
Abstract
Retinal pigment epithelium (RPE) melanin thickness maps, derived from multi-contrast images—including the degree of polarization uniformity (DOPU), optical coherence tomography (OCT) angiography, and the attenuation coefficient—are obtained using multi-contrast polarization-sensitive OCT (PS-OCT). These maps have demonstrated utility for three-dimensional assessment of changes in melanin within the RPE (RPE-melanin). While both OCT angiography and the attenuation coefficient can be derived from conventional OCT, measuring the DOPU requires PS-OCT, which is not available on standard commercial OCT systems. To overcome this limitation, we utilized a convolutional neural network to generate DOPU-like images from standard OCT images and used these to calculate a synthesized RPE-melanin thickness map. We evaluated 22 eyes from 20 patients with serous pigment epithelial detachment (PED) secondary to age-related macular degeneration. Both original and synthesized RPE-melanin thickness maps were calculated from multi-contrast PS-OCT datasets. Active RPE lesions were defined as areas with RPE-melanin thickness of ≥ 70 μm (originalRPE70 and synRPE70 for the original and synthesized maps, respectively). Both synthesized and original RPE-melanin thickness maps closely resembled near-infrared autofluorescence imaging. Furthermore, both the originalRPE70 area and synRPE70 area were significantly positively correlated with the PED volume. Synthesized RPE-melanin thickness maps may be useful for clinical quantification of RPE-melanin.
Similar content being viewed by others
Introduction
Age-related macular degeneration (AMD) is a leading cause of vision loss in older adults1. Changes in the retinal pigment epithelium (RPE) are a key clinical feature of AMD2. Pigment epithelial detachment (PED) is commonly observed in patients with AMD3. In eyes with PED—particularly drusenoid and serous types—RPE cells exhibit a range of responses, including sloughing, shedding, hypertrophy, and intraretinal migration4,5,6. These RPE changes are important indicators of RPE function, making their clinical evaluation essential for AMD management4.
Clinical retinal autofluorescence (AF) imaging is widely used to assess RPE alterations in AMD7,8. Short-wavelength AF (SW-AF), induced by excitation at 488 nm, primarily originates from lipofuscin or melanolipofuscin9. Near-infrared AF (NIR-AF), induced by excitation at 785 nm, mainly arises from melanin or melanolipofuscin10,11. Simultaneous hyper-AF in both SW-AF and NIR-AF likely indicates increased melanolipofuscin concentration within RPE cells, along with RPE cell thickening and intraretinal migration6,12. Despite its widespread use, a significant limitation of clinical AF imaging is the lack of topographical information.
Intensity-based optical coherence tomography (OCT) (i.e., standard OCT) is another crucial clinical tool for evaluating RPE changes4,5,13. Some intraretinal hyperreflective foci observed in standard OCT images are thought to result from intraretinal RPE migration14, which may also contribute to hyper-AF lesions6,7,12. Certain thickened RPE–Bruch’s membrane bands seen in standard OCT may reflect RPE dysmorphia and stacking2,4. Although standard OCT provides valuable information about RPE changes, its ability to directly visualize and assess RPE cells is limited by the lack of specific contrast for these cells, hindering direct comparison with AF images.
Polarization-sensitive OCT (PS-OCT) enhances tissue differentiation in retinal diseases15,16. Melanin-induced light scattering within the RPE causes depolarization, which is quantified by the degree of polarization uniformity (DOPU)17,18. DOPU values range from 0.0 to 1.0, with lower values indicating greater depolarization or polarization scrambling. Combining PS-OCT and AF imaging enables comprehensive assessment of RPE changes in AMD6,12,19. However, a key limitation of PS-OCT in evaluating RPE changes is the difficulty in distinguishing between melanin within the RPE (RPE-melanin) and melanin in the choroid12,19. To address this, we developed an algorithm using multi-contrast PS-OCT to automatically highlight RPE-melanin20. Multi-contrast PS-OCT simultaneously acquires OCT angiography, PS-OCT, and standard OCT images, from which we generated RPE-melanin–specific contrast OCT (RPE-melanin OCT) images for evaluating RPE changes20. Both NIR-AF and RPE-melanin OCT imaging are believed to be sensitive to RPE-melanin changes10,11,20. Prior work in AMD and Vogt–Koyanagi–Harada disease has shown similarities between NIR-AF and RPE-melanin OCT projection images, suggesting that combining RPE-melanin OCT and AF imaging offers value for quantitatively assessing RPE changes in macular diseases12,19.
However, a significant challenge remains in the clinical application of RPE-melanin OCT imaging. This imaging is calculated based on the DOPU, the attenuation coefficient, and OCT angiography. While the attenuation coefficient and OCT angiography can be derived using commonly available commercial retinal OCT devices, calculating the DOPU requires PS-OCT17. In PS-OCT, detecting the polarization state of the backscattered probe light requires capturing two orthogonal polarization components. This setup necessitates two detectors and a polarization splitter in addition to the components of a conventional retinal OCT system16. As a result, PS-OCT is more complex and costly than standard clinical retinal OCT, limiting its use to research settings. Deriving the DOPU from standard OCT with single-polarization detection would expand the capabilities of existing OCT systems and enable RPE-melanin OCT calculation without the need for PS-OCT.
Deep learning has significantly advanced the field of ophthalmology21. Recent research has demonstrated the potential of deep learning to generate PS-OCT images—including metrics such as DOPU and retardation—from standard OCT images22,23,24. Our group employed a convolutional neural network to create DOPU images from standard retinal OCT data22. We showed that these synthesized DOPU images are useful for visualizing AMD-related RPE changes, achieving results comparable to those obtained using the DOPU derived directly from PS-OCT22. A key advantage of using the synthesized DOPU rather than the PS-OCT-derived DOPU is that it enables the calculation of RPE-melanin OCT imaging from standard OCT data. In this study, we generated synthesized RPE-melanin OCT images using the attenuation coefficient and OCT angiography data combined with synthesized DOPU images. We then evaluated the effectiveness of these synthesized RPE-melanin OCT images for quantifying AMD-related RPE changes and compared the results with established RPE-melanin OCT imaging.
Methods
Participants
This prospective, observational, cross-sectional study was conducted in accordance with the Declaration of Helsinki and approved by the Tokyo Medical University Institutional Review Board (T2019-0072 and T2019-0217). It was registered with the University Hospital Medical Information Network (UMIN000039650 and 000039648; http://www.umin.ac.jp/ctr/index-j.htm). All participants provided written informed consent after receiving a full explanation of the study’s nature and implications.
Thirty-six healthy eyes from 36 Japanese participants (8 men, 28 women; age range, 20–61 years; mean age, 39.3 years) were evaluated, with the right eye of each participant selected for analysis. The exclusion criteria were a history of intraocular surgery and any history or evidence of chorioretinal, vitreoretinal, or glaucomatous disease. Additionally, 22 eyes from 20 Japanese patients with serous PEDs due to AMD (15 men, 5 women; age range, 56–84 years; mean age, 71.6 years) were examined. Eyes with retinal diseases other than AMD were excluded. Serous PED was defined as serous elevation of the RPE without retinal hemorrhage, hard exudates, or choroidal neovascularization, the latter of which was ruled out using commercial retinal OCT angiography (DRI-OCT Triton; Topcon, Tokyo, Japan). To avoid treatment-related influences, eyes with prior intravitreal injections, photodynamic therapy, or laser treatment were excluded, as were eyes with severe cataracts or other conditions significantly impairing image quality.
Axial length was measured using an optical biometer (OA-2000; Tomey, Nagoya, Japan). The mean ± standard deviation axial length was 25.1 ± 1.5 mm (range, 22.4–28.0 mm) for healthy eyes and 23.1 ± 1.1 mm (range, 20.5–25.7 mm) for eyes with serous PEDs.
Multi-contrast PS-OCT
A prototype multi-contrast PS-OCT system was used, as described in previous publications25,26. This system simultaneously acquires standard OCT images, OCT angiography, and DOPU data. Standard OCT images were generated by coherently combining four repeated scans. OCT angiography was processed using a noise-corrected, complex-correlation-based method27, and DOPU data were calculated using Makita’s noise correction with a 3- × 3-pixel kernel28. The system employs a 1.0-µm swept-source laser, achieving an axial scan rate of 100,000 A-scans per second and a 6.0-µm axial resolution in tissue. Volumetric scans covered a 6.0- × 6.0-mm area on the retina using a horizontal-fast raster scanning protocol of 512 A-lines by 256 B-scans. Transverse magnification was calibrated using a modified Littmann’s method for quantitative measurements29. Four repeated B-scans were acquired at each location, resulting in a volumetric acquisition time of 6.6 s. Only multi-contrast PS-OCT volumes free of significant motion artifacts were included in the study.
Synthesized DOPU
The DOPU synthesizing network, based on U-Net30, was used to generate the synthesized DOPU images. Details of the network architecture and training process are provided in our previous work22. Briefly, the training and validation datasets included 38 normal eyes of 26 healthy volunteers and 457 pathological eyes of 330 patients. The pathological cases included AMD, diabetic retinopathy, central serous chorioretinopathy, uveitis, retinal vein occlusion, and pathologic myopia. None of the participants in the present study were included in either dataset. The dataset, comprising volumetric OCT data, was divided on a subject-wise basis into training and validation sets using an 8:2 ratio. In total, 69,478 patches were used for training and 17,382 patches for validation. The DOPU synthesizing network was trained with standard OCT images as input and the corresponding DOPU images as ground truth, using binary cross-entropy as a cost function. The performance of the method was evaluated on both healthy and pathological eyes. The synthesized DOPU images closely resembled the actual DOPU images, and their ability to visualize RPE abnormalities showed a high level of consistency22.
Synthesized RPE-melanin OCT imaging
Details of the original RPE-melanin OCT imaging have been published previously20. To automatically distinguish RPE-melanin from choroidal melanin in DOPU images, an index called FRPE was calculated. This index incorporates the attenuation coefficient31, the DOPU, and the blood flow signal from OCT angiography:
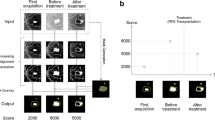
FRPE was designed to specifically highlight RPE-melanin by leveraging the absence of blood flow within the RPE. A high FRPE value suggests the presence of RPE-melanin. RPE-melanin B-scan images were generated by mapping the FRPE distribution within each B-scan, allowing for assessment of the depth-resolved RPE-melanin distribution (Fig. 1). RPE-melanin thickness maps were then created by counting pixels with high FRPE values (≥ 0.15) along each A-line in the volumetric dataset (Fig. 1).

Original and synthesized RPE-melanin OCT imaging of the healthy right eye of a 49-year-old man. (a) En face projection image of standard OCT. The yellow line indicates the scanning position of the multi-contrast PS-OCT B-scan images shown in (b–f). (b) Standard OCT B-scan image. (c) DOPU B-scan image. (d) Synthesized DOPU B-scan image. (e) Original RPE-melanin B-scan image. (f) Synthesized RPE-melanin B-scan image. (g) Original RPE-melanin thickness map. (h) Synthesized RPE-melanin thickness map.
Synthesized RPE-melanin OCT images were derived by computing synthesized FRPE, which was obtained by substituting synthesized DOPU for DOPU in the FRPE calculation. From this, synthesized RPE-melanin B-scans and thickness maps were generated (Fig. 1). For eyes with serous PED, the area of thickened RPE-melanin (≥ 70 μm: originalRPE70 for original, synRPE70 for synthesized) was quantified from these maps using Fiji32 (Figs. 2 and 3).

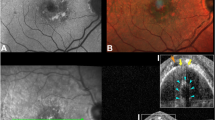
Original and synthesized RPE-melanin OCT imaging of serous PED in the left eye of a 70-year-old man. (a) SW-AF and (b) NIR-AF images show hyper-AF lesions. (a) In the SW-AF image, the hyper-AF lesion is partially obscured in the foveal region (red arrow). (c) En face projection image of standard OCT. The red line indicates the margin of the PED, and the yellow line indicates the scanning position for B-scan images in (d–f). (d) The standard OCT B-scan image shows a thickened RPE band at the site of the hyper-AF lesion. Both the (e) original and (f) synthesized RPE-melanin B-scan images show melanin accumulation at the RPE band. The (g) original and (h) synthesized RPE-melanin thickness maps closely resemble the (b) NIR-AF image, with RPE-melanin thickness clearly visualized in (i,j) the color-coded maps. (k) En face distribution of originalRPE70. (l) En face distribution of synRPE70.

Original and synthesized RPE-melanin OCT imaging of serous PED in the left eye of a 56-year-old man. (a) SW-AF and (b) NIR-AF images show hyper-AF lesions. (a) In the SW-AF image, the hyper-AF lesion is partially obscured in the foveal region (red arrow). (c) En face projection image of standard OCT. The red line indicates the margin of the PED, and the yellow line indicates the scanning positions for B-scan images in (d–f). (d) The standard OCT B-scan image shows intraretinal hyperreflective foci within the hyper-AF lesion. Both the (e) original and (f) synthesized RPE-melanin B-scan images reveal intraretinal RPE-melanin migration. The (g) original and (h) synthesized RPE-melanin thickness maps are similar to the (b) NIR-AF image, with RPE-melanin thickness clearly visualized in (i,j) the color-coded maps. (k) En face distribution of originalRPE70. (l) En face distribution of synRPE70.
Multimodal imaging
Multimodal imaging was performed to compare both original and synthesized RPE-melanin OCT images with NIR-AF and SW-AF images (Figs. 2 and 3). NIR-AF images (785-nm excitation, emission > 800 nm) and SW-AF images (488-nm excitation, emission > 500 nm) were acquired using an HRA2 system (Heidelberg Engineering, Heidelberg, Germany) and saved as eight-bit grayscale images. Retinal vasculature was manually aligned across the AF and OCT images using Adobe Photoshop version 26.3 (Adobe Systems, San Jose, CA, USA) to facilitate comparison. A retina specialist (M.M.) then subjectively assessed the distribution of hyper-AF lesions.
For eyes with PEDs, the PED volume was calculated by manually segmenting the inner boundary of the PED in each OCT B-scan. These individual segment volumes were then summed using the Cavalieri principle of stereology33 to determine the total PED volume.
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 29.0 (IBM Corp., Armonk, NY, USA). Statistical significance was defined as p < 0.05.
Results
In healthy eyes, the mean RPE-melanin thickness across the scanning area was 11.5 ± 2.5 μm (range, 6.3–16.6 μm) for the original RPE-melanin thickness map and 11.5 ± 2.3 μm (range, 7.6–16.1 μm) for the synthesized map. There was no significant difference in mean RPE-melanin thickness between the original and synthesized maps (p = 0.99, Wilcoxon signed-rank test). The original RPE-melanin thickness map showed a significant positive correlation with the synthesized map in mean RPE-melanin thickness (p < 0.0001, Pearson’s correlation coefficient = 0.95) (Fig. 4).

(a) Scatterplot showing the correlation between mean original RPE-melanin thickness and mean synthesized RPE-melanin thickness in healthy eyes, with a statistically significant positive correlation. (b) Scatterplot showing the correlation between mean original RPE-melanin thickness and mean synthesized RPE-melanin thickness in eyes with serous PEDs, also demonstrating a statistically significant positive correlation.
In eyes with serous PEDs, NIR-AF imaging revealed hyper NIR-AF lesions within the PED (Figs. 2 and 3) in 17 of the 22 eyes examined (77%). These lesions corresponded to areas of hyper SW-AF (Figs. 2 and 3); however, hyper SW-AF was partially masked in the foveal region, likely because of macular pigment. The synthesized RPE-melanin thickness maps closely resembled the original RPE-melanin thickness maps. Furthermore, both the original and synthesized thickness maps corresponded well with NIR-AF images in all patients (Figs. 2 and 3). Hyper NIR-AF lesions coincided with areas of thickened RPE-melanin, facilitating quantitative evaluation of RPE-melanin changes in hyper NIR-AF lesions using both original and synthesized thickness maps. The thickness of RPE-melanin within the PED could be easily visualized using the synthesized color-coded RPE-melanin thickness maps, similar to the original maps (Figs. 2 and 3). Synthesized RPE-melanin B-scan images, like the original B-scan images, clearly showed that thickened RPE-melanin lesions were composed of RPE-melanin accumulation at the RPE band and intraretinal RPE-melanin migration (Figs. 2 and 3). In eyes with serous PED, the mean RPE-melanin thickness in the measurement area was 15.9 ± 2.9 μm (range, 9.1–20.9 μm) for the original thickness map and 16.2 ± 2.9 μm (range, 11.6–21.3 μm) for the synthesized map. There was no significant difference in mean RPE-melanin thickness between the original and synthesized thickness maps (p = 0.40, Wilcoxon signed-rank test). The original RPE-melanin thickness map showed a significant positive correlation with the synthesized map in mean RPE-melanin thickness (p < 0.0001, Pearson’s correlation coefficient = 0.77) (Fig. 4).
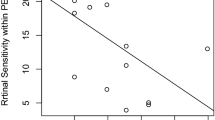
Next, the area of RPE-melanin thickened lesions (≥ 70 μm) within the PED region was examined using the original and synthesized RPE-melanin thickness maps and compared with the PED volume (Fig. 5). The mean originalRPE70 area was 0.042 ± 0.058 mm2 (range, 0.000–0.181 mm2), and the mean synRPE70 area was 0.018 ± 0.031 mm2 (range, 0.000–0.097 mm2). The mean originalRPE70 area was significantly larger than the synRPE70 area (p = 0.001, Wilcoxon signed-rank test). The synRPE70 area showed a significant positive correlation with the originalRPE70 area (p < 0.001, Pearson’s correlation coefficient = 0.92) (Fig. 5). The mean PED volume was 1.39 ± 2.16 mm3 (range, 0.003–6.93 mm3). Both the originalRPE70 area and synRPE70 area showed significant positive correlations with the PED volume (p = 0.001, Pearson’s correlation coefficient = 0.64 for originalRPE70; p = 0.036, Pearson’s correlation coefficient = 0.45 for synRPE70) (Fig. 6).

Scatterplot showing the correlation between originalRPE70 area and synRPE70 area, demonstrating a statistically significant positive correlation.

(a) Scatterplot showing the correlation between originalRPE70 area and PED volume, demonstrating a statistically significant positive correlation. (b) Scatterplot showing the correlation between synRPE70 area and PED volume, also demonstrating a statistically significant positive correlation.
Discussion
This study compared original and synthesized RPE-melanin OCT imaging in normal eyes and those with serous PED secondary to AMD. Original and synthesized RPE-melanin OCT imaging showed a strong correlation, particularly in normal eyes. In eyes with serous PED, the synthesized RPE-melanin thickness maps closely resembled NIR-AF images, consistent with prior reports using original RPE-melanin thickness maps12. This similarity highlights the complementary nature of these imaging techniques. Furthermore, in eyes with serous PED, the thickened area in the synthesized RPE-melanin thickness map correlated significantly with the PED volume, mirroring previous findings with original RPE-melanin thickness maps12. These results confirm that RPE changes in PED increase with PED size, demonstrating the utility of synthesized RPE-melanin OCT imaging for quantifying RPE activity, including intraretinal RPE migration, stacked RPE cells, and RPE dysmorphia.
In this study, the synthesized DOPU generated from standard OCT images was used for RPE-melanin OCT imaging in place of the DOPU derived from PS-OCT. The synthesized DOPU was calculated from single-polarization OCT intensity images, whereas the real DOPU requires two polarization components obtained via PS-OCT. Because the network input lacks complete polarization information, it likely relies on features in the intensity images that correlate with the DOPU, such as scattering properties34—for example, from melanin, a key source of DOPU contrast in retinal imaging18—and wavelength-dependent attenuation35. Although the exact relationship is not fully understood, these factors, which influence speckle formation, may allow the neural network model to approximate DOPU values22. The synthesized DOPU derived from these features closely resembled the actual DOPU and is considered suitable for substitution in the calculation of RPE-melanin OCT images.
Analysis of multimodal images, including synthesized RPE-melanin imaging, offers new perspectives on clinical AF findings. The similarity between the synthesized RPE-melanin thickness map and the NIR-AF image, along with the established role of the original RPE-melanin thickness map as an indicator of RPE-melanin change, suggests that synthesized RPE-melanin imaging provides a quantitative measure of RPE-associated melanin. Unlike NIR-AF, however, this synthesized imaging modality offers three-dimensional information about RPE-melanin. Both original and synthesized RPE-melanin B-scan OCT images revealed intraretinal RPE-melanin migration and accumulation at the RPE–Bruch’s membrane band in hyper NIR-AF lesions. The concurrent presence of hyper SW-AF in these lesions strongly suggests that these melanin-related findings originate from RPE changes such as intraretinal RPE migration, stacked RPE cells, and RPE dysmorphia6,12. These RPE changes are thought to reflect RPE activity4, indicating that synthesized RPE-melanin OCT imaging could be a valuable tool for evaluating RPE cellular activity in PEDs.
This study found a positive correlation between the PED volume and the area of active RPE lesions. Our prior research using PS-OCT and RPE-melanin OCT imaging, as well as a study on drusenoid PED, supports this correlation4,6,12. Several factors may contribute to RPE activation. Hypoxia, potentially resulting from reduced oxygen supply from the choriocapillaris, could play a role36. In larger PEDs, the increased distance from the choroid may hinder oxygen diffusion to the RPE4. Additionally, mechanical tension caused by architectural changes in the RPE band might be another contributing factor12. These mechanical forces could affect the extracellular matrix surrounding RPE cells, promoting RPE cell migration37. While the precise mechanism of RPE migration in serous PEDs remains unclear, both hypoxia and mechanical stress are possible causative factors in RPE changes.
In this study, the originalRPE70 area and synRPE70 area showed a strong correlation. However, the mean originalRPE70 area was significantly larger than the synRPE70 area. This difference stems from a systemic discrepancy between DOPU and synthesized DOPU values22, which is attributed to the limited performance of the neural network model used to generate the synthesized DOPU. Future improvements in the model’s architecture, learning hyperparameters, and choice of optimizer could potentially enhance its accuracy. Despite the difference in absolute values, the consistent correlation between the originalRPE70 and synRPE70 areas suggests that the deviation is systemic. Both measures are considered to reliably reflect the size of abnormal RPE lesions. Therefore, although the originalRPE70 and synRPE70 areas are not directly interchangeable, each can serve as a reasonable indicator of abnormal RPE area. In addition, it is conceivable that the gap between these values could be reduced by optimizing the FRPE threshold. However, drawing firmer conclusions will require a larger number of cases.
This study had several limitations. First, the small sample size and lack of follow-up limited the scope of RPE change evaluation in serous PEDs. Larger, longitudinal studies are needed for a more comprehensive analysis. Second, this study focused on serous PED, a specific subtype of AMD, whereas AMD encompasses various conditions involving RPE changes38. Further investigation into these diverse conditions is necessary for broader clinical application of synthesized RPE-melanin OCT imaging. Third, the detection of intraretinal RPE changes in the present study—based on the presence of melanin and lipofuscin—may have been confounded by the possible presence of infiltrating inflammatory cells39. If inflammatory cells had ingested melanosomes and lipofuscin from disintegrating RPE cells, both RPE-melanin OCT and AF imaging might have misidentified these inflammatory cells as RPE cells. Additional histopathological studies are needed to address this limitation. Fourth, although a previous study showed a monotonic relationship between DOPU and melanin17, the measurement of RPE-melanin thickness may be influenced by factors such as the incident polarization state, the DOPU kernel size18,20,28, and the melanin packing density within RPE cells40. Therefore, while RPE-melanin thickness maps correlate proportionally with actual thickness, they should be interpreted with caution because they do not represent a direct measurement. Building on our previous research12, this study focused on regions where the RPE-melanin thickness exceeded 70 μm to investigate areas of RPE activity. However, a more detailed examination of the relationship between RPE-melanin thickness and RPE activity will require a larger study cohort and correlation with histopathological findings—important directions for future research. Fifth, for future clinical applications, it is important to generate synthesized RPE-melanin OCT imaging using data from conventional commercial OCT devices. In this study, synthesized RPE-melanin OCT imaging was generated from prototype multi-contrast PS-OCT measurement data to allow direct comparison with original RPE-melanin OCT imaging. A previous study demonstrated that the synthesized DOPU can be calculated from data acquired by standard commercial retinal OCT devices (DRI-OCT Triton; Topcon), which are capable of capturing both standard OCT and OCT angiography22. Because the attenuation coefficient can be calculated from standard OCT data31, this indicates the potential for directly generating synthesized RPE-melanin OCT imaging from commercial OCT data, warranting further investigation.
In conclusion, this study demonstrated the clinical utility of synthesized RPE-melanin OCT imaging for evaluating RPE changes in serous PEDs. Synthesized RPE-melanin OCT imaging enables three-dimensional assessment of findings typically observed in AF images. Importantly, it may be possible to generate synthesized RPE-melanin OCT imaging using conventional commercial OCT systems. This suggests that implementation could be achieved through software updates to existing commercial retinal OCT devices. Synthesized RPE-melanin OCT imaging is a promising tool and may serve as a next-generation imaging modality for the clinical evaluation of macular diseases.
Data availability
Data is provided within the manuscript or supplementary information files.
References
Klein, R. & Klein, B. E. The prevalence of age-related eye diseases and visual impairment in aging: Current estimates. Invest. Ophthalmol. Vis. Sci. 54, ORSF5–ORSF13 (2013).
Zanzottera, E. C. et al. The project MACULA retinal pigment epithelium grading system for histology and optical coherence tomography in age-related macular degeneration. Invest. Ophthalmol. Vis. Sci. 56, 3253–3268 (2015).
Karampelas, M. et al. Retinal pigment epithelial detachment in age-related macular degeneration. Ophthalmol. Ther. 9, 739–756 (2020).
Curcio, C. A., Zanzottera, E. C., Ach, T., Balaratnasingam, C. & Freund, K. B. Activated retinal pigment epithelium, an optical coherence tomography biomarker for progression in age-related macular degeneration. Invest. Ophthalmol. Vis. Sci. 58, BIO211–BIO226 (2017).
Balaratnasingam, C. et al. Histologic and optical coherence tomographic correlates in drusenoid pigment epithelium detachment in age-related macular degeneration. Ophthalmology 124, 644–656 (2017).
Miura, M. et al. Evaluation of intraretinal migration of retinal pigment epithelial cells in age-related macular degeneration using polarimetric imaging. Sci. Rep. https://doi.org/10.1038/s41598-017-03529-8 (2017).
Schmitz-Valckenberg, S. et al. Fundus autofluorescence imaging. Prog. Retin Eye Res. 81, 100893. https://doi.org/10.1016/j.preteyeres.2020.100893 (2021).
Kellner, U., Kellner, S. & Weinitz, S. Fundus autofluorescence (488 NM) and near-infrared autofluorescence (787 NM) visualize different retinal pigment epithelium alterations in patients with age-related macular degeneration. Retina 30, 6–15 (2010).
Delori, F. C. et al. In vivo fluorescence of the ocular fundus exhibits retinal pigment epithelium Lipofuscin characteristics. Invest. Ophthalmol. Vis. Sci. 36, 718–729 (1995).
Keilhauer, C. N. & Delori, F. C. Near-infrared autofluorescence imaging of the fundus: Visualization of ocular melanin. Invest. Ophthalmol. Vis. Sci. 47, 3556–3564 (2006).
Lapierre-Landry, M., Carroll, J. & Skala, M. C. Imaging retinal melanin: A review of current technologies. J. Biol. Eng. https://doi.org/10.1186/s13036-018-0124-5 (2018).
Miura, M. et al. Evaluation of retinal pigment epithelium changes in serous pigment epithelial detachment in age-related macular degeneration. Sci. Rep. 11, 2764. https://doi.org/10.1038/s41598-021-82563-z (2021).
Fleckenstein, M. et al. High-resolution spectral domain-OCT imaging in geographic atrophy associated with age-related macular degeneration. Invest. Ophthalmol. Vis. Sci. 49, 4137–4144 (2008).
Ho, J. et al. Documentation of intraretinal retinal pigment epithelium migration via high-speed ultrahigh-resolution optical coherence tomography. Ophthalmology 118, 687–693 (2011).
Pircher, M., Hitzenberger, C. K. & Schmidt-Erfurth, U. Polarization sensitive optical coherence tomography in the human eye. Prog Retin Eye Res. 30, 431–451 (2011).
de Boer, J. F., Hitzenberger, C. K. & Yasuno, Y. Polarization sensitive optical coherence [invited]omography - a review [Invited]. Biomed. Opt. Express. 8, 1838–1873. https://doi.org/10.1364/boe.8.001838 (2017).
Baumann, B. et al. Polarization sensitive optical coherence tomography of melanin provides intrinsic contrast based on depolarization. Biomed. Opt. Express. 3, 1670–1683. https://doi.org/10.1364/BOE.3.001670 (2012).
Gotzinger, E. et al. Retinal pigment epithelium segmentation by polarization sensitive optical coherence tomography. Opt. Express. 16, 16410–16422. https://doi.org/10.1364/oe.16.016410 (2008).
Miura, M. et al. Evaluation of retinal pigment epithelium layer change in Vogt-Koyanagi-Harada disease with multicontrast optical coherence tomography. Invest. Ophthalmol. Vis. Sci. 60, 3352–3362 (2019).
Azuma, S. et al. Pixel-wise segmentation of severely pathologic retinal pigment epithelium and choroidal stroma using multi-contrast Jones matrix optical coherence tomography. Biomed. Opt. Express. 9, 2955–2973. https://doi.org/10.1364/boe.9.002955 (2018).
Chatzimichail, E. et al. Transforming the future of ophthalmology: Artificial intelligence and robotics’ breakthrough role in surgical and medical retina advances: A mini review. Front. Med. 11, 1434241. https://doi.org/10.3389/fmed.2024.1434241 (2024).
Makita, S., Miura, M., Azuma, S., Mino, T. & Yasuno, Y. Synthesizing the degree of polarization uniformity from non-polarization-sensitive optical coherence tomography signals using a neural network. Biomed. Opt. Express. 14, 1522–1543. https://doi.org/10.1364/boe.482199 (2023).
Sun, Y., Wang, J., Shi, J. & Boppart, S. A. Synthetic polarization-sensitive optical coherence tomography by deep learning. NPJ Digit. Med. 4, 105. https://doi.org/10.1038/s41746-021-00475-8 (2021).
Le, T. D. et al. Synthetic polarization-sensitive optical coherence tomography using contrastive unpaired translation. Sci. Rep. https://doi.org/10.1038/s41598-024-82839-0 (2024).
Makita, S. et al. Clinical prototype of pigment and flow imaging optical coherence tomography for posterior eye investigation. Biomed. Opt. Express. 9, 4372–4389. https://doi.org/10.1364/BOE.9.004372 (2018).
Azuma, S. et al. Clinical multi-functional OCT for retinal imaging. Biomed. Opt. Express. 10, 5724–5743. https://doi.org/10.1364/BOE.10.005724 (2019).
Makita, S., Kurokawa, K., Hong, Y. J., Miura, M. & Yasuno, Y. Noise-immune complex correlation for optical coherence angiography based on standard and Jones matrix optical coherence tomography. Biomed. Opt. Express. 7, 1525–1548. https://doi.org/10.1364/boe.7.001525 (2016).
Makita, S., Hong, Y. J., Miura, M. & Yasuno, Y. Degree of polarization uniformity with high noise immunity using polarization-sensitive optical coherence tomography. Opt. Lett. 39, 6783–6786 (2014).
Bennett, A. G., Rudnicka, A. R. & Edgar, D. F. Improvements on littmann’s method of determining the size of retinal features by fundus photography. Graefes Arch. Clin. Exp. Ophthalmol. 232, 361–367 (1994).
Ronneberger, O., Fischer, P. & Brox, T. U-Net: Convolutional networks for biomedical image segmentation. in Medical Image Computing and Computer-Assisted Intervention – MICCAI 2015 (eds Navab, N., Hornegger, J., Wells, W. M. & Frangi, F.) 234–241 (Springer International Publishing, 2015).
Vermeer, K. A., Mo, J., Weda, J. J., Lemij, H. G. & de Boer, J. F. Depth-resolved model-based reconstruction of Attenuation coefficients in optical coherence tomography. Biomed. Opt. Express. 5, 322–337. https://doi.org/10.1364/boe.5.000322 (2013).
Schindelin, J. et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 9, 676–682 (2012).
Prakash, Y. S., Smithson, K. G. & Sieck, G. C. Application of the Cavalieri principle in volume Estimation using laser confocal microscopy. Neuroimage 1, 325–333 (1994).
Karamata, B. et al. Multiple scattering in optical coherence tomography. I. Investigation and modeling. J. Opt. Soc. Am. Opt. Image Sci. Vis. 22, 1369–1379 (2005).
Merkle, C. W., Augustin, M., Harper, D. J., Glösmann, M. & Baumann, B. Degeneration of melanin-containing structures observed longitudinally in the eyes of SOD1-/- mice using intensity, polarization, and spectroscopic OCT. Transl. Vis. Sci. Technol. 11, 28. https://doi.org/10.1167/tvst.11.10.28 (2022).
Eamegdool, S. S., Sitiwin, E. I., Cioanca, A. V. & Madigan, M. C. Extracellular matrix and oxidative stress regulate human retinal pigment epithelium growth. Free Radic Biol. Med. 146, 357–371 (2020).
Hou, X. et al. Mechanical force enhances MMP-2 activation via p38 signaling pathway in human retinal pigment epithelial cells. Graefes Arch. Clin. Exp. Ophthalmol. 247, 1477–1486 (2009).
de Jong, P. T. Age-related macular degeneration. N. Engl. J. Med. 355, 1474–1485 (2006).
Tan, W., Zou, J., Yoshida, S., Jiang, B. & Zhou, Y. The role of inflammation in age-related macular degeneration. Int. J. Biol. Sci. 16, 2989–3001. https://doi.org/10.7150/ijbs.49890 (2020).
Pollreisz, A. et al. Visualizing melanosomes, lipofuscin, and melanolipofuscin in human retinal pigment epithelium using serial block face scanning electron microscopy. Exp. Eye Res. 166, 131–139 (2018).
Acknowledgements
We thank Angela Morben, DVM, ELS, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Author information
Authors and Affiliations
Contributions
Manuscript writing: K.Y., M.M.Development of PS-OCT: T.M., S.A., S.M., Y.Y.Development of analysis programs: M.M., S.A., T.S., S.M., Y.Y. Study design: K.Y., M.M.Collection, management, analysis, and interpretation of the data: K.Y., M.M., H.N.Review and approval of the manuscript: All authorsKosei Yanagida and Masahiro Miura contributed equally to this study.
Corresponding author
Ethics declarations
Competing interests
K. Yanagida has received lecture fees from Kowa, Chugai, Senju, and Santen. M. Miura has received lecture fees from Kowa, Chugai, Senju, and Santen and funding support from Santen and Alcon. H. Noma has received lecture fees from Chugai, Roche, Bayer, Novartis, Senju, Santen, and Kowa. S. Azuma and T. Mino are employees of Topcon Corporation. T. Seesan, S. Makita, and Y. Yasuno have received funding support from Topcon, Nikon, Santec, Skytechnology, Kao, and Panasonic.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yanagida, K., Miura, M., Noma, H. et al. Evaluation of retinal pigment epithelium changes in serous pigment epithelial detachment using synthesized multi-contrast polarization-sensitive optical coherence tomography. Sci Rep 15, 24304 (2025). https://doi.org/10.1038/s41598-025-09302-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-09302-6
