
Abstract
Determining the annual proportion of individuals newly diagnosed with human immunodeficiency virus (HIV) infection acquired within the preceding 130 days is essential to inform targeted prevention strategies. We assessed populations at increased risk of HIV infection and identified those with delayed diagnosis by analyzing the proportion of recent infections among newly diagnosed individuals. HIV-antibody avidity assays were performed to distinguish recent from longstanding infections among newly diagnosed cases during 2016–2023. Logistic regression analysis was used to assess risk factors among demographic and behavioral data, including age, nationality, region, transmission mode, marital status, HIV-testing purpose, and occupation. We investigated 7,545 individuals, representing 85.0% of the 8,875 newly diagnosed HIV-positive cases. The average proportion of recent HIV infections (RHIs) was 26.1%, which was higher among males (26.9%, P = 0.034), individuals aged < 30 years (38.8%, P < 0.001), and Korean nationals (27.3%, P < 0.001). Among testing purposes, blood donation screening yielded the highest proportion of RHIs (45.8%). Male sex, age < 30 years, and Korean nationality were identified as main risk factors for HIV infection. The RHI proportion serves as a key indicator of HIV prevention effectiveness in Korea and can inform development of effective prevention strategies.
Similar content being viewed by others
Introduction
Despite significant advancements in prevention programs and treatments, human immunodeficiency virus (HIV) infection remains a major global public health challenge. According to the Joint United Nations Programme on HIV/acquired immunodeficiency syndrome (AIDS) (UNAIDS) estimations, in 2023, approximately 1.3 million new HIV infections were reported worldwide, reflecting a 39% decline since 2010. Additionally, AIDS-related deaths decreased by 51%, with 630,000 deaths recorded. Currently, approximately 39.9 million people are living with HIV infection, of whom 86% are aware of their status and 77% are receiving antiretroviral therapy (ART)1. In South Korea, from 2016 to 2023, the annual number of newly reported HIV infections consistently ranged between 1,000 and 1,200 cases, demonstrating a sustained epidemic without a significant reduction in incidence. The burden of infection was disproportionately concentrated among young and middle-aged males, with males accounting for > 90% of new diagnoses and individuals aged 20 to 39 years comprising 64.1% of cases in 2023. Sexual transmission remained the principal mode of infection acquisition, with transmission through male-to-male sexual contact constituting approximately 54.3% of reported infections in 2023. The detection pathways for new cases include voluntary screening, routine medical examinations, and clinical assessments initiated in response to illness. The proportion of cases identified among foreign nationals increased markedly during the study period, rising from approximately 11.4% in 2016 to > 25% by 2023, reflecting demographic shifts during the epidemic2.
Achieving the UNAIDS 95–95–95 targets requires prioritization of early HIV detection, as timely diagnosis facilitates prompt ART initiation, viral load suppression, and reduced transmission. However, the proportion of early-stage diagnoses remains low, largely due to the asymptomatic nature of many recent infections, which contributes to silent transmission. According to UNAIDS, globally, 14% of people living with HIV (5.4 million) remain undiagnosed. In Korea, as of 2020, approximately 37.47% of people living with HIV were undiagnosed, with a median infection-to-diagnosis time of 6.96 years3. Data from the Korea HIV/AIDS Cohort Study revealed that from 2006 to 2023, 17.4% of participants had a CD4 + T-cell counts of < 200 cells/mm3 at cohort enrollment. The median CD4+ count at ART initiation was 161 cells/mm3 in 2001–2003 and 273 cells/mm3 in 2013–20154. These findings highlight the urgent need for early diagnosis and timely treatment to improve health outcomes and prevent further transmission.
In March 2024, as part of its commitment to global efforts to end AIDS by 2030, the Korea Disease Control and Prevention Agency (KDCA) announced the implementation of a 5-year program, The 2nd National Action Plan on HIV/AIDS Prevention and Control (2024–2028), aiming to halve the number of new HIV infections in South Korea by 2030, relative to 2023 levels. This plan includes key measures, such as infection prevention, active case identification, rapid and sustained treatment, and health rights assurance. Additionally, the plan emphasizes strengthening the foundation for HIV prevention and management, aligning national efforts with global objectives, while addressing local challenges5.
Testing for recent HIV infections (RHIs) using recency assays plays a crucial role in HIV surveillance and prevention, enabling targeted interventions and improving health outcomes. The World Health Organization (WHO) and UNAIDS advocate for recent infection testing algorithms (RITAs) to estimate HIV incidence and guide public health policies6,7. By incorporating recency data, countries can identify transmission hotspots and allocate resources more effectively. In the United States, programs such as the National HIV Surveillance System use advanced technologies, such as the limiting antigen avidity assay, to distinguish recent from longstanding infections. The Centers for Disease Control and Prevention (CDC) highlights their value in identifying high-transmission networks and evaluating prevention strategies, including pre-exposure prophylaxis and community-based testing8,9,10. Similarly, the United Kingdom has integrated recent infection assays into national surveillance, focusing on key populations, such as men who have sex with men (MSM) and African communities. Molecular epidemiology further supports efforts to track transmission patterns and inform HIV prevention strategies11,12.
Since 2015, the KDCA has performed confirmatory testing for early HIV diagnosis by integrating HIV-1 p24 antigen neutralization and HIV-1 RNA tests with the conventional antibody-based western blot assay. This approach utilizes HIV RNA and the p24 antigen as diagnostic biomarkers, which appear before anti-HIV antibodies fully develop. Consequently, the confirmed HIV positivity rate increased significantly from 10.3% in 2014 to 33.3% in 2017, while the proportion of indeterminate test results declined sharply. The adoption of HIV RNA testing allowed previously indeterminate cases, often diagnosed with western blot assays in cases in the acute phase of infection due to immature antibody development, to be reported as positive. This initiative is part of a broader testing enhancement policy aimed at identifying individuals in the early acute phase of HIV infection and linking them to treatment programs13.
In 2011, South Korea introduced the RITA system to implement nationwide RHI surveillance among newly diagnosed individuals. The testing methods have been continuously refined. Initially, the AxSYM/ARCHITECT HIV Ag/Ab Combo kit was used to perform avidity assays, and the BED HIV-1 Incidence Test was simultaneously employed14. Since 2013, the HIV-1 LAg-Avidity Enzyme Immunoassay (EIA) has been utilized for recency assays. To enhance the specificity of recent infection results, the RITA was applied considering CD4 count values and additional clinical information as recommended in the UNAIDS/WHO guide. A recent study reported that the average proportion of RHIs among individuals newly diagnosed as HIV-positive in 2008–2015 was 20.5%, with particularly higher proportion among younger age groups15.
To inform targeted prevention programs, enhance the precision of intervention strategies, and provide evidence to support the implementation of the 2nd National Action Plan, which includes identifying priority groups for enhanced HIV testing efforts, we investigated the proportion and characteristics of RHIs among individuals newly diagnosed during 2016–2023. Using advanced antibody avidity assays, we differentiated recent infections from longstanding infections and analyzed the associated demographic and behavioral risk factors.
Methods
Study samples
This study utilized residual serum or plasma samples used in HIV confirmatory testing that were deemed suitable for experimentation. The inclusion criteria was any specimen that tested positive with an HIV confirmatory test; however, only the initial sample from each individual was included. Specimens from individuals previously confirmed as HIV-positive, multiple samples from the same person, and anonymously tested specimens with unverifiable duplication were excluded.
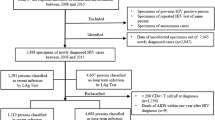
From 2016 to 2023, a total of 15,735 HIV-positive specimens in Korea, confirmed via HIV-1 p24 antigen neutralization assay, HIV-1 RNA tests, and antibody-based western blot assay, were further analyzed using the LAg-Avidity assay to determine RHI. After excluding 7,704 duplicates, previously confirmed cases, and anonymous tests, 8,031 specimens were included for recency testing, representing 90.5% of the 8,875 newly diagnosed HIV-positive cases reported during this period (Fig. 1).

Flowchart of sample inclusion and classification in the Recent human immunodeficiency virus (HIV) infection study among newly diagnosed HIV cases in South Korea during 2016–2023. Of the 15,735 HIV-positive specimens collected, 7704 were excluded due to duplication, prior HIV confirmation, or anonymous testing, leaving 8031 specimens for recency testing. Among those classified as recent infections, 80 specimens were removed based on the RITA to eliminate false recent results, and 406 specimens were excluded due to missing epidemiological data. Consequently, the final analysis included 7545 specimens. AIDS Acquired immune deficiency syndrome, RITA Recent infection testing algorithm.
HIV/AIDS is a legally notifiable disease in South Korea. The HIV/AIDS Supporting Network System is a centralized database managed by the Division of HIV/AIDS Prevention and Control at the KDCA, which maintains data on individuals confirmed to be HIV-positive. For this study, anonymized epidemiological data were obtained from the Division of HIV/AIDS Prevention and Control. The dataset included information on the following variables: date of diagnosis, age, mode of transmission, purpose of HIV testing, marital status, testing institutions, occupation, CD4 + T cell count, and HIV RNA test results.
Operational definitions
Newly identified HIV case
A case with a confirmed diagnosis of HIV infection that was not previously detected, as determined by a standardized national HIV testing algorithm13.
Recent HIV infection
An HIV infection estimated to have been acquired within approximately 118 to 142 days (mean duration: 130 days) prior to specimen collection, as determined by the Sedia HIV-1 LAg-Avidity EIA16.
Longstanding HIV infection
An HIV infection estimated to have been acquired more than 142 days prior to the date of recency testing, as determined by serological markers indicative of an established infection.
Military manpower administration (MMA) screening
In South Korea, males must complete military service at approximately 20 years of age. Since 2009, mandatory HIV testing has been one of the pre-enlistment physical. The MMA conducts this test to identify individuals with HIV and prevent transmission in military settings. Individuals with HIV are exempted from military service.
Geographical classification
Metropolitan
These are urban areas including Seoul Special City and seven metropolitan cities of South Korea, characterized by high population density, administrative autonomy, and socioeconomic concentration. These cities are hubs for governance, commerce, and culture.
Small city/rural area
These regions comprise the 10 provinces of South Korea and their subdivisions, including towns and rural areas, characterized by lower population density, diverse administrative structures, and dispersed residential and economic patterns.
HIV antibody avidity assay
The Sedia HIV-1 LAg-Avidity EIA (Sedia Biosciences Corporation, Portland, OR, USA, Cat. No. 1002) was used to identify recent HIV-1 infections among the study participants. This assay measures the avidity of HIV-1-specific IgG antibodies in plasma or serum, differentiating recent infections from long-term infections, and was performed according to the manufacturer’s instructions16. Plasma or serum specimens were diluted and added to wells coated with a limiting concentration of recombinant HIV-1 gp41 antigens. After incubation at 37 °C for 60 min, a dissociation buffer was added to elute low-avidity antibodies, while high-avidity antibodies remained bound to the antigen. Horseradish peroxidase-conjugated anti-human IgG antibodies were then added to the wells and incubated. After washing, 3,3′,5,5′-tetramethylbenzidine substrate was added to detect bound antibodies. Optical density (OD) values were measured at 450 nm using a microplate reader and normalized with an internal calibrator to calculate the normalized OD (ODn). Samples with an ODn ≤ 1.5 were classified as recent infections, based on a mean duration of recent infection of 130 (95% confidence interval [CI]: 118–142) days.
Statistical analysis
RHIs were determined using a multi-analysis algorithm integrating CD4+ T-cell counts at HIV diagnosis and AIDS-related mortality within 1 year after diagnosis. To enhance accuracy, RITA was applied to cases initially classified as RHIs based on avidity assay results. RHI cases with a CD4 count of < 200 cells/mm3 or an AIDS-related death within 1 year were excluded, without reclassification as longstanding infections, to minimize false recent results (FRRs). Of the 2,075 RHIs, 80 cases (3.9%) were excluded through application of a RITA: 67 with CD4+ counts of < 200 cells/mm3, 18 AIDS-related deaths, and 5 with both criteria. Additionally, 406 specimens were excluded due to missing socio-demographic data (e.g., sex, age, region, nationality, testing institute, or HIV testing purpose), including 379 longstanding infections and 27 recent infections. Ultimately, 7545 specimens were included in the final statistical analysis (Fig. 1).
The proportion of RHIs was calculated as the percentage of newly diagnosed HIV cases classified as recent infections each year. We analyzed HIV-testing purposes and testing institutions, including public health centers, hospitals/clinics, blood donation centers, military manpower administration, and correctional facilities. Regional distribution was examined by classifying areas as metropolitan, small city, or rural area. HIV testing purposes were categorized into the following 12 groups: outpatient clinic visits, antenatal testing, preoperative testing, health checkups, voluntary testing (named/anonymous), blood donation screening, military manpower administration screening, foreign resident screening, correctional facility admission screening, routine sexually transmitted infection (STI) screening, and contact tracing for known HIV-positive individuals. For analysis, some categories were combined.
Logistic regression analysis was used to examine the association between recent HIV infections and selected categorical variables. To assess the model assumptions, multicollinearity among independent variables was evaluated, and all variance inflation factor (VIF) values were below the commonly accepted threshold of 5. This indicated low multicollinearity and confirmed the appropriateness of including these variables in the model. Annual trends in the proportion of recent infections were assessed using the Mann–Kendall test for trends. Odds ratios (ORs) for RHIs were estimated via univariable and multivariable logistic regression. Statistical analyses were conducted using R version 4.4.0 software (R Core Team, R Foundation for Statistical Computing, Vienna, Austria), with a significance level set at P < 0.05.
Ethics approval
All experiments were reviewed and granted an exemption from ethical approval by the appropriate ethics committee (KDCA Institutional Review Board Ethics Committee; approval number: KDCA-2025-01-02-PE-01). Additionally, the requirement for obtaining informed consent from patients for this study was waived by the KDCA Institutional Review Board.
Results
Characteristics of the study population
In our study, the study population was predominantly male (Table 1). Foreign nationals accounted for less than 20% of the sample. Almost one-third of the study population was aged 30–39 years. The purpose of HIV testing was predominantly outpatient clinic visits. Notably, 70% (252/360) of those who tested HIV positive during blood donation screening were aged under 30 years of age. Male-to-male sexual contact was the mode of HIV transmission for more than one-third of the cases. Additionally, almost three-quarters of the individuals were single or unmarried.
Proportion of RHIs during 2016–2023
Among 7,545 newly diagnosed HIV cases between 2016 and 2023, RHIs accounted for 26.1% (Table 1). The proportion was higher in males than in females (P < 0.034). Age-specific analysis showed that RHIs were most prevalent in 16–19-year-olds compared to the other age groups. The proportion was significantly lower in individuals aged > 40 years than in younger age groups (P < 0.001). The proportion of RHIs among foreign nationals was significantly lower than that among Korean nationals (P < 0.001). Additionally, individuals diagnosed in metropolitan areas had a higher proportion of RHIs than those diagnosed in small cities or rural areas. Regarding transmission mode, MSM had the highest proportion of RHIs.
The proportion of RHIs varied depending on the purpose of testing. The highest proportions of RHIs were identified during testing related to blood donation. In contrast, lower proportions were found during testing related to contact tracing of known HIV-positive individuals, health checkups, preoperative testing, foreign resident screening, correctional facility admission screening, and antenatal testing (Table 1).
Notably, blood donation consistently showed the highest proportion of RHIs each year. The proportion was lower in tests where HIV infection was likely discovered incidentally, such as antenatal testing, correctional facility admission screening, foreign resident screening, and preoperative testing.
The proportion of RHIs also varied by testing institution. Blood donation centers recorded the highest proportion, followed by military manpower administration screening, public health centers, and hospitals.
Although the sample size was limited and the statistical significance was uncertain, the occupational analysis showed that students had the highest proportion of RHIs relative to other occupational groups. Service workers comprised the second highest proportion, while production workers comprised the lowest proportion among the analyzed occupational categories.
Trends in RHIs among newly diagnosed cases during 2016–2023
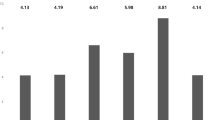
A comparative analysis of RHIs from 2016 to 2023 revealed no statistically significant year-to-year changes across any variable. In 2009, the proportion of RHIs was 16.3%, and the rate has remained above 25% since 2016. Although the overall trend has been slightly upward, 2018 (20.8%) and 2019 (22.5%) showed deviations from this pattern (Fig. 2a). RHIs were consistently approximately 10% higher in males than in females each year (Fig. 2b). Additionally, each year, foreign nationals had significantly lower proportions of RHIs than Korean nationals (Fig. 2c). Age-specific analysis revealed an inverse relationship between age and RHIs, with lower proportions observed in older age groups each year (Fig. 2d). According to testing purpose, testing related to blood donation consistently revealed the highest RHI proportion, exceeding 40% annually, while voluntary testing and military manpower administration screening also exhibited relatively high rates (Fig. 2e).

Annual proportion of recent human immunodeficiency virus (HIV) infections by (a) annual proportion of recent HIV infections, (b) sex, (c) nationality, (d) age, and (e) HIV-testing purpose among newly diagnosed HIV-positive individuals in Korea, 2016–2023. HIV Human immunodeficiency virus, RHIs Recent HIV infections
Factors associated with RHIs
The median age of individuals with RHIs was 30 (interquartile range [IQR]: 26–37) years, which was significantly lesser than the age of those with longstanding infections (36, IQR: 29–48 years). Univariate logistic regression identified several epidemiological factors that were significantly associated with RHIs, including sex, age, nationality, region, transmission mode, marital status, testing institution, and testing purpose (Table 2).
Multivariable logistic regression revealed key risk factors for RHIs. The likelihood of recent infection was higher in males than in females (adjusted OR: 1.29, 95% CI: 1.02–1.63). Younger individuals in the cohort, particularly those aged 20–29 years and those aged 30–39 years had approximately four-fold and two-fold increased odds, respectively, of having RHIs, than did those aged 60 years and older. Korean nationals were significantly more likely to have RHIs than foreign nationals (P < 0.001). Testing related to blood donation, outpatient clinic visits, and voluntary testing also showed strong associations with RHIs. The primary risk factors identified by multivariable analysis were male sex, a younger age (under 30 years), and Korean nationality, emphasizing the need for targeted prevention strategies for these high-risk groups.
Characteristics of RHIs among younger age groups (age < 30 years)
The study population included 53 individuals aged 16–19 years and 2,332 individuals in their 20 s, collectively accounting for 31.6% of all participants (Table 1). Due to the small sample size in the 16–19-year-old age group, statistical analyses were limited, and in some cases, data from both the abovementioned groups were combined. The 8-year average proportion of RHIs was 50.9% among individuals aged 16–19 years and 38.6% among those in their 20 s; both these values exceeded the overall study average of 26.1%. Among individuals in their 20 s, annual RHI proportions ranged from 31.5% in 2018 to 47.2% in 2020 (Fig. 2d), with no significant temporal trends observed.
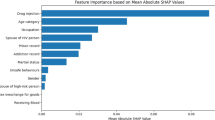
Among individuals aged under 30 years, RHIs were more prevalent among males (39.4%) than among females (26.7%) and were higher among Korean nationals (40.1%) than among foreign nationals (31.2%). The proportion was 12.7% points higher in males than in females and 8.9% points higher in Korean nationals than in foreign nationals (Fig. 3a). RHIs were most prevalent among individuals aged under 30 years who underwent testing during routine STI screening (50.0%), blood donation (49.2%), outpatient clinic visits (42.4%), preoperative testing (39.8%), contact tracing (37.5%), voluntary testing (35.5%), and military manpower administration screening (28.9%). In contrast, significantly lower RHI proportions were observed among individuals undergoing foreign resident screening (15.4%) and correctional facility admission screening (9.1%) (Fig. 3b).

Proportion of recent HIV infections by demographic and behavioral factors among newly diagnosed individuals aged 16–29 years during 2016–2023. (a) Sex, nationality, testing institute. Foreigner, foreign nationals; blood center, blood donation center; public center, public health center; military, manpower administration; prison, correctional facility (b) Testing purpose. Voluntary testing includes both named and anonymous voluntary testing. Outpatient visits include outpatient clinic visits and antenatal testing. Prisoner screening, correctional facility admission screening; military screening, military manpower administration screening; foreigner screening, foreign resident screening; HIV-positive partner, contact tracing of known HIV-positive individuals. HIV Human immunodeficiency virus, RHIs Recent HIV infections
Discussion
In this study, we analyzed the proportion of RHIs among 7,545 individuals newly diagnosed with HIV in South Korea during 2016–2023, which represented 85% of the 8,875 cases reported to the KDCA during the study period. Among this study population, the average proportion of RHIs was 26.1%, reflecting a 5.6% increase compared to 20.5% reported for the period 2008–2015. This trend appears to be associated with the rising number of newly diagnosed HIV cases in South Korea annually, which increased from approximately 900 to 1,100–1,200 cases since 2013. Furthermore, our data suggest that HIV diagnostic testing has become more widely implemented within certain high-risk populations. A logistic regression model was employed to identify independent demographic and behavioral risk factors associated with RHIs. This revealed that male sex, younger age (under 30 years), Korean nationals, and specific testing purposes such as blood donation and voluntary testing, were significantly associated with RHIs.
The high proportion of RHIs in certain high-risk groups suggests ongoing transmission and frequent HIV testing behaviors. For example, in Singapore, MSM are known to undergo testing more frequently due to heightened awareness attributed to the effectiveness of government-led sexual health campaigns17.
Findings from recent infection surveys serve as critical indicators for enhancing early HIV detection and improving diagnostic strategies. In our study, the following groups had lower proportions of RHIs: females (17.1%), foreign nationals (20.3%), and individuals aged 40 years or older (17.4%, 14.4%, and 13.7% among individuals in their 40 s, 50 s, and 60 s or older, respectively). The lower proportion of RHIs among older age groups may be attributable to decreased engagement in high-risk sexual behaviors or limited utilization of HIV screening services. Conversely, younger individuals had a significantly higher probability of RHIs, with those aged 16–19 years having a 5.5-fold higher odds and those aged 20–29 years having a 4.2-fold higher odds of having RHIs compared to individuals aged 60 years and older. The highest RHI proportion according to the HIV testing purpose was observed in the blood donation group (45.8%). This may be explained by the fact that individuals under the age of 30 years accounted for 70% of the blood donation group in this study. Furthermore, since blood donation centers perform HIV-1 RNA testing for all samples right from the initial stage of HIV screening, they can diagnose HIV infection earlier than institutions that conduct only antigen/antibody testing. The high RHI proportion in the routine STI screening group (31.5%) likely reflects regular annual HIV testing, as this group is legally required to undergo periodic screening.
The lower proportion of RHIs among females may be explained by their relatively small representation among newly diagnosed HIV cases in South Korea, where they account for less than 10% of all new diagnoses. Overall, the risk factors identified in the recent infection analysis align with the epidemiological profile of HIV incidence in Korea. Specifically, these findings were consistent with the 2023 HIV/AIDS notification surveillance data, which indicated that 89.9% of newly diagnosed cases were males, while 64.1% of cases were reported among individuals aged in their 20 s and 30 s.
Global efforts to monitor RHIs have revealed significant regional and population-based variability, emphasizing the need for targeted interventions. In the United States, recent infections account for 10–20% of newly diagnosed cases, with higher rates observed among MSM and younger individuals. Similarly, in the United Kingdom, 20–25% of new diagnoses are classified as RHIs, particularly among MSM and African communities. The notably low proportion of recent HIV infections among females in South Korea reflects a pattern seen in countries where the majority of cases occur among males, especially MSM, including the UK, Germany, and Singapore, and likely influenced by differences in transmission dynamics, gender composition, and sociocultural factors. Additional studies from countries such as Ireland, Ethiopia, and Kenya further emphasize the importance of recency testing in identifying transmission trends and informing public health strategies18,19,20,21,22,23,24.
Despite advancements in HIV surveillance, gaps in testing coverage remain, particularly among racial and ethnic minorities in the United States, where late diagnoses continue to be a challenge. Recency testing has played a crucial role in facilitating earlier care and reducing community-level transmission risks. In the United Kingdom, integrating new HIV diagnoses and late HIV diagnoses data into national surveillance systems has optimized resource allocation in high-prevalence areas, supporting progress toward the UNAIDS 95–95–95 targets25.
Beyond surveillance, recent infection testing has significant clinical implications. Acute and early HIV infections are associated with high viral loads and increased transmission risk. Individuals in the early stage of infection are up to 26 times more likely to transmit HIV than those with chronic infection. Notably, 20–50% of total HIV transmissions occur during this early period26. Early identification and treatment can reduce transmission risk, slow disease progression, and prevent complications. The success of public health interventions in the United States and United Kingdom demonstrates the potential for other countries to adopt similar strategies to enhance HIV prevention and control.
The proportion of non-Korean individuals among all HIV cases in South Korea has steadily increased, from 19.5% in 2020 to 20.7% in 2021, 22.6% in 2022, and 25.5% in 2023. Despite this upward trend, the relatively low proportion of recent infections among non-Korean individuals observed in this study suggests that this group has limited access to HIV testing, potentially leading to a higher prevalence of undiagnosed cases. Addressing these disparities requires targeted policies and programs that promote voluntary HIV testing among non-Korean populations, to facilitate earlier diagnosis and reduce transmission risk.
This study had some limitations. First, to minimize the impact of FRRs when applying a RITA, we adhered to WHO recommendations by incorporating CD4 + T-cell counts and data on individuals who died within 1 year of diagnosis. However, CD4 + T-cell data were available for only 5,607 (74.5%) of the 7,545 samples included in the study, indicating that CD4 test results were limited to these samples. Consequently, some false positives may not have been fully excluded. Nonetheless, all samples analyzed in this study were the first specimens collected from individuals newly diagnosed with HIV, ensuring that they were unaffected by antiretroviral therapy. Second, the WHO/UNAIDS technical guidelines recommend calculating the “proportion recent” by dividing the number of recent infections by the total number of individuals at risk for HIV, which includes both recent infections and those testing HIV-negative, rather than using only the total number of newly diagnosed cases7,27. However, due to the study design, which focused exclusively on confirmed positive samples, we were unable to incorporate data on individuals who tested HIV-negative in South Korea. This limitation may affect the generalizability of our findings to the broader population. Third, the insufficient epidemiological information associated with certain variables posed challenges in interpreting the underlying causes and environmental changes related to the RHI results. Notably, approximately 25% of cases were reported with unknown or non-response transmission modes, limiting the comprehensiveness of the data and complicating accurate interpretation of transmission dynamics. This limitation not only affects the reliability of our findings and the precision of epidemiological inferences but also raises concerns about potential stigma-related reporting biases. Participants may have been reluctant to disclose their transmission mode due to stigma or social sensitivity, particularly for categories such as MSM or other high-risk exposures. Furthermore, potential sampling constraints, including representativeness of the study population and associated biases, warrant careful consideration. To improve data quality and strengthen the generalizability of the findings, it is essential to implement more systematic data collection strategies, including enhanced training of personnel managing HIV epidemiological data and refinement of data collection protocols. Despite these constraints, this study holds significant value as it was based on national data covering 7,545 (85%) of the 8,875 newly diagnosed HIV cases reported in South Korea during the study period. This extensive coverage enhances the reliability of our findings and their applicability to understanding the HIV epidemic in Korea.
Conclusion
Between 2016 and 2023, 26.1% of newly diagnosed HIV cases were detected within 130 days of HIV infection acquisition (median: 118–142 days), indicating that many individuals remained unaware of their infection during the early phase. Expanding education and outreach programs is essential to encourage regular HIV testing among high-risk groups.
This study identified young Korean males aged less than 30 years as the most at-risk group for HIV infection, while foreign nationals were more likely to experience delayed diagnosis. Improving access to HIV testing for these populations is crucial to reducing transmission risks and strengthening prevention efforts. Under Korea’s 2nd National Action Plan on HIV/AIDS Prevention and Control (2024–2028), the KDCA is expanding HIV testing initiatives for key populations, including MSM, people who inject drugs, partners of individuals with HIV, and foreign nationals. These efforts include enhancing access to anonymous and rapid testing at public health centers and conducting targeted education campaigns. Collaboration with non-governmental organizations serving sexual and gender minorities has further expanded testing coverage. The plan emphasizes prevention, case finding, early treatment, stigma reduction, and antibody avidity-based monitoring to assess intervention outcomes. These efforts align with global goals and support the objective of ending AIDS by 2030. This study underscores the value of recency assays in HIV epidemic control and provides evidence for their importance in public health strategies.
Data availability
Data are available from the corresponding author upon reasonable request and is subject to restrictions.
References
Joint United Nations Programme on HIV/AIDS (UNAIDS). Global HIV & AIDS statistics-fact sheet. UNAIDS https://www.unaids.org/en/resources/fact-sheet (2024).
Kim, K., Kim, S., Kim, T. & Yu, J. HIV/AIDS Notifications in Korea, 2023. Public Health Wkly. Rep. 17, 1737–1749; https://doi.org/10.56786/PHWR.2024.17.41.3 (2024).
Lee, E., Kim, J., Lee, J. Y. & Bang, J. H. Estimation of the number of HIV infections and time to diagnosis in the Korea. J. Korean Med. Sci. 35, e41. https://doi.org/10.3346/jkms.2020.35.e41 (2020).
Ryou, S., Lee, J. G., Jeong, O., Go, M. J. & Kim, J. Long term follow-up of HIV patients: Insight and achievement from a 17 years ‘Korea HIV/AIDS cohort study’ (2006–2023). Public Health Wkly. Rep. 17, 1720–1736. https://doi.org/10.56786/PHWR.2024.17.41.2 (2024).
Kim, S., Kim, E. & Yu, J. The 2nd national action plan on HIV/AIDS prevention and control (2024–2028). Public Health Wkly. Rep. 17, 2001–2010. https://doi.org/10.56786/PHWR.2024.17.46.3 (2024).
UNAIDS. Recent infection testing algorithm technical update—applications for HIV surveillance and programme monitoring. UNAIDS https://www.unaids.org/en/resources/documents/2018/infection_testing_algorithm (2018).
UNAIDS and World Health Organization (WHO). Using recency assays for HIV surveillance: 2022 technical guidance. UNAIDS/WHO https://www.who.int/publications/i/item/9789240064379 (2022).
Wei, X. et al. Development of two avidity-based assays to detect recent HIV type 1 seroconversion using a multisubtype gp41 recombinant protein. AIDS Res. Hum. Retroviruses. 26, 61–71. https://doi.org/10.1089/aid.2009.0133 (2010).
Duong, Y. T. et al. Detection of recent HIV-1 infection using a new limiting-antigen avidity assay: Potential for HIV-1 incidence estimates and avidity maturation studies. PLoS ONE 7, e33328. https://doi.org/10.1371/journal.pone.0033328 (2012).
The Centers for Disease Control and Prevention. CDC Publishes New HIV Surveillance Reports: HIV Surveillance Supplemental Report: Estimated HIV Incidence and Prevalence in the United States, 2018–2022. CDC https://www.cdc.gov/nchhstp/director-letters/cdc-publishes-new-hiv-surveillance-reports.html (2024).
Georgios, K. N. & Andreas, G. T. Diagnostics recent HIV infection: Diagnosis and public health implications. Diagnostics. 12, 2657. https://doi.org/10.3390/diagnostics12112657 (2022).
Public health England (the UK Health Security Agency). Progress towards ending the HIV epidemic in the United Kingdom 2018 report. The UK Health Security Agency https://assets.publishing.service.gov.uk/media/5d3afad8e5274a401520b532/Progress_towards_ending_the_HIV_epidemic_in_the_UK.pdf. (2019).
Wang, J. S. et al. Effect of a confirmatory testing algorithm on early acute HIV diagnosis in Korea. Medicine 100, e25632. https://doi.org/10.1097/MD.0000000000025632 (2021).
Wang, J. S., Kee, M. K., Choi, B. S. & Kim, S. S. Modification of AxSYM human immunodeficiency virus assay to identify recent human immunodeficiency virus infections in Korean human immunodeficiency virus-positive individuals. Osong Public Health Res. Perspect. 6, 184–119. https://doi.org/10.1016/j.phrp.2015.06.002 (2015).
Yoo, M. et al. Characteristics of recent HIV infection among individuals newly diagnosed as HIV-positive in South Korea (2008–2015). Sci. Rep. 12, 10515. https://doi.org/10.1038/s41598-022-13953-0 (2022).
Sedia Biosciences Corporation. Sedia HIV-1 LAg-Avidity EIA. Cat. No. 1002, Oregon USA. (2018/2022).
Ang, L. W. et al. Epidemiological factors associated with recent HIV infection among newly-diagnosed cases in Singapore, 2013–2017. BMC Public Health 21, 430. https://doi.org/10.1186/s12889-021-10478-5 (2021).
Schwarcz, S. et al. Characteristics of persons with recently acquired HIV infection: application of the serologic testing algorithm for recent HIV seroconversion in 10 US cities. J. Acquir. Immune Defic. Syndr. 44, 112–115. https://doi.org/10.1097/01.qai.0000247228.30128.dc (2007).
Fisher, M. et al. Serological testing algorithm shows rising HIV incidence in a UK cohort of men whohave sex with men: 10 years application. AIDS 21, 2309–2314. https://doi.org/10.1097/QAD.0b013e3282ef9fed (2007).
Alexandra, H. et al. Surveillance of recent HIV infections among newly diagnosed HIV cases in Germany between 2008 and 2014. BMC Infect. Dis. 17: 484
O’Donnell, K., Moran, J. & Igoe, D. Monitoring recent HIV infection in Ireland, 2018. Dublin: HSE HPSC; 2020. HSE Health Protection Surveillance Centre https://www.hpsc.ie/a-z/hivandaids/hivdataandreports/2018reports/HIV_2018_recentinfection.pdf (2020).
Nigatu, A. et al. Recent HIV infection and associated factors among newly diagnosed HIV cases in the Southwest Ethiopia regional state: HIV case-based surveillance analysis (2019–2022). BMC Infect. Dis. 24, 609. https://doi.org/10.1186/s12879-024-09481-z (2024).
Tefera, A. et al. Recent HIV infection among newly diagnosed cases and associated factors in the Amhara regional state, Northern Ethiopia: HIV case surveillance data analysis (2019–2021). Front. Public Health. 10, 922385. https://doi.org/10.3389/fpubh.2022.922385 (2022).
Young, P. W. et al. HIV incidence, recent HIV infection, and associated factors, Kenya, 2007–2018. AIDS Res. Hum. Retroviruses. 39, 57–67. https://doi.org/10.1089/AID.2022.0054 (2023).
GOV.UK, UK Health Security Agency. Official Statistics: HIV testing, PrEP, new HIV diagnoses and care outcomes for people accessing HIV services: 2024 report. UK Health Security Agency https://www.gov.uk/government/statistics/hiv-annual-data-tables/hiv-testing-prep-new-hiv-diagnoses-and-care-outcomes-for-people-accessing-hiv-services-2024-report (2024).
William, C. M., Nora, E. R., Sarah, E. R. & Kimberly, A. Role of acute and early HIV infection in the sexual transmission of HIV. Curr. Opin. HIV AIDS. 5, 277–282 (2010).
Godin, A. et al. Inferring population HIV incidence trends from surveillance data of recent HIV infection among HIV testing clients. AIDS 35, 2383–2388 (2021).
Acknowledgements
This research was supported by the Korea Disease Control and Prevention Agency (grant No. 6331-301-210)
Author information
Authors and Affiliations
Contributions
J.-S.W. and M.-G.H. designed and conceived the study, and M.-G.H. supervised all aspects of its implementation. J.-S.W. wrote the first draft of the manuscript. E.J.K., G.K., Y.J.L., H.G.H., and M.K. performed the LAg Avidity assays. N.R.J. and T.-Y.H. analyzed the data. S.K. and H.M.K. coordinated funding for the project. K.K., S.K., and J.Y. operated the national HIV/ AIDS database. All authors have edited and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
All authors hereby declare that all experiments were reviewed and granted an exemption from ethical approval by the appropriate ethics committee (KDCA Institutional Review Board Ethics Committee; approval number: KDCA-2025-01-02-PE-01). Additionally, the requirement for obtaining informed consent from patients for this study was waived by the KDCA Institutional Review Board.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, JS., Kim, E.J., Kim, G. et al. Recent HIV infections and associated risk factors among newly diagnosed individuals in South Korea (2016–2023). Sci Rep 15, 26229 (2025). https://doi.org/10.1038/s41598-025-10444-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-10444-w
Keywords
This article is cited by
-
Trends in HIV testing and Seroprevalence among key populations at public health centers in South Korea, 2011–2023: a nationwide analysis
BMC Public Health (2025)
-
Association of demographics and psychological barriers with late presentation of HIV among men who have sex with men in Chengdu, China
Scientific Reports (2025)
