
Abstract
There is conflicting information about the association between egg intake and metabolic health status and no previous information on this association was found in Middle Eastern populations. This research aimed to investigate the relationship between egg consumption and metabolic health status in Iranian adults, focusing on the potential involvement of brain-derived neurotrophic factor (BDNF) and adropin. This cross-sectional study was done on a sample of 527 individuals (45.7% female) aged between 20 and 65 years. Participants were selected using a multistage cluster random-sampling method. Dietary intakes of participants were evaluated using a validated food frequency questionnaire. Blood samples were collected while the individuals were fasting to assess biochemical markers. Metabolic health status of individuals was assessed based on the criteria established by Wildman. Collecting data on covariates was done using pre-tested procedures. Multivariable-adjusted model revealed a statistically significant association between egg consumption and a decreased odds of metabolically unhealthy (MU) status (ORT3 vs. T1 = 0.47; 95%CI 0.24–0.92). Also, each tertile increase in egg consumption was significantly associated with decreased odds of MU status (OR = 0.68; 95%CI 0.49–0.96). This association was especially significant among males rather than females. Elevated high-sensitive C-reactive protein (hs-CRP) levels were substantially reduced among individuals with the highest consumption of egg compared to the lowest intake. Additionally, there was a slight inverse association between egg consumption and high blood pressure. There were no relationships between egg intake and having low BDNF, and adropin levels. Increased consumption of egg was associated with a decreased chance of being metabolically unhealthy in Iranian adults, especially in male participants.
Similar content being viewed by others

Introduction
These days, there is a lot of worry about the prevalence of obesity and overweight among adults1. Metabolic disorders including hypertension, hyperglycemia, and hypercholesterolemia are responsible for the adverse effects of obesity2. However, these metabolic problems might not be present in every individual with obesity or overweight. People who are overweight or obese may or may not have metabolic health issues3,4. It has been shown that 7.5% of Iranian subjects are metabolically healthy obese (MHO)5; on the other hand, 17.2% of them are metabolically unhealthy normal weight (MUNW)6. Diseases associated with metabolic abnormalities could be less common in metabolically healthy (MH) people than in metabolically unhealthy (MU) people7.
Recent data has emphasized the metabolic importance of hormones such as adropin and brain-derived neurotrophic factor (BDNF). According to prior investigations, these hormones are involved in maintaining energy balance and regulating the metabolism of lipid and glucose8,9. Reduced BDNF levels and blood levels of adropin have been seen in subjects with metabolic disorders, including diabetes, obesity, and cardiovascular diseases (CVDs)10,11,12. Reports suggested that variables including food consumption and physical activity may influence adropin and BDNF levels13,14,15,16,17. BDNF and adropin are 2 endogenous proteins that might be affected by dietary fat or protein intake. Previous evidence suggested that total dietary fat might enhance adropin levels18. Also, extracted peptides from egg could increase the expression of BDNF in mice19; egg yolk in male rat could increase expression of BDNF receptors in brain, but did not change circulating BDNF level20. Therefore, whole eggs as a source of protein, fat, and several nutrients might increase BDNF and adropin levels. Adropin and BDNF are hypothesized to have significant impacts on metabolic health status. Thus, changing their serum levels is likely a behavioral treatment for enhancing metabolic health status.
Lifestyle modifications have been shown in earlier research to be advantageous for improving metabolic problems. In recent years, several clinical and epidemiological findings have shown the significant impact of nutrition, along with other lifestyle factors, on metabolic health21. A prior cross-sectional study found, women who were obese or overweight and metabolically healthy had more healthy intakes in general, with reduced saturated fat intake, and increased fiber consumption22. The effects of increasing protein intake on metabolic health were longitudinally studied among 6504 people from Iran; results revealed that risk of metabolic syndrome (MetS) was lower in those who consumed protein more often23. Eggs have bioactive components with antibacterial, immunomodulatory, antioxidant, anticancer, and antihypertensive activities24. Consumption of eggs may reduce inflammation and increase high-density lipoprotein cholesterol (HDL-c) levels, which may protect the body against MetS25. Additionally, data from an investigation on 23,993 Korean people suggested that eating eggs 4–6 times per week and 1 time per day (compared to eating fewer than 1 egg/month) might be useful in lowering the risk of MetS26. Most previous research on the relationship among egg intake and metabolic health in men and women has been focused on American and European populations and few studies were undertaken on Iranian adults23,26,27. Also, in most previous investigations, MetS was the outcome of interest, and metabolically healthy vs. unhealthy status was less investigated. So, this study was designed to investigate egg consumption in relation to MH and MU, BDNF, and adropin levels among Iranian men and women.
Methods
Study design and participants
In the year of 2021, a cross-sectional investigation was carried out on a representative sample of people in a big city in the middle of Iran. Detailed explanations of the study design, data collection technique, sampling, and population were provided elsewhere28. In brief, this research used a stratified multistage random cluster sampling approach to cover all people aged 20–65 years employing as school supervisors, teachers, workers, assistants, or crews at 20 different schools across 6 distinct educational districts of the city. Based on prior studies29, about 49.4% of Iranian people was likely to have metabolic disorders. To ensure statistical accuracy, this research needed a minimum of 474 participants, given a type 1 error rate of 0.05, a confidence interval of 0.95, a precision (d) of 4.5%, and a power of 80%. Due to the possibility of a low response rate during the COVID-19 pandemic when the data were gathered, 600 persons were requested to participate in the study. However, individuals possessing the following features were considered ineligible to participate in the study: (1) being pregnant or lactating; (2) having a history of cardiovascular disease, cancer, type 1 diabetes, or stroke; (3) adhering to a dietary plan, whether for weight loss or gain. In total, 543 individuals agreed to participate in our study, resulting in a response rate of 90.5%. Furthermore, we excluded anyone with the following conditions: (1) were under- and over-reporters of energy intake (< 800 or > 4200 kcal/day)30 (n = 3); (2) did not complete food frequency questionnaire (FFQ) (n = 4); and (3) did not have biochemical or blood pressure evaluation (n = 9). Consequently, a total of 527 participants participated in the current analysis.
Ethical approval and consent to participate
The study was performed according to declaration of Helsinki and STROBE checklist and all participants filled out informed consent forms after carefully reading and receiving a detailed explanation. The research protocol received ethical assessment and approval from the Isfahan University of Medical Sciences Ethics Committee (no.2403156).
Egg intake assessment
In order to assess dietary consumption of egg, we utilized a semi-quantitative food frequency questionnaire (FFQ) with 168 items31. A prior validation study with 132 middle-aged Iranian participants found reasonable relationships between food intakes determined by the FFQ and those obtained from multiple 24-h dietary recalls31. A trained dietitian instructed the people to describe their meals daily, weekly, or monthly. Utilizing a conventional portion size, the quantity of eggs and other meals consumed was assessed over the past year. Then, using household measurements32, the portion amounts were converted to grams/day. In the end, nutritional intakes were calculated by inputting the grams of egg and all other items consumed into the Nutritionist IV software (Version7; N-squared computing, OR, USA). Notably, the applied software had some modifications for specific Iranian meals.
Anthropometric and cardiometabolic variables assessment
Two dietitians assessed the anthropometric parameters of the subjects. The body composition analyzer, namely the Tanita MC-780MA from Tokyo, Japan, was used to assess weight with a precision of 0.1 kg. This measurement was taken without shoes and with limited clothes. The height of subjects was assessed with a tape measure, with a precision of 0.1 cm. The waist circumference (WC) of participants was assessed by measuring the distance between the lower rib margin and iliac crest, using a non-stretchable tape measure, to the closest 0.1 cm. This measurement was taken at the end of a normal respiratory cycle33. Weight divided by square of height was used to measure body mass index (BMI) (kg/m2). A digital sphygmomanometer (OMRON, M3, HEM 7154-E) was used to monitor systolic and diastolic blood pressure (SBP and DBP), when the subjects sat up and after a 5-min rest. For each individual, blood pressure (BP) was taken twice, with a 5-min break in between, and the mean of the two measurements was used for statistical analysis. For each participant, a 12-h fasting venous blood sample was taken in the morning, in order to assess biochemical markers. On the same day, serum concentrations of fasting blood glucose (FBG), HDL cholesterol, and triglycerides (TG) were measured via an auto-analyzer (BioSystems). For the purpose of measuring additional biochemical variables, the leftover serum was stored at − 80°℃. Blood concentrations of insulin were measured using a commercial kit from Monobined Inc. The high-sensitivity C-reactive protein (hs-CRP) levels were assessed by a turbidimetry kit, specifically the latex-enhanced turbidimetric technique called Delta. DP. The Homeostasis Model Assessment Insulin Resistance (HOMA-IR) index was calculated using the formula: HOMA-IR = [(fasting insulin (mU/L) × FBG (mg/dL)]/40534. An enzyme-linked immunosorbent assay (ELISA) kit from Zellbio was used to test the amounts of BDNF and adropin in serum. Based on a previous investigation35, the first decile of serum BDNF concentrations in the current population (0.074–0.466 ng/mL or < 0.47 ng/mL) was considered as having low serum BDNF level.
Defining metabolic health status
Metabolic health status of individuals was evaluated using the criteria proposed by Wildman et al.36, which included the following risk factors: (1) hypertension (BP ≥ 130/85 mmHg) or using medications to treat hypertension; (2) hyperglycemia (≥ 100 mg/dL) or using medications that reduce blood sugar; (3) hypertriglyceridemia (≥ 150 mg/dL) or using medications that reduce lipid profile; (4) hypo-HDL-cholesterolemia (< 50 mg/dL for females or < 40 mg/dL for males); (5) chronic inflammation (hs-CRP levels > 90th percentile, or > 6.14 mg/L in this study); (6) insulin resistance (HOMA-IR > 90th percentile or > 3.99 in this study). According to this approach, participants were classified into two categories: MU vs. MH. Individuals who exhibited two or more of the aforementioned risk factors were classified as having a MU profile. Otherwise, they were categorized as individuals exhibiting an MH phenotype.
Assessment of other variables
A self-reported questionnaire was applied to collect basic demographic data including sex, age, smoking status, marital status, education level, and using anti-depression drugs. Furthermore, a validated questionnaire was used to assess the socioeconomic status (SES) of individuals37. The questionnaire evaluated many factors like the size of the family, ownership of a house, quantity, and model of cars, number of laptops/computers, and travel activities during the previous year. The validated International Physical Activity Questionnaire-short form (IPAQ-SF)38 was used to evaluate habitual physical activity. This survey consists of 7 questions on the regularity and duration of physical activity performed in one last week. Anxiety and depression were surveyed by a validated Persian version of Hospital Anxiety and Depression Scale (HADS)39 with 7 items for anxiety and 7 items for depression. A total score for anxiety and depression was calculated, ranged from 0 to 21. Participants with a score of 7 or less were classified into normal status and individuals with a score of 8 or more were classified as anxious or depressed. Psychological distress levels were evaluated by a 12-item validated Persian version of General Health Questionnaire (GHQ)40. The maximum total score could be 12, based on the bimodal method (0–0–1–1). Individuals were grouped in 2 categories: low psychological distress (0–3 points) and high psychological distress (≥ 4 points).
Statistical analysis
All following statistical analyses were conducted via SPSS software version 20 (IBM, Chicago, IL). The residual method was used to calculate the energy-adjusted intake of eggs. Then, tertiles of energy-adjusted eggs consumption were used to categorize the subjects. Mean ± standard deviation (SD)/ standard error (SE) for continuous variables and percentage for categorical variables were used for reporting. First, characteristics of individuals across tertiles of energy-adjusted egg consumption were compared using one-way analysis of variance (ANOVA) for continuous and chi-square test and categorical variables. Then, dietary intakes of people were evaluated, through the use of analysis of covariance (ANCOVA), and adjusting for age, energy intake, and sex. In order to identify any possible associations between egg intake and MU status and its components, binary logistic regression was applied. Odds ratios (ORs) and 95% confidence intervals (CIs) for MU status were calculated, in both the crude and adjusted models. In the first model, the potential influences of age, energy intake, and sex were considered. In the second model, further adjustments were made for socio-demographic characteristics including physical activity, socioeconomic status, marital status, education, and smoking status. In the third model, the effects of fruits, nuts, vegetables, soy and legumes, and whole grains intake were adjusted, as suggested by earlier research41. In the last model, BMI was also included in the adjustments. ORs were computed using the first tertile of egg consumption as the reference level. In order to assess the trend of ORs across egg intake categories, tertiles of energy-adjusted egg consumption were treated as an ordinal variable in logistic regression models. Additionally, stratified analyses were carried out based on sex (men vs. women) and BMI categories (normal-weight vs. overweight/obese). The effects of age, sex, physical activity, high blood pressure, high fasting blood glucose, high triglyceride, having anxiety, depression, high psychological distress and using anti-depression drugs were taken into account when calculating the multivariable-adjusted ORs for low BDNF levels (< 0.47 ng/mL) in tertiles of energy-adjusted egg consumption. Furthermore, linear regression analysis was used to evaluate adropin levels in tertiles of egg consumption, while age, sex, energy intake, physical activity, and BMI were considered as confounders. We considered P-values < 0.05 to be statistically significant.
Results
The current study was carried out on an overall sample of 527 participants, with an average age of 42.66 ± 11.19 years and a BMI of 26.91 ± 4.43 kg/m2. Among these individuals, 54.3% were male. Cardio-metabolic factors and general characteristics of participants across tertiles of egg intake are listed in Table 1. Compared to those in the lowest tertile of egg consumption, those in the highest tertile had lower levels of education (P < 0.05). No statistically significant variation was seen among other cardio-metabolic and general parameters among tertiles of egg consumption, including adropin, BDNF, BP, lipid profile, fasting blood glucose, and hs-CRP (P > 0.05).
Table 2 displays age, energy intake, and sex-adjusted dietary intakes of food groups and macro/micro nutrients of individuals across different tertiles of egg consumption. Compared to the first tertile, those in the third tertile of egg consumption exhibited higher energy intake, fat consumption, and vegetable consumption, as well as increased intake of vitamin E, vitamin B2, and vitamin B12. Additionally, they consumed less carbohydrates and vitamin B1 (P < 0.05). There was no statistically significant variation in case of other dietary intakes (P > 0.05).
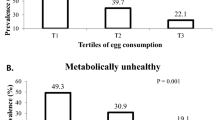
Among 527 study participants in the current cross-sectional investigation, 303 participants (57%) were metabolically healthy individuals, and 224 others (43%) had metabolically unhealthy status. Table 3 shows ORs and 95% CIs for MU status among tertiles of egg intake. In the crude model, no significant association was found between egg consumption and MU phenotype (OR = 0.90; 95% CI 0.59–1.38). Nevertheless, after accounting for all covariates, including BMI, individuals who consumed the highest number of eggs had a 53% reduced likelihood of MU compared to those who consumed the lowest amount (OR = 0.47; 95% CI 0.24–0.92). Also, each tertile increase in egg consumption was significantly associated with a decreased odds of MU status, in the maximally-adjusted model (OR = 0.68; 95% CI 0.49–0.96). According to the stratified analysis by sex, no significant relationship was seen between odds of MU and egg consumption among men intake, in crude model (OR = 0.82; 95% CI 0.47–1.43). But after adjusting for confounders, a significant relationship was found between egg consumption and the likelihood of MU in men. Such that, the chance of developing MU was 60% lower in males who ate the most eggs than in those who consumed the least (OR = 0.40; 95% CI 0.16–0.99). Additionally, a significant 38% reduction in the likelihood of MU in men was seen with each tertile increase in egg consumption (OR = 0.62; 95% CI 0.39–0.99). Neither in crude (OR = 0.97, 95% CI 0.50–1.87), nor in fully-adjusted models (OR = 0.57, 95% CI 0.19–1.74), a significant association was seen between the highest vs. lowest tertile of egg intake and MU phenotype in females. However, those women in the second tertile compared to the first tertile of egg consumption had a significant lower odds of MU in crude (OR = 0.42, 95% CI 0.22–0.83) and fully-adjusted model (OR = 0.32, 95% CI 0.11–0.98). Stratified analysis by BMI levels showed no significant relation between egg intake and MU phenotype. However, a marginally inverse association was seen between odds of MU and each tertile increase in egg consumption, in the fully adjusted model among normal-weight participants.
Table 4 displays multivariable-adjusted ORs and 95% CIs for components of MU across tertiles of egg intake. A substantial decrease in high hs-CRP odds was seen by increasing egg intake. After adjustment for all covariates, subjects in the third tertile of the egg intake had a 74% decreased odds of having high hs-CRP levels than individuals in the first tertile (OR = 0.26, 95% CI: 0.90–0.74). Moreover, the increased intake of eggs was marginally associated with a decreased likelihood of developing high blood pressure (OR = 0.52, 95% CI 0.26–1.05; P = 0.07).
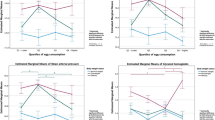
Serum BDNF levels averaged 1.25 ng/mL and adropin levels averaged 56.59 pg/mL among the individuals. Figure 1 displays multivariate-adjusted ORs for low BDNF levels across tertiles of egg consumption. Neither in crude (ORT3 vs. T1 0.87; 95% CI 0.42–1.79), nor in fully-adjusted models (OR = 0.87, 95% CI 0.40–1.88), we found a significant association between egg intake and low BDNF levels.

Multivariable-adjusted odds ratio and 95% confidence intervals for low BDNF levels across tertiles of egg intake. Model 1: Adjusted for age and sex; Model 2: More adjustments for physical activity, high blood pressure, high triglyceride and high fasting blood glucose. Model 3: more adjustments for using anti-depression drugs, having anxiety, depression, and high psychological distress. Ptrend was obtained by the use of tertiles of egg intake as an ordinal variable in the model.
As displayed in Fig. 2, our linear regression analysis revealed no significant association between each tertile increment in egg intake and serum level of adropin, both in crude (β = 3.23, 95% CI − 1.09, 7.56; Pvalue = 0.14) and multi-adjusted model (β = 3.36, 95% CI − 1.01, 7.72; Pvalue = 0.13).

Linear association between tertiles of egg intake with adropin levels. All values are regression coefficients (β) and 95% confidence intervals. Tertiles of egg intake were considered as an ordinal variable in linear regression analysis. Model 1: Adjusted for age, sex, and energy intake; Model 2: More adjustments for physical activity and BMI.
Discussion
The current study indicated that greater consumption of eggs was associated with a reduced likelihood of developing MU in Iranian adults, in a dose–response manner. In males, this association was stronger than in females. In addition, an inverse relation was observed between egg intake and elevated hs-CRP levels. Additionally, there was a slight inverse association between egg consumption and high blood pressure. But there was no substantial association between egg consumption and low BDNF or adropin levels.
The incidence of obesity is rising in most industrialized countries42. Excess weight could be linked to a significantly increased chance of coronary heart disease, which would be a well-documented negative health outcome43. Conditions such as hypertension, high cholesterol, and diabetes played a crucial role in mediating this link44. Consequently, evaluating dietary intake and improving usual dietary intake could result in mitigating the risk of metabolic disorders. In addition, current findings suggested that in adult population, more egg intake could improve metabolic health status; further studies are required to illuminate whether more egg intake as an intervention in various populations could reduce MU status and increase BDNF and adropin levels.
Several prior researches have examined the relationship between egg intake and MetS; however, the findings were inconsistent. Similar to our findings, a meta-analysis of epidemiologic studies including 331,667 people found that increased egg intake was associated with a reduced likelihood of developing MetS41. Consistent with our results, Wang et al. documented that egg intake in Chinese adults was inversely associated with prevalence of MetS; in contrast to our findings, they found a significant association in female subgroup, but not in male subgroup45. In South Korea, risk of MetS in 1663 middle-aged men and women was inversely associated with consumption of more than three eggs per week, in both cross-sectional and prospective analyses46. Some randomized controlled trials have also proved favorable effects of egg intake on metabolic risk factors. For instance, in an intervention on 955 healthy rural students in China, adding 50 g of eggs along with 200 g of milk to the regular diet over a two-year period as compared to the control diet showed benefits for growth in boys, but not in girls; while physical fitness was improved in both girls and boys47. Possible explanations for a few contradictory results include differences in study design, the methods used to measure nutritional intakes, statistical analysis, and the extent to which confounding variables were controlled. Furthermore, the aforementioned studies were carried out in various countries with diverse cultures; therefore, dietary habits and intakes of populations might impact the findings.
We discovered that highest vs. lowest egg consumption was associated with a lower likelihood of MU in men, but not in women; however, among women, moderate consumption of egg was related to lower probability of MU. This finding suggest that a u-shaped relationship might exist between egg intake and MU in women; this observed relation might be due to a stronger confounding effect of the confounders in women vs. men. Similarly, another research found that there was a negative association between egg intake and risk of developing type 2 diabetes in men, but not in women48. This suggested that there might be variations between genders in how food affects the risk of disease48. One probable reason could be the sex steroid hormones that might contribute to gender disparities. For instance, male hormones such as testosterone and dihydrotestosterone have been demonstrated to be inversely associated with risk of diabetes incidents in middle-aged or older males in prospective cohort studies49,50. By modulating insulin resistance independently of adiposity51 or by reducing fat mass52,53, high levels of androgens might mitigate the risk of insulin resistance and diabetes. In addition, some previous studies suggested that plasma testosterone levels might be inversely related to the severity of MetS characteristics54,55.
BDNF and adropin are involved in regulating several metabolisms and associated to metabolic dysfunction and CVDs8,9,10,11,12. Unfortunately, the relationships between nutritional intakes and BDNF or adropin were rarely evaluated14,17; and there was little evidence about the association of protein intake especially eggs with circulating BDNF or adropin. In previous experimental studies, ovomemolins, peptides derived from egg whites, could increase hippocampal BDNF mRNA expression in mice19. Another study indicated that egg yolk intake (compared to white yolk) in male rats might improve expression of BDNF receptors (tyrosine kinase B) in brain, while did not affect circulating BDNF20. To the best of our knowledge, in previous studies, the impacts of egg or egg contents on adropin were not examined.
Eggs are a significant contributor of dietary cholesterol, as well as a rich source of several nutrients including high-quality proteins, vitamins, minerals, and both saturated and unsaturated fatty acids56. The favorable association between egg intake and metabolic health status might be attributable to other constituents of egg, other than cholesterol, which might have beneficial effects on suppressing the progression of a metabolic unhealthy status. Shirouchi and Matsuoka proposed that including lactic-fermented egg white and egg white protein in diets could potentially prevent or mitigate the progression of MetS57. Furthermore, as phospholipids have an impact on blood cholesterol levels (mostly by increasing HDL-c), it is probable that eggs have a role in elevating plasma HDL-c levels58. One important factor that impacts lipoprotein metabolism (low-grade systemic inflammation and insulin resistance) might be the degree of metabolic imbalance, which is likely correlated with the severity of MetS59. Hence, this might partly explain the inverse relationship between egg intake and the likelihood of metabolic unhealthy in our study.
There are some limitations that need to be taken into account. Due to the cross-sectional design of the current study, it did not provide evidence for a causal association between egg consumption and metabolic unhealthy status. In addition, even though a validated FFQ was used to evaluate dietary intakes, there was still a possibility of recall bias and inaccurate categorization in self-reported dietary data. Furthermore, it was essential to acknowledge the impact of COVID-19 pandemic on food consumption and metabolic health condition. Furthermore, our investigation revealed that there was no significant association between egg consumption and low levels of BDNF or adropin. The possible explanation for this discovery may be attributed to the fact that the sample size was not set according to this hypothesis, owing to budgetary limitations. The notable features of this study consist of being one of the pioneering investigations that explores the relationship between egg intake and the metabolic health status of Iranian people, to the best of our knowledge. Furthermore, we carefully accounted for any confounding factors in our study, indicating that the obtained results were unaffected by these variables. In addition, the Wildman et al. technique was used to define metabolic health status, which encompassed not only HOMA-IR and standard cardiometabolic risk markers, but also an inflammatory index called hs-CRP. Another benefit of this research was the evaluation of adropin and BDNF blood levels, which were rarely examined in epidemiological nutrition investigations.
In conclusion, higher consumption of egg was associated with a decreased chance of MU in Iranian adults, especially in male participants. Increasing egg consumption significantly reduced high hs-CRP. Egg consumption was also related to a slight reduction in high blood pressure odds. No relationship was seen between egg intake and low levels of BDNF and adropin. Additional prospective population-based studies are necessary to validate these results in different subgroups of individuals and other populations. Also, further interventional studies are required to evaluate the effect of more egg intake on components of MU, BDNF, and adropin levels.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- ANCOVA:
-
Analysis of covariance
- ANOVA:
-
Analysis of variance
- BDNF:
-
Brain-derived neurotrophic factor
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- CI:
-
Confidence interval
- CVDs:
-
Cardiovascular diseases
- DBP:
-
Diastolic blood pressure
- ELISA:
-
Enzyme-linked immunosorbent assay
- FBG:
-
Fasting blood glucose
- FFQ:
-
Food frequency questionnaire
- HDL-c:
-
High-density lipoprotein cholesterol
- HEPA:
-
Health-enhancing physical activity
- HOMA-IR:
-
Homeostasis model assessment insulin resistance
- hs-CRP:
-
High sensitive C-reactive protein
- IPAQ-SF:
-
International physical activity questionnaire-short form
- MetS:
-
Metabolic syndrome
- MH:
-
Metabolically healthy
- MHO:
-
Metabolically healthy obese
- MU:
-
Metabolically unhealthy
- OR:
-
Odds ratio
- SBP:
-
Systolic blood pressure
- SD:
-
Standard deviation
- SE:
-
Standard error
- SES:
-
Socioeconomic status
- T:
-
Tertile
- TG:
-
Triglycerides
- WC:
-
Waist circumference
References
Abarca-Gómez, L. et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 390, 2627–2642 (2017).
Iacobini, C., Pugliese, G., Fantauzzi, C. B., Federici, M. & Menini, S. Metabolically healthy versus metabolically unhealthy obesity. Metabolism 92, 51–60 (2019).
Primeau, V. et al. Characterizing the profile of obese patients who are metabolically healthy. Int. J. Obes. 35, 971–981 (2011).
Rey-López, J. P., De Rezende, L., Pastor-Valero, M. & Tess, B. H. The prevalence of metabolically healthy obesity: a systematic review and critical evaluation of the definitions used. Obes. Rev. 15, 781–790 (2014).
Tabatabaei-Malazy, O. et al. Association between being metabolically healthy/unhealthy and metabolic syndrome in Iranian adults. Plos ONE 17, e0262246 (2022).
Hajian-Tilaki, K. & Heidari, B. Metabolically healthy obese and unhealthy normal weight in Iranian adult population: Prevalence and the associated factors. Diabetes Metab. Syndr. Clin. Res. Rev. 12, 129–134 (2018).
Blüher, M. Metabolically healthy obesity. Endocr. Rev. 41, bnaa004 (2020).
Ali, I. I., D’Souza, C., Singh, J. & Adeghate, E. Adropin’s role in energy homeostasis and metabolic disorders. Int. J. Mol. Sci. 23, 8318 (2022).
Rothman, S. M., Griffioen, K. J., Wan, R. & Mattson, M. P. Brain-derived neurotrophic factor as a regulator of systemic and brain energy metabolism and cardiovascular health. Ann. N. Y. Acad. Sci. 1264, 49–63 (2012).
Rozanska, O., Uruska, A. & Zozulinska-Ziolkiewicz, D. Brain-derived neurotrophic factor and diabetes. Int. J. Mol. Sci. 21, 841 (2020).
Wu, L. et al. Low serum adropin is associated with coronary atherosclerosis in type 2 diabetic and non-diabetic patients. Clin. Chem. Lab. Med. 52, 751–758 (2014).
Han, W. et al. Alterations of irisin, adropin, preptin and BDNF concentrations in coronary heart disease patients comorbid with depression. Ann. Transl. Med. 7, 298. https://doi.org/10.21037/atm.2019.05.77 (2019).
St-Onge, M. P. et al. Fasting plasma adropin concentrations correlate with fat consumption in human females. Obesity 22, 1056–1063 (2014).
Stevens, J. R. et al. Inverse association between carbohydrate consumption and plasma adropin concentrations in humans. Obesity 24, 1731–1740 (2016).
Fujie, S. et al. Aerobic exercise training-induced changes in serum adropin level are associated with reduced arterial stiffness in middle-aged and older adults. Am. J. Physiol. Heart Circ. Physiol. 309, H1642–H1647 (2015).
Walsh, J. J. & Tschakovsky, M. E. Exercise and circulating BDNF: Mechanisms of release and implications for the design of exercise interventions. Appl. Physiol. Nutr. Metab. 43, 1095–1104 (2018).
Gravesteijn, E., Mensink, R. P. & Plat, J. Effects of nutritional interventions on BDNF concentrations in humans: a systematic review. Nutr. Neurosci. 25, 1425–1436 (2022).
Butler, A. A. et al. Differential responses of plasma adropin concentrations to dietary glucose or fructose consumption in humans. Sci. Rep. 5, 14691. https://doi.org/10.1038/srep14691 (2015).
Nakajima, T. et al. Ovomemolins: Egg-derived peptides that improved cognitive decline after oral administration in mice. FASEB Bioadv. 6, 177–188. https://doi.org/10.1096/fba.2023-00149 (2024).
Chen, X. et al. Consuming egg yolk decreases body weight and increases serum HDL and brain expression of TrkB in male SD rats. J. Sci. Food Agric. 99, 3879–3885. https://doi.org/10.1002/jsfa.9610 (2019).
Castro-Barquero, S., Ruiz-León, A. M., Sierra-Pérez, M., Estruch, R. & Casas, R. Dietary strategies for metabolic syndrome: a comprehensive review. Nutrients 12, 2983 (2020).
Camhi, S. M., Crouter, S. E., Hayman, L. L., Must, A. & Lichtenstein, A. H. Lifestyle behaviors in metabolically healthy and unhealthy overweight and obese women: a preliminary study. PloS ONE 10, e0138548 (2015).
Hajihashemi, P. et al. The long-term association of different dietary protein sources with metabolic syndrome. Sci. Rep. 11, 19394 (2021).
Ballesteros, M. N. et al. One egg per day improves inflammation when compared to an oatmeal-based breakfast without increasing other cardiometabolic risk factors in diabetic patients. Nutrients 7, 3449–3463 (2015).
Balkan, F. Metabolik sendrom. Ankara Med. J. 13, 85–90 (2013).
Park, S.-J., Jung, J.-H., Choi, S.-W. & Lee, H.-J. Association between egg consumption and metabolic disease. Korean J. Food Sci. Anim. Resour. 38, 209 (2018).
Jurado-Fasoli, L., Castillo, M. J. & Amaro-Gahete, F. J. Dietary differences between metabolically healthy overweight-obese and metabolically unhealthy overweight-obese adults. Br. J. Nutr. 122, 1113–1119 (2019).
Poursalehi, D. et al. Diet in relation to metabolic, sleep and psychological health status (DiMetS): protocol for a cross-sectional study. BMJ Open 13, e076114 (2023).
Rahmanian, K., Shojaei, M. & Sotoodeh Jahromi, A. Prevalence and clinical characteristics of metabolically unhealthy obesity in an Iranian adult population. Diabetes Metab. Syndr. Obes. 12, 1387–1395. https://doi.org/10.2147/dmso.S197476 (2019).
Willett, W. Nutritional Epidemiology (Oxford University Press, 2012).
Mirmiran, P., Esfahani, F. H., Mehrabi, Y., Hedayati, M. & Azizi, F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 13, 654–662 (2010).
Ghafarpour, M., Houshiar-Rad, A., Kianfar, H. & Ghaffarpour, M. (Tehran: Keshavarzi Press, 1999).
Gibson, R. S. Principles of Nutritional Assessment (Oxford University Press, 2005).
Swaroop, J. J., Rajarajeswari, D. & Naidu, J. N. Association of TNF-α with insulin resistance in type 2 diabetes mellitus. Indian J. Med. Res. 135, 127–130. https://doi.org/10.4103/0971-5916.93435 (2012).
Sanchez-Villegas, A. et al. The effect of the Mediterranean diet on plasma brain-derived neurotrophic factor (BDNF) levels: the PREDIMED-NAVARRA randomized trial. Nutr. Neurosci. 14, 195–201. https://doi.org/10.1179/1476830511Y.0000000011 (2011).
Wildman, R. P. et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: prevalence and correlates of 2 phenotypes among the US population (NHANES 1999–2004). Arch. Intern. Med. 168, 1617–1624 (2008).
Garmaroudi, G. R. & Moradi, A. Socio-economic status in Iran: a study of measurement index. Payesh (Health Monitor) 9, 137–144 (2010).
Moghaddam, M. B. et al. The Iranian version of international physical activity questionnaire (IPAQ) in Iran: content and construct validity, factor structure, internal consistency and stability. World Appl. Sci. J 18, 1073–1080 (2012).
Montazeri, A., Vahdaninia, M., Ebrahimi, M. & Jarvandi, S. The hospital anxiety and depression scale (HADS): translation and validation study of the Iranian version. Health Qual Life Outcomes 1, 14. https://doi.org/10.1186/1477-7525-1-14 (2003).
Montazeri, A. et al. The 12-item general health questionnaire (GHQ-12): translation and validation study of the Iranian version. Health Qual Life Outcomes 1, 66. https://doi.org/10.1186/1477-7525-1-66 (2003).
Ding, J. Relationship between egg consumption and metabolic syndrome. A meta-analysis of observational studies. J. Nutr. Health Aging 26, 373–382 (2022).
Ogden, C. L., Flegal, K. M., Carroll, M. D. & Johnson, C. L. Prevalence and trends in overweight among US children and adolescents, 1999–2000. Jama 288, 1728–1732 (2002).
Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser 894, i-xii, 1-253 (2000).
Wilson, P. W., D’Agostino, R. B., Sullivan, L., Parise, H. & Kannel, W. B. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch. Intern. Med. 162, 1867–1872 (2002).
Wang, H. et al. Association between egg consumption and metabolic syndrome in Chinese population: a cross-sectional study. BMJ Open 11, e050317 (2021).
Woo, H. W., Choi, B. Y. & Kim, M. K. Cross-sectional and longitudinal associations between egg consumption and metabolic syndrome in adults≥ 40 years old: the Yangpyeong cohort of the Korean genome and epidemiology study (KoGES_Yangpyeong). PLoS ONE 11, e0147729 (2016).
Zhao, R. et al. Changes in fitness of rural primary school students from Southwest China after two-year’s nutrition intervention. Nutrients 13, 3544 (2021).
Lee, J. & Kim, J. Egg consumption is associated with a lower risk of type 2 diabetes in middle-aged and older men. Nutr. Res. Pract. 12, 396–405. https://doi.org/10.4162/nrp.2018.12.5.396 (2018).
Joyce, K. E. et al. Testosterone, dihydrotestosterone, sex hormone–binding globulin, and incident diabetes among older men: the cardiovascular health study. J. Clin. Endocrinol. Metab. 102, 33–39 (2017).
Stellato, R. K., Feldman, H. A., Hamdy, O., Horton, E. S. & McKinlay, J. B. Testosterone, sex hormone-binding globulin, and the development of type 2 diabetes in middle-aged men: prospective results from the Massachusetts male aging study. Diabetes Care 23, 490–494 (2000).
Selvin, E. et al. Androgens and diabetes in men: results from the Third National Health and Nutrition Examination Survey (NHANES III). Diabetes Care 30, 234–238 (2007).
Vandenput, L. et al. Androgens and glucuronidated androgen metabolites are associated with metabolic risk factors in men. J. Clin. Endocrinol. Metab. 92, 4130–4137 (2007).
Fan, W. et al. Androgen receptor null male mice develop late-onset obesity caused by decreased energy expenditure and lipolytic activity but show normal insulin sensitivity with high adiponectin secretion. Diabetes 54, 1000–1008 (2005).
Mohr, B. A., Bhasin, S., Link, C. L., O’Donnell, A. B. & McKinlay, J. B. The effect of changes in adiposity on testosterone levels in older men: longitudinal results from the Massachusetts male aging study. Eur. J. Endocrinol. 155, 443–452 (2006).
Rodriguez, A. et al. Aging, androgens, and the metabolic syndrome in a longitudinal study of aging. J. Clin. Endocrinol. Metab. 92, 3568–3572 (2007).
Rizzi, C. & Marangon, A. Quality of organic eggs of hybrid and Italian breed hens. Poult. Sci. 91, 2330–2340 (2012).
Shirouchi, B. & Matsuoka, R. Alleviation of metabolic syndrome with dietary egg white protein. J. Oleo Sci. 68, 517–524 (2019).
Mutungi, G. et al. Dietary cholesterol from eggs increases plasma HDL cholesterol in overweight men consuming a carbohydrate-restricted diet, 2. J. Nutr. 138, 272–276 (2008).
Cornier, M.-A. et al. The metabolic syndrome. Endocr. Rev. 29, 777–822 (2008).
Funding
The financial support for conception, design, data analysis and manuscript drafting comes from Nutrition and Food Security Research Center, Isfahan University of Medical Sciences, Isfahan, Iran (no.2403156).
Author information
Authors and Affiliations
Contributions
AG, SF Conceptualization, Methodology, Formal analysis, Funding acquisition, Writing-original draft. ZM: Investigation, Writing-original draft. F.S: Investigation. Z.H: Investigation and Data Curation. P.R: Investigation and Data curation. P.S: Conceptualization, Methodology, Supervision, Resource, Formal analysis, Funding acquisition, Writing-editing and reviewing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Grigorian, A., Farzam, S., Moradmand, Z. et al. Egg intake in relation to metabolic health status, serum brain derived neurotrophic factor, and adropin levels in Iranian adults. Sci Rep 15, 8274 (2025). https://doi.org/10.1038/s41598-025-92729-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-92729-8
