
Abstract
The magnitude of weight reduction in the SURMOUNT-1 trial of the dual GLP-1 and GIP receptor agonist tirzepatide suggests that this treatment may be particularly effective in addressing the treatment needs of people with severe obesity (body mass index >40 kg m−2), some of whom may carry rare penetrant genetic variants. Here we investigated the clinical response of men and women in the SURMOUNT-1 trial who carried pathogenic mutations in the melanocortin 4 receptor (MC4R) gene, the most common genetic cause of obesity. We found that 32 of 2,291 people (1.4%) for whom data were available carried pathogenic MC4R mutations. At baseline, MC4R mutation carriers exhibited a higher body mass index compared with noncarriers (40 kg m−2 versus 38 kg m−2; P = 0.036). In the treatment arm, the weight loss trajectory over 72 weeks was comparable in both groups: 18.3% weight reduction in MC4R mutation carriers versus 19.9% in noncarriers. We conclude that tirzepatide is an effective treatment for the most common genetic subtype of obesity, MC4R deficiency.
Similar content being viewed by others

Main
The new generation of obesity medications that target the glucagon-like peptide-1 (GLP-1) receptor and/or the glucose-dependent insulinotropic polypeptide (GIP) receptor are transforming the clinical care of people with obesity and its complications1. In clinical trials, the dual GIP and GLP-1 receptor agonist tirzepatide has been shown to result in substantial weight reduction (~20%) in people with obesity, with and without type 2 diabetes2,3. This magnitude of weight reduction suggests that tirzepatide may be particularly beneficial in people with severe obesity (defined as a body mass index (BMI) >40 kg m−2), who have the highest burden of complications and highest mortality from cardiovascular disease.
Twin, family and adoption studies have consistently demonstrated that genetic factors influence the variation in body weight seen in an obesogenic environment4. The heritable contribution to body weight is greatest in people with severe obesity who have both a higher burden of common obesity susceptibility alleles and a higher prevalence of rare penetrant alleles that drive weight gain from childhood5. The melanocortin 4 receptor (MC4R) is expressed in the hypothalamus, brainstem and other brain regions and plays a pivotal role in the regulation of hunger, satiety and food preference6. Heterozygous MC4R mutations that are dominantly inherited and cause loss of function (LoF) in cells are defined as pathogenic7,8. Pathogenic MC4R mutations have been found in both clinical and population-based cohorts9 at varying frequencies depending on ascertainment criteria: 0.3% of an unselected UK birth cohort10, 1% of adults with a BMI >30 kg m−2, 2% of children with obesity11 and up to 5% of children with severe obesity7. MC4R deficiency, which represents the most common genetic form of obesity, is characterized by hyperphagia (increased drive to eat), weight gain that begins in the first 5 years of life, disproportionate hyperinsulinemia and accelerated linear growth in childhood7,12,13. Adults with MC4R deficiency often have severe obesity but with a lower prevalence of hypertension and reduced systolic and diastolic blood pressure associated with impaired sympathetic nervous system tone14,15.
Obesity due to MC4R deficiency is challenging to treat. Two studies have shown that intense dietary and physical activity interventions11,16 are less effective in children with MC4R deficiency, and weight reduction is harder to maintain in this group. While melanocortin receptor agonists can act as pharmacological chaperones to rescue signaling by some MC4R-mutant receptors in cells17,18, clinical trials of a MC4R agonist have not demonstrated efficacy in this patient group17. As such, there is currently no licensed treatment for people with obesity due to MC4R deficiency. GLP-1 receptor agonists predominantly target non-MC4R-dependent neural pathways in mice19, and there is evidence from a small clinical study with liraglutide20 that they may be effective in people with MC4R deficiency. Here, to investigate the efficacy of tirzepatide in people with MC4R deficiency, we examined genetic data obtained from participants in a randomized controlled trial (SURMOUNT-1) of people with a BMI ≥30 kg m−2, or ≥27 kg m−2 with at least one weight-related comorbidity2, treated with tirzepatide versus placebo.
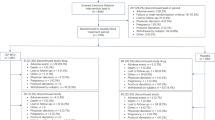
DNA samples of sufficient quality were obtained on 2,291 people (90%) randomized in the SURMOUNT-1 trial. These samples were genotyped using the Axiom genotyping array from Affymetrix. We identified 24 different missense, frameshift and amino acid insertion or deletion mutations; 14 of these mutations have been shown to reduce MC4R function in cells (that is, LoF; https://www.mc4r.org.uk/), giving a prevalence of pathogenic MC4R mutations of 1.4% (n = 32/2,291) in adults with obesity in the SURMOUNT-1 study (Extended Data Table 1). People carrying either of the two prevalent gain-of-function MC4R variants (V103I and I251L; n = 88), associated with lower BMI in cohort studies21, were excluded from all analyses.
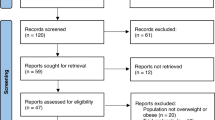
We found that, at baseline, the BMI distribution differed between MC4R mutation carriers and noncarriers (P = 0.036); a greater proportion of people with MC4R deficiency had severe obesity and increased waist circumference (P = 0.012); they were also slightly younger at recruitment (Table 1 and Fig. 1a). A trend toward lower total cholesterol was observed, consistent with findings from larger clinical case series of individuals with MC4R deficiency and from MC4R mutation carriers in the UK Biobank population cohort (accompanying paper, Zorn et al.22). Otherwise, the clinical characteristics of carriers of MC4R mutations and noncarriers were broadly similar (Table 1 and Extended Data Table 2).

a, The distribution of BMI at baseline for MC4R mutation carriers and noncarriers. b, Least-squares mean estimands of the percentage change in body weight from baseline to week 72, with error bars representing 95% confidence intervals (CI). Genetic effects on change in body weight were assessed using aggregated data on carriers of 14 MC4R LoF mutations (beta coefficient −0.88, SEM 3.2); statistical significance was assessed using a REGENIE collapsed burden test incorporating the treatment interaction effect (unadjusted two-sided P value 0.79). c, Time course effect on body weight change. Least-squares mean estimands were generated for each time point based on a three-way interaction among MC4R carrier status, pooled treatment and visit. Blue and gray bars represent tirzepatide treatment and placebo arms, respectively, with error bars representing 95% CI.
We compared the weight loss trajectory at 72 weeks in the 32 MC4R mutation carriers and 2,259 noncarriers. People with MC4R deficiency responded to tirzepatide similarly to those with a normal MC4R genotype, demonstrating the effectiveness of tirzepatide in this subgroup of people with obesity (Fig. 1b,c). Furthermore, there was no differential impact of treatment (versus placebo) on metabolic parameters in MC4R mutation carriers versus noncarriers (Extended Data Table 3). All the MC4R mutation carriers in the placebo-treated group were female (Extended Data Table 2). This probably represents a chance occurrence given the rarity of MC4R deficiency and the fact that the SURMOUNT-1 cohort recruited twice as many females as males (males 825, females 1,714, total 2,539).
These results suggest that tirzepatide may be an effective treatment option for the most common form of monogenic obesity, MC4R deficiency. Given the severity of obesity in mutation carriers, equitable access to obesity medications should be a priority for this group, in whom diet and exercise interventions are unlikely to be effective. Roux-en-Y bypass surgery is effective in carriers of heterozygous but not homozygous mutations in MC4R, suggesting that central melanocortin circuits mediate some of the effects of bariatric surgery23. In a case report, a homozygous MC4R mutation carrier not responding to RYGB surgery was found to respond to GLP-1 receptor agonist treatment24.
Ongoing studies of the safety and efficacy of chronic treatment with obesity medications will be important for the management of patients with MC4R deficiency and other clinical groups. As MC4R deficiency presents with severe obesity from childhood, trials of tirzepatide (NCT06439277 and NCT06075667) and other obesity medications in children and adolescents with obesity, including those with MC4R deficiency, are needed to provide the evidence base for earlier, and potentially chronic, treatment in genetically driven obesity.
Methods
Study cohort (SURMOUNT-1 clinical trial)
Ethical approval and study populations
The study was conducted in accordance with the principles of the Declaration of Helsinki, Good Clinical Practice guidelines and all applicable regulatory requirements Study protocol and informed consent documents were approved by independent ethics committees and institutional review boards at all participating trial sites. Trial site investigators obtained consent, recruited participants, collected data and adhered to ethical standards. The sponsor conducted centralized monitoring with strict ethical oversight.
Genotyping
DNA was extracted from whole blood samples from participants enrolled in the SURMOUNT-1 trial (supported by Eli Lilly and Company.; ClinicalTrials.gov number NCT04184622) who consented to genetic analyses. Samples were quantified using a Quant-iT PicoGreen dsDNA assay to measure the DNA concentration. Samples were genotyped using the customized Axiom Biobank genotyping array (version 3) from Affymetrix. The array was customized using an Affymetrix UK BioBank backbone and incorporated all known genetic variants associated with genes or pathways related to various pathophysiological manifestations of obesity and related complications. A total of 2,474 patient samples along with duplicates and HapMap controls were genotyped, and data on 726,107 variants were generated. Standard metrics for genome-wide level data quality control were applied. After excluding variants with a call rate below 95% (n = 1,931), discordant variants in duplicate samples (n = 493) and monomorphic variants (n = 77,179), 646,504 variants and 2,291 samples passed quality control screening.
Statistical methods and details
Mixed-model repeated-measures weight loss imputation
A mixed model was run using SAS, including baseline weight, country, sex, prediabetes status, treatment, visit and the treatment-by-visit interaction as fixed effects, with a subject-level random effect. Any visits that did not have a recorded weight value were imputed as the predicted value from the mixed effect model. The value for the imputed weight percentage change from baseline was computed as (Predicted − Baseline) × 100/Baseline for all imputed visits. To ensure enough visits for imputation, we used only participants with a visit at week 24 or later (n = 2,291).
Genetic analysis
REGENIE was used to perform statistical association analyses for gene-level and single mutation-level testing25. For both models, the imputed weight loss percentage change from baseline at week 72 was used as the outcome. The model tested for genetic interaction with pooled treatment (collapsed 5, 10 and 15 mg treatment groups versus placebo), adjusting for age, sex, study country, baseline weight, prediabetes status and the first ten principal components.
Default settings were used in REGENIE genotypic data preparation and testing. For gene-level MC4R carrier testing, 14 LoF mutations were used to define the MC4R mask for collapsed burden testing, which measures the genotype–treatment interaction effect.
Mixed-model repeated-measures least-square means
A mixed-effects model for the imputed weight outcome at week 72 was created, including the same fixed covariates as in the genetic analysis, as well as visit, and a subject-level random effect. The least-square means estimands were generated for the three-way interaction for MC4R carrier status, pooled treatment (collapsed 5, 10 and 15 mg treatment groups versus placebo) and visit. Week 72 visit estimands were plotted to visualize the single-time-point treatment and MC4R LoF carrier interaction effect (Fig. 1b), while estimands from all available visits were plotted over time to illustrate the visit interaction effect (Fig. 1c).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The trial sponsor (Eli Lilly and Company) participated in the design and execution of the study, as well as collection, management, analysis and interpretation of the data. Patient-related information was anonymized and collected as part of the SURMOUNT-1 clinical trial and will be subject to confidentiality restrictions. Primary reasons for controlled access of this data are participant confidentiality and ethical compliance. Request for data access can be submitted via Vivli, and expected time for response is around 60 days.
References
Kusminski, C. M. et al. Transforming obesity: the advancement of multi-receptor drugs. Cell 187, 3829–3853 (2024).
Jastreboff, A. M. et al. Tirzepatide once weekly for the treatment of obesity. N. Engl. J. Med. 387, 205–216 (2022).
Frías, J. P. et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N. Engl. J. Med. 385, 503–515 (2021).
van der Klaauw, A. A. & Farooqi, I. S. The hunger genes: pathways to obesity. Cell 161, 119–132 (2015).
Khera, A. V. et al. Polygenic prediction of weight and obesity trajectories from birth to adulthood. Cell 177, 587–596 (2019).
Anderson, E. J. P. et al. 60 years of POMC: regulation of feeding and energy homeostasis by α-MSH. J. Mol. Endocrinol. 56, T157–T174 (2016).
Farooqi, I. S. et al. Clinical spectrum of obesity and mutations in the melanocortin 4 receptor gene. N. Engl. J. Med. 348, 1085–1095 (2003).
Brouwers, B. et al. Human MC4R variants affect endocytosis, trafficking and dimerization revealing multiple cellular mechanisms involved in weight regulation. Cell Rep. 34, 108862 (2021).
Turcot, V. et al. Protein-altering variants associated with body mass index implicate pathways that control energy intake and expenditure in obesity. Nat. Genet. 50, 26–41 (2018).
Wade, K. H. et al. Loss-of-function mutations in the melanocortin 4 receptor in a UK birth cohort. Nat. Med. 27, 1088–1096 (2021).
Trier, C. et al. Obesity treatment effect in Danish children and adolescents carrying melanocortin-4 receptor mutations. Int J. Obes. 45, 66–76 (2021).
Martinelli, C. E. et al. Obesity due to melanocortin 4 receptor (MC4R) deficiency is associated with increased linear growth and final height, fasting hyperinsulinemia, and incompletely suppressed growth hormone secretion. J. Clin. Endocrinol. Metab. 96, E181–E188 (2011).
Iepsen, E. W. et al. Adults with pathogenic MC4R mutations have increased final height and thereby increased bone mass. J. Bone Min. Metab. 38, 117–125 (2020).
Sayk, F. et al. Sympathetic function in human carriers of melanocortin-4 receptor gene mutations. J. Clin. Endocrinol. Metab. 95, 1998–2002 (2010).
Greenfield, J. R. et al. Modulation of blood pressure by central melanocortinergic pathways. N. Engl. J. Med. 360, 44–52 (2009).
Reinehr, T. et al. Lifestyle intervention in obese children with variations in the melanocortin 4 receptor gene. Obesity 17, 382–389 (2009).
Collet, T.-H. et al. Evaluation of a melanocortin-4 receptor (MC4R) agonist (Setmelanotide) in MC4R deficiency. Mol. Metab. 6, 1321–1329 (2017).
René, P. et al. Pharmacological chaperones restore function to MC4R mutants responsible for severe early-onset obesity. J. Pharmacol. Exp. Ther. 335, 520–532 (2010).
Clemmensen, C. et al. Dual melanocortin-4 receptor and GLP-1 receptor agonism amplifies metabolic benefits in diet-induced obese mice. EMBO Mol. Med. 7, 288–298 (2015).
Iepsen, E. W. et al. Patients with obesity caused by melanocortin-4 receptor mutations can be treated with a glucagon-like peptide-1 receptor agonist. Cell Metab. 28, 23–32 (2018).
Lotta, L. A. et al. Human gain-of-function MC4R variants show signaling bias and protect against obesity. Cell 177, 597–607 (2019).
Zorn, S. et al. Obesity due to MC4R deficiency is associated with reduced cholesterol, triglycerides and cardiovascular disease risk. Nat. Med. (in the press).
Hatoum, I. J. et al. Melanocortin-4 receptor signaling is required for weight loss after gastric bypass surgery. J. Clin. Endocrinol. Metab. 97, E1023–E1031 (2012).
Iepsen, E. W. et al. GLP-1 receptor agonist treatment in morbid obesity and type 2 diabetes due to pathogenic homozygous melanocortin-4 receptor mutation: a case report. Cell Rep. Med. 1, 100006 (2020).
Mbatchou, J. et al. Computationally efficient whole-genome regression for quantitative and binary traits. Nat. Genet. 53, 1097–1103 (2021).
Acknowledgements
I.S.F. is supported by Wellcome (207462/Z/17/Z), Botnar Fondation, the Bernard Wolfe Health Neuroscience Endowment and a NIHR Senior Investigator Award. The funding bodies had no role in the design or conduct of the study; collection, management, analysis or interpretation of the data; preparation, review or approval of the manuscript; or the decision to submit the manuscript for publication. The views expressed are those of the authors and not necessarily those of the NIHR, the Department of Health and Social Care or the UK government. Eli Lilly and Company was the sponsor of this study. We thank the patients who consented to participate in the SURMOUNT-1 study. We also thank K. M. Kelly for assisting in internal approval processes and informed consent document review, and D. W. Bedwell for coordinating with the contract research organization for sample shipments, genotyping and secure data transfer.
Author information
Authors and Affiliations
Contributions
I.S.F. and P.B. conceptualized the project, analyzed the data, interpreted the results and drafted the manuscript. N.N.A provided clinical guidance, facilitated access to the data and assisted in securing funding for the study. N.N.A. and M.C. contributed to formalizing study plans, data analyses and interpretation. X.L. offered operational support to execute the analyses and secure timely delivery of the results. L.M.K. provided critical review of the results and interpretation. All authors reviewed the manuscript for accuracy, edited subsequent revisions of the draft and approved the final paper.
Corresponding author
Ethics declarations
Competing interests
I.S.F. has consulted for Eli Lilly, Novo Nordisk, Sanofi, Nodthera Therapeutics and Rhythm Pharmaceuticals on anti-obesity medications. L.M.K. is a scientific and/or medical consultant to Altimmune, Amgen, Boehringer Ingelheim, Cytoki, Gilead, Johnson & Johnson, Kallyope, Eli Lilly and Company, Novo Nordisk, Optum, Perspectum, Pfizer, Xeno Biosciences and Zealand. N.N.A., M.C., X.L. and P.B. are employees and shareholders of Eli Lilly and Company.
Peer review
Peer review information
Nature Medicine thanks Anke Hinney, Edra London and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editors: Ashley Castellanos-Jankiewicz and Sonia Muliyil, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bhatnagar, P., Ahmad, N.N., Li, X. et al. Tirzepatide leads to weight reduction in people with obesity due to MC4R deficiency. Nat Med 31, 3294–3296 (2025). https://doi.org/10.1038/s41591-025-03913-2
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41591-025-03913-2
This article is cited by
-
Monogenic obesity due to MC4R deficiency: lessons from a multigenerational case
Molecular and Cellular Pediatrics (2026)
-
Obesity due to MC4R deficiency is associated with reduced cholesterol, triglycerides and cardiovascular disease risk
Nature Medicine (2025)
