
Abstract
The study examined the effect of a 12-week Bungy Pump Training (BPT) program on cardiorespiratory fitness (CRF), metabolic syndrome (MetS) factors and body composition in postmenopausal women (PW). Fifty-six participants were assigned to the BPT group (n = 30) and the Daily Activity (DA) group (n = 26). The BPT group completed 60-minute sessions 3 times a week, and the DA group performed daily activities. Body composition, maximum oxygen uptake (VO2max), heart rate, blood pressure (BP), glucose and lipid profiles were assessed at baseline and post-intervention. In the CRF and MetS factors, BPT produced a significant group-by-time interaction for VO2max, with increases of 7% (L/min) and 9% (mL/kg/min) compared with DA. Time effects in BP and total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol were observed in both groups, but significant within-group improvements occurred only in BPT. In body composition, significant interactions were found for basal metabolic rate (BMR), visceral fat area (VFA), percent body fat (PBF), and body fat mass (BFM), with BMR increasing by 2% and VFA, PBF, and BFM decreasing by 7%, 5%, and 7%, respectively. Both groups showed improvements in MetS factors over time, whereas the 12-week BPT performed 3 times a week was superior only for VO2max and specific body composition (BMR, VFA, PBF, and BFM). This finding supports considering BPT as a non-pharmacological intervention for PW.
Trial registration: Clinical Trials. NCT06781541
Similar content being viewed by others


Introduction
By 2040, global female life expectancy is projected to increase by 4.4 years (2.1–6.4 years) to 79.7 years (77.4–81.8 years)1. Aging is accompanied by metabolic risks associated with worsening cardiovascular disease (CVD), such as high blood pressure, high body mass index (BMI), and high fasting glucose1. CVD is the leading cause of death globally1,2, with total incidence increasing from 271 million cases (257–285) in 1990 to 523 million cases (497–550) in 20192. Postmenopausal women (PW) experience a decline in estrogen levels3 and an increased risk of CVD with age4, potentially exceeding that of men5. The American Heart Association (AHA) found that 70% of PW will develop CVD6, experiencing a low level of cardiorespiratory fitness (CRF)7,8, an increased risk of metabolic syndrome (MetS)9,10 and an adverse body composition11,12.
Adverse CRF changes are mainly characterized by decreased maximum oxygen uptake (VO2max) and increased resting heart rate (HR)7,13. MetS factors are reflected in unfavourable changes on blood pressure (BP), glucose, and lipid metabolic indices14,15,16. Body composition is mainly an increase on body weight (BW)17, and body fat18 and a decrease on lean body mass19, and basal metabolic rate (BMR)20. Therefore, improving CRF, MetS factors, and body composition in PW is important to prevent CVD and reduction in mortality risk.
Physical exercise such as aerobic exercise, muscle strengthening, flexibility, and balance21 may prevent CVD for the elderly by favourably improving blood lipids, BW and hypertension14,22. The results of emerging physical exercise modes were similar, such as High-Intensity Interval Training, Pilates, Tai chi and yoga22. For PW, inappropriate physical activities may worsen their musculoskeletal and cardiovascular health22. Compared to walking, Nordic Walking (NW) is a safe and popular physical exercise among the elderly with proven health benefits23,24. The NW technique with poles involves circular, repetitive and alternative movements of the whole body25. In PW, NW has been shown to be effective in improving CRF (VO2max23, HR23), MetS factors (BP23, basic lipid15,26, fasting blood glucose26, and body composition (BW23, fat mass23.
To improve the effects of NW, a new form of NW has been produced by combined aerobic and strength training (CT) - Bungy Pump Training (BPT)27. CT has been shown to improve muscular strength, balance, and bone health in PW28,29,30. It also contributes to healthier CRF, MetS, and body composition3,30,31. CT is considered a simple and effective approach to enhancing overall health in PW. BPT is performed using a modified pole that contains a built-in resistance shock absorber. The elastic band between the two permanent elements in the poles allows for additional resistance, increasing the intensity of training and calorie consumption27. The study shows that an 8-week BPT program led to improvements on the femur strength index and VO2max but not BP in PW32,33. A 12-week BPT program induced improvements on cognitive functions and physical performance in the elderly. In contrast, no glucose homeostasis or lipid profile changes were found34. Compared with NW, the 8-week BPT resulted in greater improvements in carbohydrate and lipid metabolic indices and cardiorespiratory efficiency in PW32,35. In short, BPT improves physical performance in PW but appears to differ in glucose homeostasis or lipid profile. Most BPT studies have been limited by small sample sizes, short trial durations and lack of a control group. In addition, CRF strongly predicts the risk of developing CVD36 and MetS factors have been linked to elevated risk of CVD16, but little has been done regarding CRF and MetS in PW. Given the growing popularity of BPT among the elderly in Europe37, further studies are warranted to evaluate its impact on CRF, MetS, and body composition in this population.
Therefore, the study aimed to examine the effects of BPT on CRF, MetS factors, and body composition in untrained PW with no previous experience of this sport. We hypothesised that the participants’ CRF, MetS factors, and body composition would improve after the intervention.
Materials and methods
Study design
The study was registered with ClinicalTrials.gov (NCT06781541), which consisted of a non-randomised controlled trial with two parallel groups: the BPT group and the Daily Activity (DA) group. Allocation to groups was determined using a geographic location-based quasi-randomisation method. This research combined pretest & posttest with a repeated measures design component to capture within-subject changes over time with a quasi-experimental study to assess between-group differences. Participants underwent the same baseline and post-intervention assessments in the laboratory, including body composition, CRF, and MetS factors. Participants in the BPT group were monitored during all training sessions, while DA participants were monitored for 7 consecutive days. Participants were instructed not to alter their diet throughout the entire duration. The study design is detailed in Fig. 1. This study received approval from the Bioethics Committee of the District Medical Chamber in Gdańsk in compliance with the Declaration of Helsinki under procedure number KB-5/22. All the participants were informed about the intervention and possible adverse events before the commencement of the trial and signed an informed consent form.

Study design.
Participants
Invitations to participate in the study were sent out at the University of the Third Age (UTA) in Gdansk and Sopot. Recruitment was also carried out in clinics, churches and on local bulletin boards. Untrained PW aged 61–88 years and in menopause for at least 12 months were invited to participate in this study. Exclusion criteria included participation in any structured or regular physical exercise program (e.g., aerobic training, resistance training, or NW) or performed more than 150–300 min of moderate-intensity aerobic activity (or an equivalent amount of vigorous-intensity activity) per week during the six months prior to enrollment; prior experience with BungyPump or similar pole-based exercise modalities; uncontrolled hypertension, rheumatoid arthritis, type 2 diabetes, current or previous antibiotic and/or antifungal therapy within the past 4 weeks, and contraindications to physical exercise. The screening process was conducted in two sequential stages. The first stage involved a self-reported questionnaire used to assess age, menopausal status (defined as the absence of menstruation for at least 12 consecutive months), and general health. Participants who passed the pre-screening proceeded to a Comprehensive Medical Assessment to further evaluate their eligibility for BPT. This assessment included a detailed review of comorbidities, current medications, and prior physical activity levels, along with the evaluation of health records accessed through the facility’s medical information system.
Sample size calculation
A power calculation was conducted to estimate the sample size using G * Power (Version 3.1). Based on data published in previous research, the effect size of the primary outcome measure (relative VO₂max) was large (Cohen’s d = 1.09)23. A sample size calculation for the main study indicated that 23 participants per group would be required to yield a power of 0.95 in a 2-sided test with a 5% level of α = 0.05.
Intervention
The training program was based on the principles of the health-related training process and the American College of Sport Medicine21 guidelines for elderly in good health conditions and lasted 12 weeks (3 weekly 60-minute for 36 sessions). Each training session was performed three times a week, on Mondays, Wednesdays, and Fridays from 9:00 to 10:00 a.m. The specific schedule was as follows: 10 min of warm-up, 40 min of BPT training, and 10 min of relaxation. Participants in the BPT group participated in training sessions using built-in resistance shock absorber of 4 kg (Slimline Bungy Pump, Sports Progress International AB, Sweden), Participants in the BPT group were trained by a Bungy Pump trainer (Polish Nordic Walking Federation-qualified) and at least two assistants. BPT emphasis was placed on performing correct Bungy Pump techniques. The 4 kg resistance was selected because it is recommended for older adults and beginners due to its safety and effectiveness. Although the resistance remained constant, progression was achieved by gradually increasing the complexity and variety of exercises, along with controlled enhancements in movement coordination, balance demands, and the number of repetitions (ranging from 8 to 12). Each training was performed at 75%–85% maximal heart rate (HRmax). The maximum heart rate calculation method: HRmax= 206 − 0.88 × age38. The intensity of sessions during training was monitored using Polar V-800 sports testers (Polar Electro Oy, Finland), and instructors adjusted walking speed based on heart rate and participants’ perceived exertion to ensure safe and effective training. During the training sessions, the distance marched was gradually increased from 2.8 to 3.6 km and the average heart rate (HRmean) for the intensity of the exercise was 114 ± 14 bpm, corresponding to 79 ± 9.49% HRmax.
Participants performed two 60-minute sessions of correct marching technique before the start of the training. At the beginning of each training session, the participants warmed up for approximately 10 min including a versatile exercise with the Bungy Pump pole. The 40-minute BPT consists of approximately 10 min of marching alternating with approximately 5 min of strength and balance training. Strength and balance training was based on the elastic resistance of the Bungy Pump pole for 8–12 repetitions of each movement. The approximately 10-minute cool-down was completed by static and dynamic flexibility exercises using the Bungy Pump pole.
The DA group performed daily activities without additional intervention. Participants in the DA group were involved in normal daily activities appropriate to their age range. The DA group received instructions to refrain from engaging in structured physical training sessions. However, based on ethical and health considerations, participation in individual daily physical activities or an overall increase in physical activity level was permitted.
Participants were required to report their involvement in such activities.
Participants were required to report their involvement in daily activities, and their physical activity levels were monitored for seven consecutive days using Polar V800 sport testers (Polar Electro Oy, Finland), a duration consistent with internationally accepted standards.
Measures and outcomes
All the participants were evaluated at baseline and after intervention. The evaluations were performed on two separate days. On the first day, blood samples were collected and preliminary analyses of body composition and dietary records were conducted. On the second day, physical and psychological tests were performed at the Sports Exercise Laboratory in the Gdansk University of Physical Education and Sport. Biological materials were frozen and subsequently tested by contractors at the Sports Genetics Laboratory of Gdansk University of Physical Education and Sport. Given the independence of the intervention and evaluation, the evaluator used a blinded test during the evaluation.
Primary outcome
Fasting blood samples were collected between 6:30 and 7:30 a.m. after a minimum of 12 h of fasting. The samples were used to assess glucose, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), non-high-density lipoprotein cholesterol (non-HDL-C), aspartate aminotransferase (AST), and alanine aminotransferase (ALT)39. Analyses were performed using Abbott diagnostic assays on the Abbott Alinity c platform, following IFCC-referenced spectrophotometric procedures. After centrifugation, serum absorbance was measured at defined wavelengths to quantify lipid and cholesterol concentrations. AST and ALT activities were determined via enzymatic spectrophotometry: AST catalyzes aspartate and α-ketoglutarate, while ALT catalyzes alanine and α-ketoglutarate, with changes tracked by NADH consumption at 340 nm. The Alinity c system demonstrated metrological traceability to IFCC reference procedures and exhibited acceptable measurement uncertainty for AST and ALT40. Glucose concentration was measured via a glucose-oxidase/peroxidase reaction, producing a color change proportional to glucose amount and quantified spectrophotometrically41. Analyses were conducted at the beginning and end of the training program under identical analytical conditions (calibration, temperature control, quality assurance), ensuring high repeatability and data reliability.
Heart rate and blood pressure: resting HR, SBP and DBP were assessed using the Omron HEM-907XL device (Omron Healthcare, Inc., IL, USA) after the participant had rested in a supine position for 15 min in a quiet, temperature-controlled room (20 °C to 22 °C).
VO2max was estimated using the EKBLOM-BAK test in a laboratory environment. The EKBLOM-BAK submaximal cycle ergometry test, performed in accordance with standard procedures, was used to estimate VO2max42, and was selected for its safety and validated application in older adults, especially in elderly women43, despite not being mode-specific to the walking-based intervention. The testing procedure begins with the calibration of the ergometry cycle according to standard procedures, followed by verifying that the participant has adhered to the pre-test conditions, such as avoiding heavy meals, alcohol, smoking, and intense physical activity for at least 3 h before the test. Prior to starting the test, the seat and handlebars of the cycle should be properly adjusted, and the participant should be introduced to the Borg’s Rating of Perceived Exertion (RPE) scale.
In the first phase of the test, the participant begins pedaling for 4 min at a standard workload (60 rpm), previously selected to achieve a heart rate of 110–140 bpm. After the 4-minute period, the average heart rate is measured based on four time points (3:15, 3:30, 3:45, and 4:00), and the results are averaged. The resistance is then increased to a higher workload, chosen to allow the participant to further elevate their heart rate and reach the target range. After 2 min at the higher workload, the participant is asked to rate their perceived exertion using the RPE scale. If the RPE is less than 10, the resistance is increased by 1 kp, and the RPE is measured again. If the RPE is between 10 and 11, the resistance is increased by 0.5 kp. If the RPE is between 12 and 16, the resistance remains unchanged, and the test continues at the same intensity. If the RPE exceeds 17, the test is stopped, and the participant rests for 20 min before attempting the test again at a lower intensity.
After completing the test, the average heart rate during the 4 min at the higher intensity is measured again, and the participant is asked to rate their overall exertion using the RPE scale. Based on the data collected during the test, VO2max is estimated using a mathematical formula42:
VO2max = 4.98196–2.88618 (ΔHR/ΔPO) + 0.65015 (sex) – 0.01712 (age),
where for sex male = 1 and female = 0, HR - heart rate, PO - power output.
Alternatively, an online application is available to calculate VO2max based on the test results. The application used to calculate the VO2max during the Ekblom-Bak test was downloaded from the website of the Swedish School of Sport and Health Sciences (https://www.gih.se/english/research/laboratories/the-astrand-laboratory/the-ekblom-bak-test), last accessed on June 25, 2025. The test is designed for individuals aged 20 to 86 years and provides a reliable estimation of VO2max44.
Secondary outcome
Height was assessed with the participant standing upright barefoot. BW, PBF, VFA, and regional lean mass were assessed by the Octapole Bioimpedance InBody 720 analyzer (Biospace, Seoul, South Korea) following standard protocols. Participants wore light clothing without shoes during the measurements. It employs eight contact electrodes on the hands and feet to independently analyze five body segments (left and right upper limbs, trunk, and left and right lower limbs) at multiple frequencies (1, 5, 50, 250, 500, and 1,000 kHz). BMI is calculated as weight/height2 (kg/m2).
Statistical analyses
Data were expressed as mean ± standard deviation (SD), and data were analysed using SPSS (SPSS Version 27.0, IBM, Chicago, USA). GraphPad Prism 9 (GraphPad Software, San Diego, CA) was used for figure making. Data normality was examined using the Shapiro-Wilk test and visual histogram. Descriptive statistics were used to describe the characteristics of the participants. The t-test and Mann-Whitney U test were used to assess the significance of differences between groups of participants. The t-test and Wilcoxon test were used to test for differences before and after training. A 2 × 2 (group × time) repeated-measures ANOVA was used to assess the effect of training type on time-assessed body composition, CRF, and MetS factors. For interaction effects (“time × group”) and main effects (“time” and “group”), p ≤ 0.05 was statistically significant. Eta-squared (η2) was used to determine effect sizes, with values of 0.02, 0.13 and 0.26 and above considered small, medium and large effect sizes45.
Results
Participants characteristics
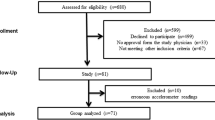
A total of 56 volunteers were selected from an initial pool of 121 women who expressed interest in participating in the study. 56 participants were assigned to the BPT group and the DA group. A total of five participants withdrew. In the DA group, two individuals discontinued participation with no specific reason. In the BP group, three participants withdrew—one was lost to follow-up, one due to a broken toe and the other due to a loss of interest in continuing with the study (Fig. 2). Table 1 summarizes the characteristics of all participants. 51 participants (age 70 ± 5 years, height 159 ± 6 cm, BW 70.4 ± 11.5 kg and BMI 27.8 ± 4.1) were assessed at baseline. No significant differences were found between the groups in terms of the variables assessed at baseline (Table 1). Detailed analysis of dietary data in the dietary interviews was limited by inaccuracies and omissions in participants’ self-reported diets, including inconsistent reporting of the number, portion size, and type of foods consumed. After the assessment, it was found that 11.1% of participants in the BPT group and 16.6% in the DA group were undergoing hormone replacement therapy.

TREND diagram of the study procedures.
Primary outcome
No significant differences were found in participants’ characteristics and outcomes at baseline.
A group x time effect (interaction) was observed for VO2max (L/min; p = 0.012), and VO2max (mL/kg/min; p = 0.005), showing that the BPT group increased more than the DA group. After intervention, the BPT group significantly increased VO2max (L/min; p = 0.001) and VO2max (mL/kg/min; p = 0.001). A time effect was observed for HR, indicating that both groups decreased HR (p = 0.004), with a significant reduction (p = 0.008) only in the DA group (Table 2).
A time effect was observed for SBP (p = 0.001), DBP (p = 0.001), TC (p = 0.002), HDL-C (p = 0.003), Non-HDL-C (p = 0.021), and LDL-C (p = 0.028), indicating that both groups improved. After intervention, PW in the BPT group increased HDL-C (p = 0.009) and reduced SBP (p = 0.001), DBP (p = 0.001), TC (p = 0.005), Non-HDL-C (p = 0.006), and LDL-C (p = 0.014). A group effect was observed for SBP (p = 0.018) and HDL-C (p = 0.032), indicating that the BPT group exhibited lower SBP and higher HDL-C compared with those in the DA group. At post-intervention, SBP (p = 0.009) was lower and HDL-C (p = 0.016) higher in BPT than DA, without significant interactions (Table 2).
Significant differences in ALT and AST were observed between groups at baseline. A time effect was also observed for ALT (p = 0.011) and AST (p = 0.001). No significant between-group differences were found in the values of changes in ALT (p = 0.851) or AST (p = 0.655) (Table 2).
Secondary outcome
An interaction effect was observed for BMR(p = 0.04), VFA (p = 0.037), PBF (p = 0.007), and BFM (p = 0.009), showing that the BPT group increased more than the DA group. After intervention, the BPT group increased BMR (p = 0.006) and reduced VFA (p = 0.006), PBF (p = 0.001), and BFM (p = 0.001), and the DA group reduced VFA (p = 0.007), PBF (p = 0.045), and BFM (p = 0.046). A time effect was observed for BW (p = 0.004), BMI (p = 0.002), BMR (p = 0.009), VFA (p = 0.001), PBF (p = 0.001), SMM (p = 0.037), BFM (p = 0.001), FFM (p = 0.007), SLM (p = 0.034), RLLM (p = 0.001), and LLLM (p = 0.001), indicating that both groups improved. After intervention, the BPT group increased SMM (p = 0.01), FFM (p = 0.014), SLM (p = 0.01), RLLM (p = 0.002), and LLLM (p = 0.001) and reduced BW (p = 0.001), BMI (p = 0.001). (Table 2).
Adherence
The adherence of participants to the 12-week BPT program was closely monitored to ensure compliance with the protocol and the reliability of the intervention. The BPT group included 27 participants and completed a program consisting of 36 training sessions. Across all sessions, a total of 97 absences were recorded, resulting in an adherence rate of 90.0%.
Adverse events
No adverse events were recorded in participants during the program.
Discussion
The main objective of this study was to examine the effects of a 12-week BPT on CRF, MetS factors, and body composition to assess whether the training can be beneficial to PW. The present study found that 12-week BPT significantly improves CRF (VO2max) and body composition, including BMR, VFA, PBF, and BFM, compared with DA. BPT significantly improves MetS factors—BP, TC, HDL-C, Non-HDL-C, and LDL-C— as well as additional body composition, including BW, BMI, SMM, FFM, SLM, RLLM, and LLLM after intervention.
Favourable changes in CRF reduce CVD risk factors and CVD morbidity and mortality46. The effect of VO2max in the present study showed a significant improvement in PW in the BPT group by 7% and 9% after the intervention, but not in the DA group. A 6-month study by Muollo et al., in which participants engaged in either walking or NW three times per week, showed improvements in VO2max of 3.14% and 3.91%, respectively, in the elderly47. The metabolism of working muscles during BPT is characterized by a higher reliance on oxygen metabolism compared to NW. Increased mitochondrial content and desaturation of myoglobin in skeletal muscle tissue after exercise increases the oxidative capacity of skeletal muscle and leads to an increase in VO2max35,48,49. The reactive hyperemia induced by CT is accompanied by an increase in nitric oxide bioavailability, which improves flow-mediated dilation in the elderly and enhances VO2max50. In addition, an increase in VO2max may also be associated with positive changes in cardiac morphology and physiology as well51. The result of the present study was superior to the findings of Domaszewska et al.35. The present study found an increase in VO2max of 2.99 ± 2.14 mL·kg− 1·min− 1 in PW. In comparison, Domaszewska et al. reported an increase of 2.40 ± 3.87 mL·kg− 1·min− 1 following BPT performed twice weekly for 8 weeks35. It could be seen that increasing training frequency and duration of training may be more effective in increasing VO2max in PW.
Several studies have shown that both walking and NW can significantly reduce HR in PW52,53. In the present study, HR was reduced in both groups. The DA significantly reduced HR, while the effect of BPT was consistent with the findings of a previous study involving NW performed three times per week for 12 weeks24. A decrease in HR may be an indication of improved cardiac regulation. The HR values of the BPT group were less than the DA group’s at baseline, which may explain why there was only a time effect without any significant improvement.
CRF is strongly inversely related to MetS54. CRF is a key predictor of CVD mortality and MetS is a well-established risk factor for CVD55,56. The present study showed that both groups reduced BP. Although no significant interaction was found, SBP and DBP decreased significantly in the BPT group by 7% and 7%, respectively. Witkowska et al. found that SBP decreased by 0.39% and DBP increased by 0.8% in women over 55 years of age after NW was performed three times per week for 12 weeks24. It seemed like the BPT was better at improving BP. Sun et al. found that CT is recommended as the preferred training for improving vascular function in PW57, It may reduce arterial stiffness50, which could be related to a decrease in BP. Secondly, increased sympathetic nerve excitability induces an increase in HR, which increases cardiac output. The present study showed that BPT decreased the HR of PW, which may also contribute to the decrease in BP. The results of meta-analysis by Xi et al. indicated that CT can significantly reduce BP in PW58. The results of the present study are consistent with those of Xi et al. The present results showed that the SBP of PW in the BPT group was significantly better than that in the DA group after intervention. Exercise intensity is closely related to blood pressure regulation, with moderate intensity exercise effectively affecting SBP59. Overall, 12 weeks of BPT was effective in improving BP in PW.
However, our findings indicated no significant improvement in glucose with BPT. Our results are consistent with those of Rodziewicz-Flis et al., who conducted a 12-week BPT program performed three times per week34. The improvement in glucose depends largely on the improvement in insulin sensitivity60. Ratajczak et al. found that a 12-week CT program performed three times per week had minimal effects on HOMA-IR, glucose and lipid metabolism61. The present study performed 12 weeks of BPT and may require a longer duration to improve glucose. Evidence from previous studies indicates that it has a more pronounced effect on glucose in diabetics62. In contrast, most PW have normal glucose at baseline, which may have a relatively weak effect in the healthy population.
The present study showed that both groups improved TC, HDL-C, Non-HDL-C and LDL-C. Although no significant interaction was found, the BPT group demonstrated significant improvements in TC, HDL-C, non-HDL-C, and LDL-C (8%, 7%, 8%, and 8%, respectively). Comparing our results with those of another study, 12 weeks of NW, with three 60-minute sessions per week, also showed improvements in lipid profiles. While some parameters were not significant, HDL-C was significantly different between groups63. This is consistent with the results of the present study. Exercise training contributes to the lipolytic process through the regulation of exerkines, lipolysis-associated enzymes and cofactors, miRNA and lncRNA, hormones, essential components of cell signaling and lipophagy64. This enhances lipoprotein metabolism to increase cholesterol uptake. Exercise training produces beneficial changes in lipid profiles, with CT yielding the most favorable effects65. TG is affected by various factors such as blood glucose and insulin resistance, which did not change significantly in the present study66. BPT involves more muscle groups and increases cardiovascular load, and may contribute more to HDL-C. Liang et al. concluded that CT maximises HDL-C benefits67. More muscle groups are involved in BPT, increasing the load on the upper body, which may stimulate more lipoprotein metabolism and promote improved lipids. In the present study, ALT and AST were found to be within the normal physiological range in the BPT group, although there was no significant change68. A similar study found that combined training did not have significant changes in ALT and AST69.
The studies revealed that CT improved body composition in PW3 and reduced the incidence of CVD70. The present study also found that BPT significantly improved BMR, VFA, PBF, and BFM compared with DA, by 2%, 7%, 5%, and 7%, respectively. Although no significant interaction was found, BPT led to significant improvements in BW, BMI, and lean mass, except for RALM, LALM, and TLM after intervention. A meta-analysis showed that aerobic training was effective for fat loss, whereas resistance training was effective for muscle gain3. Mechanistically, aerobic training promotes fat mobilization and oxidation, thereby facilitating reductions in adiposity, while resistance training enhances muscle metabolic function, contributing to improvements in BMR71. BPT provides additional resistance during marching and improves muscle strength through increased muscle activation27, which may explain why BPT leads to an increase in basal metabolic rate and a reduction in body fat. Although BPT did not significantly improve RALM, LALM and TLM, resulted in a slower loss of lean body mass than DA. In addition, Grgic et al. found that the gains in muscle strength in the early phase of training in older adults resulted primarily from neural adaptations, whereas muscle hypertrophy or muscle fibre hypertrophy became significant in the later phase72. Several authors examined the effects of twice-weekly BPT for 8 weeks on body composition in PW. Huta-Osiecka et al. reported significant improvements in BM, BMI, Fat mass, and PFM following the intervention32. Similarly, Domaszewska et al.observed significant reductions in BM and BMI after the intervention, but not in PBF, VFA, FFM, SMM35. This is inconsistent with some of the results of the present study, and it is possible that increasing the duration and frequency of training is more conducive to improvements on body composition. NW training mainly burns fatty acids as a source of muscle ATP and reduces adipose tissue levels when physical exercise is increased26.
Based on previous trials, BPT seems to be particularly favourable in PW as it is safe and feasible25,27,32,34. Adherence to exercise protocol is a major issue in exercise intervention trials. The high rate of adherence in this trial may be largely attributed to the high level of interest in participating in the exercise intervention.
BPT, as a new form of NW, efficiently improves CRF and MetS factors in PW. With the increasing acceptance and life expectancy of BPT in PW, we believe that further research in BPT is important for different populations for CVD prevention.
Strengths of the current study include that taking PW as subjects is important to prevent cardiovascular diseases and maintain their health. BPT, as a modified form of NW, provides a reference for the study of the effects of different exercise forms in PW. The results involve a rather basic but covering the main health parameters of physiological, biochemical and body composition measurements, providing a comprehensive analysis of the health status of PW.
The trial has several limitations. The use of randomization based on geographical location also had some limitations. First, although the distances between the cities were relatively small, this method does not fully eliminate the risk of uneven distribution of other variables, such as education level or access to healthcare, which may differ between cities. Additionally, geographical location may introduce some biases related to differences in health habits among residents of different regions, which could affect the overall representativeness of the sample. Despite these limitations, the use of geographical location-based division allowed for controlling environmental variables, which increased the internal validity of the study by minimizing the risk of systematic differences between groups. Second, the study population included both obese and normal-weight PW. However, the weight status of postmenopausal women in real life is diverse. Therefore, the results of the study may be informative in a wider population. Third, the lack of dietary control. Although dietary intake was monitored, limitations in the accuracy of self-reported food records precluded a comprehensive analysis of energy and protein intake as potential confounders. However, participants were asked not to change their diet during the training program. Future studies are encouraged to incorporate objective dietary assessment tools to better account for the potential influence of dietary factors. Fourth, the lack of data on time since menopause and hormone therapy use, which may influence physiological responses to exercise in PW. Although the average participant age suggests about 18 years based on Kaczmarek73 since menopause, individual differences could have influenced the results. Future research should consider these factors to better understand their potential moderating effects. Finally, although physical activity in the DA group was objectively monitored for seven consecutive days, these data were not analysed. Therefore, the actual level of daily activity performed could have been relatively high, potentially reducing the differences observed between the BPT and DA groups in some outcomes.
Conclusions
The present study demonstrated that the 12-week BPT completed 60-minute sessions 3 times a week significantly improved CRF (VO2max) and body composition (increased BMR; decreased VFA, PBF, and BFM) compared with DA. Both groups showed improvements in MetS factors (BP, TC, HDL-C, Non-HDL-C, and LDL-C) over time. Overall, BPT proved to be a more effective training modality than DA for enhancing CRF and body composition in untrained PW.
These results could provide important guidelines for PW to consider incorporating BPT as a non-pharmacological intervention, especially for improving CRF, body composition and MetS in untrained older individuals.
Data availability
Data from this study are provided in the manuscript and can also be obtained by contacting the corresponding author (Zbigniew Ossowski).
Abbreviations
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- BMR:
-
Basal metabolic rate
- BP:
-
Blood pressure
- BFM:
-
Body fat mass
- BW:
-
Body weight
- BMI:
-
Body-mass index
- BPT:
-
Bungy Pump Training
- CRF:
-
Cardiorespiratory fitness
- CVD:
-
Cardiovascular disease
- DA:
-
Daily activity
- DBP:
-
Diastolic blood pressure
- FFM:
-
Fat-free mass
- HR:
-
Heart rate
- HRmax :
-
Maximal heart rate
- HRmean :
-
Average heart rate
- HDL-C:
-
High-density lipoprotein cholesterol
- LALM:
-
Left arm lean mass
- LLLM:
-
Left leg lean mass
- LDL-C:
-
Low-density lipoprotein cholesterol
- VO2max :
-
Maximum oxygen uptake
- MetS:
-
Metabolic syndrome
- Non-HDL-C:
-
Non-high-density lipoprotein cholesterol
- NW:
-
Nordic walking
- PBF:
-
Percent body fat
- PW:
-
Postmenopausal women
- RALM:
-
Right arm lean mass
- RLLM:
-
Right leg lean mass
- SLM:
-
Skeletal lean mass
- SMM:
-
Skeletal muscle mass
- SBP:
-
Systolic blood pressure
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- TLM:
-
Trunk lean mass
- VFA:
-
Visceral fat area
References
Foreman, K. J. et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet 392, 2052–2090 (2018).
Roth, G. A. et al. Global burden of cardiovascular diseases and risk Factors, 1990–2019. J. Am. Coll. Cardiol. 76, 2982–3021 (2020).
Khalafi, M. et al. The effects of exercise training on body composition in postmenopausal women: a systematic review and meta-analysis. Front. Endocrinol. (Lausanne). 14, 1183765 (2023).
Stojanovska, L., Apostolopoulos, V., Polman, R. & Borkoles, E. To exercise, or, not to exercise, during menopause and beyond. Maturitas 77, 318–323 (2014).
Wang, X., Han, Y., Li, H., Wang, X. & Wang, G. Impact of a precision intervention for vascular health in Middle-Aged and older postmenopausal women using Polar heart rate sensors: A 24-Week RCT study based on the new compilation of Tai Chi (Bafa Wubu). Sens. (Basel). 24, 5832 (2024).
Lobo, R. A. et al. Metabolic and cardiovascular effects of TX-001HR in menopausal women with vasomotor symptoms. Climacteric 22, 610–616 (2019).
Chodzko-Zajko, W. J. et al. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 41, 1510 (2009).
Jo, E. A. et al. Effects of exergaming in postmenopausal women with high cardiovascular risk: A randomized controlled trial. Clin. Cardiol. 43, 363–370 (2020).
Carr, M. C. The emergence of the metabolic syndrome with menopause. J. Clin. Endocrinol. Metab. 88, 2404–2411 (2003).
Torréns, J. I. et al. Relative androgen excess during the menopausal transition predicts incident metabolic syndrome in midlife women: study of women’s health across the Nation. Menopause 16, 257–264 (2009).
Friedenreich, C. M. et al. Adiposity changes after a 1-year aerobic exercise intervention among postmenopausal women: a randomized controlled trial. Int. J. Obes. (Lond). 35, 427–435 (2011).
Irwin, M. L. et al. Effect of exercise on total and intra-abdominal body fat in postmenopausal women: a randomized controlled trial. JAMA 289, 323–330 (2003).
Hsia, J. et al. Resting heart rate as a low tech predictor of coronary events in women: prospective cohort study. BMJ 338, b219 (2009).
Chrysant, S. G. The cardiometabolic benefits of exercise in postmenopausal women. J. Clin. Hypertens. (Greenwich). 22, 1691–1693 (2020).
Hagner-Derengowska, M. et al. The influence of a ten-week nordic walking training-rehabilitation program on the level of lipids in blood in overweight and obese postmenopausal women. J. Phys. Ther. Sci. 27, 3039–3044 (2015).
Tune, J. D., Goodwill, A. G., Sassoon, D. J. & Mather, K. J. Cardiovascular consequences of metabolic syndrome. Transl Res. 183, 57–70 (2017).
Abdulnour, J. et al. The effect of the menopausal transition on body composition and cardiometabolic risk factors: a Montreal-Ottawa new emerging team group study. Menopause 19, 760–767 (2012).
Santosa, S. & Jensen, M. D. Adipocyte fatty acid storage factors enhance subcutaneous fat storage in postmenopausal women. Diabetes 62, 775–782 (2013).
Abildgaard, J. et al. Menopause is associated with decreased whole body fat oxidation during exercise. Am. J. Physiology-Endocrinology Metabolism. 304, E1227–E1236 (2013).
Elliott, K. J., Sale, C. & Cable, N. T. Effects of resistance training and detraining on muscle strength and blood lipid profiles in postmenopausal women. Br. J. Sports Med. 36, 340–344 (2002).
Nelson, M. E. et al. Physical activity and public health in older adults: recommendation from the American college of sports medicine and the American heart association. Med. Sci. Sports Exerc. 39, 1435–1445 (2007).
Mendoza, N. et al. Benefits of physical exercise in postmenopausal women. Maturitas 93, 83–88 (2016).
Cebula, A. et al. Physiological response and cardiorespiratory adaptation after a 6-week nordic walking training targeted at lipid oxidation in a group of post-menopausal women. PLoS One. 15, e0230917 (2020).
Witkowska, A., Grabara, M., Kopeć, D. & Nowak, Z. The effects of nordic walking compared to conventional walking on aerobic capacity and lipid profile in women over 55 years of age. J. Phys. Act. Health. 18, 669–676 (2021).
Marciniak, K., Maciaszek, J., Cyma-Wejchenig, M., Szeklicki, R. & Stemplewski, R. The effect of nordic walking training with Poles with an integrated resistance shock absorber on the body balance of women over the age of 60. Healthc. (Basel). 9, 267 (2021).
Pilch, W. B. et al. The influence of a 12-week program of physical activity on changes in body composition and lipid and carbohydrate status in postmenopausal women. Prz Menopauzalny. 14, 231–237 (2015).
Marciniak, K. et al. The effect of nordic walking training with Poles with an integrated resistance shock absorber on the functional fitness of women over the age of 60. Int. J. Environ. Res. Public. Health. 17, 2197 (2020).
Xiaoya, L. et al. Effect of different types of exercise on bone mineral density in postmenopausal women: a systematic review and network meta-analysis. Sci. Rep. 15, 11740 (2025).
Marques, A. C. F. et al. Combined aerobic and strength training improves dynamic stability and can prevent against static stability decline in postmenopausal women: A randomized clinical trial. Rev. Bras. Ginecol. Obstet. 45, e465–e473 (2023).
Khalafi, M. et al. Influence of exercise type and duration on cardiorespiratory fitness and muscular strength in post-menopausal women: a systematic review and meta-analysis. Front. Cardiovasc. Med. 10, 1190187 (2023).
Tan, A. et al. Effects of exercise training on metabolic syndrome risk factors in post-menopausal women – A systematic review and meta-analysis of randomised controlled trials. Clin. Nutr. 42, 337–351 (2023).
Huta-Osiecka, A. et al. Influence of nordic walking with Poles with an integrated resistance shock absorber on carbohydrate and lipid metabolic indices and white blood cell subpopulations in postmenopausal women. PeerJ 10, e13643 (2022).
Sobczak, K., Nowinka, P., Wochna, K. & Domaszewska, K. The effects of nordic walking with Poles with an integrated resistance shock absorber on red blood cell distribution and cardiorespiratory efficiency in postmenopausal Women—A randomized controlled trial. Biology (Basel). 12, 179 (2023).
Rodziewicz-Flis, E. et al. Nordic walking training in bungypump form improves cognitive functions and physical performance and induces changes in amino acids and kynurenine profiles in older adults. Front. Endocrinol. (Lausanne). 14, 1151184 (2023).
Domaszewska, K. et al. The effects of nordic walking with Poles with an integrated resistance shock absorber on cognitive abilities and cardiopulmonary efficiency in postmenopausal women. Front. Aging Neurosci. 12, 586286 (2020).
Kodama, S. et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA 301, 2024–2035 (2009).
Skórkowska-Telichowska, K. et al. Nordic walking in the second half of life. Aging Clin. Exp. Res. 28, 1035 (2016).
Mansur, A. J. & Nunes, R. A. B. Heart rate response and chronotropic incompetence in exercise stress testing of asymptomatic women. Womens Health (Lond). 6, 785–787 (2010).
Liu, Y. et al. Relationship between physical activity and abdominal obesity and metabolic markers in postmenopausal women. Sci. Rep. 14, 26496 (2024).
Aloisio, E. et al. Traceability validation of six enzyme measurements on the Abbott alinity c analytical system. Clin. Chem. Lab. Med. 58, 1250–1256 (2020).
Lapić, I. et al. Analytical validation of 39 clinical chemistry tests and 17 immunoassays on the alinity analytical system. Scand. J. Clin. Lab. Invest. 82, 199–209 (2022).
Ekblom-Bak, E., Björkman, F., Hellenius, M. L. & Ekblom, B. A new submaximal cycle ergometer test for prediction of VO 2max. Scandinavian Med. Sci. Sports. 24, 319–326 (2014).
Väisänen, D. et al. Criterion validity of the Ekblom-Bak and the Åstrand submaximal test in an elderly population. Eur. J. Appl. Physiol. 120, 307–316 (2020).
Björkman, F., Ekblom-Bak, E., Ekblom, Ö. & Ekblom, B. Validity of the revised Ekblom bak cycle ergometer test in adults. Eur. J. Appl. Physiol. 116, 1627–1638 (2016).
Boutcher, Y. N., Boutcher, S. H., Yoo, H. Y. & Meerkin, J. D. The effect of sprint interval training on body composition of postmenopausal women. Med. Sci. Sports Exerc. 51, 1413–1419 (2019).
Lavie, C. J., Ozemek, C., Carbone, S., Katzmarzyk, P. T. & Blair, S. N. Sedentary Behavior, Exercise, and cardiovascular health. Circ. Res. 124, 799–815 (2019).
Muollo, V. et al. Prolonged unsupervised nordic walking and walking exercise following six months of supervision in adults with overweight and obesity: A randomised clinical trial. Nutr. Metab. Cardiovasc. Dis. 31, 1247–1256 (2021).
Harber, M. P. et al. Impact of cardiorespiratory fitness on All-Cause and Disease-Specific mortality: advances since 2009. Prog Cardiovasc. Dis. 60, 11–20 (2017).
Pinckard, K., Baskin, K. K. & Stanford, K. I. Effects of exercise to improve cardiovascular health. Front. Cardiovasc. Med. 6, 69 (2019).
Silva, R. S. N., da, Silva, D. S., de da, Oliveira, P. C., Waclawovsky, G. & Schaun, M. I. Effects of aerobic, resistance and combined training on endothelial function and arterial stiffness in older adults: a systematic review and meta-analysis. PLOS One. 19, e0308600 (2024).
Lavie, C. J. et al. Exercise and the cardiovascular system: clinical science and cardiovascular outcomes. Circ. Res. 117, 207–219 (2015).
Pilch, W. et al. Effects of 6-week Nordic walking training on changes in 25(OH)D blood concentration in women after 55 years of age. J. Sports Med. Phys. Fitness 57, 124 (2016).
Güzel, Y., Atakan, M. M., Turnagöl, H. H. & Koşar, ŞN. Effects of 10 weeks of walking-based exercise training on resting substrate oxidation in postmenopausal women with obesity. Eur. J. Clin. Nutr. https://doi.org/10.1038/s41430-024-01546-1 (2024).
Earnest, C. et al. Maximal estimated cardiorespiratory Fitness, cardiometabolic risk Factors, and metabolic syndrome in the aerobics center longitudinal study. Mayo Clin. Proc. 88, 259–270 (2013).
Singh, B. et al. Comparison of objectively measured and estimated cardiorespiratory fitness to predict all-cause and cardiovascular disease mortality in adults: A systematic review and meta-analysis of 42 studies representing 35 cohorts and 3.8 million observations. J. Sport Health Sci. 14, 100986 (2025).
Wu, Z. et al. The causal relationship between metabolic syndrome and its components and cardiovascular disease: A Mendelian randomization study. Diabetes Res. Clin. Pract. 211, 111679 (2024).
Sun, W., Han, Y. & Gu, S. Effects of five types of exercise on vascular function in postmenopausal women: a network meta-analysis and systematic review of 32 randomized controlled trials. PeerJ 12, e17621 (2024).
Xi, H. et al. Effect of combined aerobic and resistance exercise on blood pressure in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Exp. Gerontol. 155, 111560 (2021).
Ross, R., Hudson, R., Stotz, P. J. & Lam, M. Effects of exercise amount and intensity on abdominal obesity and glucose tolerance in obese adults: a randomized trial. Ann. Intern. Med. 162, 325–334 (2015).
Czech, M. P. Insulin action and resistance in obesity and type 2 diabetes. Nat. Med. 23, 804–814 (2017).
Ratajczak, M. et al. Effects of 12-Week combined strength and endurance circuit training program on insulin sensitivity and Retinol-Binding protein 4 in women with insulin-Resistance and overweight or mild obesity: A randomized controlled trial. Diabetes Metab. Syndr. Obes. 17, 93–106 (2024).
Valenti, V. E. et al. Effect of combined aerobic exercise and resistance training on postmenopausal women with type 2 diabetes: a systematic review and meta-analysis. Gynecol. Endocrinol. 41, 2450338 (2025).
Pospieszna, B. et al. Influence of 12-week nordic walking training on biomarkers of endothelial function in healthy postmenopausal women. J. Sports Med. Phys. Fit. 57, 1178–1185 (2017).
Zhu, J. Y. & Guo, L. Exercise-regulated lipolysis: its role and mechanism in health and diseases. J. Adv. Res. https://doi.org/10.1016/j.jare.2024.11.031 (2024).
Smart, N. A. et al. The effect of exercise training on blood lipids: a systematic review and meta-analysis. Sports Med. 55, 67–78 (2025).
Justesen, J. M. et al. Increasing insulin resistance accentuates the effect of triglyceride-associated loci on serum triglycerides during 5 years. J. Lipid Res. 57, 2193–2199 (2016).
Liang, M., Pan, Y., Zhong, T., Zeng, Y. & Cheng, A. S. K. Effects of aerobic, resistance, and combined exercise on metabolic syndrome parameters and cardiovascular risk factors: a systematic review and network meta-analysis. Rev. Cardiovasc. Med. 22, 1523–1533 (2021).
Clayton-Chubb, D. et al. Serum transaminases and older adults: distribution and associations with All-Cause mortality. J. Gerontol. Biol. Sci. Med. Sci. 79, glae203 (2024).
Hejazi, K. & Hackett, D. Effect of exercise on liver function and insulin resistance markers in patients with Non-Alcoholic fatty liver disease: A systematic review and Meta-Analysis of randomized controlled trials. J. Clin. Med. 12, 3011 (2023).
Srikanthan, P., Horwich, T. B. & Tseng, C. H. Relation of muscle mass and fat mass to cardiovascular disease mortality. Am. J. Cardiol. 117, 1355–1360 (2016).
Khalafi, M. et al. The effects of concurrent training versus aerobic or resistance training alone on body composition in middle-aged and older adults: a systematic review and meta-analysis. Health Care (Don Mills). 13, 776 (2025).
Grgic, J. et al. Effects of resistance training on muscle size and strength in very elderly adults: A systematic review and Meta-Analysis of randomized controlled trials. Sports Med. 50, 1983–1999 (2020).
Kaczmarek, M. The timing of natural menopause in Poland and associated factors. Maturitas 57, 139–153 (2007).
Acknowledgements
We would like to thank the staff of Gdansk University of Physical Education and Sport for their help in organizing the study.
Author information
Authors and Affiliations
Contributions
Conceptualization, Y.N. and Z.O.; methodology, Y.N. and Z.O.; formal analysis, Y.N.; investigation, Y.N., L.R., G.Q., and Z.O.; resources, Z.O.; data curation, Y.N. and Z.O.; writing—original draft preparation, Y.N.; writing—review and editing, Y.N., G.Q. and Z.O.; supervision, G.Q., A.S. and Z.O.; project administration, Z.O. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee of the District Medical Chamber in Gdansk (protocol code KB-5/22).
Informed consent
Written informed consent has been obtained from the patient(s) to publish this paper. Registration number of the clinical trial: NCT06781541.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Niu, Y., Radzimiński, Ł., Qian, G. et al. Effect of a 12-week bungy pump training on cardiorespiratory fitness, metabolic syndrome factors and body composition in postmenopausal women. Sci Rep 15, 41938 (2025). https://doi.org/10.1038/s41598-025-25909-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-25909-1
