
Abstract
Idiopathic pulmonary fibrosis (IPF) is an age-related interstitial lung disease of unknown cause. Oxidative stress, an imbalance between oxidants and antioxidants, is implicated in IPF pathogenesis and prognosis but needs further study. We used transcriptome sequencing data (GSE70866) and oxidative stress-related genes from GeneCards. A prognostic risk model for IPF patients was constructed using LASSO. Functional and pathway differences were analyzed between risk score groups, along with comparisons of immune cells and functions. An IPF rat model with vitamin D3 (VD3) intervention was also established. Finally, we used IL-4 to induce M2 macrophages to explore the mechanism of action of CCL2. We identified 483 DEGs and 50 oxidative stress-related DEGs (OSDEGs). Single-factor COX regression identified 34 prognostic OSDEGs, and LASSO identified an 8-gene signature for the risk model. The high-risk group had more CD8 + T cells, macrophages, APC costimulation, and cytokine-cytokine receptor activity. CCL2 was significantly correlated with macrophages in IPF. VD3 inhibited the TGF-β signaling pathway and reduced macrophage M2 infiltration in the rat model. In the IL-4 induced M2 macrophage model, we found that M2 macrophages produced more CCL2, and the production of CCL2 was significantly reduced after VD3 intervention. We established prognostic markers of eight oxidative stress-related genes. The risk score effectively predicts adverse outcomes in IPF. VD3 may alleviate IPF by reducing macrophage infiltration and inhibiting the TGF-β signaling pathway.
Similar content being viewed by others


Introduction
Idiopathic pulmonary fibrosis (IPF) is an age-related interstitial lung disease (ILD) of unknown etiology, characterized by a chronic progressive course, high morbidity, and poor survival rates1,2. Patients with IPF have a short life expectancy, with median survival rates of 50% at 3 years and 20% at 5 years post-diagnosis3,4. Currently, there are only two medications, nintedanib and pirfenidone, which have been shown to be both safe and efficacious in slowing disease progression5, albeit with varying degrees of adverse reactions6,7, and their therapeutic efficacy remains limited. Consequently, given its devastating nature, unclear pathogenesis, and challenging therapeutic prospects, there is an urgent need to explore novel biomarkers for the diagnosis, optimization of treatment, and prognosis assessment of IPF.
Oxidative stress is defined as an imbalance between the production of oxidants and antioxidant defenses, favoring the former. This leads to an increased generation of highly reactive free radicals, such as superoxide radicals (O2), hydrogen peroxide (H2O2), hydroxyl radicals (OH), hypochlorous acid (HOCl), and peroxynitrite (ONOO). Excessive production of reactive oxygen species (ROS) leads to oxidative stress, resulting in cellular damage. Numerous studies have reported the involvement of oxidative stress in the pathogenesis of IPF8,9,10. Recently, Fois et al. conducted a systematic review to describe the types of oxidative stress biomarkers identified in various biological samples from IPF patients, showing elevated levels of oxidative stress biomarkers across different sample types11, with further results indicating an increase in oxidative stress biomarker concentrations or a decrease in antioxidant markers irrespective of the type of biological sample12. These observations strongly support the involvement of oxidative stress in the occurrence and progression of IPF. However, the role of oxidative stress-related genes in the mechanisms and prognosis of IPF remains largely unconfirmed and requires further investigation.
Vitamin D3 (VD3) has been shown to play a crucial role in cell proliferation, differentiation, and immune regulation13. Previous studies have found that VD3 exhibits anti-fibrotic effects, reducing fibrotic lesions in various animal models14. The anti-fibrotic mechanisms of VD3 may be related to its ability to inhibit inflammation and epithelial-mesenchymal transition (EMT), as well as induce the expression of anti-fibrotic cytokines15.
In this study, differential gene expression (DEG) analysis was performed between control and IPF samples in the GSE70866 dataset, followed by intersection with oxidative stress-related genes to obtain oxidative stress-related differential gene expression (OSDEGs). Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment analyses were conducted for OSDEGs. Subsequently, based on univariate, least absolute shrinkage and selection operator (LASSO), and multivariate regression analyses, eight oxidative stress genes were included in the training set to establish a risk score prognostic model. Then, validation of the aforementioned risk model demonstrated it as an independent and reliable prognostic factor for IPF patients. Finally, we established an IPF rat model to explore the effects of VD3 intervention on IPF and we used IL-4 to induce M2 macrophages to explore the mechanism of action of CCL2. Overall, our results suggest that the oxidative stress-related gene CCL2 is a promising therapeutic target in IPF. VD3 can reduce the expression of CCL2 in IPF, potentially influencing macrophage M2 polarization.
Results
Identification of prognosis-related oxidative stress genes in IPF
We initially investigated the expression of differential genes between 20 normal samples and 176 IPF samples. Genes with p < 0.05 were considered as DEGs, resulting in a total of 483 DEGs (Fig. 1A). Intersection analysis with 1398 oxidative stress genes (out of which 1399 were identified, with 1 duplicate gene) yielded 50 genes considered as Oxidative Stress-Related Differential Genes (OSDEGs) (Fig. 1B). These OSDEGs were subjected to univariate Cox regression analysis. Results indicated that 34 oxidative stress-related genes were associated with prognosis in IPF patients (p < 0.05), with 5 genes upregulated and 29 genes downregulated (Fig. 1C). The Protein–Protein Interaction (PPI) network consisted of 64 nodes and 367 edges (Fig. 1D).

Identification of Prognosis-Related Oxidative Stress Genes. (A) Volcano plot of differential genes between normal samples and IPF samples. (B) Intersection of differential genes and oxidative stress genes. (C) Univariate COX regression analysis of OSDEGs. (D) Protein interaction diagram.
Construction of risk model
In order to select key genes from the aforementioned 34 genes, we conducted LASSO and multivariate Cox regression analyses to construct a risk score prognostic model. Finally, eight genes were identified to establish the risk score prognostic model (Fig. 2A,B). The risk score coefficients for these eight genes are presented in Table 1. Patients were stratified into high-risk and low-risk groups based on the median risk score as the dividing point according to the risk score formula. To evaluate the performance of the risk score model in predicting prognosis of IPF patients, Kaplan–Meier curves were generated. The results indicated that patients in the high-risk group had significantly shorter overall survival (OS) compared to those in the low-risk group (p < 0.001) (Fig. 2C). Additionally, the heatmap demonstrated significant differential expression of these eight genes between high-risk and low-risk patients (Fig. 2D). These findings suggest that we have constructed a risk model capable of predicting patient prognosis, with all eight genes comprising this gene signature showing elevated expression levels in IPF.

Construction of risk model. (A, B) LASSO regression analysis screens gene signatures to build risk models. (C) Survival curves of high-risk group samples and low-risk group samples. (D) Heat map of the expression levels of 8 genes in high-risk group and low-risk group samples for constructing the prognosis model.
Identification of risk models
The GAP index can be used as a simple and rapid method to assess the risk of IPF patients16. To determine whether the risk score-prognostic model is an independent prognostic factor for IPF, univariate and multivariable regression analyzes were performed. We integrated risk scores and clinical parameters (including age, sex, and GAP index) for analysis. Univariate regression analysis showed that GAP index and risk score were associated with prognosis (Fig. 3A). In multivariable regression analysis, risk score and GAP index proved to be an independent prognostic indicator (Fig. 3B). We further performed ROC analysis to evaluate the risk score. The area under the ROC curve (AUC) values were 0.860 for 1 year, 0.857 for three years, and 0.910 for 5 years (Fig. 3C). These findings indicate that the risk score prognostic model is reliable in predicting survival in patients with IPF.

Identification of risk models. (A) Univariate COX regression analysis. (B) Univariate COX regression analysis. (C) ROC curve to show the accuracy of the model.
GO and KEGG enrichment analysis
To gain further insights into the role of these OSDEGs in IPF, we conducted GO and KEGG enrichment analyses. GO analysis categorizes genes into three classes: Biological Process (BP), Cellular Component (CC), and Molecular Function (MF). Regarding BP, DEGs were predominantly enriched in oxidative stress-related leukocyte migration, cell chemotaxis, and leukocyte chemotaxis. Concerning CC, the top two enriched terms were oxidative stress-related endocytic vesicle and apical part of cell. As for MF, the top two terms were cytokine activity and receptor ligand activity (Fig. 4A). In terms of KEGG pathways, DEGs were also enriched in oxidative stress-related pathways, with the most significant pathway being the cytokine-cytokine receptor interaction pathway (Fig. 4B). These findings suggest that OSDEGs may exert their effects in IPF through these functionalities.

Enrichment analysis. (A, B) GO and KEGG enrichment analysis.
Comparative analysis of immune function
Bronchoalveolar lavage fluid (BALF) of IPF patients contains blood cells that may affect the progression of pulmonary fibrosis17,18. Therefore, we explored the levels of immune cell infiltration in high- and low-risk populations. We found that the high-risk group still had more macrophages than the low-risk group (Fig. 5A). In addition, the high-risk group showed high scores for antigen-presenting cell (APC) costimulation, cytokine-cytokine receptor (CCR) interaction, inflammatory side reaction checkpoint, Cytolytic-activity, and Parainflammation (Fig. 5B).

Relationship between risk score and IPF immune cells and immune function. (A) Boxplot showing the difference in immune cell infiltration level between the high and low OSDEGs score groups. (B) Boxplot showing the difference in immune function between the high and low OSDEGs score groups. (*P < 0.05, **P < 0.01, ***P < 0.001).
Validation of the model in the test set
In order to further verify the universality of the risk scoring model on the training set, the obtained formula was applied to the test set. Calculate the risk score for each patient in the test set based on the formula in the training set. Subsequently, patients in the test set were divided into high-risk and low-risk groups based on the median risk score in the training set. Similarly, we found that patients in the high-risk group had worse OS than the low-risk group in the test set (Fig. 6A). In addition, the AUC for the one-, three-, and five-year risk scores were 0.850, 0.847, and 0.922, respectively (Fig. 6B). Univariate regression analysis showed that GAP index and risk score were associated with prognosis (Fig. 6C). In multivariable regression analysis, risk score and GAP index proved to be an independent prognostic indicator (Fig. 6D). Regarding immune cells or immune function, we explored the infiltration levels of immune cells in high-risk and low-risk groups in the test set. We found that the high-risk group had more CD8 + T cells and macrophages than the low-risk group (Fig. 6E). The high-risk group still showed APC costimulation, CCR interaction, and inflammatory side effects. High scores for checkpoints, Cytolytic-activity and Parainflammation (Fig. 6F). These findings demonstrate the generalizability and robustness of risk score prognostic models.

Identification of risk models. (A) Survival curves of high-risk group samples and low-risk group samples. (B) ROC curve to show the accuracy of the model. (C) Univariate COX regression analysis. (D) Univariate COX regression analysis. (E) Boxplot showing the difference in immune cell infiltration level between the high and low OSDEGs score groups. (F) Boxplot showing the difference in immune function between the high and low OSDEGs score groups. (*P < 0.05, **P < 0.01, ***P < 0.001).
The role of CCL2 in IPF
These studies highlight the significant roles of hub genes in the immune cells and immune microenvironment in IPF. To identify suitable targets, we further analyzed the correlations between ACOX2, ADM, CCL2, NRG1, PLA2G7, SFTPB, SPP1, SOD3, and immune cells (Fig. 7). In both the training and test groups, we found that CCL2, PLA2G7, and SPP1 were significantly positively correlated with macrophage infiltration in IPF (Fig. 7A,B). Combined with the results from Fig. 1D and Supplementary Table 3, CCL2 appears to have a more critical significance in IPF.

IPF and Macrophage Infiltration. (A, B) Correlation of immune cell infiltration levels with hub genes in the training and test groups of IPF. (*P < 0.05, **P < 0.01, ***P < 0.001).
Establishment of an IPF rat model
To further investigate the mechanism of action of CCL2 in idiopathic pulmonary fibrosis (IPF), we constructed an IPF rat model. In this study, we first measured the body weight and lung weight of the SD rats. This step was not only to assess the effectiveness of the model establishment but also to physiologically evaluate the severity of pulmonary fibrosis. IPF is a progressive lung disease that is usually accompanied by structural and functional changes in lung tissue. Pulmonary fibrosis can lead to a decline in gas exchange capacity, ultimately affecting overall respiratory function. Therefore, we chose the ratio of body weight to lung weight (lung coefficient) as our evaluation index.
The experimental results showed that the lung coefficient of rats in the model group was significantly higher than that of the control group, indicating that the bleomycin-induced IPF model was successfully established (Table 2). Specifically, the lung weight of the model group increased, while body weight relatively decreased, reflecting a negative correlation between pathological changes in the lungs and physiological status. Among the treatment groups, we observed a significant reduction in lung coefficients in the anti-CCL2 group, VD3 group, and combination treatment group (anti-CCL2 + VD3), suggesting that these interventions effectively alleviated lung lesions to some extent (Fig. 8). However, despite the decrease in lung coefficients in these treatment groups compared to the model group, they remained higher than in the control group, indicating that although the interventions had some therapeutic effect, they may not have fully reversed the pathological changes induced by bleomycin. This suggests that single interventions may not fully restore lung function, and future research may need to explore more comprehensive multi-target treatment strategies.

Lung coefficients of rats in different treatment groups. Compared to the model group versus control group, p ≤ 0.05 is marked as *, p ≤ 0.01 is marked as **; comparisons of the remaining groups with the model group: p ≤ 0.05 is marked as #, p ≤ 0.01 is marked as ##.
Histological assessment of lung fibrosis
To further validate the establishment of the pulmonary fibrosis model, we performed hematoxylin and eosin (H&E) and Masson’s trichrome staining. H&E staining allowed for visualization of tissue architecture and revealed infiltration of inflammatory cells and structural alterations within the lung tissue. In the model group (Fig. 9), H&E staining demonstrated a marked chronic inflammatory response, characterized by the infiltration of lymphocytes, monocytes, and macrophages. Furthermore, prominent pathological changes, including alveolar wall thickening and airway remodeling, consistent with the hallmarks of idiopathic pulmonary fibrosis (IPF), were observed. Masson’s trichrome staining, specific for collagen deposition, revealed a significant increase in blue-stained collagen fibers in the model group, indicating a positive correlation between collagen deposition and the extent of fibrosis (Fig. 10), and this observation highlighting the crucial role of aberrant collagen deposition in the pathogenesis of this disease.

H&E staining of different treatment groups.

Masson’s trichrome staining of different treatment groups.
Ashcroft scoring
Quantitative assessment of lung fibrosis using the Ashcroft scoring system revealed a significant increase in fibrosis in the model group compared to the control group (p < 0.001). The model group exhibited a mean Ashcroft score of 6.36 ± 0.29, while the control group showed a mean score of 1.22 ± 0.17. Treatment with anti-CCL2 and VD3 individually resulted in a significant reduction in Ashcroft scores compared to the model group (p < 0.001 for both treatments). The anti-CCL2 group had a mean score of 4.44 ± 0.25, and the VD3 group had a mean score of 5.12 ± 0.22. Combined treatment with anti-CCL2 and VD3 further attenuated the Ashcroft score to 3.16 ± 0.20, demonstrating a greater reduction in fibrosis compared to either monotherapy (p < 0.001 for both comparisons)(Fig. 11).

Ashcroft Scoring of different treatment groups.
VD3 inhibits CCL2 expression to alleviate lung fibrosis
The Transforming Growth Factor β (TGF-β) superfamily signaling pathways play a crucial role in regulating cell growth, differentiation, and development across various biological systems. Generally, signal transduction is initiated by ligand-induced serine/threonine receptor kinase oligomerization and the phosphorylation of cytoplasmic signaling molecules19, which is a key pathogenic mechanism in IPF. Therefore, we validated this in WB analysis, we repeated the results three times, and the samples were in the following order: Model, Con, VD3, VD3 + CCL2, and CCL2 (Fig. 12). The results showed that the TGF-β signaling pathway expression was significantly elevated in the IPF model, while the expression level of p-Smad3 significantly decreased after CCL2 silencing. Following VD3 intervention, CCR2 levels were notably reduced, indicating that VD3 can significantly reduce macrophage infiltration in IPF, thereby improving the condition. Unprocessed WB original images in Supplementary Fig. 1.

WB of VD3 Intervention in IPF.
Immunofluorescence
We used immunofluorescence to analyze the differences in the expression of the macrophage M2 marker (CD206) between the IPF model group and the control group (Fig. 13). The results showed that macrophage M2 infiltration levels were significantly higher in the model group compared to the normal control group, indicating that macrophage M2 plays a significant role in IPF.

Expression of macrophage M2 marker CD206 in the IPF model.
Induction of M2 macrophages
In previous studies, we have identified a correlation between M2 macrophages and CCL2. Subsequently, we explored the causal relationship between M2 macrophages and CCL2 through the induction of M2 polarization in cells (Fig. 14). Our results showed that, compared to the control group, the expression of CCL2 was significantly elevated in the M2 macrophage induction group. After VD3 intervention, the expression of CCL2 significantly decreased. These results suggest that M2 polarization can produce more CCL2, which plays an important role in its function in IPF, and that VD3 intervention can reduce the production of CCL2 by M2 macrophages. This finding provides reliable support for our understanding of the mechanism of action of M2 macrophages in IPF.

Expression of CCL2 and CD206 among different treatment groups. Comparison of the model group with the control group showed p ≤ 0.0001, marked as ****, and p ≤ 0.01, marked as **.
Discussion
IPF is a chronic disease characterized by lung structural damage, fibrosis, and loss of function, the etiology and pathogenesis of which remain incompletely understood12. Bronchoalveolar lavage (BAL) cells aggregate on the outer surface of the alveoli, typically collected via bronchoscopy, and their gene expression profiles can predict survival in IPF20. Therefore, constructing a multi-gene signature of BAL cells is crucial for predicting the prognosis of IPF patients21. Oxidative stress may play a crucial role in the development of IPF, influencing the onset and progression of the disease22. Oxidative stress arises from an imbalance between the production of reactive oxygen species (ROS) and reactive nitrogen species (RNS) and antioxidant defenses, leading to cellular dysfunction and tissue damage. Exogenous or endogenously generated ROS/RNS may directly damage the alveolar epithelium, promoting fibrotic interstitial lung responses8. Besides directly damaging the lung epithelium, ROS/RNS may also promote pulmonary fibrosis by altering the expression of mediators implicated in the pathogenesis of IPF, such as the pro-fibrotic growth factor, transforming growth factor β (TGF-β). Additionally, the oxidative stress mechanism of IPF involves Reduced GSH23, superoxide dismutase24, catalase25, among others. In this study, by analyzing oxidative stress-related genes in bronchoalveolar lavage fluid, we investigated the potential roles of these genes in the prognosis of IPF. The results showed a series of differentially expressed oxidative stress-related genes in the bronchoalveolar lavage fluid of IPF patients, some of which are associated with patient prognosis (ACOX2, ADM, CCL2, NRG1, PLA2G7, SFTPB, SPP1, SOD3). These genes intertwine in the pathological process of IPF, potentially influencing inflammation, fibrosis, and lung structural damage and remodeling through multiple key pathways. Furthermore, the differential expression of these genes may reveal the roles of oxidative stress in different stages of IPF development, providing new clues for predicting disease progression and patient survival prognosis.
In this study, eight key genes associated with prognosis were identified (ACOX2, ADM, CCL2, NRG1, PLA2G7, SFTPB, SPP1, SOD3), with CCL2 being the most significant gene. Additionally, CCL2 was identified as one of the top 10 hub genes in the PPI network. Substantial evidence from animal models and human data suggests the involvement of CCL2 in the pathogenesis of pulmonary fibrosis26. CCL2 acts as a chemotactic agent, participating in the recruitment of fibroblasts and pro-fibrotic macrophages27. Conversely, macrophages can also secrete CCL2 to promote pulmonary fibrosis28. Typically, CCL2 exerts its pro-fibrotic effects by binding to its receptor CCR2. The role of CCR2 signaling in fibrosis was initially confirmed in the FITC model of pulmonary fibrosis29. Importantly, the pro-fibrotic properties of CCR2 have subsequently been validated in many other pulmonary fibrosis supplementary models27. Elevated levels of CCL2 and its receptor (CCR2) have also been observed in patients with chronic heart failure, leading to the recruitment and differentiation of pulmonary monocytes, which may exacerbate pulmonary fibrosis and worsen patients’ respiratory difficulties30. This study identified CCL2 as one of the key genes involved in IPF induced by oxidative stress. However, the specific mechanism remains unclear and warrants further investigation to elucidate the relationship between CCL2, oxidative stress, and IPF.
In this study, it was found that the high-risk group of IPF had more CD8 + T cells and macrophages compared to the low-risk group, with macrophages showing the most significant difference. Macrophages are the most abundant leukocytes in the airway and play a crucial role in regulating immune responses31. Known for their ability to generate reactive oxygen species (ROS) and reactive nitrogen species (RNS), they act as a defense mechanism against invading pathogens32. The host protects itself from these reactive species by increasing the expression of antioxidants. Oxidative stress arises from an imbalance between the generation of oxidants and antioxidant defense mechanisms33. This imbalance in interstitial pulmonary fibrosis diseases may be related to disease development and severity33. Most studies suggest that M2 macrophages, rather than M1 phenotype, are involved in the process of pulmonary fibrosis. Generally, M2 macrophages act as important regulators of fibrosis, exacerbating the progression of pulmonary fibrosis34,35. M2 polarization agents promote fibrosis progression. A study found that rat overexpressing IL-10 could lead to pulmonary fibrosis, with a significant increase in the number of M2 macrophages not only in bronchoalveolar lavage fluid but also in whole lung tissue36. One study found that the loss of phosphatase and tensin homolog maintained PI3K activation and promoted M2 macrophage phenotype, resulting in exacerbation of bleomycin-induced pulmonary fibrosis37. Additionally, the tyrosine phosphatase Shp2 inhibits M2 macrophage polarization by regulating JAK1/STAT6 activity and prevents bleomycin-induced pulmonary fibrosis38. The therapeutic effects of recombinant TNF-α are observed in rat with bleomycin-induced fibrosis, where it diminishes the pro-fibrotic M2 phenotype39. During bleomycin-induced pulmonary fibrosis, IL-33 induces the expression of IL-13 and TGF-β1 via ST2 signaling. The polarization of M2 macrophages is induced by IL-33 and IL-13 synergistically. Treatment with anti-IL-33 antibodies and ST2 deficiency can alleviate lung inflammation and fibrosis induced by bleomycin40. Macrophages are divided into M1 and M2 types, each exhibiting different metabolic characteristics regulated by oxidative-reductive mechanisms that modulate their polarization in various subgroups41. Oxidative stress activates glycolysis and lipid biosynthesis but maintains the M1 phenotype by inhibiting the tricarboxylic acid cycle and oxidative phosphorylation. Due to changes in the redox state, these metabolic characteristics of M2 macrophages are reversed42. Macrophages play numerous functional roles under physiological and pathological conditions, and these processes are closely associated with the synthesis of cytokines, ROS, and nitrogen species (ROS/RNS)43. Thus, redox signaling is one of the major regulatory factors in macrophage reprogramming. However, the relationship between macrophages and oxidative stress in IPF has not been clearly elucidated.
In clinical studies of pulmonary fibrosis, the mortality rate of patients is associated with their levels of VD344. It has been reported that VD3 inhibits the fibrotic phenotype of lung fibroblasts and epithelial cells induced by the pro-fibrotic factor TGF-β45. The TGF-β signaling pathway is a typical pathway involved in the occurrence and development of IPF46. The selective activation of macrophages (M2) is primarily achieved through the secretion of pro-fibrotic cytokines such as TGF-β. TGF-β is considered the most important pro-fibrotic cytokine47. Our results show that after VD3 treatment, TGF-β-related markers were significantly reduced, and the expression level of CCR2 also decreased accordingly. Immunofluorescence results indicate that the level of macrophage M2 infiltration in IPF significantly decrease. Subsequently, we investigated the causal relationship between macrophage M2 and CCL2 through induced macrophage M2 polarization in cells. Our results show that, compared to the control group, the expression level of CCL2 significantly increased in the macrophage M2-induced group. After VD3 intervention, the expression level of CCL2 significantly decreased. This result suggests that macrophage M2 polarization can produce more CCL2, which is an important mechanism by which it exerts its effects in IPF, and that VD3 intervention can reduce the production of CCL2 by macrophage M2. This finding provides reliable support for understanding the mechanism of macrophage M2’s role in IPF.
While the potential mechanisms underlying the susceptibility to oxidative stress in pulmonary diseases have been a hot research topic in recent years, the elusive regulatory mechanisms between IPF immunity and oxidative stress remain elusive. Based on differential genes between different risk groups, functional enrichment analysis was conducted, revealing enrichment in inflammation and immune-related pathways. Indeed, inflammation and immune-related pathways play crucial roles in the development of IPF, where immune processes can coordinate existing fibrotic responses48. Interestingly, in terms of immune function, the high-risk group exhibited higher scores in antigen-presenting cells (APC) co-stimulation, chemokine-chemokine receptor (CCR) interactions, inflammation-related checkpoint, cytolytic activity, and parainflammation, with CCR showing the greatest differential expression. Numerous studies have found that chemokine and chemokine receptor signaling play roles in cell migration, activation, and lung injury repair responses, including IPF, and neutralizing antibodies against chemokines may help treat IPF49,50. These findings align with our study conclusions. However, specific mechanisms require further investigation.
Finally, this study has some limitations. First, our data came from GEO, a relatively small sample. Although we constructed a rat IPF model, we still lacked a clinical sample for comparison. Second, building a predictive model based on a single trait while ignoring other traits may result in the exclusion of many important IPF prognostic genes. Finally, the therapeutic role of VD3 still needs to be further validated in clinical samples.
Conclusion
In summary, this study established novel prognostic markers consisting of eight oxidative stress-related genes. The risk score may serve as an effective model for predicting adverse outcomes in IPF. Subsequently, we found that CCL2 is positively correlated with macrophage infiltration levels in IPF, and that VD3 intervention can alleviate IPF by reducing macrophage infiltration and inhibiting the TGF-β signaling pathway.
Methods
Data download and preparation
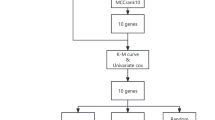
The dataset GSE70866 was downloaded from the Gene Expression Omnibus (GEO) database website (GEO, www.ncbi.nlm.nih.gov/geo)51. This dataset comprises two platform files, GPL14550 and GPL17077, containing clinical data and prognostic information of IPF patients. We utilized the mRNA expression profiles from GPL14550 (including 20 healthy controls and 112 IPF patients) as the training set, and the mRNA expression profiles from GPL17077 (comprising 64 IPF patients) as the validation set. Standardization of expression data was performed using the R “limma” package. Ethical approval from the hospital ethics committee was not required for this study since GEO data is publicly available, and we strictly adhered to GEO’s data access policies and publication guidelines. Clinical information for the GSE70866 cohort is presented in Supplementary Table 1. Further analysis involved downloading 1399 oxidative stress-related genes with relevance scores ≥ 7 from the GeneCards database (https://www.genecards.org) for subsequent investigation (Supplementary Table 2). The overall design of the study is presented in a flow diagram (Fig. 15).

Flowchart.
Identification of oxidative stress-related OSDEGs
The “limma” R software package was utilized to investigate differential gene expression (DEG) between normal and IPF samples. Genes with p < 0.05 and |logFC|> 1 were considered DEGs. Subsequently, the intersection of oxidative stress-related genes with DEGs was applied to obtain oxidative stress-related differential genes (OSDEGs).
Construction and validation of risk score prediction model
Univariate Cox regression analysis was performed on the training set to identify prognosis-related genes among OSDEGs. To mitigate the risk of overfitting, we employed the Least Absolute Shrinkage and Selection Operator (LASSO) Cox regression model via the glmnet R package52,53. The formula for the risk score model was as follows: risk score = Σ (βi * Expi), where βi denotes the LASSO coefficient of the i-th gene and Expi represents the expression value of the i-th candidate gene. Risk scores for each sample were computed using this formula. Samples were stratified into high-risk and low-risk groups based on the median risk score. Multifactorial prognostic analysis results for the subgroups associated with cellular necrosis were obtained using the “forestplot” package. Kaplan–Meier analysis and log-rank tests were performed using the “survival” R package to compare survival differences between the two risk groups. The predictive accuracy of the model was evaluated using receiver operating characteristic (ROC) curves with the “survival ROC” R package54. The distribution of risk scores among IPF patients and the correlation between survival time and risk scores were visualized using the “pheatmap” R package. To validate whether our prognostic model was applicable to other datasets, external validation was conducted using an independent IPF dataset as the test set.
Correlation analysis between risk score and clinical parameters
The Gender-Age-Physiology (GAP) index is a staging system for IPF patients, which utilizes gender (G), age (A), and two lung physiology variables (P), including forced vital capacity (FVC) and diffusing capacity for carbon monoxide (DLCO)16. IPF samples were stratified into different groups based on clinical parameters, and the differences in risk scores between these groups were compared.
GO and KEGG enrichment analysis
The differential expression genes of the risk model were subjected to Gene Ontology (GO) enrichment analysis using the R package "clusterprofiler." The background gene set "org.Hs.eg.db" was selected for human genome annotation, covering biological processes (BP), cellular components (CC), and molecular functions (MF). Screening criteria included pvalueCutoff = 0.05 and qvalueCutoff = 0.05. Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis was conducted using the same tool based on KEGG database.
Immune cell infiltration and immune-related functional analysis
A recent variant of Gene Set Enrichment Analysis (GSEA) is single-sample gene set enrichment analysis (ssGSEA)55. By employing ssGSEA, the gene expression data of the sample set are compared with the gene expression data provided by the gene set, and enrichment scores are calculated. A higher enrichment score indicates a greater degree of enrichment. In this study, we evaluated marker genes for 28 different types of immune cells, determined the enrichment scores of immune cells in each sample, and subsequently conducted further analysis.
BLM-induced rat IPF model and drug treatment protocol
Adult male rats were purchased from Beijing Vital River Laboratory Animal Technology Co., Ltd. (Beijing, China). The rats were acclimatized for 7 days before the start of the experiment. All rat were housed under standard 12-h light/dark cycles (lights on at 8:00 AM), at a constant temperature of (24 ± 1) °C, with a relative humidity of (45 ± 15%), and had free access to food and water. All experimental procedures involving the rat were conducted in accordance with the guidelines of the Institutional Animal Care and Use Committee. The protocol was approved by the Animal Experiment Ethics Committee of the Fifth Affiliated Hospital of Zhengzhou University (Approval No.: KY-D-2024025). We selected 15 male SD rats aged 6–8 weeks and randomly divided them into five groups: the control group, model group, anti-CCL2 group, VD3 group, and anti-CCL2 + VD3 group. To induce lung fibrosis, intratracheal administration of 2.0 mg/kg Bleomycin (BLM) in saline was performed56. Rat in the CCL2 group were injected with CCL2-shRNA lentivirus (LV-shRNA-CCL2). The target sequence, from 5′ to 3′, was TCGCGAGCTATAGAAGAAT. After 14 days of BLM treatment, VD3 (2 μg/kg) was administered by intraperitoneal injection once a day for 14 days in VD3 group. Finally, 24 h after the last dosage, the rats were weighed, and the whole lungs were harvested. The lungs were carefully removed, and the lung weight was recorded. The left lung was rapidly frozen in liquid nitrogen, while the right lung was subjected to fixation to prepare for subsequent histological analysis.
Hematoxylin and eosin (H&E) staining
Fresh lung tissues were fixed in formalin for at least 24 h to ensure complete fixation. Following fixation, the target areas were trimmed using a scalpel and dehydrated through a graded series of ethanol solutions. The tissues were then embedded in paraffin wax after infiltration at 65 °C. Sections of 4 μm thickness were cut using a microtome, deparaffinized, and stained with hematoxylin. After rinsing with tap water and differentiation, sections were blued using a bluing agent. Subsequently, the sections were dehydrated through a graded ethanol series and mounted with neutral mounting medium.
Masson’s trichrome staining
Paraffin-embedded sections were deparaffinized using a xylene substitute and anhydrous ethanol, followed by a rinse with tap water to remove residual alcohol. Cryosections were allowed to reach room temperature after retrieval from − 20°C storage and fixed for 15 min in formalin. Sections were then stained overnight with Masson’s A solution and rinsed with tap water the following day. Masson’s B and C solutions were mixed in equal proportions and applied to the sections for 1 min, followed by differentiation. Sections were subsequently stained with Masson’s D solution for 6 min and Masson’s E solution for 1 min. Without rinsing in water, the sections were briefly drained and stained with Masson’s F solution. Finally, sections were rinsed with 1% acetic acid, dehydrated, cleared, and mounted with neutral mounting medium.
Ashcroft scoring
Lung fibrosis was assessed using the Ashcroft scoring system. Paraffin-embedded lung sections stained with H&E were examined under a light microscope. Five random fields were selected per section, and each field was assigned a score from 0 to 8 based on the degree of fibrotic changes, according to the established Ashcroft criteria57 (Table 3). The scores for the five fields were averaged to obtain a mean Ashcroft score for each lung section. A higher score indicates a greater degree of fibrosis. The observer performing the scoring was blinded to the experimental groups.
Induction of M2 macrophages
Cells were cultured in DMEM medium containing 10% fetal bovine serum and 1% penicillin/streptomycin, ensuring that the cells grew under conditions of 37 °C and 5% CO₂. When the cells reached 70–80% confluence, they were washed twice with PBS, followed by digestion with trypsin. Gentle agitation was applied to facilitate digestion, typically lasting 2–5 min. After digestion, fresh medium was added to neutralize the trypsin, and then the cells were centrifuged to remove the supernatant and resuspended in culture medium, adjusting the cell concentration to 1 × 108 cells/ml.
Based on this, the cells were seeded into 6-well plates or culture flasks, and 20 ng/ml of recombinant IL-4 was added to induce polarization, mixed gently to avoid bubble formation. The cells were then placed in a 37 °C, 5% CO₂ incubator for 24 h. The cells were divided into three groups: the control group, the induced M2 macrophage group, and the induced M2 macrophage + VD3 treatment group. In the induced M2 macrophage + VD3 treatment group, 50 nM VD3 was administered for 24 h.
Western blot analysis
Lung tissues from rat lungs, were collected and stored in liquid nitrogen. For protein extraction, tissues or cells were homogenized in ice-cold RIPA lysis buffer containing phenylmethylsulfonyl fluoride (China Biosharp) and a phosphatase inhibitor cocktail (Sigma, USA). After centrifugation at 14,000 xg for 30 min at 4 °C, the supernatant was collected as the total protein, and the protein concentration was determined using the BCA Protein Assay Kit (Thermo Fisher Scientific, USA).
Equal amounts of protein (20 μg) were separated by 10% SDS-PAGE and transferred to a PVDF membrane. The membrane was blocked with 5% non-fat milk at room temperature for 1 h and then incubated overnight at 4 °C with primary antibodies. The next day, the membrane was washed three times with TBST and incubated with secondary antibodies at room temperature for 1 h. Finally, protein bands were visualized using a chemiluminescence reagent (Thermo Fisher Scientific, USA). ImageJ software was used for image analysis.
The following primary antibodies were used: Smad3 (Abcam, ab40854), p-Smad3 (Abcam, ab52903), CCR2 (Abcam, ab273050), TGF-β (Abcam, ab215715), and GAPDH (Abcam, ab8245).
Immunofluorescence assay
Tissues were fixed with 4% paraformaldehyde for 30 min. Fixed tissues were washed and permeabilized with 0.1% Triton X-100 for 10 min. Tissues were blocked with goat serum for 30 min and incubated with the anti-β-catenin antibody (1:100, 8480S, CST) overnight at 4 °C. After washing with PBS, the cells were subsequently incubated with Alexa Fluor 488-conjugated anti-rabbit IgG antibody (1:1000, ab150077, Abcam) for 1 h. The nuclei were stained with DAPI (62248, Thermo Scientific). Images were acquired using a Zeiss LSM710 confocal microscope (Zeiss, Germany) at 100 × magnification.
Statistical analysis
Statistical analysis was performed using R software (version 4.1.3). The comparison of gene expression between two groups was conducted using the Wilcoxon test. Univariate Cox regression, LASSO, and multivariate Cox regression analyses were carried out to identify prognosis-related genes. Kaplan–Meier analysis combined with log-rank tests was employed to explore the differences in overall survival (OS) between the two groups of patients. The accuracy of the risk score prognostic model was evaluated using ROC analysis. Statistical results were visualized using GraphPad software (version 8.0). A significance level of p < 0.05 was considered statistically significant.
Data availability
Publicly available datasets were analyzed in this study. This data can be found here: Gene Expression Omnibus (GEO, available at: https://www.ncbi.nlm.nih.gov/geo/) database.
Abbreviations
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under curve
- GO:
-
Gene ontology
- KEGG:
-
Kyoto encyclopedia of genes and genome
- PPI:
-
Protein–protein interaction
- GEO:
-
Gene Expression Omnibus
- IPF:
-
Idiopathic pulmonary fibrosis
- LASSO:
-
Least absolute shrinkage and selection operator
References
Raghu, G. et al. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 183(6), 788–824 (2011).
Lederer, D. J. & Martinez, F. J. Idiopathic pulmonary fibrosis. N. Engl. J. Med. 378(19), 1811–1823 (2018).
Cho, S. J. & Stout-Delgado, H. W. Aging and lung disease. Annu. Rev. Physiol. 82, 433–459 (2020).
Vancheri, C., Failla, M., Crimi, N. & Raghu, G. Idiopathic pulmonary fibrosis: A disease with similarities and links to cancer biology. Eur. Respir. J. 35(3), 496–504 (2010).
Spagnolo, P. et al. Idiopathic pulmonary fibrosis: Disease mechanisms and drug development. Pharmacol. Ther. 222, 107798 (2021).
Heukels, P., Moor, C. C., von der Thusen, J. H., Wijsenbeek, M. S. & Kool, M. Inflammation and immunity in IPF pathogenesis and treatment. Respir. Med. 147, 79–91 (2019).
Galli, J. A. et al. Pirfenidone and nintedanib for pulmonary fibrosis in clinical practice: Tolerability and adverse drug reactions. Respirology 22(6), 1171–1178 (2017).
Brenner, D. A. Molecular pathogenesis of liver fibrosis. Trans. Am. Clin. Climatol. Assoc. 120, 361–368 (2009).
Cheresh, P., Kim, S. J., Tulasiram, S. & Kamp, D. W. Oxidative stress and pulmonary fibrosis. Biochim. Biophys. Acta 1832(7), 1028–1040 (2013).
Kliment, C. R. & Oury, T. D. Oxidative stress, extracellular matrix targets, and idiopathic pulmonary fibrosis. Free Radic. Biol. Med. 49(5), 707–717 (2010).
Fois, A. G. et al. Evaluation of oxidative stress biomarkers in idiopathic pulmonary fibrosis and therapeutic applications: A systematic review. Respir. Res. 19(1), 51 (2018).
Paliogiannis, P. et al. Oxidative stress-linked biomarkers in idiopathic pulmonary fibrosis: A systematic review and meta-analysis. Biomark. Med. 12(10), 1175–1184 (2018).
Artaza, J. N., Sirad, F., Ferrini, M. G. & Norris, K. C. 1,25(OH)2vitamin D3 inhibits cell proliferation by promoting cell cycle arrest without inducing apoptosis and modifies cell morphology of mesenchymal multipotent cells. J. Steroid. Biochem. Mol. Biol. 119(1–2), 73–83 (2010).
Huang, G. R. et al. Mechanism of combined use of vitamin D and puerarin in anti-hepatic fibrosis by regulating the Wnt/beta-catenin signalling pathway. World J. Gastroenterol. 24(36), 4178–4185 (2018).
Park, J. W. et al. Renoprotective effects of paricalcitol on gentamicin-induced kidney injury in rats. Am. J. Physiol. Renal. Physiol. 298(2), F301-313 (2010).
Ley, B. et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann. Intern Med. 156(10), 684–691 (2012).
Lv, M., Liu, Y., Ma, S. & Yu, Z. Current advances in idiopathic pulmonary fibrosis: The pathogenesis, therapeutic strategies and candidate molecules. Future Med. Chem. 11(19), 2595–2620 (2019).
Yin, Y. Q. et al. Construction of prediction model of inflammation related genes in idiopathic pulmonary fibrosis and its correlation with immune microenvironment. Front. Immunol. 13, 1010345 (2022).
Yadav, H. et al. Protection from obesity and diabetes by blockade of TGF-beta/Smad3 signaling. Cell Metab. 14(1), 67–79 (2011).
Prasse, A. et al. BAL cell gene expression is indicative of outcome and airway basal cell involvement in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 199(5), 622–630 (2019).
He, Y. et al. An 8-ferroptosis-related genes signature from Bronchoalveolar Lavage Fluid for prognosis in patients with idiopathic pulmonary fibrosis. BMC Pulm. Med. 22(1), 15 (2022).
Cameli, P. et al. Oxidant/antioxidant disequilibrium in idiopathic pulmonary fibrosis pathogenesis. Inflammation 43(1), 1–7 (2020).
Liu, R. M. et al. Transforming growth factor beta suppresses glutamate-cysteine ligase gene expression and induces oxidative stress in a lung fibrosis model. Free Radic. Biol. Med. 53(3), 554–563 (2012).
Rabbani, Z. N. et al. Overexpression of extracellular superoxide dismutase reduces acute radiation induced lung toxicity. BMC Cancer 5, 59 (2005).
Murthy, S. et al. Modulation of reactive oxygen species by Rac1 or catalase prevents asbestos-induced pulmonary fibrosis. Am. J. Physiol. Lung Cell Mol. Physiol. 297(5), L846-855 (2009).
Suga, M. et al. Clinical significance of MCP-1 levels in BALF and serum in patients with interstitial lung diseases. Eur. Respir. J. 14(2), 376–382 (1999).
Osterholzer, J. J. et al. Implicating exudate macrophages and Ly-6C(high) monocytes in CCR2-dependent lung fibrosis following gene-targeted alveolar injury. J. Immunol. 190(7), 3447–3457 (2013).
Nie, Y. et al. NFATc3 promotes pulmonary inflammation and fibrosis by regulating production of CCL2 and CXCL2 in macrophage. Aging Dis. https://doi.org/10.14336/AD.2022.1202 (2023).
Moore, B. B. et al. CCR2-mediated recruitment of fibrocytes to the alveolar space after fibrotic injury. Am. J. Pathol. 166(3), 675–684 (2005).
Puukila, S. et al. Monocyte chemotactic protein (MCP)-1 (CCL2) and its receptor (CCR2) are elevated in chronic heart failure facilitating lung monocyte infiltration and differentiation which may contribute to lung fibrosis. Cytokine 161, 156060 (2023).
de Groot, L. E. S. et al. Oxidative stress and macrophages: Driving forces behind exacerbations of asthma and chronic obstructive pulmonary disease?. Am. J. Physiol. Lung Cell Mol. Physiol. 316(2), L369–L384 (2019).
Forman, H. J. & Torres, M. Reactive oxygen species and cell signaling: Respiratory burst in macrophage signaling. Am. J. Respir. Crit. Care Med. 166(12 Pt 2), S4-8 (2002).
Cheng, P., Li, S. & Chen, H. Macrophages in lung injury, repair, and fibrosis. Cells 10(2), 436 (2021).
Wynn, T. A. & Vannella, K. M. Macrophages in tissue repair, regeneration, and fibrosis. Immunity 44(3), 450–462 (2016).
Yao, Y. et al. Chop deficiency protects mice against bleomycin-induced pulmonary fibrosis by attenuating M2 macrophage production. Mol. Ther. 24(5), 915–925 (2016).
Sun, L. et al. New concepts of IL-10-induced lung fibrosis: Fibrocyte recruitment and M2 activation in a CCL2/CCR2 axis. Am. J. Physiol. Lung Cell Mol. Physiol. 300(3), L341-353 (2011).
Kral, J. B. et al. Sustained PI3K Activation exacerbates BLM-induced Lung Fibrosis via activation of pro-inflammatory and pro-fibrotic pathways. Sci. Rep. 6, 23034 (2016).
Tao, B. et al. Myeloid-specific disruption of tyrosine phosphatase Shp2 promotes alternative activation of macrophages and predisposes mice to pulmonary fibrosis. J. Immunol. 193(6), 2801–2811 (2014).
Redente, E. F. et al. Tumor necrosis factor-alpha accelerates the resolution of established pulmonary fibrosis in mice by targeting profibrotic lung macrophages. Am. J. Respir. Cell Mol. Biol. 50(4), 825–837 (2014).
Li, D. et al. IL-33 promotes ST2-dependent lung fibrosis by the induction of alternatively activated macrophages and innate lymphoid cells in mice. J. Allergy Clin. Immunol. 134(6), 1422–1432 (2014).
Canton, M. et al. Reactive oxygen species in macrophages: sources and targets. Front. Immunol. 12, 734229 (2021).
Perez, S. & Rius-Perez, S. Macrophage polarization and reprogramming in acute inflammation: A redox perspective. Antioxidants 11(7), 1394 (2022).
Herb, M. & Schramm, M. Functions of ROS in macrophages and antimicrobial immunity. Antioxidants (Basel) 10(2), 313 (2021).
Olson, A. L., Swigris, J. J., Raghu, G. & Brown, K. K. Seasonal variation: mortality from pulmonary fibrosis is greatest in the winter. Chest 136(1), 16–22 (2009).
Ramirez, A. M. et al. Vitamin D inhibition of pro-fibrotic effects of transforming growth factor beta1 in lung fibroblasts and epithelial cells. J. Steroid. Biochem. Mol. Biol. 118(3), 142–150 (2010).
Khan, R. & Sheppard, R. Fibrosis in heart disease: Understanding the role of transforming growth factor-beta in cardiomyopathy, valvular disease and arrhythmia. Immunology 118(1), 10–24 (2006).
Wang, S., Zhao, X., Yang, S., Chen, B. & Shi, J. Knockdown of NLRC5 inhibits renal fibroblast activation via modulating TGF-beta1/Smad signaling pathway. Eur. J. Pharmacol. 829, 38–43 (2018).
Desai, O., Winkler, J., Minasyan, M. & Herzog, E. L. The role of immune and inflammatory cells in idiopathic pulmonary fibrosis. Front. Med. (Lausanne) 5, 43 (2018).
Keane, M. P. et al. Neutralization of the CXC chemokine, macrophage inflammatory protein-2, attenuates bleomycin-induced pulmonary fibrosis. J. Immunol. 162(9), 5511–5518 (1999).
Ma, Z. et al. Role of CXCL16 in BLM-induced epithelial-mesenchymal transition in human A549 cells. Respir. Res. 22(1), 42 (2021).
Ma, L. et al. Tumor cell biodiversity drives microenvironmental reprogramming in liver cancer. Cancer Cell 36(4), 418–430 (2019).
Tibshirani, R. The lasso method for variable selection in the Cox model. Stat. Med. 16(4), 385–395 (1997).
Simon, N., Friedman, J., Hastie, T. & Tibshirani, R. Regularization paths for Cox’s proportional hazards model via coordinate descent. J. Stat. Softw. 39(5), 1–13 (2011).
Charoentong, P. et al. Pan-cancer immunogenomic analyses reveal genotype-immunophenotype relationships and predictors of response to checkpoint blockade. Cell Rep. 18(1), 248–262 (2017).
Chen, Y. et al. A novel immune-related gene signature to identify the tumor microenvironment and prognose disease among patients with oral squamous cell carcinoma patients using ssGSEA: A bioinformatics and biological validation study. Front. Immunol. 13, 922195 (2022).
Xiang, J. et al. Neotuberostemonine attenuates bleomycin-induced pulmonary fibrosis by suppressing the recruitment and activation of macrophages. Int. Immunopharmacol. 36, 158–164 (2016).
Hubner, R. H. et al. Standardized quantification of pulmonary fibrosis in histological samples. Biotechniques 44(4), 507–511 (2008).
Acknowledgements
We are highly thankful to our colleagues, who are not listed as an author of this manuscript, for their support in completing this study. We also acknowledge the role of institutes and departments involved in this study.
Funding
This study was supported by the Henan Provincial Science and Technology Project (grant number SBGJ202102185), and the Henan Provincial Medical Science and Technology Research Program Joint Construction Project (grant number LHGJ20210482).
Author information
Authors and Affiliations
Contributions
The study was conceived and designed by Wenfei Zhao and Guojun Zhang. Statistical analyses and Corresponding experiments were performed by Bing Bai. Software package was prepared by Hongyun Li. Manuscript was written and revised by Yonghai Feng, Jun Sun and Yang Fang. Pengyuan Zheng revised the final draft. Guojun Zhang concepted study, oversaw overall work, reviewed and revised the final draft. All authors contributed to the article and approved the submitted version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent to participate and ethics statement
All the animal experiments in this work were approved by the Ethics Committee of the Fifth Affiliated Hospital of Zhengzhou University (KY-D-2024025). All methods were performed following the relevant guidelines and regulations. The study is reported in accordance with ARRIVE guidelines.
Informed consent
Informed consent was obtained from all subjects involved in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhao, W., Bai, B., Li, H. et al. The role of oxidative stress-related genes in idiopathic pulmonary fibrosis. Sci Rep 15, 5954 (2025). https://doi.org/10.1038/s41598-025-89770-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89770-y
