insulin-dependent diabetes. N. Engl. J. Med. 312, 617–621 (1985).
Cherney, D. Z. et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation 129, 587–597 (2014).
Cherney, D. Z. I. et al. Kidney effects of empagliflozin in people with type 1 diabetes. Clin. J. Am. Soc. Nephrol. 16, 1715–1719 (2021).
Sridhar, V. S. et al. Efficacy and safety of sotagliflozin in patients with type 1 diabetes and CKD. J. Am. Soc. Nephrol. https://doi.org/10.1681/ASN.0000000540 (2024).
American Diabetes Association Professional Practice Committee. 14. Children and Adolescents: Standards of Care in Diabetes—2025. Diabetes Care 48, S283–S305 (2025).
Gaebe, K. et al. Evaluation of novel glomerular filtration rate estimation equations in adolescents and young adults with type 1 diabetes. J. Diabetes Complications 36, 108081 (2022).
Favel, K., Irvine, M., Ronsley, R., Panagiotopoulos, C. & Mammen, C. Glomerular filtration rate abnormalities in children with type 1 diabetes. Can. J. Diabetes 46, 457–463.e1 (2022).
Kong, Y. W. et al. Continuous ketone monitoring: exciting implications for clinical practice. Diabetes Obes. Metab. 26, 47–58 (2024).
Thomson, S. C. et al. Acute and chronic effects of SGLT2 blockade on glomerular and tubular function in the early diabetic rat. Am. J. Physiol. 302, R75–R83 (2012).
Perrin, N. & Berg, U. B. Estimated glomerular filtration rates cannot replace measured GFR in type 1 diabetes patients with hyperfiltration. Acta Paediatr. 104, 730–737 (2015).
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 105, S117–S314 (2024).
Acknowledgements
We thank the study participants and the study coordinators and research nurses at each of the clinical trial sites for the overall coordination and conduct of the trial. Additionally, we thank Bay Area Research Logistics (BARL) for their services of receiving, packaging, storing and distributing study medication to the clinical trial sites.
This study was funded by Canadian Institutes for Health Research (CIHR, grant number 157203, to F.H.M.) and Breakthrough T1D (formerly Juvenile Diabetes Research Foundation Canada, grant number 3-SRA-2018-652-Q-R, to F.H.M.) as part of the Strategies for Patient Oriented Research (SPOR) Innovative Clinical Trials (iCT). Additional support was provided by the Children’s Hospital Colorado (CHCO) and University of Colorado Anschutz Medical Campus (to P.B.). The funders had no role in planning, conduct, analysis or decision to publish. AstraZeneca donated study drug and placebo. Dexcom partially donated CGM supplies. This was presented, in part, at the American Diabetes Association 84th Scientific Sessions Symposium (CT-SY47-1) in Orlando, Florida, on 24 June 2024.
Author information
Authors and Affiliations
Contributions
F.H.M. and D.Z.I.C. conceptualized and designed the study, with important contributions made by P.B. and C.C. F.H.M. wrote the paper, and all coauthors (P.B., C.C., A.C., S.J.A., J.C., Y.T.E., L.M., R.M., S.K., N.C., M.M., M.F., F.B., K.L.T., J.H., M.C.R., P.P., L.H., H.J.L.H. and D.Z.I.C.) equally contributed, reviewed and edited the paper. R.M., an external and independent biostatistician, analyzed the data for this paper. The decision to submit the paper for publication was made jointly by all authors.
Corresponding author
Ethics declarations
Competing interests
F.H.M. receives research support from the Canadian Institutes of Health Research (CIHR) and Breakthrough T1D (formerly Juvenile Diabetes Research Foundation (JDRF) Canada). P.B. receives salary and research support from the National Institutes of Health (National Institute of Diabetes and Digestive and Kidney Diseases and National Heart, Lung, and Blood Institute), Breakthrough T1D (formerly JDRF) and the American Heart Association. P.B. also receives research support from the University of Washington Medicine Diabetes Institute and Seattle Children’s Research Institute and holds the Raisbeck Endowed Chair of Diabetes Research at the University of Washington. P.B. reports serving or having served as a consultant for AstraZeneca, Bayer, Bristol Myers Squibb, Boehringer Ingelheim, Eli Lilly, LG Chemistry, Sanofi, Novo Nordisk and Horizon Pharma. P.B. also serves or has served on advisory boards and/or steering committees of AstraZeneca, Bayer, Boehringer Ingelheim, Novo Nordisk and XORTX. P.B. reports grant funding from AstraZeneca, Novo Nordisk, Eli Lilly, Boehringer Ingelheim and Horizon Pharma. D.Z.I.C. is the Gabor Zellerman Chair in Nephrology Research at the University of Toronto and was supported by a Department of Medicine, University of Toronto, Merit Award. He receives support from the CIHR, Diabetes Canada and the Heart & Stroke/Richard Lewar Centre of Excellence in Cardiovascular Research. D.Z.I.C. is also the recipient of a 5-year CIHR–Kidney Foundation of Canada Team Grant award with additional support from Breakthrough T1D. D.Z.I.C. has received honoraria from Boehringer Ingelheim–Lilly, Merck, AstraZeneca, Sanofi, Mitsubishi-Tanabe, AbbVie, Janssen, Amgen, Bayer, Prometic Life Sciences, Bristol Myers Squibb, Maze, Gilead, CSL-Behring, Otsuka, Novartis, Youngene, Lexicon, Inversago, GlaxoSmithKline, Biobridge, Vantage, Altimmune and Novo Nordisk and has received operational funding for clinical trials from Boehringer Ingelheim-Lilly, Merck, Janssen, Sanofi, AstraZeneca, CSL-Behring, Lexicon, Novo Nordisk and Bayer. H.J.L.H. reports funding to conduct clinical trials from AstraZeneca, Bayer, Boehringer Ingelheim, Janssen and Novo Nordisk (payments to his institution, the University of Groningen); consulting fees from AstraZeneca, Alexion, Alnylam, Bayer, Boehringer Ingelheim, BioCity Biopharma, Dimerix, Eli Lilly, Gilead, Idorsia, Janssen, Novartis, Novo Nordisk, Roche and Travere Therapeutics (payments to his institution, the University of Groningen); honoraria for lectures from AstraZeneca, Bayer and Novo Nordisk; and support for traveling to and attending the American Diabetes Association meeting and the American Society of Nephrology meeting from AstraZeneca and Eli Lilly (payment to his institution, the University of Groningen). K.L.T. receives salary and research support from the National Institutes of Health (National Heart, Lung, and Blood Institute) and the American Diabetes Association. K.L.T. also receives research support from the Seattle Children’s Research Institute. The other authors declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks Rhonda Bacher, Mark Cooper, Danijela Tatovic and Katherine Tuttle for their contribution to the peer review of this work. Primary Handling Editors: Liam Messin and Ashley Castellanos-Jankiewicz, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
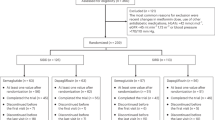
Extended Data Fig. 1 Adolescent Type 1 diabetes Treatment with SGLT2i for hyperglycEMia & hyPerfilTration Trial (ATTEMPT) Schema.
ATTEMPT is a multi-center, double blind, randomized, placebo-controlled trial designed to evaluate the effect of treatment with Dapagliflozin when compared to placebo, in combination with adjustable insulin, on measured GFR and HbA1c in adolescents with T1D over a 22-week evaluation period (16-week treatment period) to test the hypotheses that treatment with dapagliflozin, in combination with adjustable insulin, will reduce mean measured GFR and HbA1c when compared with placebo.
Supplementary information
Supplementary Information (download PDF )
Supplementary Figs. 1–3, Tables 1–4, study protocol and statistical analysis plan.
Source data
Source Data Figs. 2 and 3 (download XLSX )
Statistical source data.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mahmud, F.H., Bjornstad, P., Clarson, C. et al. Adjunct-to-insulin therapy using SGLT2 inhibitors in youth with type 1 diabetes: a randomized controlled trial. Nat Med 31, 2317–2324 (2025). https://doi.org/10.1038/s41591-025-03723-6
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41591-025-03723-6
