
Abstract
Electrical stimulation is increasingly applied as a non-invasive intervention for managing urinary incontinence in women, aiming to improve both urinary symptoms and quality of life. The purpose of this systematic review and meta-analysis was to evaluate the effectiveness of electrical stimulation on quality of life and relevant clinical outcomes in women with urinary incontinence, and to explore sources of heterogeneity through subgroup and meta-regression analyses. This review was conducted according to PRISMA 2020. Six electronic databases were searched for randomized controlled trials evaluating electrical stimulation interventions for women with urinary incontinence published between 1995 and 2025. Fourteen randomized controlled trials met the inclusion criteria. A random-effects model was used to synthesize effect sizes (Hedges’ g). Heterogeneity was assessed using Cochran’s Q and I2. Subgroup and meta-regression analyses were conducted to explore potential moderators. Publication bias was evaluated using funnel plots, Egger’s and Begg’s tests, and the trim-and-fill method. Additionally, a network meta-analysis was conducted to facilitate indirect comparisons among intervention types. The pooled effect size for quality of life was not statistically significant (Hedges’ g = –0.29, 95% CI –0.72 to 0.14, p = .182), with high heterogeneity (I2 = 91.1%). Subgroup analyses revealed significant effects in studies using the I-QoL, ICIQ, and Wagner’s QoL tool, participants with urgency urinary incontinence, in smaller sample sizes, and in interventions involving fewer sessions or continuous stimulation. Meta-regression confirmed that outcome tool, sample size, urinary incontinence type, and study quality were significant moderators. In the network meta-analysis, which included ES, ES + PFMT, PFMT, biofeedback, and control, no statistically significant differences in quality of life were observed among the interventions, and no inconsistency was detected between direct and indirect comparisons. For secondary outcomes, electrical stimulation significantly improved symptom severity, micturition frequency, nocturia, and urinary incontinence episodes, but not pad test results or pelvic floor muscle strength. Electrical stimulation appears to have limited overall effects on improving quality of life and symptoms in patients with urinary incontinence. However, it may be effective under specific conditions, when adjusted for the subtype of urinary incontinence, the method of electrical stimulation application, and the quality of life measures used.
Similar content being viewed by others


Introduction
Urinary incontinence (UI) is a common disease among women worldwide and significantly affects their quality of life (QoL)1. According to the International Urogynecological Association (IUGA) and International Continence Society (ICS), UI is a symptom of involuntary urine leakage and is classified into stress urinary incontinence (SUI), urgency urinary incontinence (UUI), mixed urinary incontinence (MUI), and others2.
The prevalence of UI in women is reported to be 25–45% worldwide3, and in Korea, 24.4% of women aged 19 years or older experience urinary incontinence, with SUI and MUI being the most common4. In particular, UI in women is closely related to increasing age, fertility, obesity, smoking, and other diseases, and is considered one of the major causes of decreased QoL after middle age5. Women with UI experience serious limitations in their daily lives, and it is also related to negative mental health such as depression or anxiety and decreased QoL6,7. Therefore, incontinence should be considered a complex health problem that goes beyond a simple physical problem and affects overall mental and social health.
Electrical stimulation (ES) therapy is recognized as one of the noninvasive and effective interventions for the treatment of UI8. This treatment mainly uses electrodes on the vagina, anus, tibia, or sacrum of women to stimulate the pelvic floor muscles or related nerves to induce muscle contraction and promote nerve rehabilitation8,9. However, despite various clinical applications, systematic studies of ES in women with UI remain limited. Although therapeutic effects have been shown, they vary by UI subtype and type of ES8,9,10. Similarly, the effects of ES on QoL are similar. Individual studies have reported that ES therapy is effective in improving QoL8,10, but on the contrary, systematic studies have reported that it is difficult to confirm significant changes11. Therefore, a systematic review of the effects of ES in improving QoL is needed.
The effects of ES therapy have limitations in that it is difficult to draw consistent conclusions because the intervention method, frequency, period, and evaluation tools are different for each study. In particular, quantitative and integrated analysis of the effect of improving QoL is still insufficient. However, QoL is an outcome indicator as important as simple symptom improvement in the treatment of urinary incontinence. QoL is a multidimensional concept encompassing health status, autonomy, social relationships, and emotional satisfaction. It is a key indicator of patient-centered treatment12.
QoL related to UI is mainly measured by King’s Health Questionnaire (KHQ), Incontinence Quality of Life Questionnaire (I-QoL), International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF) and others. These QoL measures are essential for understanding the clinical significance of treatment effects and the overall level of recovery of patients13. Although many studies on ES have been published, meta-analyses focusing on QoL improvement to demonstrate consistency of treatment effects and clinical utility are very limited. Therefore, this meta-analysis quantitatively analyzed the effect of ES on QoL in women with UI, and compared the differences in the effects of sub-analyses according to the QoL measurement tool and the intervention characteristics of ES. This analysis can provide a basis for evidence-based practice required for nurses when caring for UI patients.
Methods
Eligibility criteria
The eligibility criteria for this meta-analysis were defined according to the PICOS framework. The Population included adults aged 18 years or older diagnosed with UI, specifically SUI, UUI, or MUI. The Intervention was ES, and the Comparison group included participants receiving usual care, no intervention, or an alternative intervention other than ES. The Primary Outcome was QoL, while Secondary Outcomes included symptom severity, results of the pad test, daytime micturition frequency, nocturia, number of SUI or UUI episodes, and pelvic muscle strength. In studies that included more than one intervention group (study IDs: 2, 3, and 13), each intervention was treated as a separate comparison to calculate effect sizes. Only randomized controlled trials (RCTs) were included. Moreover, studies were eligible for quantitative synthesis only if they reported the sample size, mean, and standard deviation for both groups. Studies were excluded if they met any of the following conditions: (1) the study population included participants younger than 19 years, or patients with UI subtypes other than SUI or UUI; (2) the intervention in the experimental group was not ES, or the QoL outcome was not reported; (3) the data required for effect size calculation (i.e., means, standard deviations, and sample sizes) were not available; (4) the article was not published in English or Korean, or the full text could not be retrieved, including conference abstracts and unpublished manuscripts; and (5) the study had a single-group design with no control group for comparison.
Information sources and search strategy
This systematic review and meta-analysis involved searches of six electronic databases: PubMed, EMBASE, CINAHL, SCOPUS, DBpia, and RISS. Searches were conducted between April 10 and June 19, 2025, and were limited to articles published between January 1, 1995, and March 31, 2025, in English or Korean. The search strategy focused on identifying RCTs investigating the effects of ES on UI and QoL among adult female populations. In PubMed, both Medical Subject Headings (MeSH) and free-text terms were used in combination with Boolean operators (AND, OR). Core search terms included “urinary incontinence”, “electric stimulation”, "quality of life", "randomized controlled trial", “female”, and “adult”. Similar conceptual strategies were adapted to other databases according to their structure. This systematic review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420251030013. The protocol can be accessed at: https://www.crd.york.ac.uk/PROSPERO/view/CRD420251030013.
Selection process
The study selection process was conducted in accordance with the PRISMA 2020 guidelines. Initially, two reviewers independently screened the titles and abstracts of all retrieved records. In cases of disagreement regarding study inclusion, consensus was reached through discussion with a third reviewer. Full-text articles of potentially eligible studies were then assessed independently using the same process, and only studies meeting the predefined inclusion criteria were included in the final analysis. No automation tools were used at any stage of the selection process; all screening and eligibility assessments were conducted manually.
The overall selection process is visualized using the PRISMA 2020 Flow Diagram, which illustrates the steps of identification, duplicate removal, title and abstract screening, full-text review, and final inclusion (see Fig. 1).

PRISMA flow diagram of study extraction.
Data collection and extracted items
Data extraction was performed using a pre-developed standardized form. Two reviewers independently extracted the data. Any discrepancies in extracted outcomes were resolved through discussion with a third reviewer. When necessary, the original full-text articles were re-examined. No automation tools were used. To minimize the risk of missing data items, a structured Excel spreadsheet was developed in advance and used to systematically document extracted information. All data collection was conducted manually. The primary outcome of interest was QoL, while secondary outcomes included symptom severity, pad test results, number of micturition per day, nocturia episodes, frequency of SUI or UUI episodes, and pelvic floor muscle strength. In addition, the following study-level variables were extracted: year of publication, study design, IRB approval status, funding source, sample size (per group), participants’ mean age, type of UI (SUI, UUI, or mixed), characteristics of the ES intervention (type, stimulation site, intensity, duration, number of sessions, session duration), type of control group intervention, measurement variables (including instruments used for QoL), and risk of bias or quality appraisal scores.
Study risk of bias assessment
The methodological quality of the included studies was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for RCTs14. Two reviewers independently evaluated the risk of bias after reviewing the question guidance and reaching a consensus on the evaluation criteria in advance. The JBI checklist consists of 13 items, each rated as ‘Yes’, ‘No’, ‘Unclear’, or ‘Not applicable’. For synthesis purposes, the responses were dichotomized: ‘Yes’ was assigned a score of 1, and all other responses were scored as 0, with a total score calculated for each study. Discrepancies between reviewers were resolved through discussion with a third reviewer until consensus was achieved. The final quality score, based on the number of ‘Yes’ responses, was used to assess the overall methodological rigor of each study and was also considered in the sensitivity analysis. The quality assessment results were presented in tabular form (Table 2). No automation tools were used, and all assessments were conducted manually.
Effect measures
In this meta-analysis, standardized mean differences (SMDs) and 95% confidence intervals (CIs) were calculated using Hedges’ g to estimate the effect sizes15. Hedges’ g, a bias-corrected version of Cohen’s d, was chosen as it provides more accurate estimates in meta-analyses that include small-sample studies, which applied to our included trials16. Effect sizes were calculated using the post-intervention means and standard deviations from both the intervention and control groups. Given the variability in measurement tools used across studies to assess QoL and urinary incontinence-related outcomes, the SMD approach was applied to ensure comparability of results17.
Synthesis methods
All statistical analyses were conducted using a random-effects model to account for heterogeneity across studies18 and were performed with Comprehensive Meta-Analysis software (version 4; Biostat, Englewood, NJ, USA). To estimate pooled effect sizes, this meta-analysis employed the standardized mean difference (SMD) using Hedges’ g. The effect size for each study was computed based on the post-intervention means, standard deviations, and sample sizes of both intervention and control groups. The statistical significance of the pooled SMD was determined by checking whether the 95% CI excluded zero and whether the p values were less than 0.0519. Between-study heterogeneity was assessed using Cochran’s Q test and the I2 statistic, with I2 values of 25%, 50%, and 75% interpreted as low, moderate, and high heterogeneity, respectively20. When substantial heterogeneity (I2 > 50%) or a significant Q statistic was identified, subgroup analyses and meta-regression were performed to explore potential sources of heterogeneity. Subgroup analyses were conducted based on predefined study-level characteristics (e.g., type of incontinence, stimulation site, and intervention characteristics). Within each subgroup, pooled effect sizes were calculated using a random-effects model. Differences between subgroups were evaluated using a fixed-effects model for subgroup comparisons, following a mixed-effects model approach21. Statistical significance of subgroup differences was tested using the Z-test for interaction, based on Hedges’ g and its standard error. Sensitivity analyses were conducted using a leave-one-out approach, in which each study was sequentially removed to examine its impact on the overall pooled effect size. This method enabled the identification of studies that disproportionately influenced the results and provided an assessment of the robustness and stability of the meta-analytic findings. To assess publication bias, visual inspection of funnel plots was supplemented with the trim-and-fill method, which estimates the number of potentially missing studies and recalculates the adjusted pooled effect size accordingly22. Additionally, Egger’s regression test and the Begg–Mazumdar rank correlation test were conducted. Egger’s test offers greater sensitivity in detecting bias in small-sample meta-analyses, while Begg’s test provides a more conservative evaluation23. In addition to conventional pairwise meta-analyses, a network meta-analysis (NMA) was conducted using the netmeta package (version 3.2–0) in R (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria) to enable indirect and mixed treatment comparisons24. The interventions included electrical stimulation (ES) and combined ES with pelvic floor muscle training (ES + PFMT), compared against PFMT, biofeedback, and control, with the control group serving as the reference. Summary effects were synthesized using a random-effects model, and between-study variance (τ2) was estimated via the DerSimonian–Laird method25. To ensure consistent directionality across studies, treatment effects (TEs) were coded such that negative values indicated improvement in quality of life. Multi-arm trials were accounted for using the built-in procedures in netmeta, including consistency checks for multi-arm designs. The network geometry was visualized with the netgraph() function, and summary results were presented using network forest plots.
Reporting bias assessment
In this meta-analysis, the potential for reporting bias was assessed using both visual and statistical methods. For the primary outcome, QoL and funnel plot asymmetry was visually examined. Quantitative evaluations were conducted using Egger’s regression test and the Begg-Mazumdar rank correlation test. As the number of included studies exceeded ten, Duval and Tweedie’s trim-and-fill method was applied to estimate the number of potentially missing studies and to calculate an adjusted pooled effect size22. The certainty of evidence was not formally assessed using the GRADE framework in this review.
Results
Study selection
A total of 2050 records were identified through six electronic databases. After removing 108 duplicates, 1942 records were screened based on titles and abstracts. Of these, 1886 were excluded for not meeting the eligibility criteria, and 56 articles were retrieved for full-text review. The full-text review was conducted in two stages. In the first stage, 28 articles were excluded for the following reasons: one article could not be retrieved in full text, and the remaining 27 were excluded due to inappropriate study design (e.g., not RCTs) or because QoL was not reported as a primary outcome. In the second stage of the remaining 28 articles, 14 were excluded for the following reasons: population did not meet eligibility criteria (n = 1), intervention did not involve ES (n = 5), no QoL outcomes were reported (n = 6), or the article was not an original study (n = 2). Ultimately, 14 RCTs were included in the meta-analysis. The entire study selection process is illustrated in the PRISMA 2020 flow diagram (Fig. 1).
Study characteristics
A total of 14 RCTs were included in this meta-analysis, all of which involved female patients diagnosed with UI. The studies were published between 2008 and 2025, with the majority conducted within the last five years. The sample sizes ranged from 30 to 148 participants, and most studies reported a balanced distribution between experimental and control groups. The interventions in the experimental groups included either ES alone or combined with pelvic floor muscle training (PFM) or lifestyle modification education. The anatomical sites of stimulation varied, including the ankle, thigh, and gluteal region, suprapubic and ischial region, and intravaginal application. Frequencies of ES ranged from 10 to 50 Hz, with individual session durations from 15 to 30 min. The intervention period ranged from 4 to 15 weeks, and the number of sessions varied from 8 to 60. Control groups received sham ES, PFM alone, biofeedback, or usual care. In some studies, lifestyle education was also provided to the control group. The primary outcome, QoL, was assessed using validated tools, including ICIQ-SF, KHQ, I-QoL, the Overactive Bladder questionnaire (OAB-q) and Wagner’s QoL. All included studies were approved by an institutional ethics committee, and 10 out of the 14 studies reported receiving funding. The methodological quality of the studies was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Tool for RCTs. Total scores ranged from 9 to 12, with a mean score of 10.5 (SD = 1.09), indicating an overall moderate to high quality of evidence (Table 1).
Risk of bias in studies
All 14 RCTs included in this meta-analysis were assessed for methodological quality using the Joanna Briggs Institute (JBI) critical appraisal tool for RCTs, which comprises 13 items14. The mean quality score across all studies was 10.5 (SD = 1.09, range: 9–12), with 7 studies (50.0%) scoring equal to or above the mean. Regarding individual items, Q1 (Randomization), Q6 (Equal treatment except intervention), Q8 (Same outcome measurement), Q9 (Reliable measurement), Q10 (Follow-up and attrition), Q11 (Intention-to-treat analysis), Q12 (Appropriate statistical analysis), and Q13 (Trial design suitability) were rated as “Yes” in all studies, indicating consistent adherence to these quality criteria. In contrast, Q5 (Provider blinding) was either not implemented or not clearly reported in any of the included studies, and Q4 (Participant blinding) was clearly reported in only 4 studies (Table 2).
Results of syntheses
Effect of ES on QoL
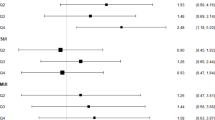
This meta-analysis included 14 RCTs that examined the effects of ES on QoL in women with urinary incontinence. A random-effects model was applied to account for heterogeneity across studies. The pooled effect size was Hedges’ g = − 0.29 (95% CI − 0.72 to 0.14, p = 0.182), indicating no statistically significant improvement in QoL in the ES group compared to control interventions. The heterogeneity among studies was substantial, with Cochran’s Q = 180.72 (Q-df = 148.57, p < 0.001) and I2 = 91.1%, suggesting a high level of inconsistency (Fig. 2). To explore potential sources of heterogeneity, subgroup analyses, and meta-regression were conducted.

The effect of electrical stimulation intervention on quality of life. CI confidence interval. Superscript a and b were studies divided by intervention. *Control group participants were counted only once in studies with multiple intervention arms to prevent duplication of participants.
Network meta-analysis
The network meta-analysis included five interventions: ES, ES + PFMT, PFMT, biofeedback, and usual care (control), with both direct and indirect comparisons contributing to the estimates. No statistically significant differences in quality of life (QoL) were observed among the interventions (Fig. 3A). Compared with the control, none of the interventions, including biofeedback (95% CI − 2.57 to 0.88), ES (95% CI − 0.57 to 0.52), ES + PFMT (95% CI − 1.70 to 1.25), or PFMT (95% CI − 1.30 to 1.64), demonstrated significant improvements (Fig. 3B). No inconsistency was detected between direct and indirect comparisons.

Network meta-analysis. (A) Network geometry of included interventions. Nodes are proportional to sample size, and edges reflect the number of studies per comparison. (B) Forest plot of network meta-analysis. The forest plot presents effect sizes (SMDs with 95% CIs) for each intervention compared with the control group, with the control group as the reference.
Subgroup analyses
Subgroup analyses based on QoL measurement tools revealed that studies using the ICIQ, I-QoL, or Wagner QoL reported significantly improved QoL, and the difference in effect sizes between measurement tools was statistically significant (Z = − 2.21, p = 0.027). Studies published after 2020, those with fewer than 50 participants, and those targeting patients with UUI showed significant and large effect sizes. Additionally, interventions involving fewer than 18 sessions or using continuous stimulation reported more pronounced effects. Subgroup analyses based on the type of control group intervention revealed that studies using pelvic floor muscle (PFM) training or biofeedback as control treatments demonstrated significant improvements in QoL. However, the differences in effect sizes according to characteristics of the included studies were not statistically significant (Table 3).
Meta-regression
Meta-regression analyses were conducted to investigate the impact of moderators on heterogeneity (Table 4). Studies that used the I-QoL as the outcome measure had smaller sample sizes, included participants with SUI, or had lower overall methodological quality scores showed significantly larger pooled effect sizes.
Sensitivity analyses
Sensitivity analyses were conducted by sequentially removing each individual study to assess the robustness of the results (Table 5). No single study was found to exert a disproportionate influence on the overall effect estimate, supporting the stability and reliability of the synthesized results.
Secondary outcomes of ES interventions
In addition to QoL, this meta-analysis evaluated the effects of ES interventions on seven other clinical outcomes (Table 6). A significant improvement was observed in urinary symptom severity, with a pooled effect size of Hedges’ g = − 0.80 (95% CI − 1.34 to − 0.26, p = 0.004), although the level of heterogeneity was high (Q = 104.45, p < 0.001; I2 = 89.5%). Similarly, daytime micturition frequency significantly decreased (Hedges’ g = − 0.50, 95% CI − 0.86 to − 0.15, p = 0.005), with a moderate-to-high level of heterogeneity (I2 = 75.3%). Nocturia showed a highly significant reduction (Hedges’ g = − 0.66, 95% CI − 0.91 to − 0.40, p < 0.001) with minimal heterogeneity (I2 = 3.6%). For SUI-related episodes, the effect size was Hedges’ g = − 0.31 (95% CI − 0.54 to − 0.07, p = 0.011), and for UUI-related episodes, Hedges’ g = − 0.56 (95% CI − 0.89 to − 0.23, p = 0.001); both outcomes showed statistically significant improvement with moderate heterogeneity (I2 = 66.3% and 58.9%, respectively). The pad test result showed a non-significant trend favoring the intervention (Hedges’ g = − 0.43, 95% CI − 0.86 to 0.01, p = 0.057), with a high degree of heterogeneity (I2 = 87.2%). In addition, no significant effect was found for pelvic floor muscle strength (Hedges’ g = 0.13, 95% CI − 0.67 to 0.93, p = 0.749), accompanied by very high heterogeneity (I2 = 92.3%).
Reporting biases
In this meta-analysis, the possibility of publication bias was assessed both visually and statistically. A funnel plot based on the primary outcome (QoL) was visually inspected (Fig. 4A), showing an approximately symmetrical distribution of studies. To further evaluate potential asymmetry, Duval and Tweedie’s trim-and-fill method was applied (Fig. 4B). This procedure estimated that no studies were missing, and the adjusted pooled effect size (Hedges’ g = − 0.29, 95% CI − 0.72 to 0.14) was identical to the original estimate, indicating that publication bias is unlikely to have influenced the results meaningfully (Table 7). Statistical tests were also conducted to evaluate reporting bias. The Begg and Mazumdar rank correlation test revealed a statistically significant result (Tau-b = − 0.36, Z = 1.98, p = 0.048), suggesting a potential small-study effect. In contrast, Egger’s regression intercept test, which quantitatively assesses funnel plot asymmetry, yielded an intercept of − 4.49 (t = 1.59, p = 0.132), indicating no statistically significant asymmetry. Although the findings from Begg’s and Egger’s tests were somewhat inconsistent, the visual inspection and the trim-and-fill analysis support the conclusion that the overall results of this meta-analysis were robust and minimally influenced by publication bias.

Funnel plot for the effect of electrical stimulation on quality of life in patients with urinary incontinence (Hedges’ g). (A) Funnel plot of observed studies for the effect of electrical stimulation on quality of life. (B) Funnel plot including imputed studies based on the trim-and-fill method.
Discussion
UI is a health condition that has been shown in previous studies to reduce the QoL26. UI is a disease that affects many people worldwide, with more than one in four people reported to experience incontinence during their lifetime27. However, incontinence is underestimated in many ways because it is perceived as a natural process of aging and is overlooked for various reasons28.
A meta-analysis of UI and QoL reported that incontinence was associated with poor QoL and moderate to high strength26. The literature shows that people with incontinence generally have more comorbidities than those without incontinence, which are related to gender, age, cognitive function, and motor skills26. In addition, patients with incontinence changed their lifestyles, such as suppressing physical activity due to shame, and developed mental disorders26. Therefore, active interventions are required to improve patients’ QoL in addition to incontinence symptoms.
ES has been selected as one of the nonsurgical treatments applicable to various types of UI29. It is a method of stimulating the muscles and nerves around the urethra by controlling ES according to the individual’s symptoms and condition and transmitting the stimulation to the pelvic floor muscles29. On the other hand, the possibility of side effects is low9. In individual studies, the results of studies on the improvement of incontinence symptoms and QoL by ES have been reported several times9,11. However, meta-analyses have not reported consistent results on the effectiveness9,11, and the effect on QoL in particular has been unclear11. In addition, existing meta-studies mainly examined the effect of ES on SUI among UIs and improvement of physical symptoms. Therefore, this study aimed to examine the overall effect of ES therapy on the QoL of various female UI patients.
In this meta-analysis, the pooled effect size of ES for QoL was not statistically significant. However, substantial heterogeneity was observed across studies (I2 = 91.1%), and subgroup analyses showed that certain conditions, such as the use of specific tools, smaller sample sizes, UUI patient groups, and shorter or more continuous stimulation protocols, were associated with significantly improved QoL.
The non-significant pooled effect may reflect methodological heterogeneity, particularly the wide variation in QoL measurement tools. QoL is multidimensional, and the included instruments differ in sensitivity and subdomains, limiting comparability30. The QoL measurement tools included in this meta-analysis had different directionality of score interpretation in particular. I-QoL, OAB-q, and Wagner QoL indicate that higher scores indicate higher QoL31,32,33, but ICIQ and KHQ interpret them in the opposite13,34. In other words, it would have been difficult to analyze the effect of QoL by integrating tools with such different directions to have a statistically significant effect.
Subgroup analysis results showed that studies using ICIQ, I-QoL, and Wagner QoL significantly improved QoL compared to studies using other instruments. In addition, meta-regression analysis results showed that I-QoL had a significantly greater effect on improving QoL when ICIQ was used as the criterion. ICIQ is a tool that measures the severity of urinary incontinence, including frequency, amount, and interference with daily life13. I-QoL does not directly measure symptoms, but rather measures avoidance and restriction behaviors, psychosocial impact, and social embarrassment31,32. In contrast, the OAB-q is more specific to overactive bladder symptoms and includes sleep disturbances due to symptoms33. The KHQ includes more general measures such as sleep/energy and overall health perceptions34. Although there may be differences between tools, such as sensitivity and scoring direction, the effect of improving QoL in patients with UI seems to be greater when focusing more on the direct impact of urinary incontinence.
The effects of ES on QoL also differed by participant characteristics. ES interventions showed significant improvements in individuals with UUI (g = − 0.85, p = 0.013), whereas no significant effect was found in those with SUI. However, meta-regression revealed that studies focusing on SUI reported greater effect sizes compared to UUI (β = 1.49, p = 0.003), suggesting possible interactions between UI subtype and the measurement instrument used.
The characteristics of the intervention also influenced the effectiveness of ES. Subgroup analysis showed that continuous stimulation had a significant effect (g = − 0.63, p = 0.011), whereas intermittent stimulation had no effect. In addition, interventions of less than 18 sessions significantly improved QoL (g = − 0.60, p = 0.023). This suggests that even short-term protocols can help improve QoL, which can provide more persuasive interventions to patients. These findings suggest that continuous stimulation protocols may facilitate more stable neuromuscular adaptation, while shorter-term regimens with fewer sessions could improve feasibility and adherence in real-world clinical practice. However, because the number of studies in each subgroup was relatively small, these results should be interpreted with caution, and further high-quality trials are warranted to confirm parameter-specific effects.
Beyond QoL, ES also showed significant improvements in outcomes such as symptom severity (g = − 0.80, p = 0.004), micturition frequency (g = − 0.50, p = 0.005), nocturia (g = − 0.66, p < 0.001), and both SUI and UUI episodes. The meta results showing that ES was effective in improving UI symptoms are similar to previous studies9,11. This symptom improvement may have had a positive effect in studies that used tools that focused on symptoms to measure the QoL of UI patients.
Taken together, these results suggest that ES can be an effective intervention for improving QoL and reducing urinary symptoms in women with UI, particularly when tailored by subtype, stimulation parameters, and outcome measurement tools. However, heterogeneity in study design, measurement tools, and intervention characteristics underscores the need for standardized protocols and further high-quality RCTs to optimize its clinical application.
In clinical nursing practice, electrical stimulation is often applied in conjunction with pelvic floor muscle training or bladder training. Therefore, when interpreting the impact of electrical stimulation on quality of life, it is essential to consider patient education, compliance, and the nursing environment in which these interventions are provided. From a nursing perspective, incorporating patient-reported outcome measures, such as condition-specific quality of life instruments, into routine assessments can improve individualized treatment and outcome monitoring.
This study has several limitations. First, the small number of studies per subgroup limited the power to detect moderating effects. Second, although Begg’s test suggested the presence of small-study effects (p = 0.048), this indication was not supported by Egger’s regression test or the trim-and-fill analysis. Given the inconsistent findings across methods and the known limitations of each test, especially in the context of high heterogeneity and a small number of studies, the possibility of publication bias cannot be completely ruled out. Lastly, due to inconsistent reporting of QoL subdomains, we were unable to analyze differential impacts across physical, social, or psychological domains. In addition, heterogeneity may also stem from the underlying causes of UI itself. Women with urethral hypermobility, intrinsic sphincter deficiency, or overactive bladder may respond differently to electrical stimulation due to distinct pathophysiological mechanisms and coexisting conditions. This inherent variability across subtypes is difficult to fully resolve in meta-analyses and should be recognized as an expected limitation.
Conclusions
This meta-analysis showed that ES did not significantly improve QoL in women with UI when combined across studies. However, subgroup analyses showed significantly greater effects in studies using condition-specific instruments such as the I-QoL, ICIQ, and Wagner’s QoL, particularly in urge incontinence, small samples, and studies using specific stimulation protocols. These results suggest that the observed heterogeneity may be due to differences in outcome measures and intervention characteristics. Thus, rather than concluding that there is no effect of ES on QOL in UI women, these results highlight the need for targeting appropriate subgroups and better adjustment of measurement criteria. Future studies should adopt validated disease-specific QoL instruments and provide detailed intervention descriptions to improve comparability and practical application.
Data availability
All data generated or analyzed during this study are included in the published article. However, additional datasets used and/or analyzed during this study can be obtained from the corresponding author upon reasonable request.
Abbreviations
- ES:
-
Electrical stimulation
- QoL:
-
Quality of life
- UI:
-
Urinary incontinence
- SUI:
-
Stress urinary incontinence
- UUI:
-
Urgency urinary incontinence
- MUI:
-
Mixed urinary incontinence
- RCT:
-
Randomized controlled trials
References
Kwon, C. S. & Lee, J. H. Prevalence, risk factors, quality of life, and health-care seeking behaviors of female urinary incontinence: Results from the 4th Korean National Health and Nutrition Examination Survey VI (2007–2009). Int. Neurourol. J. https://doi.org/10.5213/inj.2014.18.1.31 (2014).
Haylen, B. T. et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int. Urogynecol. J. https://doi.org/10.1007/s00192-009-0976-9 (2010).
Milsom, I. & Gyhagen, M. The prevalence of urinary incontinence. Climacteric https://doi.org/10.1080/13697137.2018.1543263 (2019).
Lee, K. S., Sung, H. H., Na, S. & Choo, M. S. Prevalence of urinary incontinence in Korean women: Results of a National Health Interview Survey. World J. Urol. https://doi.org/10.1007/s00345-008-0239-2 (2008).
Batmani, S., Jalali, R., Mohammadi, M. & Bokaee, S. Prevalence and factors related to urinary incontinence in older adults women worldwide: A comprehensive systematic review and meta-analysis of observational studies. BMC Geriatr. https://doi.org/10.1186/s12877-021-02135-8 (2021) (Erratum In: BMC Geriatr. 2022; 10.1186/s12877-022-03111-6).
Kim, T. Y. et al. Urinary incontinence in middle-aged and older Korean women and its impact on quality of life: A cross-sectional study. Eur. Geriatr. Med. https://doi.org/10.1007/s41999-018-0112-9 (2018).
Coyne, K. S. et al. Urinary incontinence and its relationship to mental health and health-related quality of life in men and women in Sweden, the United Kingdom, and the United States. Eur. Urol. https://doi.org/10.1016/j.eururo.2011.07.049 (2012).
Schreiner, L., Santos, T. G., Souza, A. B., Nygaard, C. C. & Silva Filho, I. G. Electrical stimulation for urinary incontinence in women: A systematic review. Int. Braz. J. Urol. https://doi.org/10.1590/S1677-5538.IBJU.2013.04.02 (2013).
Han, X., Shen, H., Chen, J. & Wu, Y. Efficacy and safety of electrical stimulation for stress urinary incontinence in women: A systematic review and meta-analysis. Int. Urogynecol. J. https://doi.org/10.1007/s00192-021-04928-2 (2022).
Yu, T. Y. et al. Comparison of nonimplantable electrical stimulation in women with urinary incontinence: A systematic review and network meta-analysis of randomized controlled trials. Sci. Rep. https://doi.org/10.1038/s41598-024-78358-7 (2024).
Stania, M., Niemiec, B., Kamieniarz, A. & Chmielewska, D. Intravaginal electrical stimulation as a monotherapy for female stress urinary incontinence: A systematic review and meta-analysis. Complement Ther. Clin. Pract. https://doi.org/10.1016/j.ctcp.2022.101624 (2022).
Patrick, D. L. & Deyo, R. A. Generic and disease-specific measures in assessing health status and quality of life. Med. Care https://doi.org/10.1097/00005650-198903001-00018 (1989).
Avery, K. et al. ICIQ: A brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourol. Urodyn. https://doi.org/10.1002/nau.20041 (2004).
Barker, T. H. et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid. Synth. https://doi.org/10.11124/JBIES-23-00227 (2023).
Lin, L. & Aloe, A. M. Evaluation of various estimators for standardized mean difference in meta-analysis. Stat. Med. https://doi.org/10.1002/sim.8781 (2021).
Taylor, J. M. & Alanazi, S. Cohen’s and Hedges’ g. J. Nurs. Educ. https://doi.org/10.3928/01484834-20230415-02 (2023).
Murad, M. H., Wang, Z., Chu, H. & Lin, L. When continuous outcomes are measured using different scales: Guide for meta-analysis and interpretation. BMJ https://doi.org/10.1136/bmj.k4817 (2019).
Dettori, J. R., Norvell, D. C. & Chapman, J. R. Fixed-effect vs random-effects models for meta-analysis: 3 points to consider. Glob. Spine J. https://doi.org/10.1177/21925682221110527 (2022).
Flechner, L. & Tseng, T. Y. Understanding results: P-values, confidence intervals, and number need to treat. Indian J. Urol. https://doi.org/10.4103/0970-1591 (2011).
Ruppar, T. Meta-analysis: How to quantify and explain heterogeneity?. Eur. J. Cardiovasc. Nurs. https://doi.org/10.1177/1474515120944014 (2020).
Sørensen, A. L. & Marschner, I. C. Linear mixed models for investigating effect modification in subgroup meta-analysis. Stat. Methods Med. Res. https://doi.org/10.1177/09622802231163330 (2023).
Duval, S. & Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics https://doi.org/10.1111/j.0006-341x.2000.00455.x (2000).
Lin, L. et al. Empirical comparison of publication bias tests in meta-analysis. J. Gen. Intern. Med. https://doi.org/10.1007/s11606-018-4425-7 (2018).
Rücker, G. Network meta-analysis, electrical networks and graph theory. Res. Synth. Methods 3(4), 312–324. https://doi.org/10.1002/jrsm.1058 (2012).
DerSimonian, R. & Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 7(3), 177–188. https://doi.org/10.1016/0197-2456(86)90046-2 (1986).
Pizzol, D. et al. Urinary incontinence and quality of life: A systematic review and meta-analysis. Aging Clin. Exp. Res. https://doi.org/10.1007/s40520-020-01712-y (2021).
Ebbesen, M. H., Hunskaar, S., Rortveit, G. & Hannestad, Y. S. Prevalence, incidence and remission of urinary incontinence in women: longitudinal data from the Norwegian HUNT study (EPINCONT). BMC Urol. https://doi.org/10.1186/1471-2490-13-27 (2013).
Elenskaia, K. et al. The greatest taboo: urinary incontinence as a source of shame and embarrassment. Wien Klin Wochenschr https://doi.org/10.1007/s00508-011-0013-0 (2011).
Stewart, F., Berghmans, B., Bø, K. & Glazener, C. M. Electrical stimulation with non-implanted devices for stress urinary incontinence in women. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD012390.pub2 (2017).
Haraldstad, K. et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. https://doi.org/10.1007/s11136-019-02214-9 (2019).
Patrick, D. L. et al. Quality of life of women with urinary incontinence: Further development of the incontinence quality of life instrument (I-QOL). Urology https://doi.org/10.1016/s0090-4295(98)00454-3 (1999).
Wagner, T. H., Patrick, D. L., Bavendam, T. G., Martin, M. L. & Buesching, D. P. Quality of life of persons with urinary incontinence: Development of a new measure. Urology https://doi.org/10.1016/s0090-4295(99)80384-7 (1996).
Coyne, K. et al. Psychometric validation of an overactive bladder symptom and health-related quality of life questionnaire: The OAB-q. Qual. Life Res. https://doi.org/10.1023/a:1016370925601 (2002).
Kelleher, C. J., Cardozo, L. D., Khullar, V. & Salvatore, S. A new questionnaire to assess the quality of life of urinary incontinent women. Br. J. Obstet. Gynaecol. https://doi.org/10.1111/j.1471-0528.1997.tb11006.x (1997).
Author information
Authors and Affiliations
Contributions
MKC and YHC participated in the design of the study. MKC and YHC undertook the literature review process. MKC conducted a meta-analysis. MKC and YHC drafted the manuscript. MKC and YHC reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cho, MK., Cho, Y.H. Systematic review and meta-analysis of electrical stimulation for quality of life in women with urinary incontinence. Sci Rep 15, 44274 (2025). https://doi.org/10.1038/s41598-025-27854-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-27854-5
