
Abstract
Insulin resistance (IR) has been associated with incident frailty. However, the precise association between the estimated glucose disposal rate (eGDR) and the development of frailty remains insufficiently understood. We hypothesized that a lower eGDR, indicating greater IR, would be associated with a higher risk of developing frailty and with accelerated frailty progression across cohorts. This study aimed to systematically investigate and clarify this association. Data were obtained from three prospective cohorts: the China Health and Retirement Longitudinal Study (CHARLS), the English Longitudinal Study of Ageing (ELSA), and the Health and Retirement Study (HRS). Frailty was assessed using the Rockwood Frailty Scale. Baseline eGDR, changes in eGDR, and cumulative eGDR from baseline to the most recent survey wave, as well as the frailty index for each survey year, were evaluated. Logistic and Cox regression models were used to examine the association between eGDR and incident frailty. To assess frailty progression over time, we applied linear mixed-effects models and evaluated potential nonlinear trends. In addition, K-means clustering was conducted as an exploratory analysis to describe heterogeneity in longitudinal eGDR trajectories. A total of 7,666 participants were included from CHARLS (female: 51%, mean age: 58.27 years), 4,296 from ELSA (female: 53%, mean age: 64.89 years), and 4,370 from HRS (female: 56%, mean age: 66.63 years). A significant association was observed between lower eGDR and an increased risk of frailty (hazard ratio [HR]: 0.91, 95% CI 0.88–0.94; HR: 0.90, 95% CI 0.87–0.94; and HR: 0.95, 95% CI 0.92–0.98 for CHARLS, ELSA, and HRS, respectively) and with an accelerated increase in frailty index (β: −0.005, 95% CI −0.007 to − 0.004; β: −0.009, 95% CI −0.010 to − 0.008; and β: −0.009, 95% CI −0.010 to − 0.008 for CHARLS, ELSA, and HRS, respectively). Similarly, increases in cumulative eGDR and in changes in eGDR over time were associated with lower risks of incident frailty and frailty index. Subgroup and sensitivity analyses demonstrated consistent findings across subgroups. The elbow method suggested that three clusters represented the optimal solution; however, these clusters did not differ significantly in frailty outcomes and were therefore interpreted as descriptive rather than predictive. These findings highlight the importance of early detection of eGDR reduction and the implementation of targeted interventions to mitigate incident frailty.
Similar content being viewed by others


Introduction
The global population has been aging for more than a century, leading to a substantial increase in frailty rates and associated health burdens among older adults1,2. Frailty, a degenerative condition, refers to an age-related state arising from the loss of physiological capacity across multiple organ systems, which renders individuals increasingly vulnerable to stressors as they age2,3. Once established, frailty tends to progress naturally through the aging process and is associated with a higher likelihood of geriatric syndromes such as falls, incontinence, cognitive decline, pressure ulcers, mild cognitive impairment, and delirium4,5. Moreover, frailty is strongly correlated with mortality, independent of chronological age, and with cause-specific mortality6. Given the high global prevalence of frailty among older adults, preventing its onset and progression has become a critical public health priority. Early intervention to slow or delay frailty-related decline, even years before death, may help prevent adverse health outcomes and extend the healthy lifespan of older individuals7. However, current intervention strategies remain limited in efficacy, underscoring the need to identify precise biomarkers and develop more targeted therapeutic approaches8.
Insulin resistance (IR) is characterized by a reduced biological response or impaired sensitivity to insulin5,9. Although the exact mechanisms linking IR to frailty remain unclear, it has been proposed that IR may contribute to metabolic disturbances affecting energy and lipid metabolism, which could underlie the development of frailty and related metabolic syndromes10. Individuals with IR also exhibit several pathological and physiological processes associated with aging, including oxidative stress, inflammation, and reduced muscle function11,12,13. Multiple cohort studies have reported associations between metabolic syndrome, IR, and frailty5,14,15,16. Collectively, current evidence supports a link between IR and frailty; however, the precise mechanisms and long-term trajectories remain insufficiently understood.
Recent evidence suggests that a simpler indicator, the estimated glucose disposal rate (eGDR), can serve as an alternative biomarker for IR. Compared with traditional measures such as the homeostatic model assessment of insulin resistance (HOMA-IR), eGDR offers several advantages: it does not require fasting insulin measurements, which are often unavailable or inconsistently collected in large epidemiological cohorts, has been validated against the gold-standard euglycemic–hyperinsulinemic clamp, and can be easily derived from routinely collected clinical variables. These features make eGDR particularly suitable for cross-cohort analyses such as those conducted in the China Health and Retirement Longitudinal Study (CHARLS), the ELSA, and the HRS. However, despite its growing use, the association between eGDR and frailty, particularly longitudinal changes in eGDR and their influence on frailty onset and progression, remains poorly characterized. This represents a critical gap in current knowledge. In this study, we analyzed three prospective cohorts: CHARLS, ELSA, and HRS, to investigate whether fluctuations in eGDR are associated with incident frailty and frailty progression. Findings from this work are expected to provide a foundation for developing more precise therapeutic strategies to address frailty and to overcome the limitations of current interventions. Our central hypothesis is that lower eGDR, indicating greater IR, is associated with an increased risk of incident frailty and with accelerated frailty progression among older adults.
Methods
Study population
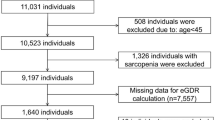
Comprehensive information on the study designs of the CHARLS, the ELSA, and the HRS is available in previous publications17,18,19. These cohorts were prospectively designed to represent the national populations of China, the United Kingdom, and the United States, respectively. Participants were eligible if they were aged 45 years or older at baseline, had available data on the eGDR and the frailty index, and completed at least one follow-up assessment. Individuals were excluded if they had missing baseline frailty data, missing baseline eGDR data, were younger than 45 years at baseline, or lacked follow-up information. The age threshold of 45 years was selected in accordance with the CHARLS study design and comparable aging cohorts, as it represents the transition from midlife to older adulthood when IR and frailty-related physiological changes typically begin to emerge. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines. Baseline waves were defined as wave 1 (2011) for CHARLS, wave 2 (2004–2005) for ELSA, and wave 8 (2006) for HRS. Follow-up continued through the most recent available survey waves: wave 4 (2018) for CHARLS, wave 9 (2018–2019) for ELSA, and wave 15 (2020) for HRS. Ethical approval for each cohort was granted by the respective institutional review boards, the Peking University (CHARLS), the London Multi-Centre Research Ethics Committee (ELSA), and the University of Michigan (HRS). All methods were performed in accordance with the relevant guidelines and regulations. All participants provided written informed consent. Figure 1 presents an overview of the study design. Across CHARLS, ELSA, and HRS, a total of 45,785 participants were included in the analyses. First, 9,477 and 14,819 participants with missing frailty and eGDR data, respectively, were excluded. In addition, 796 participants were excluded because they were younger than 45 years or lacked follow-up information. After applying these exclusion criteria, 20,693 participants with baseline frailty data were included in the initial sample. Consequently, 16,332 participants who were non-frail at baseline were included in the primary analyses. Transitional analyses were subsequently conducted among participants who met the baseline criteria. Of these, 14,805 participants with complete frailty and eGDR data at both baseline and follow-up were included. Finally, 12,088 non-frail participants with complete eGDR data at baseline and follow-up were included in the transitional analyses.

Flowchart of the study population. CHARLS, China Health and Retirement Longitudinal Study; eGDR, estimated glucose disposal rate; ELSA, English Longitudinal Study of Ageing; HRS, Health and Retirement Study.
Assessment of frailty
Frailty was assessed using a frailty index derived by aggregating multiple age-related health deficits. The index was constructed according to previously established procedures20,21,22,23. Twenty-eight items were selected from the CHARLS, ELSA, and HRS datasets, encompassing domains of disease, symptoms, disability, physical function, depression, and cognition (Supplementary Table S1). Based on established cut-off values, items 1–27 were dichotomized to indicate the presence or absence of each deficit, coded as 1 or 0, respectively. Item 28, representing the cognitive score, was treated as a continuous variable ranging from 0 to 1. The cognitive score was calculated as (memory test score + orientation test score)/14 and then rescaled to a 0–1 scale, with higher values indicating poorer cognitive function. For each participant, the frailty index was computed by dividing the total number of observed deficits by the number of non-missing items, thereby allowing for missing data to be handled through averaging across available variables. Participants with more than 10% missing items (i.e., ≥ 3 of 28) were excluded from the analysis. The resulting frailty index ranged from 0 to 1, with higher values indicating greater frailty. A score greater than 0.25 was classified as frail5,24. The 28-item frailty index was harmonized across CHARLS, ELSA, and HRS using identical coding schemes for all items, except for depressive symptoms, which were assessed using the CESD-10 in CHARLS and the CESD-8 in ELSA and HRS; these measures were harmonized using established cut-offs.
CHARLS wave 1, ELSA wave 2, and HRS wave 8 were used as the baseline waves. Follow-up analyses of frailty and eGDR began with wave 2 of CHARLS, wave 3 of ELSA, and wave 9 of HRS. In this study, follow-up ended at the first occurrence of frailty, death, or the censoring date, whichever came first. Participants were censored according to the date of their most recent survey participation. Ideally, the final survey waves corresponded to wave 4 (2018) for CHARLS, wave 9 (2018–2019) for ELSA, and wave 15 (2020) for HRS. Mortality data were available beginning from the baseline wave in CHARLS and HRS, whereas in ELSA, death information became available starting from wave 6 (2012–2013)25,26.
Assessment of eGDR
The eGDR at baseline was used as the primary exposure variable in this study. eGDR was calculated using the following formula: eGDR (mg/kg/min) = 21.158 − (0.09 × waist circumference [WC]) − (3.407 × hypertension) − (0.551 × glycated haemoglobin [HbA1c]) [WC (cm), hypertension (yes = 1/no = 0), and HbA1c (%)]27. CHARLS, ELSA, and HRS calculate the cumulative eGDR as follows: (eGDRw1 + eGDRw3)/2 × time (w3 − w1), (eGDRw2 + eGDRw4 + eGDRw6)/3 × time (w6 − w2), and (eGDRw8 + eGDRw9 + eGDRw10 + eGDRw11 + eGDRw12 + eGDRw13)/6 × time (w13 − w8) in CHARLS, ELSA and HRS, respectively. This approach was used to approximate the cumulative exposure to eGDR over time. Because eGDR was measured only at discrete survey waves, the mean of the available values within each interval was calculated and multiplied by the corresponding time span. This procedure is mathematically equivalent to estimating the area under the eGDR–time curve, which represents the total burden of exposure. Averaging across waves minimizes random error from single measurements, whereas weighting by elapsed time accounts for irregular survey intervals. This nonparametric approximation avoids assuming a specific functional form for the trajectory and is a widely applied method in longitudinal cohort analyses with intermittent repeated measures. The percentage change in eGDR between baseline and the follow-up wave was calculated as: (eGDRmax- eGDRbaseline)/eGDRbaseline × 100.
In addition to the regression analyses, K-means clustering was applied to examine whether distinct longitudinal patterns of eGDR change could be identified in an unsupervised manner. Because outcome variables were not included in the clustering procedure, this approach provided an unbiased characterization of heterogeneity in eGDR trajectories. The elbow method indicated that three clusters represented the optimal solution (Supplementary Figure S1). K-means clustering was selected instead of trajectory-modeling approaches because it does not require strong distributional assumptions or the specification of functional forms of change, which is advantageous given the irregular survey intervals and intermittent laboratory measurements across these cohorts.
Covariates
Several covariates were assessed, including age, sex, marital status, education level, smoking status, drinking status, diabetes, body mass index (BMI), systolic blood pressure, high-density lipoprotein cholesterol (HDL-C), C-reactive protein (CRP), and obesity. To ensure consistency across CHARLS, ELSA, and HRS, marital status was categorized as either married or partnered or other marital status (including separated, divorced, unmarried, or widowed). Education level was classified into three categories: below high school, high school or above, and college or higher. Smoking status was divided into never smokers and ever smokers, with the latter including both former and current smokers. Similarly, drinking status was grouped into never drinkers and ever drinkers. Obesity was defined as BMI ≥ 28 kg/m2 in CHARLS, and BMI ≥ 30 kg/m2 in ELSA and HRS. Dietary intake and physical activity were not included because harmonized measures were unavailable across cohorts; socioeconomic status was partly represented by education level.
Statistical analyses
In the descriptive analyses, continuous variables were summarized as means with standard deviations (SDs) or medians with interquartile ranges (IQRs), whereas categorical variables were presented as percentages (%). Differences in characteristics between normally and non-normally distributed variables were compared using ANOVA and the Kruskal–Wallis H test, respectively. The chi-square test was used to assess differences among categorical variables.
Cox proportional hazards regression models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for the associations between eGDR and incident frailty during the follow-up period. Model 1 was unadjusted; Model 2 was adjusted for age, sex, marital status, education level, smoking status, and drinking status; and Model 3 was further adjusted for BMI, HDL-C, CRP, diabetes, and obesity. The first measurement of eGDR was obtained during the baseline wave (wave 1 in CHARLS, wave 2 in ELSA, and wave 8 in HRS). Frailty was defined as the first occurrence of frailty status during follow-up, with assessments performed at each survey wave. Participants identified as frail at baseline were recorded as frail at the first follow-up wave in which frailty occurred. Logistic regression was employed to estimate odds ratios (ORs) and 95% CIs for the associations between eGDR and frailty at baseline or during follow-up. Cox regression was selected as the primary analytical method because it accounts for time-to-event information and censoring. Logistic regression was additionally used as a sensitivity analysis to estimate ORs for frailty status at baseline and at fixed follow-up points, thereby providing a complementary cross-sectional perspective. Restricted cubic splines (RCS) were applied to assess potential non-linear associations between eGDR and frailty, as previous evidence and biological plausibility suggest that the relationship between IR and adverse outcomes may not be strictly linear. The outcome variables included all available repeated measures of the frailty index (including the baseline value), with fixed effects for eGDR, time (follow-up duration), and covariates. In this context, eGDR represented the baseline measure, and the corresponding regression coefficient reflected the association between changes in eGDR and annual changes in the frailty index. Analyses were repeated for different representations of eGDR change, including cumulative change and percentage changes over time. Cox regression models were further stratified by baseline characteristics to examine potential subgroup differences in the associations between eGDR and frailty. Because eGDR is derived from waist circumference (WC), hypertension, and glycated hemoglobin (HbA1c), a weighted quantile sum (WQS) regression was applied in a fully adjusted model. The variables were categorized into quartiles, and 100 bootstrap iterations were conducted to analyze the data. The sample was randomly divided into a training set (40% of the data) and a validation set (60%) to determine the relative weights of WC, hypertension, and HbA1c. These weights quantified each variable’s contribution to the overall effect, with higher weights indicating stronger predictive influence in the model. For the sensitivity analyses, the primary analysis was replicated after including participants with baseline frailty, with statistical significance defined as P < 0.05. In addition, multiple imputation with five imputed datasets was performed to address missing covariate data. To account for the competing risk of death before frailty onset, Fine–Gray subdistribution hazard models were employed, with frailty as the event of interest and death as the competing event. Subdistribution hazard ratios (sHRs) and corresponding 95% CIs were estimated. For comparison, cause-specific Cox models were also fitted separately for frailty and death. These competing-risk approaches were conducted as sensitivity analyses to assess the robustness of the primary Cox regression findings.
Results
Baseline characteristics
Baseline analyses of eGDR and frailty status included 7,666 participants from CHARLS (51% female; mean age: 58.27 years), 4,296 from ELSA (53% female; mean age: 64.89 years), and 4,370 from HRS (56% female; mean age: 66.63 years). Table 1 presents the baseline characteristics of the study participants. The mean baseline eGDR values were 9.90 ± 2.07 in CHARLS, 8.48 ± 2.19 in ELSA, and 7.49 ± 2.44 in HRS. Supplementary Table S2 summarizes the baseline characteristics of participants classified as frail at baseline. As part of the transitional analysis, Supplementary Tables S3-S5 provide summaries of baseline characteristics across survey waves. The distributions of the frailty index across survey waves are shown in Fig. 2A, whereas the distributions of eGDR across survey waves are shown in Supplementary Figure S2.

Longitudinal distributions and trajectories of frailty index and eGDR across CHARLS, ELSA, and HRS. (A) Distribution of the frailty index and eGDR across survey waves in CHARLS, ELSA, and HRS. Each color of distribution represents a survey wave, showing how the distribution shifts over time. Later waves are generally shifted toward higher frailty and lower eGDR, indicating progressive health decline with aging. (B) Distribution of cumulative eGDR quantiles across survey waves. The curves illustrate how the cumulative burden of impaired glucose regulation accumulates over time, with later waves showing a greater proportion of individuals in lower quantiles. (C) Distribution of changes in cumulative eGDR across different clusters. CHARLS, China Health and Retirement Longitudinal Study; eGDR, estimated glucose disposal rate; ELSA, English Longitudinal Study of Ageing; HRS, Health and Retirement Study.
Associations of baseline eGDR with incident frailty
Cox regression analyses indicated that each one-unit increase in eGDR was associated with a lower risk of incident frailty in CHARLS (HR: 0.91, 95% CI 0.88–0.94), ELSA (HR: 0.90, 95% CI 0.87–0.94), and HRS (HR: 0.95, 95% CI 0.92–0.98) (Table 2). Quartile-based analyses further demonstrated a graded inverse association between eGDR and frailty risk across all three cohorts, although the magnitude of association was slightly weaker in HRS. Despite this difference, the direction and statistical significance of the associations were consistent across cohorts.
RCS analyses revealed that the association between continuous eGDR and frailty risk was not nonlinear in CHARLS (P for nonlinear = 0.001, Supplementary Figure S3). In contrast, the relationships appeared approximately linear in ELSA and HRS (P for non-linear = 0.937 and 0.590, respectively, Supplementary Figure S3).
Association of cumulative eGDR and changes in eGDR with incident frailty
To evaluate the influence of longitudinal changes in eGDR on the development of frailty, cumulative eGDR and change in eGDR variables were constructed. The quartile distribution of cumulative eGDR is shown in Fig. 2B. To further illustrate the longitudinal relationship between glycemic exposure and frailty, trajectories of the frailty index were plotted according to baseline eGDR quartiles, as well as by cumulative eGDR and change in eGDR during follow-up (Supplementary Figure S4). Participants in lower baseline eGDR quartiles consistently exhibited higher frailty index values over time, and similar patterns were observed when stratifying by cumulative eGDR and by decreases in eGDR. As shown in Table 3, a one-unit increase in cumulative eGDR was associated with a significantly lower risk of incident frailty (HR: 0.97, 95% CI 0.96–0.98, HR: 0.98, 95% CI 0.98–0.99, and HR: 0.99, 95% CI 0.99–0.99 for CHARLS, ELSA, and HRS, respectively). Quartile-based analyses further supported a graded inverse association, with participants in the highest quartile demonstrating a substantially reduced risk of frailty compared with those in the lowest quartile.
K-means clustering identified three distinct patterns of eGDR change (Figs. 2C and 3): (1) a relatively stable or slightly decreasing trajectory, (2) a rapid decline followed by stabilization, and (3) a steady increase. These clusters reflected the heterogeneity of eGDR dynamics across participants. However, comparisons of frailty outcomes among the clusters revealed no statistically significant differences.

Data visualization for the clusters of the change in the eGDR. (A) CHARLS. (B) ELSA. (C) HRS. Three distinct trajectory patterns were identified: (1) a relatively stable or slightly decreasing trajectory, (2) a rapid decline followed by stabilization, and (3) a steady increase. These clusters highlight heterogeneity in health trajectories, with the second group reflecting accelerated deterioration and the third suggesting potential improvement or resilience. CHARLS, China Health and Retirement Longitudinal Study; ELSA, English Longitudinal Study of Ageing; HRS, Health and Retirement Study.
Association of baseline eGDR, cumulative eGDR, and changes in eGDR with frailty index
Linear mixed-effects model analyses provided further insights into the relationships between baseline eGDR, cumulative eGDR, and the frailty index. In the fully adjusted models, each one-unit increase in eGDR was significantly associated with a lower frailty index (β: −0.005 per year, 95% CI −0.007 to − 0.004 per year; β: −0.009 per year, 95% CI −0.010 to − 0.008 per year; β: −0.009 per year, 95% CI −0.010 to − 0.008 per year for CHARLS, ELSA, and HRS, respectively) (Table 4). Although the β coefficients appear numerically small, they correspond to an approximately 25–50% slower progression of frailty over time, which is considered clinically meaningful. Quartile-based analyses further demonstrated a graded inverse association, with participants in the highest quartile exhibiting significantly slower frailty progression compared with those in the lowest quartile. A statistically significant linear trend was observed (P < 0.001).
Similarly, cumulative eGDR showed consistent associations, with each one-unit increase associated with a slower rate of frailty index decrease across all three cohorts. Quartile-based analyses again demonstrated that participants in the highest quartile had the most favorable frailty trajectories, accompanied by consistent linear trends (P for trend < 0.001).
Stratified and sensitivity analyses
In stratified analyses, the associations between eGDR and incident frailty were generally consistent across subgroups (Fig. 4). Participant age appeared to have a moderating effect on the association between eGDR and incident frailty in CHARLS and HRS (P for interaction < 0.05). In contrast, no significant interactions were observed with sex, smoking, drinking, or diabetes in any cohort (P for all interactions > 0.05).

Subgroup analysis of eGDR and incident frailty stratified by participant characteristics. Hazard ratios (HRs) with 95% confidence intervals (CIs) for the association between eGDR and incident frailty are shown across subgroups of age, sex, smoking, drinking, and diabetes status in CHARLS, ELSA, and HRS. Each subgroup analysis was stratified by participant characteristics, with corresponding P values and P for interaction provided. Adjusted covariates include age, sex, marital status, education, smoking, drinking status, BMI, HDL-C, hsCRP, diabetes, and obesity. BMI, body mass index; CHARLS, China Health and Retirement Longitudinal Study; CRP, C-reactive protein; eGDR, estimated glucose disposal rate; ELSA, English Longitudinal Study of Ageing; HRS, Health and Retirement Study; HDL-C, high-density lipoprotein cholesterol.
Sensitivity analyses yielded robust results. The associations between eGDR and incident frailty remained consistent when participants with baseline frailty were included (Supplementary Table S5). Similarly, the longitudinal associations of eGDR with incident frailty (Supplementary Table S6) and with the rate of change in frailty index (Supplementary Table S7) were materially unchanged. The associations obtained using multiple imputation to account for missing covariates also remained consistent (Supplementary Table S8).
In Fine–Gray competing risk models, higher eGDR was consistently associated with a lower cumulative incidence of frailty across all three cohorts. For each one-unit increase in eGDR, the sHR was 0.92 (95% CI 0.89–0.94; P < 0.001) in CHARLS, 0.91 (95% CI 0.87–0.94; P < 0.001) in ELSA, and 0.93 (95% CI 0.90–0.96; P < 0.001) in HRS. When modeled by quartiles, participants in higher eGDR quartiles exhibited progressively lower risks of frailty compared with those in the lowest quartile, with significant linear trends across all cohorts (P for trend < 0.001). These findings were consistent with results from the Cox proportional hazards models, indicating that accounting for mortality as a competing risk did not materially alter the association between eGDR and frailty (Supplementary Table S9).
WQS analyses
In the CHARLS, ELSA, and HRS cohorts, baseline HbA1c contributed the most to the accelerated development of frailty after covariate adjustment in Model 3, with weights of 0.604, 0.616, and 0.568, respectively (Fig. 5). The prevalence of hypertension was the second largest contributor to frailty development, with corresponding weights of 0.356, 0.289, and 0.287 for CHARLS, ELSA, and HRS, respectively.

Evaluated weights assigned to baseline eGDR with the WQS model. Weights of baseline eGDR components were estimated using the weighted quantile sum (WQS) regression model in CHARLS, ELSA, and HRS. The model was adjusted for age, sex, marital status, education, smoking, drinking status, BMI, HDL-C, CRP, diabetes, and obesity. BMI, body mass index; CHARLS, China Health and Retirement Longitudinal Study; CRP, C-reactive protein; eGDR, estimated glucose disposal rate; ELSA, English Longitudinal Study of Ageing; HRS, Health and Retirement Study; HDL-C, high-density lipoprotein cholesterol; WQS, weighted quantile sum.
Discussion
The present study aimed to examine the associations of baseline eGDR, cumulative eGDR, and changes in eGDR with incident frailty and frailty index across three large prospective cohorts. The findings demonstrated significant associations between lower eGDR values and both higher frailty index and increased risk of incident frailty. These relationships remained consistent after adjustment for multiple covariates. The results were generally robust across populations and subgroups, indicating that eGDR may serve as a useful risk indicator for frailty. Sensitivity analyses, including participants with baseline frailty and longitudinal models, further confirmed the stability of these associations, supporting the potential of eGDR as a biomarker for identifying individuals at elevated risk of frailty. Because death before frailty onset is a major competing event in aging populations, Fine–Gray competing risk models were employed. The findings were highly consistent with those from the primary Cox regression models, with higher eGDR levels remaining significantly associated with lower frailty risk across all cohorts. Although the magnitude of the association was slightly weaker in HRS compared with CHARLS and ELSA, the overall direction and statistical significance were consistent, underscoring the robustness of the results. These findings collectively suggest that the observed associations are unlikely to be explained by differential mortality, although residual confounding cannot be entirely excluded. The nonlinear association observed in CHARLS may reflect baseline differences, as only this cohort showed greater frailty prevalence in the highest eGDR quartile compared with the third quartile, likely due to its more heterogeneous population. In contrast, the narrower eGDR distributions in ELSA and HRS were consistent with linear associations. These cohort-specific patterns suggest that both biological and methodological factors may underlie the observed differences, while the overall consistency across studies reinforces the robustness of the findings. In the subgroup analyses stratified by age (cutoff = 65 years), the protective association between higher eGDR and lower frailty risk was stronger among participants younger than 65 years, whereas this association was attenuated in those aged 65 years or older. This pattern, observed in both CHARLS and HRS, suggests that insulin sensitivity may play a more prominent role in frailty risk during the earlier stages of aging. Taken together, these findings indicate that eGDR may represent a relevant biomarker for identifying individuals at higher risk of frailty and may help inform targeted preventive strategies.
With the rapid expansion of the global elderly population, frailty has become an increasingly important public health concern. To the best of our knowledge, eGDR has not previously been examined in relation to frailty. Reduced insulin sensitivity is known to disrupt the oxidative–antioxidative balance and accelerate inflammatory responses due to the accumulation of adipose tissue and the decline in skeletal muscle mass. In addition, chronic low-grade inflammation associated with immunosenescence can promote the accumulation of reactive oxygen species, impair antioxidant capacity, and contribute to the development of multiple age-related diseases27,28,29 When immune function is compromised, this imbalance in oxidative and antioxidative processes may further exacerbate pathological conditions such as metabolic syndrome and frailty10. Dysregulation of glucose metabolism during the prediabetic state may also trigger chronic inflammation and metabolic disturbances, thereby contributing to frailty, with IR representing one of the principal mechanisms underlying the onset of prediabetes30. Moreover, prediabetic conditions are commonly accompanied by comorbidities such as hypertension, which further intensify metabolic dysfunction and IR. Collectively, these mechanisms provide a strong biological rationale for eGDR as an indicator of frailty risk: higher HbA1c reflects chronic hyperglycemia and IR that drive oxidative stress and inflammation; greater waist circumference indicates central adiposity with pro-inflammatory and metabolic consequences; and hypertension signifies vascular dysfunction and diminished physiological resilience. Together, these interrelated pathways increase susceptibility to frailty.
Previous studies have demonstrated that IR, as assessed by the HOMA-IR, and elevated proteinuria levels contribute to cognitive decline in frail older adults with prediabetes, thereby accelerating frailty progression30,31. Another study using HOMA-IR also reported a significant association between IR and frailty14. Similarly, a recent study conducted among Chinese adults found that a higher triglyceride–glucose body mass index was associated with faster frailty index progression and a higher incidence of frailty4.
Moreover, eGDR has been linked to several health outcomes that are closely related to frailty. Previous research has reported that lower eGDR values are associated with an increased long-term risk of cardiovascular disease events and cardiovascular disease–related mortality32,33,34,35. A strong association has also been observed between eGDR and hypertension36. Furthermore, individuals with lower eGDR levels are more likely to develop non-alcoholic fatty liver disease37. In young adults with type 1 diabetes, eGDR has been inversely associated with the presence of retinopathy and kidney disease38. Improved IR has also been linked to a reduction in peripheral neuropathy39. These findings collectively suggest that IR may underlie multiple adverse health outcomes associated with frailty. However, research examining longitudinal changes in eGDR in relation to frailty remains limited. To date, only one published study has investigated the association between baseline eGDR and incident cardiovascular disease in middle-aged and older Chinese adults32.
In addition to its clinical significance, this study carries important implications for public health. First, integrating eGDR assessments into frailty management, particularly among older adults, could enhance early detection and prevention strategies. Individuals with lower eGDR levels should be prioritized for targeted interventions aimed at delaying frailty progression and reducing frailty burden. Previous studies have suggested that recovery from frailty primarily involves improvements in physical function (items 20–26)24. Consistent with these findings, our results indicate that interventions enhancing physical capacity may mitigate frailty progression. Further research using both real-world data and clinical trials is required to evaluate the efficacy and safety of such interventions for frailty reversal. Thus, concerted efforts are needed to develop and implement effective intervention strategies for reversing frailty.
Beyond its research value, our findings highlight the potential for eGDR to be incorporated into clinical risk assessment tools and public health frameworks. Because eGDR is derived from routinely collected clinical indicators, waist circumference, HbA1c, and hypertension status, it could be feasibly integrated into community health check-ups or electronic health record–based risk calculators to identify older adults at elevated risk of frailty. In clinical practice, eGDR may complement existing frailty assessment tools by introducing a metabolic dimension of risk, thereby enabling earlier identification of vulnerable individuals. From a public health perspective, targeting individuals with low eGDR through lifestyle interventions, such as promoting physical activity, optimizing dietary patterns, and managing body weight, may offer a scalable and cost-effective strategy to delay the onset and progression of frailty.
Our findings have important implications for both clinical practice and public health. Because eGDR is calculated from routinely collected clinical indicators, waist circumference, HbA1c, and hypertension status, it can be feasibly integrated into community health screenings or electronic health record–based risk calculators to identify older adults at elevated risk of frailty. In clinical settings, eGDR may complement existing frailty assessment tools by introducing a metabolic dimension of risk, thereby enabling earlier identification of vulnerable individuals. Importantly, eGDR is potentially modifiable: lifestyle interventions such as structured physical activity, dietary optimization, and weight management can reduce central adiposity and improve insulin sensitivity; optimizing glycemic control can lower HbA1c; and antihypertensive therapy and behavioral interventions can improve blood pressure regulation. Collectively, these strategies may enhance eGDR values and, in turn, help delay or prevent frailty progression. From a policy perspective, incorporating eGDR into preventive health programs could facilitate scalable and cost-effective strategies to mitigate the burden of frailty in aging populations.
This study has several notable strengths. To our knowledge, it is the first to comprehensively investigate the association between eGDR and both frailty onset and progression. Incident frailty among participants was assessed using multiple statistical approaches, including Cox regression and linear mixed-effects models, to provide a robust understanding of the temporal relationship between eGDR and frailty progression. The large sample size and extended follow-up period enabled a comprehensive evaluation of this association. Moreover, the inclusion of three well-established prospective cohorts from diverse ethnic backgrounds strengthens the external validity of our findings. Consistent associations observed across CHARLS, ELSA, and HRS underscore the generalizability of the results. Finally, the robustness of our findings was further supported through extensive sensitivity analyses.
Several limitations should be acknowledged in this study. First, all disease-related information was self-reported by participants, which may have introduced misclassification bias. However, previous validation studies have demonstrated that 77.5% of self-reported coronary heart disease cases in ELSA corresponded with medical record documentation40. Moreover, another study found that misreporting of stroke was largely nonsystematic, suggesting that self-reported stroke data in HRS are suitable for assessing both stroke incidence and its associated risk factors41. Based on this evidence, the likelihood of substantial misclassification bias appears limited. Second, although we adjusted for multiple potential confounders, some unmeasured factors, such as dietary and genetic influences, may still have contributed to IR and incident frailty42,43. Additionally, harmonized measures of dietary intake and physical activity were unavailable across CHARLS, ELSA, and HRS, precluding their inclusion in the models. Socioeconomic status was only partially captured through education level, a commonly used proxy in cross-cohort analyses. Therefore, residual confounding by unmeasured lifestyle or socioeconomic factors cannot be fully excluded. Third, participants with baseline frailty were excluded from the Cox regression analysis to reduce the risk of reverse causation. However, given that this was an observational study, definitive causal inference cannot be established. Fourth, only participants who completed follow-up surveys were included, which may have introduced selection bias. Individuals who were lost to follow-up due to severe frailty or death may have experienced rapid health deterioration, potentially leading to an underestimation of the association between eGDR and frailty. Fifth, in ELSA, mortality data were available only up to wave 6, whereas outcome data extended through wave 9. The absence of mortality information between waves 7 and 9 may have led to an overestimation of follow-up time, as participants lost to follow-up during this interval could not be definitively classified as deceased or censored due to non-response. This limitation may have introduced bias into the estimated associations. Sixth, although the K-means clusters did not differ significantly in frailty outcomes, this analysis underscores that individuals follow heterogeneous eGDR trajectories over time. This exploratory finding adds value by demonstrating that frailty risk in our cohorts was driven primarily by cumulative eGDR exposure, rather than by distinct trajectory subgroups. Finally, although our findings were consistent across three large cohorts, differences in study design, cultural context, and ethnic composition may limit generalizability. Further validation in independent and more diverse populations is warranted.
Conclusion
Our study demonstrated that the eGDR, a reliable indicator of IR, was strongly associated with incident frailty and may serve as a useful biomarker for identifying individuals at elevated risk. Individuals with lower eGDR levels were more likely to develop frailty during follow-up. These findings suggest that monitoring eGDR could facilitate the early identification of high-risk individuals and inform targeted preventive and management strategies aimed at reducing frailty risk in aging populations.
Data availability
This study was conducted using data that could be obtained from the official websites of the China Health and Retirement Longitudinal Study (http://charls.pku.edu.cn), the English Longitudinal Study of Ageing (http://ukdataservice.ac.uk), and the Health and Retirement Study (https://hrs.isr.umich.edu).
References
Clegg, A., Young, J., Iliffe, S., Rikkert, M. O. & Rockwood, K. Frailty in elderly people. Lancet 381, 752–762. https://doi.org/10.1016/s0140-6736(12)62167-9 (2013).
Hoogendijk, E. O. et al. Frailty: implications for clinical practice and public health. Lancet 394, 1365–1375. https://doi.org/10.1016/s0140-6736(19)31786-6 (2019).
Doody, P., Lord, J. M., Greig, C. A., Whittaker, A. C. & Frailty pathophysiology, theoretical and operational definition(s), impact, prevalence, management and Prevention, in an increasingly economically developed and ageing world. Gerontology 69, 927–945. https://doi.org/10.1159/000528561 (2023).
Xue, Q. L. The frailty syndrome: Definition and natural history. Clin. Geriatr. Med. 27, 1–15. https://doi.org/10.1016/j.cger.2010.08.009 (2011).
Guo, K. et al. Relationship between changes in the triglyceride glucose-body mass index and frail development trajectory and incidence in middle-aged and elderly individuals: A National cohort study. Cardiovasc. Diabetol. 23, 304. https://doi.org/10.1186/s12933-024-02373-1 (2024).
Fan, J. et al. Frailty index and all-cause and cause-specific mortality in Chinese adults: A prospective cohort study. Lancet Public. Health 5, e650–e660. https://doi.org/10.1016/s2468-2667(20)30113-4 (2020).
Cohen-Mansfield, J., Skornick-Bouchbinder, M. & Brill, S. Trajectories of end of life: A systematic review. J. Gerontol. B Psychol. Sci. Soc. Sci. 73, 564–572. https://doi.org/10.1093/geronb/gbx093 (2018).
Dent, E. et al. Management of frailty: Opportunities, challenges, and future directions. Lancet 394, 1376–1386. https://doi.org/10.1016/s0140-6736(19)31785-4 (2019).
Lee, S. H., Park, S. Y. & Choi, C. S. Insulin resistance: From mechanisms to therapeutic strategies. Diabetes Metab. J. 46, 15–37. https://doi.org/10.4093/dmj.2021.0280 (2022).
Dzięgielewska-Gęsiak, S. & Muc-Wierzgoń, M. Inflammation and oxidative stress in frailty and metabolic syndromes-two sides of the same coin. Metabolites. https://doi.org/10.3390/metabo13040475 (2023).
El Assar, M. et al. Frailty is associated with lower expression of genes involved in cellular response to stress: results from the Toledo study for healthy aging. J. Am. Med. Dir. Assoc. 18, 734.e731–734.e737 (2017).
El Assar, M. & Angulo, J. Rodríguez-Mañas, L. Frailty as a phenotypic manifestation of underlying oxidative stress. Free Radic. Biol. Med. 149, 72–77. https://doi.org/10.1016/j.freeradbiomed.2019.08.011 (2020).
Rodríguez-Mañas, L. et al. Dual effects of insulin resistance on mortality and function in non-diabetic older adults: Findings from the Toledo study of healthy aging. Geroscience 44, 1095–1108. https://doi.org/10.1007/s11357-021-00384-4 (2022).
Pérez-Tasigchana, R. F. et al. Metabolic syndrome and insulin resistance are associated with frailty in older adults: A prospective cohort study. Age Ageing 46, 807–812. https://doi.org/10.1093/ageing/afx023 (2017).
Peng, P. S. et al. Association between HOMA-IR and frailty among U.S. middle-aged and elderly population. Sci. Rep. 9, 4238. https://doi.org/10.1038/s41598-019-40902-1 (2019).
Zeng, P. et al. Association of metabolic syndrome severity with frailty progression among Chinese middle and old-aged adults: A longitudinal study. Cardiovasc. Diabetol. 23, 302. https://doi.org/10.1186/s12933-024-02379-9 (2024).
Zhao, Y., Hu, Y., Smith, J. P., Strauss, J. & Yang, G. Cohort profile: The China health and retirement longitudinal study (CHARLS). Int. J. Epidemiol. 43, 61–68. https://doi.org/10.1093/ije/dys203 (2014).
Steptoe, A., Breeze, E., Banks, J. & Nazroo, J. Cohort profile: the english longitudinal study of ageing. Int. J. Epidemiol. 42, 1640–1648. https://doi.org/10.1093/ije/dys168 (2013).
Sonnega, A. et al. Cohort profile: The health and retirement study (HRS). Int. J. Epidemiol. 43, 576–585. https://doi.org/10.1093/ije/dyu067 (2014).
Searle, S. D., Mitnitski, A., Gahbauer, E. A., Gill, T. M. & Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 8, 24. https://doi.org/10.1186/1471-2318-8-24 (2008).
He, D. et al. Associations of metabolic heterogeneity of obesity with frailty progression: Results from two prospective cohorts. J. Cachexia Sarcopenia Muscle. 14, 632–641. https://doi.org/10.1002/jcsm.13169 (2023).
He, D. et al. Preserved ratio impaired spirometry and COPD accelerate frailty progression: Evidence from a prospective cohort study. Chest 165, 573–582. https://doi.org/10.1016/j.chest.2023.07.020 (2024).
Moorhouse, P. & Rockwood, K. Frailty and its quantitative clinical evaluation. J. R Coll. Physicians Edinb. 42, 333–340. https://doi.org/10.4997/jrcpe.2012.412 (2012).
He, D. et al. Changes in frailty and incident cardiovascular disease in three prospective cohorts. Eur. Heart J. 45, 1058–1068. https://doi.org/10.1093/eurheartj/ehad885 (2024).
Parker, M., Bucknall, M., Jagger, C. & Wilkie, R. Population-based estimates of healthy working life expectancy in England at age 50 years: Analysis of data from the english longitudinal study of ageing. Lancet Public. Health. 5, e395–e403. https://doi.org/10.1016/s2468-2667(20)30114-6 (2020).
Bourassa, K. J., Ruiz, J. M. & Sbarra, D. A. Smoking and physical activity explain the increased mortality risk following marital separation and divorce: Evidence from the english longitudinal study of ageing. Ann. Behav. Med. 53, 255–266. https://doi.org/10.1093/abm/kay038 (2019).
Cisneros, B. et al. Immune system modulation in aging: Molecular mechanisms and therapeutic targets. Front. Immunol. 13, 1059173. https://doi.org/10.3389/fimmu.2022.1059173 (2022).
Scheithauer, T. P. M. et al. Gut microbiota as a trigger for metabolic inflammation in obesity and type 2 diabetes. Front. Immunol. 11, 571731. https://doi.org/10.3389/fimmu.2020.571731 (2020).
Guo, K. et al. Effect of aqueous extract of seed of broccoli on inflammatory cytokines and Helicobacter pylori infection: A randomized, double-blind, controlled trial in patients without atrophic gastritis. Inflammopharmacology 30, 1659–1668. https://doi.org/10.1007/s10787-022-01030-x (2022).
Mone, P. et al. Insulin resistance drives cognitive impairment in hypertensive pre-diabetic frail elders: The CENTENNIAL study. Eur. J. Prev. Cardiol. 30, 1283–1288. https://doi.org/10.1093/eurjpc/zwad173 (2023).
Santulli, G. et al. Frail hypertensive older adults with prediabetes and chronic kidney disease: insights on organ damage and cognitive performance - preliminary results from the CARYATID study. Cardiovasc. Diabetol. 23, 125. https://doi.org/10.1186/s12933-024-02218-x (2024).
Zhang, Z., Zhao, L., Lu, Y., Xiao, Y. & Zhou, X. Insulin resistance assessed by estimated glucose disposal rate and risk of incident cardiovascular diseases among individuals without diabetes: Findings from a nationwide, population based, prospective cohort study. Cardiovasc. Diabetol. 23, 194. https://doi.org/10.1186/s12933-024-02256-5 (2024).
He, H. M. et al. The additive effect of the triglyceride-glucose index and estimated glucose disposal rate on long-term mortality among individuals with and without diabetes: A population-based study. Cardiovasc. Diabetol. 23, 307. https://doi.org/10.1186/s12933-024-02396-8 (2024).
Yi, J., Qu, C., Li, X. & Gao, H. Insulin resistance assessed by estimated glucose disposal rate and risk of atherosclerotic cardiovascular diseases incidence: The multi-ethnic study of atherosclerosis. Cardiovasc. Diabetol. 23, 349. https://doi.org/10.1186/s12933-024-02437-2 (2024).
Li, Y., Li, H., Chen, X. & Liang, X. Association between various insulin resistance indices and cardiovascular disease in middle-aged and elderly individuals: Evidence from two prospectives nationwide cohort surveys. Front. Endocrinol. (Lausanne). 15, 1483468. https://doi.org/10.3389/fendo.2024.1483468 (2024).
Chillarón, J. J. et al. Insulin resistance and hypertension in patients with type 1 diabetes. J. Diabetes Complicat. 25, 232–236. https://doi.org/10.1016/j.jdiacomp.2011.03.006 (2011).
Grzelka-Woźniak, A. et al. Indirect insulin resistance markers are associated with nonalcoholic fatty liver disease in type 1 diabetes. Pol. Arch. Intern. Med. https://doi.org/10.20452/pamw.16404 (2023).
Linn, W. et al. Estimated glucose disposal rate is associated with retinopathy and kidney disease in young people with type 1 diabetes: A nationwide observational study. Cardiovasc. Diabetol. 22, 61. https://doi.org/10.1186/s12933-023-01791-x (2023).
Mao, Y. & Zhong, W. Changes of insulin resistance status and development of complications in type 1 diabetes mellitus: Analysis of DCCT/EDIC study. Diabetes Res. Clin. Pract. 184, 109211. https://doi.org/10.1016/j.diabres.2022.109211 (2022).
Xie, W., Zheng, F., Yan, L. & Zhong, B. Cognitive decline before and after incident coronary events. J. Am. Coll. Cardiol. 73, 3041–3050. https://doi.org/10.1016/j.jacc.2019.04.019 (2019).
Glymour, M. M. & Avendano, M. Can self-reported strokes be used to study stroke incidence and risk factors? Evidence from the health and retirement study. Stroke 40, 873–879. https://doi.org/10.1161/strokeaha.108.529479 (2009).
Watanabe, D. et al. Diet quality and physical or comprehensive frailty among older adults. Eur. J. Nutr. 61, 2451–2462. https://doi.org/10.1007/s00394-022-02819-w (2022).
Ye, Y. et al. A genome-wide association study of frailty identifies significant genetic correlation with neuropsychiatric, cardiovascular, and inflammation pathways. Geroscience 45, 2511–2523. https://doi.org/10.1007/s11357-023-00771-z (2023).
Acknowledgements
We would like to express our appreciation to the original data collectors, depositors, copyright holders, and funders of the China Health and Retirement Longitudinal Study, the English Longitudinal Study of Ageing, and the Health and Retirement Study.
Funding
This work was supported by the Drug Safety Research Project of Guangxi Zhuang Autonomous Region (Guiyaojiankezhishu[2023]017).
Author information
Authors and Affiliations
Contributions
Conception and design: Yan Li, Xi Ye, and Xueyan Liang. Collection of data: Yan Li. Data analysis and interpretation: All authors. Manuscript writing: Yan Li and Xueyan Liang. Final approval of manuscript: All authors. Funding acquisition: Yan Li.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The China Health and Retirement Longitudinal Study was approved by the Ethics Review Committee of Peking University. The English Longitudinal Study of Ageing was approved by the Ethics Review Committee of London Multi-Centre Research. The Health and Retirement Study was approved by the Ethics Review Committee of the University of Michigan. Informed consent was obtained from each subject in these three cohorts.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, Y., Ye, X., Chen, X. et al. Estimated glucose disposal rate and frailty in middle and older aged adults from three prospective cohorts. Sci Rep 16, 116 (2026). https://doi.org/10.1038/s41598-025-28740-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-28740-w
