
Abstract
This study aims to investigate the impact of cerebral white matter lesions (CWMLs) on auditory, speech, and non-verbal cognitive (NVC) outcomes following cochlear implantation (CI) in children with prelingually sensorineural deafness (PLSND) and to identify prognostic factors for these domains. This province-wide retrospective cohort study included PLSND patients with CWMLs undergoing CI, employing propensity score matching for control. Participants were categorized into four groups based on CWMLs severity for auditory, speech, and NVC assessments at various post-CI intervals. Mixed models were used to analyze prognostic factors. In a cohort of 1163 children with PLSND, 15% exhibited CWMLs. CWMLs patients exhibited poorer pre-CI auditory and reduced post-implantation outcomes, correlated with lesion severity. Recovery patterns varied (auditory: rapid-slow; speech: slow-rapid-slow; NVC: rapid-stable), with speech recovery trailing auditory recovery. Greater severity of CWMLs and elevated pre-CI hearing thresholds are risk factors for poorer post-CI auditory and speech outcomes. Conversely, higher income, enhanced pre-CI auditory and NVC capabilities, prolonged rehabilitation, and cesarean delivery are protective factors for these outcomes. Greater severity of CWMLs served as an independent risk factor for post-CI NVC, while cesarean delivery, strong pre-CI speech capabilities, and Advanced Bionics CI device emerged as independent protective factors. This study highlights the importance of incorporating CWMLs severity, perinatal history, and clinical characteristics into preoperative assessments to refine CI candidacy criteria. The identified recovery patterns further guide personalized rehabilitation strategies, contributing to improved long-term outcomes in children with PLSND.
Similar content being viewed by others
Introduction
Speech development is a critical milestone in early childhood, particularly before the age of three. Prelingual sensorineural deafness (PLSND), which occurs due to hearing loss during this crucial period, affects approximately one in every 1,000 children globally1. Without early auditory stimulation, children with PLSND face significant challenges in auditory, speech, and non-verbal cognitive (NVC) development compared to those with postlingual deafness2,3. These difficulties often extend to emotional and social domains, significantly reducing quality of life4,5.
Cochlear implantation (CI) remains the primary intervention for restoring hearing in these children, requiring detailed radiological assessment before surgery. Advances in medical imaging, particularly cranial magnetic resonance imaging (MRI), have improved the detection of brain abnormalities in hearing-impaired children. Among these abnormalities, CWMLs are notably common and are often linked to perinatal brain injuries or structural remodeling induced by hearing loss6,7,8,9. CWMLs may disrupt neural signal conduction, potentially affecting auditory, speech, and NVC outcomes. However, the impact of CWMLs on rehabilitation outcomes following CI remains controversial. For example, Luthra et al. reported that children with PLSND and CWMLs showed varying degrees of auditory and speech impairments after CI10, whereas Shen et al. found no significant differences in outcomes regardless of CWML presence11. These conflicting results underscore the need for further research to clarify the role of CWMLs in CI outcomes.
The conflicting results in existing studies highlight several limitations, such as small sample sizes, short follow-up periods, failure to address confounding factors, and the lack of a standardized approach to assess CWML severity. Notably, NVC, a critical component of rehabilitation, has received limited attention. NVC development varies significantly across age groups, and the absence of a unified assessment tool has hindered its precise evaluation in children with PLSND and CWMLs.
To address these gaps, our study adopts a multicenter retrospective cohort design to expand the sample size and extend follow-up durations. For the first time, we utilize propensity score matching to balance diverse confounding factors(e.g., perinatal history, age at implantation, duration of preimplantation hearing aid use, and socioeconomic status, etc.), improving the comparability between children with and without CWMLs. CWML severity is assessed using the comprehensive Scheltens scale, enabling subgroup analysis. Additionally, we employ a standardized Z score to integrate NVC assessments across different age groups, providing a unified evaluation framework. Using cumulative link mixed models and linear mixed models, we further explore prognostic factors for auditory, speech, and NVC outcomes following CI in children with PLSND and CWMLs. These methodological innovations aim to provide robust evidence for evaluating the effects of CWMLs on rehabilitation outcomes and to support clinical decision-making for this unique population.
This study aims to address the following key questions: (1) Does the presence and severity of CWMLs impact the long-term auditory, speech, and NVC rehabilitation outcomes following CI? (2) What prognostic factors influence auditory, speech, and NVC outcomes following CI in children with PLSND and CWMLs?
Results
Demographics and clinical characteristics of the study population
In a cohort of 1163 PLSND patients treated with CI 56.9% (662) were male, with a median implantation age of 41(interquartile range 29–62) months. CWMLs were observed in 15% (175) of cases. Perinatal history included toxic substance exposure (4 cases, 0.3%), trauma (5 cases, 0.4%), noise exposure (11 cases, 0.9%), infection (41 cases, 3.5%), medication (40 cases, 3.4%), hypoxia (44 cases, 3.8%), cesarean delivery (564 cases, 48.5%), preterm birth (51 cases, 4.4%), and low birth weight (79 cases, 6.8%). The median durations for preoperative hearing aid use and rehabilitation were 19 months and 10 months, respectively. Preoperative audiometry showed median unaided, aided, and ASSR hearing thresholds in the better ear of 114 dB HL, 93.75 dB HL, and 107.75 dB HL, respectively. The types of devices implanted were Cochlear (555 cases, 47.7%), MED-EL (374 cases, 32.2%), Advanced Bionics (205 cases, 17.6%), and NUROTRON (27 cases, 2.3%) (see Supplementary Table S1 online).
These data comprehensively summarize the characteristics of the study population, including socioeconomic status predominantly from low- to middle-income families and a male-dominated gender distribution, with a high prevalence of certain perinatal risk factors. The population also exhibited severe preoperative hearing loss, prolonged preoperative hearing aid use, shorter preoperative rehabilitation durations, and diverse rehabilitation center distribution. Additionally, cochlear implantation was generally delayed, with Cochlear-brand devices being the most commonly used. The proportion of cerebral white matter lesions among implanted children was 15%.
Characteristics of the CWMLs patients
In 175 PLSND children with CWMLs, the median Scheltens score was 6 (range 2–12). At six-month follow-up, 2 cases showed reduced severity (from 16 to 12 and 3 to 1), and 2 normalized (from 2 to 0). CWMLs were divided into mild (range 2–2), moderate (range 6–8), and severe (range 12–16) subgroups based on tertiles (Fig. 1b; Table 1).
Overall, these findings describe the distribution of CWMLs severity in the study population, with most cases showing no significant changes in severity over the follow-up period and only a small proportion (2.3%) exhibiting improvement.

Study design flowchart and distribution of Scheltens scores in PLSND patients with CWMLs. (a) Overview of the study design and analysis workflow. (b) Violin plot illustrating the distribution of Scheltens scores across CWMLs patients with varying severity levels, showing median, interquartile range, and overall distribution. Significant differences were observed between the mild, moderate, and severe groups. CWMLs, cerebral white matter lesions; PLSND, prelingual sensorineural deafness. *p < 0.05, **p < 0.01, ***p < 0.001.
Comparison of clinical characteristics between the CWMLs group and the control group before propensity score matching
The pre-propensity score matching analysis revealed no significant differences in gender ratio or median family income between the CWMLs and control groups. Nevertheless, the CWMLs group exhibited higher incidences of perinatal infections (6.9% vs. 2.9%) and low birth weight (12.0% vs. 5.9%) than the controls. Moreover, the CWMLs group had higher pre-implantation unaided and aided hearing thresholds in the better ear by approximately 3 dB HL (116.88 vs. 114.00) and 2 dB HL (96.00 vs. 93.75), respectively. The implantation age was also higher in the CWMLs group (44 vs. 40 months). No differences in device type were observed between the groups, yet significant variations were noted in the implanting hospitals and rehabilitation institutions (Table 1).
These findings indicate that before propensity score matching, the CWMLs group had higher rates of perinatal infections and low birth weight, poorer auditory thresholds, older implantation age, and differences in the distribution of implanting centers and rehabilitation institutions, while other characteristics showed no significant differences.
Comparison of clinical characteristics between the CWMLs group and the control group after propensity score matching
Propensity score matching matched 175 case pairs, minimizing baseline differences between CWMLs and control groups. After adjusting for 17 confounders, the pre-implantation unaided hearing threshold in the better ear of the CWMLs group was still higher (116.88 vs. 113.75), yet no significant differences were observed in the aided thresholds across groups. Moreover, differences in perinatal infections, low birth weight, CI centers, and rehabilitation institutions between the groups were eliminated following matching (Table 2). The data indicate that, after propensity score matching, the pre-implantation unaided hearing threshold in the better ear was significantly higher in the CWMLs group, while other baseline characteristics showed no significant differences.
Auditory performance evaluation
Preoperative assessments indicated no significant difference in the Categories of Auditory Performance (CAP) scores between the CWMLs and control groups (0.97 ± 0.04 vs. 1.03 ± 0.03). However, at 6, 12, and 18 months post-activation, the CWMLs group exhibited significantly lower CAP scores compared to the controls (2.73 ± 0.06 vs. 3.17 ± 0.04, 3.89 ± 0.07 vs. 4.19 ± 0.04, 4.62 ± 0.06 vs. 4.80 ± 0.05, respectively; all p < 0.05). Differences in CAP scores between the groups disappeared from 2 years post-activation onwards. (Fig. 2a). In summary, the results show that while preoperative CAP scores were comparable between groups, the CWMLs group exhibited significantly lower CAP scores in the short term following activation, but these differences were no longer apparent in the long term.

The impact of CWMLs on auditory, speech, and NVC outcomes in children with PLSND. (a), (b), and (c) depict the comparison of preoperative and post-activation CAP, SIR, and Z scores, respectively, in the overall CWMLs group versus the control group. Significant differences in CAP scores between the two groups were observed from 6 to 18 months post-activation, with the differences disappearing after 2 years. For SIR scores, significant differences persisted from 6 to 36 months post-activation, disappearing at 30 months. Z scores showed significant differences between the two groups from 6 to 24 months post-activation. The recovery patterns were independent of the presence of cerebral white matter lesions (auditory: rapid-slow; speech: slow-rapid-slow; NVC: rapid-stable), with speech recovery lagging behind auditory recovery. (d), (e), and (f) illustrate the same comparisons within subgroups of the CWMLs patients. The significant differences were primarily concentrated between the severe CWMLs group and the control group. (g), (h), and (i) show a negative correlation between CAP, SIR, and Z scores and Scheltens scores in CWMLs patients. CWMLs, cerebral white matter lesions; NVC, non-verbal cognition; PLSND, prelingual sensorineural deafness; CAP, Categories of Auditory Performance; SIR, Speech Intelligibility Rating. *p < 0.05, **p < 0.01, ***p < 0.001 vs. control group.
Subgroup analyses by CWMLs severity uncovered overall significant differences in CAP scores at each assessment point (Pre H = 16.87, p < 0.001; 6 M H = 144.93, p < 0.001; 1Y H = 63.93, p < 0.001; 18 M H = 10.81, p < 0.05; 2Y H = 15.76, p < 0.001; 30 M H = 7.98, p < 0.05; 3Y H = 9.64, p < 0.05). Pairwise comparisons showed that the severe CWMLs group consistently had lower CAP scores than controls across all time points (Pre H = 31.47, p < 0.01; 6 M H = 151.02, p < 0.001; 1Y H = 96.29, p < 0.001; 18 M H = 43.84, p < 0.01; 2Y H = 41.28, p < 0.01; 30 M H = 38.73, p < 0.05; 3Y H = 41.99, p < 0.05). The mild and moderate CWMLs groups had comparable CAP scores to the control group at all time points (Fig. 2d). These findings demonstrate that CAP scores differed significantly across CWMLs severity subgroups, with the severe group consistently scoring lower than the control group. Additionally, a negative correlation existed between CAP and Scheltens scores, with varying coefficients over time: preoperative (− 0.27), 6 M (− 0.69), 12 M (− 0.46), 18 M (− 0.30), 24 M (− 0.25), 30 M (− 0.32), and 36 M (− 0.36) (Fig. 2g).
Speech performance evaluation
The preoperative Speech Intelligibility Rating (SIR) scores revealed no significant difference between CWMLs and control groups (1.05 ± 0.02 vs. 1.07 ± 0.03). However, at 6, 12, 18, and 24 months post-activation, the SIR scores of the CWMLs group were significantly lower than those of the control group (1.61 vs. 1.76, 2.11 vs. 2.28, 2.89 vs. 3.07, and 3.16 vs. 3.38 respectively). From 30 months post-activation onwards, SIR score differences between groups ceased to be significant (Fig. 2b). Overall, while preoperative SIR scores were comparable between the two groups, the CWMLs group exhibited significantly lower SIR scores than the control group in the short-to-medium term following activation; however, these differences diminished over time.
Subgroup analysis revealed no overall significant preoperative differences in SIR scores. However, significant differences emerged at all postoperative intervals (6 M H = 16.52, p < 0.001; 1Y H = 20.85, p < 0.001; 18 M H = 52.51, p < 0.001; 2Y H = 15.68, p < 0.001; 30 M H = 22.89, p < 0.001; 3Y H = 12.48, p < 0.01). Paired comparisons revealed no significant preoperative differences in SIR scores between the severe CWMLs and control groups. Postoperatively, the severe CWMLs group exhibited consistently lower SIR scores than the controls at all time points (6 M H = 53.98, p < 0.01; 1Y H = 52.31, p < 0.001; 18 M H = 75.78, p < 0.001; 2Y H = 44.26, p < 0.01; 30 M H = 56.52, p < 0.001; 3Y H = 45.71, p < 0.01). The mild and moderate CWMLs groups exhibited no significant differences in SIR scores compared to the control group at any assessment point (Fig. 2e). These results highlight the fact that postoperative SIR scores differed significantly across CWMLs severity subgroups, with the severe group consistently exhibiting poorer speech performance compared to the control group. Furthermore, an inverse correlation between SIR and Scheltens scores was noted, with coefficients changing over time: preoperative (− 0.13), 6 M (− 0.27), 12 M (− 0.34), 18 M (− 0.43), 24 M (− 0.26), 30 M (− 0. 0.41), and 36 M (− 0. 39) (Fig. 2h).
Non-verbal cognitive evaluation
Preoperatively, the CWMLs group exhibited significantly lower NVC Z scores than the control group (− 0.59 ± 0.08 vs. − 0.17 ± 0.05). Postoperatively, the CWMLs group’s NVC Z scores continued to be significantly lower than those of the control group at all assessed time points (1Y − 0.08 ± 0.03 vs. 0.06 ± 0.02; 2Y − 0.03 ± 0.03 vs. 0.12 ± 0.03; 3Y − 0.05 ± 0.02 vs. 0.04 ± 0.02) (Fig. 2c). The data indicate that the CWMLs group had significantly lower NVC Z scores than the control group both preoperatively and at all postoperative assessment points.
Subgroup analysis revealed overall significant Z score differences at all assessment times (Pre H = 71.50, p < 0.001; 1Y H = 77.93, p < 0.001; 2Y H = 38.72, p < 0.001; 3Y H = 90.97, p < 0.001). Pairwise comparisons showed the CWMLs group’s Z scores were consistently lower than those of the control group at each time point (Pre H = 122.01, p < 0.001; 1Y H = 130.52, p < 0.001; 2Y H = 88.84, p < 0.001; 3Y H = 128.15, p < 0.001). For the moderate CWMLs group, preoperative and at 1 and 3 years post-activation, Z scores were significantly lower than those of the control group, with no differences noted at 2 years (Pre H = 70.27, p < 0.001; 1Y H = 55.32, p < 0.01; 3Y H = 64.64, p < 0.001). No significant Z score differences were observed between the mild CWMLs and control groups at any time point (Fig. 2f). From these results, it can be observed that the overall group differences in NVC Z scores were primarily driven by lower scores in the severe and, to a lesser extent, moderate CWMLs subgroups. Additionally, an inverse correlation between the Z score and Scheltens score was observed, with coefficients at preoperative, 12, 24, and 36 months post-activation of − 0.40, − 0.49, − 0.39, and − 0.59, respectively (Fig. 2i).
Prognostic factors for auditory performance
A cumulative link mixed model was employed to investigate the prognostic factors of post-CI CAP score. Univariate analysis identified 11 potential prognostic factors, including household per capita annual income, aided sound field thresholds in the better ear, duration of preimplantation hearing aid use, age at implantation, preimplantation Z score, Scheltens score, preimplantation CAP score, preimplantation SIR score, evaluation time (rehabilitation duration), cesarean section, and rehabilitation facility (Fig. 3). These variables were subsequently entered into a multivariate analysis, with backward elimination through Likelihood Ratio (LR) testing, resulting in a final model comprising seven variables: household per capita annual income, aided sound field thresholds in the better ear, preimplantation Z score, Scheltens score, preimplantation CAP score, evaluation time(rehabilitation duration), and cesarean section. The final model identified aided sound field thresholds in the better ear and Scheltens score as independent risk factors for CAP score prognosis (β < 0). In contrast, household per capita annual income, preimplantation Z score, preimplantation CAP score, evaluation time(rehabilitation duration), and cesarean section were identified as independent protective factors for CAP score prognosis (β > 0) (Fig. 4a). Notably, no significant interaction effects between the predictors were identified during the evaluation process, and no interaction terms were included in the final model.

Univariate analysis of the CLMM for CAP score in PLSND children with CWMLs. Univariate analysis identified 11 potential prognostic factors, including household per capita annual income, aided sound field thresholds in the better ear, duration of preimplantation hearing aid use, age at implantation, preimplantation Z score, Scheltens score, preimplantation CAP score, preimplantation SIR score, evaluation time (rehabilitation duration), cesarean section, and rehabilitation facility. The dark blue variables to the left of the zero line represent candidate risk factors, while the dark red variables to the right of the zero line represent candidate protective factors. β, the regression coefficient; .L, the linear term of this ordinal variable; ASSR, auditory steady-state response; CAP, Categories of Auditory Performance; SIR, Speech Intelligibility Rating; C1–C4, cochlear implantation center pseudonyms; R1-R10, rehabilitation facility pseudonyms. CLMM, cumulative link mixed models; PLSND, prelingual sensorineural deafness; CWMLs, cerebral white matter lesions. ˙p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.

Multivariate analysis for CAP, SIR, and NVC Z scores in PLSND children with CWMLs. (a) and (b) depict the multivariate analysis using the CLMM for CAP and SIR scores, respectively. The CAP score and SIR score share the same seven prognostic factors, including household per capita annual income, aided sound field thresholds in the better ear, preimplantation Z score, Scheltens score, preimplantation CAP score, evaluation time(rehabilitation duration), and cesarean section. (c) shows the analysis using the LMM for NVC Z score in the CWMLs group. Multivariate analysis identified four prognostic factors, including Scheltens score, preoperative SIR score, cesarean section, and CI device. The dark blue variables to the left of the zero line represent risk factors, while the dark red variables to the right of the zero line represent protective factors. β, the regression coefficient; .L, the linear term of this ordinal variable; CAP, Categories of Auditory Performance; SIR, Speech Intelligibility Rating. CLMM, cumulative link mixed models; LMM, Linear mixed model; NVC, non-verbal cognition; PLSND, prelingual sensorineural deafness; CWMLs, cerebral white matter lesions. ˙p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.
Sensitivity analysis results indicated that the four models exhibited similar effect sizes (β), confidence intervals, and statistical significance across seven common variables, demonstrating consistency among the results of different models (see Supplementary Fig. S1 online). The Final model adjusted for the seven variables identified in the previous paragraph. Model 1 additionally accounted for the Rehabilitation facility, Model 2 further included the Cochlear implantation center, and Model 3 simultaneously added adjustments for both the Rehabilitation facility and the Cochlear implantation center. The marginal R² of the four cumulative link mixed models was 86.9%, 87.4%, 87.0%, and 87.5%, respectively, while the conditional R² was consistently 91.9% for all models. The likelihood ratio test results showed no significant differences (Model 1 vs. Final model, ANOVA Pr (> Chisq) = 0.14; Model 2 vs. Final model, ANOVA Pr (> Chisq) = 0.27; Model 3 vs. Final model, ANOVA Pr (> Chisq) = 0.17), indicating that these models have similar predictive accuracy (see Supplementary Table S2 online). No significant differences were observed between these models, further confirming the robustness of the model results.
Prognostic factors for speech performance
A cumulative link mixed model was used to investigate the prognostic factors affecting the post-CI SIR score. Twelve candidate prognostic factors were identified through univariate analysis, including household per capita annual income, aided sound field thresholds in the better ear, duration of preimplantation hearing aid use, age at implantation, preimplantation Z score, Scheltens score, preimplantation CAP score, preimplantation SIR score, evaluation time, cesarean section, cochlear implant device, and rehabilitation facility (Fig. 5). These variables were then included in a multivariate analysis using the LR test with backward elimination, which resulted in a final model comprising seven variables: household per capita annual income, aided sound field thresholds in the better ear, preimplantation Z score, Scheltens score, preimplantation CAP score, evaluation time(rehabilitation duration), and cesarean section. In the final model, aided sound field thresholds in the better ear and Scheltens score were identified as independent risk factors for SIR score prognosis (β < 0), while household per capita annual income, preimplantation Z score, preimplantation CAP score, evaluation time(rehabilitation duration), and cesarean section were identified as independent protective factors for SIR score prognosis (β > 0) (Fig. 4b). Notably, no significant interaction effects between the predictors were identified during the evaluation process, and no interaction terms were included in the final model.

Univariate analysis of the CLMM for SIR score in PLSND children with CWMLs. Univariate analysis identified 12 potential prognostic factors, including household per capita annual income, aided sound field thresholds in the better ear, duration of preimplantation hearing aid use, age at implantation, preimplantation Z score, Scheltens score, preimplantation CAP score, preimplantation SIR score, evaluation time (rehabilitation duration), cesarean section, cochlear implant device, and rehabilitation facility. The dark blue variables to the left of the zero line represent candidate risk factors, while the dark red variables to the right of the zero line represent candidate protective factors. β, the regression coefficient; .L, the linear term of this ordinal variable; ASSR, auditory steady-state response; CAP, Categories of Auditory Performance; SIR, Speech Intelligibility Rating; C1–C4, cochlear implantation center pseudonyms; R1-R10, rehabilitation facility pseudonyms. CLMM, cumulative link mixed models; PLSND, prelingual sensorineural deafness; CWMLs, cerebral white matter lesions. ˙p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.
Sensitivity analysis results indicated that the four models exhibited similar effect sizes (β), confidence intervals, and statistical significance across seven common variables, demonstrating consistency among the results of different models (see Supplementary Fig. S2 online). The Final model accounted for the seven variables outlined in the previous paragraph. Model 1 additionally incorporated the Rehabilitation facility, Model 2 further included the Cochlear implantation center, and Model 3 simultaneously added adjustments for both the Rehabilitation facility and the Cochlear implantation center. The marginal R² of the four cumulative link mixed models was 86.7%, 87.4%, 86.9%, and 87.5%, respectively, while the conditional R² was consistently 93.1% for all models. The likelihood ratio test results indicated no significant differences (Model 1 vs. Final model, ANOVA Pr (> Chisq) = 0.07; Model 2 vs. Final model, ANOVA Pr (> Chisq) = 0.29; Model 3 vs. Final model, ANOVA Pr (> Chisq) = 0.12), suggesting that these models have similar predictive accuracy (see Supplementary Table S3 online). No significant differences were observed among these models, further confirming the robustness of the model results.
Prognostic factors for non-verbal cognitive
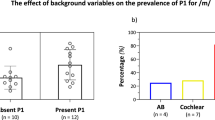
An linear mixed model was used to investigate NVC Z score prognostic factors. Initial univariate analysis identified eight prognostic factors: Scheltens score, preoperative SIR score, cesarean section, CI device, preoperative Z score, assessment time, CI center, and rehabilitation facility (Fig. 6). Subsequent multivariate analysis and backward elimination through the Likelihood Ratio (LR) test distilled these to a final model comprising four variables: Scheltens score, preoperative SIR score, cesarean section, and CI device. The final model identified Scheltens score as an independent risk factor (β < 0), and the SIR score, cesarean section, and CI device (Advanced Bionics) as protective factors (β > 0) for NVC Z score prognosis (Fig. 4c). Notably, no significant interaction effects between the predictors were identified during the evaluation process, and no interaction terms were included in the final model.

Univariate analysis of the LMM for NVC Z score in PLSND children with CWMLs. Univariate analysis identified 12 potential prognostic factors, including Scheltens score, preoperative SIR score, cesarean section, CI device, preoperative Z score, assessment time (rehabilitation duration), CI center, and rehabilitation facility. The dark blue variables to the left of the zero line represent candidate risk factors, while the dark red variables to the right of the zero line represent candidate protective factors. β, the regression coefficient; .L, the linear term of this ordinal variable; .Q, the quadratic term of this ordinal variable; ASSR, auditory steady-state response; CAP, Categories of Auditory Performance; SIR, Speech Intelligibility Rating; C1–C4, cochlear implantation center pseudonyms; R1-R10, rehabilitation facility pseudonyms. LMM, linear mixed model; NVC, non-verbal cognition; PLSND, prelingual sensorineural deafness; CWMLs, cerebral white matter lesions. ˙p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.
Sensitivity analysis revealed consistent β, confidence intervals, and levels of statistical significance across five models for the Scheltens score, preoperative SIR score, cesarean section, and CI device (see Supplementary Fig. S3 online). The Final model adjusted for the four variables outlined in the previous paragraph. Model 1 additionally incorporated the Rehabilitation facility, Model 2 further included the Cochlear implantation center, Model 3 simultaneously added adjustments for both the Rehabilitation facility and the Cochlear implantation center, and Model 4, reconstructed using Generalized Estimating Equations (GEE), adjusted for the same four variables as the Final model. The root mean square error (RMSE) for the four linear mixed models was 25.1%, 25.3%, 25.2%, and 25.4%, respectively, with marginal R² values of 29.4%, 31.1%, 30.2%, and 32.2%, and a consistent conditional R² of 42.1% for all models. The likelihood ratio test showed no significant difference (Model 1 vs. Final model, ANOVA Pr (> Chisq) = 0.36; Model 2 vs. Final model, ANOVA Pr (> Chisq) = 0.19; Model 3 vs. Final model, ANOVA Pr (> Chisq) = 0.18), indicating similar predictive performance among these models. Compared to Model 4, the selected linear mixed model showed a similar RMSE, highlighting stable predictive accuracy despite structural differences (see Supplementary Table S4 online). The absence of significant differences reinforced the robustness of the models.
Discussion
This study comprehensively evaluated the impact of CWMLs on auditory, speech, and NVC outcomes following CI in children with PLSND and further investigated the factors influencing these postoperative outcomes in PLSND children with CWMLs. The key findings of this study are summarized as follows: (1) Approximately 15% of PLSND children were found to have CWMLs, with only 2% showing slight reduction in lesion severity upon preoperative follow-up. (2) Compared to non-CWMLs patients, those with CWMLs exhibited higher initial hearing thresholds preoperatively and poorer auditory, speech, and NVC performance post-CI. (3) The postoperative auditory, speech, and NVC outcomes of CWMLs patients were closely related to the severity of the lesions, with mild CWMLs patients able to achieve the same level of rehabilitation as non-CWMLs patients within three years, while those with severe CWMLs struggled to reach the same level within the same period. (4) Both CWMLs and non-CWMLs patients exhibited similar recovery patterns post-CI, indicating that the recovery trajectory is independent of CWMLs presence (auditory: rapid-slow; speech: slow-rapid-slow; NVC: rapid-stable), with speech recovery lagging behind auditory recovery. (5) Greater CWMLs severity and higher preoperative hearing thresholds were identified as risk factors for auditory and speech outcomes post-CI. In contrast, higher income, stronger preoperative auditory and NVC capabilities, longer rehabilitation duration, and cesarean delivery were protective factors for these outcomes. Additionally, greater CWMLs severity was an independent risk factor for NVC outcomes post-CI, whereas cesarean delivery, stronger preoperative speech abilities, and the use of Advanced Bionics CI devices were independent protective factors.
The relationship between CWMLs and PLSND
The underlying mechanisms linking CWMLs and PLSND remain unclear; however, growing evidence suggests that damage, degeneration, and remodeling of the white matter in the central nervous system may play a fundamental role. CWMLs and PLSND share several common etiological factors, including genetic, immune, and metabolic influences, as well as drug toxicity, infections, and perinatal brain injuries, which can lead to damage or degeneration of the white matter in the central nervous system, significantly contributing to the development of PLSND and potentially predisposing young children to CWMLs12,13. Additionally, when the damaged or degenerated white matter in CWMLs affects the neural pathways related to the central auditory system, it may result in central deafness, a manifestation of PLSND, while PLSND itself may induce remodeling of the brain’s white matter, as evidenced by reduced fractional anisotropy (FA) and the presence of CWMLs on MRI scans8,14,15.The complex interrelationships between CWMLs and PLSND indicate a strong correlation, with these conditions frequently co-occurring. Martinez-Biarge et al. suggested an association between CWMLs and an increased risk of PLSND16. Additionally, another study discovered that CWMLs frequently coexist with severe hearing loss17. Consistent with prior findings, our study found children with CWMLs exhibited significantly higher initial hearing thresholds preoperatively compared to those without lesions.
The impact of CWMLs on CI outcomes
Numerous studies have investigated the factors influencing CI outcomes in children with PLSND, revealing that a variety of variables significantly impact auditory and language development. Generally, children who undergo CI surgery at older ages exhibit less improvement in auditory and language abilities18,19. In contrast, children from families with higher socioeconomic status tend to achieve better speech and language acquisition postoperatively20. Additionally, patients who used hearing aids prior to CI surgery often demonstrate superior auditory outcomes following implantation21. However, factors such as perinatal infections, low birth weight, inner ear malformations, and intraoperative complications may limit the effectiveness of speech perception after CI surgery22. Recent research suggests that CWMLs may be a potential factor affecting CI outcomes in PLSND patients; however, evidence regarding their impact remains inconsistent10,13. Therefore, the effect of CWMLs on CI outcomes in PLSND patients warrants further investigation.
This study found that, prior to propensity score matching, the CWMLs group had a higher prevalence of perinatal infection histories, lower birth weights, and older implantation ages, which may be associated with their unique developmental and clinical characteristics. Lower birth weight typically reflects impaired intrauterine development, which is closely linked to white matter injury or delayed brain development, thereby increasing the risk of CWMLs23. Perinatal infections may trigger white matter damage through the release of non-infectious messengers via microbial colonization, further promoting the formation of CWMLs24. In addition, the older implantation age observed in CWMLs patients may be due to the clinical requirement of observing at least six months following initial diagnosis, along with follow-up MRI assessments to confirm lesion stability, which delays implantation timing. Although a difference of 3 dB and 2 dB HL was observed between the two groups of children, this difference falls within the test-retest reliability thresholds typically reported for audiological measurements. Such minimal differences likely have limited clinical significance, as small threshold variations would not substantially alter auditory perception or rehabilitation potential. These confounding factors suggest that direct comparison alone cannot establish CWMLs as independent prognostic factors for post-CI outcomes in PLSND. Consequently, we selected patients without CWMLs as controls and conducted 1:1 propensity score matching.
After propensity score matching, the statistical differences in perinatal infection history, birth weight, and implantation timing between the CWMLs group and the Control group disappeared, thereby eliminating the bias introduced by these factors. However, the overall late timing of implantation observed in both groups may universally limit the overall improvement in outcomes following CI. This general tendency toward delayed implantation could potentially hinder the optimal benefits of CI surgery. Post-matching, significant differences in auditory, speech, and NVC outcomes among CWMLs patients suggested these lesions as independent adverse prognostic factors for post-CI rehabilitation in PLSND. CI generally compensates and restores peripheral auditory functions effectively. However, CWMLs’ extension to central auditory, language processing, and cognitive areas may impair postoperative auditory, speech, and cognitive functions. The complexity of brain networks means that CWMLs’ extension to areas not directly related to auditory, speech, and cognitive functions can still negatively impact postoperative rehabilitation25. This may account for the observed declines in post-CI auditory, speech, and cognitive performance among patients with CWMLs in numerous studies.
This section’s findings align with the overall conclusions of previous studies, indicating that patients with CWMLs exhibit poorer postoperative recovery outcomes. However, unlike prior research, this study utilized the propensity score matching method to eliminate the confounding effects of perinatal characteristics, economic status, and preoperative rehabilitation duration. For the first time, it definitively identifies CWMLs as an independent risk factor. This discovery provides a critical foundation for more accurate prognostic evaluation of postoperative outcomes in patients with CWMLs. Furthermore, this study is the first to reveal that patients with CWMLs demonstrate significantly lower postoperative NVC performance compared to those without lesions, further underscoring the profound impact of CWMLs on central cognitive function.
The influence of CWMLs severity on CI outcomes and rehabilitation patterns
Identifying the most responsive CWMLs and PLSND patients to CI is crucial for optimizing implant benefits and facilitating the shift to personalized medicine. Therefore, we subdivided CWMLs patients into three severity-based groups for further analysis. All subgroups showed significant postoperative improvements in auditory, speech, and cognitive functions after standardized rehabilitation. Patients with mild and moderate CWMLs matched non-lesion peers in auditory and speech recovery within three years, but those with severe lesions lagged despite improvements. Our correlational analysis further confirmed a negative correlation between the severity of CWMLs and rehabilitation outcomes. This finding is consistent with the results of another previous study26. Additionally, patients with moderate and severe CWMLs did not regain NVC functions to the level of non-lesion patients within three years. This indicates a greater impact of CWMLs on NVC than on auditory and speech functions. Likewise, our correlational analysis supported this observation. The postoperative differences between subgroups indicate that significant rehabilitation disparities emerge only when CWMLs’ severity is sufficient to significantly impact or disrupt neural signal conduction. On the other hand, in cases of mild CWMLs, brain remodeling triggered by auditory function recovery may facilitate partial repair of damaged neural fibers and synapses or promote functional compensation. Animal studies have shown that congenital or neonatal deafness leads to functional degradation of the auditory system, including degeneration of ganglion cells and synapses as well as impaired temporal processing ability. However, early cochlear implantation with electrical stimulation can effectively restore auditory function and reestablish temporal processing of auditory signals by repairing synaptic structures, enhancing neural activity, and improving cell survival27,28,29,30,31. Additionally, studies have demonstrated that recovery in auditory and speech functions follows specific patterns18. As the auditory pathway is upstream of the language pathway, speech recovery lags behind auditory recovery since comprehension and clarity in hearing are prerequisites for speech. This is consistent with the findings of our study.
Moreover, this study is the first to reveal that the recovery of NVC function follows a distinct pattern, which differs significantly from the recovery trajectories of auditory and language functions. Specifically, auditory function recovery exhibits a “rapid-slow” pattern, language function recovery follows a “slow-rapid-slow” pattern, while NVC function recovery is more consistent with a “rapid-stable” pattern. This finding suggests that, although auditory, language, and NVC functions are interlinked during the recovery process, their mechanisms of recovery may be regulated by distinct neural pathways and brain networks. This novel discovery not only further supports the hypothesis that recovery patterns are influenced by the complexity of neural networks but also provides critical insights for future investigations into the recovery mechanisms of NVC function and the development of optimized intervention strategies.
Prognostic factors for CI outcomes in children with CWMLs
This study represents the first systematic analysis of prognostic factors for auditory, Language, and NVC function outcomes in children with CWMLs following CI, addressing a significant gap in the current field. By employing composite linear mixed models and linear mixed models, we comprehensively evaluated the independent risk and protective factors influencing functional recovery across different dimensions. These models explained 92% of the variance in postoperative auditory outcomes, 93% of the variance in Language outcomes, and 42.06% of the variance in NVC outcomes, demonstrating exceptional predictive power and robustness. We found that patients with CWMLs who underwent CI had the same prognostic factors for auditory and speech aided sound field thresholds in the better ear and Scheltens score were identified as independent risk factors, while household per capita annual income, preimplantation Z score, preimplantation CAP score, evaluation time (rehabilitation duration), and cesarean section were identified as independent protective factors.
A higher aided sound field threshold suggests significant preoperative damage to the auditory pathway, which not only impairs sound transmission but also disrupts the brain’s processing of auditory signals32. As a result of this damage, the brain’s neural networks are forced to undergo restructuring, but this process often falls short of fully restoring normal function, leading to reduced processing efficiency. This inefficiency in auditory processing hinders not only the recovery of hearing but also the restoration of speech function, as accurate speech perception and production rely heavily on precise auditory input. In contrast, a higher CAP score indicates relatively intact preoperative auditory pathway function, providing a strong foundation for successful postoperative hearing and speech rehabilitation33.
Higher per capita household income likely reflects a family’s capacity to provide a more stable supportive environment and richer opportunities for linguistic interaction in the postoperative period. Hart and Risley estimated that by the age of three, children from high socioeconomic status (SES) families are exposed to 30 million more words compared to their low-SES counterparts34. Evidence demonstrates that the development of key neurocognitive domains—such as executive functioning, sequential processing and sequence learning, and concept formation—critically depends on auditory experience and linguistic exposure35. The enriched linguistic interactions typically available in high-income families provide a foundational framework for the maturation of these advanced cognitive functions. Such a rich language environment and cognitive stimulation are essential for the recovery of auditory and speech abilities, not only by fostering language acquisition but also by enhancing neural connectivity and plasticity in brain regions associated with language processing, thereby accelerating functional recovery36,37,38. Furthermore, higher income facilitates improved rehabilitation outcomes through access to additional therapeutic services, increased availability of standardized rehabilitation programs, and the benefit of higher parental education levels. High-income families are better positioned to afford individualized interventions, overcome logistical barriers to high-quality care, and effectively understand and implement rehabilitation strategies. Collectively, these advantages underscore the critical role of addressing socioeconomic disparities in optimizing recovery outcomes.
The preimplantation Z score reflects patients’ NVC abilities. Previous research has demonstrated a significant correlation between higher non-verbal cognitive functioning and enhanced auditory and speech recovery following cochlear implantation35. Non-verbal cognitive resources, encompassing executive functions and visuospatial processing capabilities, effectively facilitate auditory information processing and establishment of linguistic representations, thereby promoting language development39. Cognitive neuroscience investigations have demonstrated that executive function networks and auditory processing pathways share neural substrates, particularly within the inferior frontal gyrus and superior temporal gyrus. The integrity of these shared neural networks may elucidate why enhanced non-verbal cognitive abilities potentiate auditory rehabilitation following cochlear implantation40. These cognitive mechanisms provide a robust neurocognitive foundation that enables children with hearing impairment to efficiently integrate novel auditory input and develop speech competencies after receiving cochlear implants.
Assessment time (rehabilitation duration), identified as an independent protective factor, underscores that auditory and linguistic recovery constitutes a continuous process. Auditory and language capabilities in patients exhibit progressive enhancement with sustained rehabilitation interventions. This protective effect operates through two principal mechanisms. Primarily, continuous rehabilitation establishes a stable, incremental auditory stimulation environment that enables the central auditory system to optimize adaptation to electrical stimulation patterns—a neural plasticity process necessitating adequate temporal intervals for consolidation41. Additionally, prolonged rehabilitation facilitates the development of neural correlates between auditory inputs and semantic comprehension, a mapping relationship that requires consistent practice for formation and reinforcement42. These observations emphasize the clinical significance of extended postoperative monitoring and rehabilitation protocols. Systematic rehabilitation regimens coupled with periodic functional assessments remain essential components for facilitating sustained improvements in patients’ auditory processing and linguistic competencies.
Alexander et al. reported higher placental bacterial colonization rates in vaginal deliveries compared to cesarean sections, attributed to repeated cervical examinations43. Microbial colonization can release non-infectious messengers into the fetal brain, causing inflammation and brain damage24. Additionally, hypoxic conditions during vaginal delivery are more severe than those during cesarean section44. Moreover, vaginal delivery often causes significant fetal head compression, potentially leading to various complications45. Therefore, cesarean section may reduce the risks of inflammation, severe hypoxia, and significant head compression associated with vaginal delivery, thereby decreasing the likelihood of brain injury and protecting auditory, speech, and NVC functions.
In patients with CWMLs undergoing CI, we identified several prognostic factors for NVC outcomes. In addition to the degree of CWMLs and cesarean section, preoperative speech levels and the type of implant device were also found to significantly affect NVC function. Improved preoperative speech levels may enhance brain plasticity, particularly during critical periods of brain development, fostering the growth of areas involved in non-verbal tasks46. Furthermore, this higher speech ability reflects more efficient neural network integration and bolsters cognitive reserve, equipping the brain to better handle postoperative challenges47. Children with strong cognitive reserve are better positioned to benefit from postoperative rehabilitation, facilitating NVC recovery, whereas those with poorer preoperative speech levels may face limitations in NVC recovery due to insufficient cognitive reserve.Additionally, our study found that patients using specific cochlear implant devices, such as Advanced Bionics, showed better postoperative NVC, potentially related to the number of internal electrodes, memory settings of the external processor, and compatibility with hearing aids on the other side48.
An intriguing finding of this study was that preoperative brain MRI was revisited for all 175 patients with CWMLs. Yet, a slight reduction in the severity of these lesions was observed in only four patients. This suggests that CWMLs in children with PLSND are primarily stable, limiting the clinical value of routine brain MRI follow-up. Nevertheless, brain MRI follow-up prior to CI remains necessary to rule out other potential brain abnormalities in patients with CWMLs.
Limitations and future directions
Although this study, with its large sample size and extended follow-up period, provides valuable insights into the impact of CWMLs on the postoperative rehabilitation of PLSND children following CI, the limitations of its retrospective design may weaken the ability to infer causality. This study addressed confounding factors using propensity score matching and controlled for biases related to hierarchical structure and repeated measures through mixed models. Additionally, while two cognitive assessment tools (GDS-C and H-NTLA-CR) were employed, the similarity in their assessment goals and content, along with standardized scoring systems and established reliability, likely minimized any potential biases.
Another limitation lies in the complexity of CWMLs’ anatomical distribution and their varied impacts on functional pathways, including auditory, speech, and cognitive networks. Most lesions were multifocal with coexisting involvement of both periventricular and deep white matter. Conventional MRI (T1WI, T2WI, and FLAIR) lacked the resolution and the ability to provide microstructural information, such as fiber integrity or functional connectivity, which are critical for understanding the mechanisms underlying functional outcomes. Future studies should adopt advanced imaging techniques, such as DTI and fMRI, to quantify white matter microstructure and connectivity, and include children with CWMLs limited to a single lesion site to better isolate the specific impacts of lesion location on rehabilitation outcomes.
Additionally, this study did not directly measure daily device use, which has been widely recognized as a critical factor influencing speech recognition outcomes in cochlear implant recipients. Standardized rehabilitation protocols implemented across all centers likely ensured similar device usage among patients, reducing variability. Nevertheless, the absence of objective measures, such as datalogging, may limit a more comprehensive understanding of its impact. Future studies should incorporate such measures to better explore the relationship between daily device use and rehabilitation outcomes.
At the time of the study, most CI devices were incompatible with MRI, and even those that were compatible often produced significant artifacts, limiting our ability to directly observe changes in white matter lesions post-CI. However, with the advancement of new CI devices and sophisticated imaging technologies such as SEMAC and MAVRIC sequences, these obstacles are gradually being overcome. Future research should leverage these advancements to explore white matter remodeling after CI using high-resolution MRI and adopt prospective designs to better elucidate causality, ultimately refining CI surgical indications and optimizing rehabilitation strategies for patients with white matter lesions.
Conclusions
In children with PLSND and CWMLs, the CWMLs are generally stable, and these children usually present poorer initial auditory thresholds. CWMLs negatively impact auditory, speech, and NVC outcomes in children with PLSND following CI, with the effects strongly correlated with lesion severity. Additionally, this study revealed that speech rehabilitation for patients with CWMLs often trails behind auditory rehabilitation, and elevated preoperative speech levels may safeguard against postoperative NVC decline. This highlights the critical need to concentrate on speech development during treatment and to devise long-term, targeted speech therapy strategies. Therefore, a comprehensive assessment incorporating the severity of CWMLs, perinatal history, and clinical features is essential for delivering personalized interventions to children with PLSND.
Materials and methods
Participating rehabilitation facilities
This study was based on retrospective records from ten different rehabilitation institutions governed by the Hubei Disabled Persons’ Federation Rehabilitation Center, the Hubei Deaf Infant Healing Center, and the Wuhan Yimeng Hearing Rehabilitation Center. This study was approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (approval number: [2023]0911). All methods were conducted in accordance with the relevant guidelines and regulations, including the Personal Information Protection Law of the People’s Republic of China and international data protection regulations. All patient data were de-identified to ensure privacy. A waiver of informed consent was obtained from the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology due to the anonymized nature of patient data, the retrospective design, and the observational nature of the study. These rehabilitation institutions cover all designated CI rehabilitation centers in Hubei Province, distributed across various prefecture-level cities, providing a diverse rehabilitation environment conducive to a comprehensive assessment of the impact of CWMLs on CI outcomes. All rehabilitation institutions regularly undergo training and employ a standardized rehabilitation training method (auditory-verbal therapy, AVT), assessment procedures, assessment intervals (biannually post-activation), and recording templates. We collected core information on demographics, clinical and surgical characteristics (such as age at diagnosis of deafness, residual hearing, duration of hearing aid use pre-surgery, preoperative rehabilitation duration, age at implantation, brands of implant device), and pre-and postoperative assessments of auditory, speech, and non-verbal cognitive functions.
Participants
The inclusion criteria for CI participants in this study were as follows: bilateral severe to profound sensorineural deafness (> 70 dB); onset of hearing loss before the development of speech capabilities; unilateral CI; age at implantation ≤ 14 years. Exclusion criteria include serious complications such as intraoperative or postoperative gusher, cerebrospinal fluid leakage, meningitis, and facial paralysis; previous contralateral CI or cochlear reimplantation; and patients with cognitive impairments, cerebral palsy, visual impairments, or other cerebral pathologies. The CI dates for all participants in this study ranged from January 2012 to December 2020.
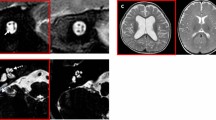
Neuroimaging
In this study, two radiologists analyzed preoperative brain MRI images of 175 children with CWMLs. In T1-weighted images, CWMLs appeared as low signals, while in T2-weighted and Fluid-Attenuated Inversion Recovery (FLAIR) imaging, they presented as high signals. All children underwent at least one follow-up brain MRI six months post-preoperative evaluation, with assessments based on the most recent scan. The severity of CWMLs was graded according to the Scheltens scale, which assesses the involvement of deep cerebral white matter and periventricular cerebral white matter49. CWMLs were categorized based on Scheltens score into three subgroups: (1) Mild CWMLs (Scheltens scale 1–3, n = 57); (2) Moderate CWMLs (Scheltens scale 4–10, n = 60); (3) Severe CWMLs (Scheltens scale > 10, n = 58).
Auditory performance evaluation
Auditory performance was assessed using the Categories of Auditory Performance (CAP) scale, applicable to patients of all ages. The CAP scale is widely used to measure patients’ daily communication abilities and serves as a crucial indicator of their auditory development50. Senior rehabilitation assessors at each rehabilitation institution conducted the CAP assessments at baseline (pre-implantation) and 6, 12, 18, 24, 30, and 36 months post-activation, to monitor changes in auditory performance.
Speech performance evaluation
To measure speech capabilities, this study utilized the Speech Intelligibility Rating (SIR) scale, which applies to assessing speech development in patients of all ages51. Senior rehabilitation assessors at each rehabilitation institution conducted the SIR assessments at baseline (pre-implantation) and 6, 12, 18, 24, 30, and 36 months post-activation, to monitor the progress of speech performance.
Non-verbal cognitive evaluation
To assess non-verbal cognitive abilities, this study utilized the Chinese version of the Griffiths Mental Development Scale (GDS-C) and the Chinese revision of the Hiskey-Nebraska Test of Learning Aptitude (H-NTLA-CR)52,53. The Griffiths Mental Development Scale (GDS) is globally used to evaluate non-verbal cognitive development in children from birth to 8 years of age54. The Chinese version (GDS-C), revised in 2010 based on the 2006 version, has been validated as an accurate and effective tool for assessing non-verbal cognitive development in young children52 The Hiskey-Nebraska Test of Learning Aptitude (H-NTLA) assesses non-verbal cognitive development in children aged 3-1755. Its Chinese revision, H-NTLA-CR, was re-revised in 2010, and its reliability and validity have been evaluated53 Both tests share similarities in evaluating aspects such as motor manipulation, attention, memory, logical reasoning, and visual-spatial skills. In our study, GDS-C was used for children under 3 years, while H-NTLA-CR was used for those aged 3 and above. The non-verbal cognitive assessments were conducted by senior rehabilitation assessors at each institution, at baseline and 12, 24, and 36 months post-activation. Non-verbal cognitive performance scores (GDS-C and H-NTLA-RC) were compared with the normative data for deaf children in China, standardized into Z scores, and combined into a single score (non-verbal cognitive Z score)53,56. This standardization allows comparability between scores from different ranges57. According to the DSM-5, children with Z scores above − 1 are considered within the normal range, while those with scores between − 1 and − 2 are regarded as borderline in intellectual functioning58. This study focused its assessments on children within the normal and borderline intellectual functioning ranges.
Propensity score matching
To control for imbalances in covariates between the CWMLs group and the control group, this study employed the propensity score matching method. A total of 17 variables were used for matching, including gender, perinatal exposure to toxic substances history, perinatal trauma history, perinatal noise history, perinatal infection history, perinatal medication history, perinatal hypoxia history, cesarean section, premature birth, Low birth weight, household per capita annual income, duration of preimplantation hearing aid use, duration of preimplantation rehabilitation, age at implantation, rehabilitation facility, CI center, and CI device. A 1:1 nearest-neighbor matching method was used, with a caliper set at 0.01. Numerous studies have shown that CWMLs can affect pre-implantation auditory, speech, and non-verbal cognitive functions59,60. Furthermore, in this study, baseline assessments of auditory, speech, and non-verbal cognitive functions were conducted after exposure to CWMLs. Thus, these baseline assessments may represent both the initial outcomes of CWMLs and potential mediating variables between the lesions and the outcomes. Therefore, to avoid attenuating or eliminating the effect of exposure, leading to erroneous conclusions, baseline auditory, speech, and non-verbal cognitive functions were not used as covariates in the matching. Ultimately, analyses were conducted on 175 children with CWMLs and an equal number of children in the control group (Fig. 1a).
Data analysis
Continuous variables included household per capita annual income, unaided sound field thresholds in the better ear, aided sound field thresholds in the better ear, ASSR thresholds in the better ear, duration of preimplantation hearing aid use, duration of preimplantation rehabilitation, age at implantation, and non-verbal cognitive Z score. Ordinal categorical variables included Scheltens score, CAP score, SIR score, and assessment time. Unordered categorical variables comprised gender, perinatal exposure to toxic substances history, perinatal trauma history, perinatal noise history, perinatal infection history, perinatal medication history, perinatal hypoxia history, cesarean section, premature birth, low birth weight, CI device, CI center, and rehabilitation facility. The assumptions of normal distribution and homogeneity of variances for the independent variables were tested using the Kolmogorov-Smirnov test and the test for equality of variances, respectively. As all continuous variables failed to meet the assumptions of normality and homogeneity of variances, non-parametric statistical methods were employed for their analysis to ensure robustness and reliability.
Continuous variables were described using median values (with interquartile ranges) and compared using the Mann-Whitney U test for intergroup differences and the Kruskal-Wallis (K-W) test for subgroup differences. Ordinal categorical variables were presented as mean ± SEM and analyzed using the Mann-Whitney U test for intergroup differences and the Kruskal-Wallis test for subgroup differences. Nominal categorical variables were presented in terms of frequency and proportion, with the Chi-square test or Fisher’s exact test employed for intergroup comparisons. All subgroup analyses were adjusted using the Bonferroni correction.
Additionally, this study utilized Allometric functions to fit the nonlinear relationships between the Scheltens score and both the CAP score and SIR score, as well as the Log3P1 function to fit the nonlinear relationship between the Scheltens score and non-verbal cognitive Z score. The Spearman method was employed to analyze the correlations between Scheltens score and CAP score, SIR score, and non-verbal cognitive Z score.
A cumulative link mixed model was employed to investigate prognostic factors for CAP and SIR scores, while a linear mixed model was used to analyze prognostic factors for non-verbal cognitive Z scores. Both models incorporated subject-specific random intercepts to account for inter-individual variability. Variables with p-values < 0.1 in the univariate analyses were included in the multivariate analyses. The multivariate analyses utilized the backward likelihood ratio (LR) method for variable selection, with an exclusion criterion of p ≥ 0.05 to retain significant predictors in the final model. Additionally, potential interaction effects between key predictors were evaluated in the final models to explore whether the combined influence of two or more variables significantly impacted the outcomes. Interaction terms were introduced stepwise into the models and their significance was assessed using likelihood ratio tests. Interaction terms were retained only if they were significant (p < 0.05), ensuring the final models’ parsimony and interpretability.
Multiple sensitivity analyses were conducted to verify the robustness of the study results. The final model was developed in two steps: first identifying variables through univariable analysis, and then refining the model using multivariable analysis. In Model 1, additional adjustments were made for rehabilitation institutions compared to the final model. In Model 2, hospitals were additionally adjusted, beyond what was done in the final model. In Model 3, both rehabilitation institutions and hospitals were further adjusted in addition to the final model. In Model 4, the model was reconstructed using Generalized Estimating Equations (GEE), adjusting for the variables included in the final model.
Less than 3.88% of our sample data were missing, which were considered to be missing at random and were handled by pairwise deletion in the analysis. Intergroup and subgroup differences were analyzed using SPSS 29.0 (SPSS, Chicago, IL, USA). Curve fitting and plotting, as well as scatter plotting, were performed using Origin10.1 (OriginLab Corporation, Northhampton, MA, USA). Linear mixed-effects models were established in R (4.3.2) using lme4 (1.1–35.1) and lmerTest (3.1.3). GEE models were fitted using Geepack (1.3.9). Inference and comparison of models were conducted using MuMIn (1.47.5). Forest plots and regression coefficient plots were generated using ggplot2 (3.4.4). All statistical tests were two-sided, with a P-value < 0.05 considered significant.
Data availability
The data that support the findings of this study are available from the ten rehabilitation institutions (as described previously). Restrictions apply to the availability of these data, which were used under license for this study. Data are available from the corresponding authors with the permission of the ten rehabilitation institutions (as described previously).
References
MORTON, N. E. Genetic epidemiology of hearing impairment. Ann. N. Y. Acad. Sci. 630, 16–31 (1991).
Kral, A., Dorman, M. F. & Wilson, B. S. Neuronal development of hearing and language: Cochlear implants and critical periods. Annu. Rev. Neurosci. 42, 47–65 (2019).
Kral, A. & O’Donoghue, G. M. Profound deafness in childhood. N. Engl. J. Med. 363, 1438–1450 (2010).
Polat, F. Factors affecting psychosocial adjustment of deaf students. J. Deaf Stud. Deaf Edu. 8, 325–339 (2003).
Haukedal, C. L., Lyxell, B. & Wie, O. B. Health-Related quality of life with cochlear implants: The children’s perspective. Ear Hear. 41, 330–343 (2020).
Assiri, M., Alshalan, A., Alqahtani, R., Abdelsamad, Y. & Alsanosi, A. Brain MRI findings of prelingually deaf children and cochlear implant outcome: Preliminary results. Int. J. Pediatr. Otorhinolaryngol. 162, 111302 (2022).
Hüppi, P. S. et al. Microstructural brain development after perinatal cerebral white matter injury assessed by diffusion tensor magnetic resonance imaging. Pediatrics 107, 455–460 (2001).
Lin, Y. et al. Diffusion tensor imaging of the auditory pathway in sensorineural hearing loss: Changes in radial diffusivity and diffusion anisotropy. J. Magn. Reson. Imaging 28, 598–603 (2008).
Armstrong, N. M. et al. Association of poorer hearing with longitudinal change in cerebral white matter microstructure. JAMA Otolaryngol. Head Neck Surg. 146, 1035 (2020).
Luthra, S. & Nagarkar, A. 1418 Leukodystrophy & its effects on rehabilitation of children with cochlear implant: A preliminary case study. Pediatr. Res. 68, 701–701 (2010).
Shen, M., Chen, Z. & Li, Y. Behavioral and electrophysiological investigation of hearing and speech outcomes in pre-linguistic deaf children with white matter changes after cochlear implantation. Acta Otolaryngol. (Stockh). 139, 1090–1097 (2019).
Kumar, S., Gautam, P., Sharma, R. & Taneja, V. Etiological factors for pediatric sensorineural hearing loss. Indian J. Otol. 17, 162 (2011).
Xu, X. Q., Wu, F. Y., Hu, H., Su, G. Y. & Shen, J. Incidence of brain abnormalities detected on preoperative brain MR imaging and their effect on the outcome of cochlear implantation in children with sensorineural hearing loss. Int. J. Biomed. Imaging 2015, 1–6 (2015).
Musiek, F. E., Chermak, G. D. & Cone, B. Central deafness: A review of past and current perspectives. Int. J. Audiol. 58, 605–617 (2019).
Kim, Y. S. et al. Full etiologic spectrum of pediatric severe to profound hearing loss of consecutive 119 cases. Sci. Rep-UK 14, 12335 (2022).
Martinez-Biarge, M. et al. White matter and cortical injury in hypoxic-Ischemic encephalopathy: Antecedent factors and 2-Year outcome. J. Pediatr. 161, 799–807 (2012).
Sayyid, Z. N. et al. Congenital hearing loss is associated with a high incidence of central nervous system abnormalities. Otol Neurotol. 41, 1397–1405 (2020).
Lyu, J. et al. Long-term follow-up of auditory performance and speech perception and effects of age on cochlear implantation in children with pre-lingual deafness. Chin. Med. J. (Engl). 132, 1925–1934 (2019).
Culbertson, S. R. et al. Younger age at cochlear implant activation results in improved auditory skill development for children with congenital deafness. J. Speech Lang. Hear. Res. 65, 3539–3547 (2022).
Sharma, S., Bhatia, K., Singh, S., Lahiri, A. K. & Aggarwal, A. Impact of socioeconomic factors on paediatric cochlear implant outcomes. Int. J. Pediatr. Otorhinolaryngol. 102, 90–97 (2017).
Baser, B., Patidar, M. & Surana, P. A. Study to determine various factors influencing auditory outcomes in paediatric cochlear implantation. Indian J. Otolaryngol. 72, 453–456 (2020).
Kang, D. H., Lee, M. J., Lee, K. Y., Lee, S. H. & Jang, J. H. Prediction of cochlear implant outcomes in patients with prelingual deafness. Clin. Exp. Otorhinolar. 9, 220–225 (2016).
Skranes, J. et al. Abnormal cerebral MRI findings and neuroimpairments in very low birth weight (VLBW) adolescents. Eur. J. Paediatr. Neurol. 12, 273–283 (2008).
Dammann, O. & Leviton, A. Role of the fetus in perinatal infection and neonatal brain damage. Curr. Opin. Pediatr. 12, 99 (2000).
Duffau, H. Stimulation mapping of white matter tracts to study brain functional connectivity. Nat. Rev. Neurol. 11, 255–265 (2015).
Wang, S. et al. Cochlear implantation in children with white matter lesions. Med. (Baltim). 100, e23355 (2021).
Ryugo, D. K., Kretzmer, E. A. & Niparko, J. K. Restoration of auditory nerve synapses in cats by cochlear implants. Science 310, 1490–1492 (2005).
Berger, C., Kühne, D., Scheper, V. & Kral, A. Congenital deafness affects deep layers in primary and secondary auditory cortex. J. Comp. Neurol. 525, 3110–3125 (2017).
Klinke, R., Kral, A., Heid, S., Tillein, J. & Hartmann, R. Recruitment of the auditory cortex in congenitally deaf cats by Long-Term cochlear electrostimulation. Science 285, 1729–1733 (1999).
Fallon, J. B., Irvine, D. R. F. & Shepherd, R. K. Cochlear implant use following neonatal deafness influences the cochleotopic organization of the primary auditory cortex in cats. J. Comp. Neurol. 512, 101–114 (2009).
Leake, P. A., Hradek, G. T. & Snyder, R. L. Chronic electrical stimulation by a cochlear implant promotes survival of spiral ganglion neurons after neonatal deafness. J. Comp. Neurol. 412, 543–562 (1999).
Yuan, D. et al. Early-stage use of hearing aids preserves auditory cortical structure in children with sensorineural hearing loss. Cereb. Cortex 34, bhae145 (2024).
Fontenot, T. E. et al. Residual cochlear function in adults and children receiving cochlear implants: Correlations with speech perception outcomes. Ear Hear. 40, 577–591 (2019).
Hart, B. & Risley, T. The Early Catastrophe the 30 Million Word Gap by Age 3, Published in Meaningful Differences in the Everyday Experience of Young American Children. (Brookes, 1995).
Kral, A., Kronenberger, W. G., Pisoni, D. B. & O’Donoghue, G. M. Neurocognitive factors in sensory restoration of early deafness: A connectome model. Lancet Neurol. 15, 610–621 (2016).
Panda, S. et al. Comprehensive analysis of factors leading to poor performance in prelingual cochlear implant recipients. Otol Neurotol. 40, 754–760 (2019).
Romeo, R. R. et al. Neuroplasticity associated with changes in conversational turn-taking following a family-based intervention. Dev. Cogn. Neurosci. 49, 100967 (2021).
Romeo, R. R. et al. Language exposure relates to structural neural connectivity in childhood. J. Neurosci. 38, 7870–7877 (2018).
Burkholder, R. A. & Pisoni, D. B. Speech timing and working memory in profoundly deaf children after cochlear implantation. J. Exp. Child. Psychol. 85, 63–88 (2003).
Hickok, G. & Poeppel, D. The cortical organization of speech processing. Nat. Rev. Neurosci. 8, 393–402 (2007).
Fu, Q. J. & Galvin, J. J. Perceptual learning and auditory training in cochlear implant recipients. Trends Amplif. 11, 193–205 (2007).
Ingvalson, E. M. & Wong, P. C. M. Training to improve Language outcomes in cochlear implant recipients. Front. Psychol. 4 (2013).
Alexander, J. M. et al. The impact of digital cervical examination on expectantly managed preterm rupture of membranes. Am. J. Obstet. Gynecol. 183, 1003–1007 (2000).
Berger, N., Vaillancourt, C. & Boksa, P. Interactive effects of anoxia and general anesthesia during birth on the degree of CNS and systemic hypoxia produced in neonatal rats. Exp. Brain Res. 131, 524–531 (2000).
Lear, C. A. et al. Fetal defenses against intrapartum head compression—Implications for intrapartum decelerations and hypoxic-ischemic injury. Am. J. Obstet. Gynecol. 228, S1117–S1128 (2023).
Schlaug, G., Marchina, S. & Norton, A. Evidence for plasticity in White-Matter tracts of patients with chronic Broca’s aphasia undergoing intense Intonation‐based speech therapy. Ann. N. Y. Acad. Sci. 1169, 385–394 (2009).
Barulli, D. & Stern, Y. Efficiency, capacity, compensation, maintenance, plasticity: Emerging concepts in cognitive reserve. Trends Cogn. Sci. 17, 502–509 (2013).
Spahr, A. J. & Dorman, M. F. Performance of subjects fit with the advanced bionics CII and nucleus 3G cochlear implant devices. Arch. Otolaryngol. Head Neck Surg. 130, 624 (2004).
Scheltens, P. et al. A semiquantative rating scale for the assessment of signal hyperintensities on magnetic resonance imaging. J. Neurol. Sci. 114, 7–12 (1993).
Archbold, S., Lutman, M. E. & Nikolopoulos, T. Categories of auditory performance: Inter-user reliability. Br. J. Audiol. 32, 7–12 (1998).
Allen, M. C., Nikolopoulos, T. P. & O’Donoghue, G. M. Speech intelligibility in children after cochlear implantation. Am. J. Otol. 19, 742–746 (1998).
Tso, W. W. Y. et al. The Griffiths development Scales-Chinese (< scp > GDS‐C): A cross‐cultural comparison of developmental trajectories between Chinese and British children. Child. Care Health Dev. 44, 378–383 (2018).
Yang, X., Qu, C., Sun, X., Zhu, F. & Wang, J. Norm revision of H-NTLA for children from 3 to 7 years old in China. Chin. J. Clin. Psychol. 19, 195–197 (2011).
Griffiths, R. The Abilities of Young Children: A Comprehensive System of Mental Measurement for the First Eight Years of Life (The Test Agency, 1984).
Hiskey, M. S. Hiskey-Nebraska Test of Learning Aptitude (Union College, 1966).
Qu, C. et al. A comparative study on the mental development of 308 hearing-impaired children and 473 normal-hearing children 3 years old. Chin. Sci. J. Hear. Speech Rehabil. 15–18. https://doi.org/10.3969/j.issn.1672-4933.2010.05.002 (2010).
Micheletti, S. et al. Cognitive improvement after cochlear implantation in deaf children with associated disabilities. Dev. Med. Child. Neurol. 62, 1429–1436 (2020).
Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (5th edition). Ref. Rev. 28, 36–37 (2014).
Woodward, L. J., Anderson, P. J., Austin, N. C., Howard, K. & Inder, T. E. Neonatal MRI to predict neurodevelopmental outcomes in preterm infants. N. Engl. J. Med. 355, 685–694 (2006).
Inder, T. E., Volpe, J. J. & Anderson, P. J. Defining the neurologic consequences of preterm birth. N. Engl. J. Med. 389, 441–453 (2023).
Acknowledgements
This work was supported by the National Natural Science Foundation of China [Grant numbers 82071057, 82101229] and Key Research and Development Program of Hubei Province Project [Grant 2021BCA144].
Author information
Authors and Affiliations
Contributions
Hejie Li: Conceptualization, Methodology, Formal Analysis, Investigation, Data Curation, Writing – Original Draft, Writing – Review & Editing, Visualization. Shimin Zong, Hongjun Xiao: Conceptualization, Methodology, Validation, Supervision, Project Administration, Funding Acquisition, Writing – Review & Editing. Wei Tang, Ting Li: Formal Analysis, Investigation, Data Curation, Writing – Original Draft, Visualization. Shanhong Wang, Hui Li, Muqin Yun, Jing Xu, Weilin Tan, Xiaoxia Jin, Hongyan Li, Yuanlin Teng, Zaihong Du, and Hongzheng Tian: Investigation, Data Curation, Writing – Review & Editing, Resources.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical considerations
This study was approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (approval number: [2023]0911). All research methods complied with relevant guidelines and regulations, including the Personal Information Protection Law of the People’s Republic of China and international data protection regulations. As this was a retrospective and observational study with anonymized patient data, the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology granted a waiver of informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, H., Tang, W., Li, T. et al. Outcomes and prognostic factors in prelingually sensorineural deaf children with cerebral white matter lesions following cochlear implantation: a multicenter, retrospective study. Sci Rep 15, 16337 (2025). https://doi.org/10.1038/s41598-025-01158-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01158-0
