
Abstract
Psoriasis is a persistent inflammatory dermatological disorder characterized by dysregulated hyperproliferation of keratinocytes and pathological immune cell infiltration, impacting a significant population globally. Conventional systemic therapies, including oral and injectable formulations, are often limited by adverse off-target effects, which limit their utility in long-term clinical management. To address this challenge, we developed a soluble bilayered microneedle patch (Methotrexate and dexamethasone co-loaded bilayer microneedles, MTX@DXM-MNs), which consists of an outer layer of gelatine-polyvinyl alcohol hydrogel loaded with dexamethasone (DXM) and an inner layer of aminocrystallized hyaluronic acid methacrylate hydrogel loaded with methotrexate (MTX). The patch successfully traversed imiquimod (IMQ)-induced thickened epidermis in murine models to achieve intralesional drug delivery and effectively alleviate psoriasis-like skin inflammation. Versus tacrolimus ointment (positive control), MTX@DXM-MNs markedly alleviated the manifestations of stratum corneum thickening, erythema, and scaling in a mouse model and attenuated the levels of inflammatory mediators in skin tissues and peripheral blood as well as splenic indices. In conclusion, the MTX@DXM-MN bilayered microneedle patch provides a new strategy for the efficient and safe treatment of psoriasis through the temporal and spatial synergistic effects of an outer layer for the immediate release of a hormone and an inner layer for the slow release of an immunosuppressant. Thus, this patch has potential as a future clinical alternative for the treatment of psoriasis.
Similar content being viewed by others


Introduction
Psoriasis is a chronic immune-mediated inflammatory papulosquamous skin disease located mainly on the limbs and scalp1,2. Its pathological features are mainly characterized by abnormal proliferation and incomplete differentiation of epidermal keratinocytes, resulting in epidermal thickening, hyperkeratosis and hypertrophy of the stratum spinosum. Significant inflammatory cell infiltration is seen in the dermis, especially the aggregation of T cells, dendritic cells and neutrophils.This condition substantially increases psychosocial distress in patients and is closely linked to a range of comorbidities, such as psoriatic arthritis, metabolic syndrome, cardiovascular disease, and malignant neoplasms3. It affects approximately 2–3% of the global population4. Its pathogenesis is complex and involves genetic susceptibility, immune dysregulation (e.g., TNF-α5, IL-66, and IL-177-mediated inflammation), keratinocyte hyperproliferation, angiogenesis8, and external influences (e.g., infections from streptococcal bacteria, along with stress, smoking, being overweight, and consuming alcohol)9. Psoriasis is currently incurable, and treatment goals focus on early intervention to minimize damage, identifying and preventing comorbidities, implementing lifestyle interventions, and adopting individualized treatment strategies9.
Standard treatment of psoriasis is graded according to the severity of the disease: mild cases are mainly topical, including glucocorticoids, vitamin D3 derivatives and keratin modifiers; moderate to severe cases require combined phototherapy (e.g., narrow-spectrum UVB) or systemic medications, such as methotrexate, cyclosporine, and avitaminosis. Refractory or arthritic types can use biological agents such as TNF-α and IL-17/23 inhibitors. Treatment emphasizes regularity, safety, individualization, avoidance of hormone abuse, regular assessment of efficacy and side effects, and rotation or combination of regimens when necessary.
Among them, methotrexate (MTX), a classical immunomodulator, remains the cornerstone of long-term systemic therapy and has good efficacy and safety10. Dexamethasone (DXM) is a potent long-acting glucocorticoid with significant anti-inflammatory and immunosuppressive effects11. Both agents rapidly alleviate symptoms through the downregulation of key inflammatory mediators, including TNF-α, IL-6, and IL-17, leading to a reduction in erythaematous, scaling, and pruritic manifestations, along with the suppression of pathological keratinocyte proliferation and immune infiltration12,13. However, achieving effective drug delivery in the epidermis is still challenging. Although oral MTX inhibits keratinocyte overproliferation, the first-pass effect and insufficient skin accumulation lead to reduced bioavailability and systemic side effects12,14. The chronic relapsing nature of psoriasis requires repeated dosing over a long period, further increasing the cumulative dose and risk of side effects15. Although topical administration reduces systemic exposure, its efficiency is limited by the skin barrier effect, which significantly impedes penetration16,17, the physicochemical properties of the drug/carrier, and its interaction with the skin18. In conclusion, MTX has high water solubility, poor transdermal permeability, and large oral gastrointestinal side effects; DXM has moderate fat solubility, but significant first-pass effects, and long-term systemic use of the drug is prone to hormone-related adverse reactions; the transdermal route bypasses the first-pass metabolism, reduces systemic toxicity, and is suitable for the maintenance treatment of chronic psoriasis.Therefore, it is crucial to develop delivery strategies with high efficiency and few side effects.
Microneedles (MNs) are microscale needle arrays (height: 10–2000 μm; width: 10–50 μm) that painlessly bypass the stratum corneum, enabling targeted dermal delivery and overcoming the cutaneous barrier19. MNs are extensively employed in transdermal delivery platforms20, owing to their high efficiency, safety, painlessness, and minimal invasiveness, and they enhance drug skin retention and penetration through site-specific delivery to improve patient compliance21,22. A previous study reported that cannabidiol-loaded MN patches could treat psoriasis by inhibiting the TRIM14/TRAF3/NF-κB axis23. Compared with conventional single-layered microneedles, the double-layered design overcomes limitations such as low drug loading, monomodal release kinetics, and limited drug combination capacity. By implementing spatiotemporally controlled release, bilayered microneedles provide a promising platform for precise, sustained, and synergistic transdermal combination therapy with enhanced clinical translation potential.
Herein, we developed a bilayered microneedle patch for the sustained codelivery of MTX and DXM for psoriasis treatment (Fig. 1). The outer layer was made of a gelatine-polyvinyl alcohol (Gel-PVA) hydrogel, a carrier that combines good mechanical properties (gelatine provides toughness and PVA enhances strength and ensures stratum corneum penetration)24, stimulus responsiveness (temperature/pH), and excellent drug-carrying capability (i.e., can be loaded with hydrophobic molecules via electrostatic/hydrogen bonding). For the inner layer, a methacrylate-amidated hyaluronic acid hydrogel (MeHA-NH2) was selected, which integrates the biological functions of hyaluronic acid (HA) with the photocrosslinking properties of methacrylate moieties, providing significant advantages in drug delivery25. The above properties suggest that this microneedle patch has great potential for application in the clinical treatment of psoriasis, enabling convenient and programmable individualized treatment.

Synthesis and therapeutic mechanism of MTX@DXM-MN patch.
Methods
Preparation of gelatine Polyvinyl alcohol hydrogel (Gel-PVA)
First, 1.0 g of gelatine (Bloom 250–280, Sigma‒Aldrich) was added to 9.0 mL of sterile PBS (pH 7.4) and magnetically stirred (300 rpm, 1 h) at 60 °C until completely dissolved. Then, 1.0 g of PVA (87–89% hydrolysis, Alfa Aesar) was added to 9.0 mL of PBS and stirred (500 rpm, 2 h) at 90 °C until clarified, after which it was cooled to 60 °C, and the two stock solutions were mixed 1:1 at 60 °C. Subsequently, DXM(98%,Shanghai Rhawn Reagents Co., Ltd.) 0.01% (w/v) was added and mixed with PVA-Gel hydrogel.The hydrogel was formed by physical crosslinking. The samples were freeze-dried and analysed using FTIR (Perkin Elmer Spectrum 3, UK, 4000–400 cm−1).
Modification of hyaluronic acid (HA) to aminated hyaluronic acid (HA-NH₂)
HA (100–200 kDa, 1–2 wt%, Macklin) was dissolved in MES buffer (Shanghai yuanye Bio-Technology Co., Ltd, pH 5.5). EDC(Ethyldimethylaminopropyl Carbodiimide, Shanghai Rhawn Reagents Co., Ltd.) and NHS (N-Hydroxysuccinimide, Shanghai Rhawn Reagents Co., Ltd.) (2:1) were added for 2 h at 4 °C to trigger the formation of carboxyl moieties. EDA (Ethylenediamine, Sigma-Aldrich) (COOH: NH₂ = 1:5–1:10) was then added dropwise; the solution was stirred for 12–24 h at room temperature in the dark to obtain HA-NH₂. Purification was carried out by removing unreacted reagents by dialysis (3.5–10 kDa threshold, 48 h, deionized water). The white fluffy solid obtained after lyophilization was stored at 4 °C and characterized by FTIR spectroscopy (PerkinElmer Spectrum 3, UK; 4000–400 cm-¹).
Synthesis of methacrylate-amidated hyaluronic acid (MeHA-NH2) and Preparation of hydrogels
The methacrylation of HA-NH₂ predominantly targets the primary amine groups (-NH₂) under mild alkaline conditions (pH 8.0), where their enhanced nucleophilicity favors the formation of methacrylamide linkages over potential esterification with the less reactive hydroxyl groups. This mechanism, analogous to GelMA synthesis, ensures amide bond formation is the primary pathway.
HA-NH₂ (1 g) was dissolved in 100 ml of ultrapure water, and 5 ml of methacrylic anhydride(94%, Shanghai Rhawn Reagents Co., Ltd.) was introduced dropwise under stirring. The reaction was kept at a pH of 8.0 (adjusted with 5 M NaOH) and allowed to proceed overnight on ice. After dialysis (8 kDa threshold) and lyophilization for 4 days, the resulting MeHA-NH₂ was dried and stored. To form hydrogels, MeHA-NH₂ and LAP (Lithium phenyl-2,4,6-trimethylbenzoylphosphinate, Shanghai Rhawn Reagents Co., Ltd.) photoinitiators were dissolved in PBS to obtain 0.5–2% (v/v) of the polymer and 0.25% (v/v) of the LAP precursor solution, respectively. The mixtures were irradiated by UV light (405 nm, 25 mW cm−²) until crosslinking. The lyophilized hydrogels were characterized by FTIR spectroscopy (PerkinElmer Spectrum 3, UK; 4000–400 cm−¹).
Crosslinking of MeHA-NH2 with MTX amide reaction
MTX(98%,Shanghai yuanye Bio-Technology Co., Ltd.) was dissolved in DMSO and reacted with EDC: NHS: MTX = 2:2:1 (molar ratio) at 4 °C for 2 h to activate the carboxyl groups; then, MeHA-NH₂ was added and reacted overnight to form amide bonds between the carboxyl moieties of MTX and the amino groups of MeHA-NH₂. The products were dialyzed in a 3.5 kDa dialysis bag in deionized water for 3 days, lyophilized to obtain the MTX-MeHA-NH₂ coupling compound, and characterized by FTIR (PerkinElmer Spectrum 3, UK; 4000–400 cm−¹).
Preparation of MTX@DXM-MN
The following types of microneedle moulds were used: negative moulds (microneedle array, 12 × 12; needle length, 800 μm; bottom diameter, 420 μm) and resin-positive moulds (microneedle array, 12 × 12; needle length, 780 μm; bottom diameter, 400 μm). Outer layer: The prepared Gel-PVA and dexamethasone were mixed with thorough stirring, the drug was crosslinked with the hydrogel by hydrogen bonding and vacuum defoaming, the prepared gel was injected into the negative mould by vacuum infusion, and the resin-positive mould was inserted into the negative mould and dried at room temperature for 24 h. The layer serves as the structural backbone of the microneedle and provides the main mechanical strength for its puncture process.Inner layer: First, 2% MTX-MeHA-NH2 was dissolved in PBS with 0.25% LAP photoinitiator, and the hydrogel was photo-crosslinked by exposure to a 405 nm UV light source at an intensity of 25 mW cm-2 for 30 s (cumulative energy density: 300 mJ cm-2). This concentration ensures MTX loading while avoiding the increase in microneedle brittleness due to excessive cross-linking of the inner layers, helping to maintain overall mechanical toughness and achieving sustained MTX release through the formation of a moderately dense gel network.The positive resin mould was removed, the gel was prepared through vacuum infusion into the mould, and 10% PVA substrate liquid was added as the backing layer. The sample was dried at room temperature for 24 h, after which the mould was released under light pressure.This bilayer design achieves partitioned loading and controlled release of both drugs while taking into account mechanical robustness.The microneedles are stored under the following conditions after demolding: temperature: 25 ± 2 °C; humidity: < 30% RH; and protected from light.
Cell culture
The immortalized human keratinocyte line HaCaT was obtained from the BeNa Culture Collection (BNCC, Beijing, China). Upon arrival, the cells were immediately expanded in complete growth medium consisting of high-glucose Dulbecco’s modified Eagle’s medium (Gibco, Grand Island, CA, USA; catalogue no. 11,995,040) supplemented with 10% (v/v) foetal bovine serum (FBS) of Australian origin (Gibco, 10099141 C), 100 U/ml penicillin G sodium, and 100 g/ml streptomycin sulphate. The medium was sterilely filtered (0.22 μm) prior to use and renewed every 48–72 h. The cells were incubated at 37 °C in a humidified environment of 5% CO₂/95% air and subcultured to 70–80% confluence with 0.25% trypsin.
Cell counting kit-8 (CCK8) assay
HaCaT cells were seeded at 8 × 10³ cells per well in 96-well plates and exposed to the specified treatments for the indicated periods. After the corresponding treatments, according to the instructions of the CCK-8 assay kit (Beyotime, Nanjing, China), the cells were maintained at 37 °C for 60 min in fresh high-glucose DMEM containing 10% CCK-8 reagent as the replacement medium. The absorbance value at a wavelength of 450 nm was read on a Multiskan FC microplate reader (Thermo Fisher Scientific, Waltham, MA, USA). The data were normalized to those of the untreated controls and analysed using GraphPad Prism 10.
Staining of proliferating activity by edu
For the proliferation assessment, HaCaT cells were plated at 5 × 10³ cells per well in 48-well plates and cultured for 48 h at 37 °C and 5% CO₂. After a 2-h EdU pulse, the cultures were fixed, permeabilized, and stained with a Beyotime EdU kit. Fluorescence images were acquired on an Olympus BX61 microscope, and EdU-positive nuclei were quantified using ImageJ.
Animal experiments
Male BALB/c mice (18–20 g) were obtained from Yunnan University’s Laboratory Animal Center. The samples were maintained at 21 ± 1 °C and 40–70% relative humidity under a normal light cycle. The experiments followed Kunming Medical University’s IACUC guidelines. Psoriasis-like lesions were induced by the daily topical administration of 62.5 mg of 5% imiquimod cream on the shaved back for seven days; 0.1% tacrolimus ointment (80 mg) was applied dorsally ~ 1 h after each imiquimod dose as a positive control. To minimize animal suffering, mice were humanely euthanized after the final treatment. This was performed by intraperitoneal injection of an overdose of sodium pentobarbital (≥ 150 mg/kg). Death was confirmed by continuous observation for at least 2 min, followed by complete cardiac and respiratory cessation. Cervical spinal dislocation was then used as a secondary physical method to ensure death. Throughout the procedure, animals were handled calmly to avoid unnecessary stress.
Immunohistochemistry and Immunofluorescence staining
Freshly collected mouse skin, heart, liver, spleen, lung and kidney tissues, as well as cells cultured in vitro, were immersed in precooled 4% paraformaldehyde (PFA) fixative at 4 °C for 12–24 h. Subsequently, the tissue blocks were dehydrated, clarified, dipped in wax, embedded, and sectioned. H&E staining was carried out in accordance with the instructions of the HE Staining Kit (Solarbio). H&E-stained and immunostained slides were imaged on an Olympus BX61 upright microscope with consistent exposure parameters, and the resulting images were exported by the accompanying software for subsequent quantitative analysis.
Permeation properties of MTX@DXM-MNs
To assess subcutaneous penetration, fluorescently labelled MTX@DXM-MN/RhB was prepared by incorporating rhodamine B (RhB) into the microneedle matrix at a 1:100 mass ratio. The dorsal skin of healthy mice was shaved, depilated, and disinfected prior to perpendicular application of the microneedle array. After 30 min, a 6-mm-diameter, full-thickness skin sample was collected from the application site, embedded in OCT, cryosectioned, and visualized using fluorescence microscopy.
In vitro biocompatibility of the hydrogels
Cells were inoculated at 5 × 10³/well in 24-well plates and cocultured with the material for 5 d. Calcein-AM/PI live-dead staining was used to label live (green) and dead (red) cells to evaluate gel toxicity. Haemocompatibility was determined by haemolysis: mouse eye blood was anticoagulated with heparin and centrifuged at 3000 rpm for 15 min at 4 °C. Then, the supernatant was discarded, and the cells were washed with PBS until the supernatant was colourless, followed by resuspension to yield a 2% erythrocyte suspension. Subsequently, 1 mL of the sample was mixed with 1 mL of the suspension and incubated at 37 °C for 3 h (with PBS as a negative control and ddH₂O as a positive control). Then, the supernatant was centrifuged at 3500 rpm for 5 min, after which the absorbance was measured at 540 nm, and the haemolysis rate was calculated.
Drug release from MTX@DXM-MNs
Dialysis-based in vitro release of MTX and DXM from MTX@DXM-MNs was assessed under two distinct conditions: physiological (pH 7.4, 32 °C) and inflamed (pH 5.0, 32 °C) conditions. The MTX@DXM-MN patch was sealed inside a dialysis bag and immersed in PBS, followed by incubation at 32 °C with agitation at 100 rpm. At 0, 2, 4, 6, 8, 12, 24 and 48 h, 3 mL of medium was withdrawn, and the mixture was replenished with an equal volume of fresh buffer. The release of MTX was measured at 302 nm and DXM at 240 nm using a UV‒visible spectrophotometer, and the cumulative release curves of MTX and DXM were plotted.
Inflammatory factor analysis
Protein level determination by ELISA
On day 7 post-modeling, orbital blood was collected from the mice. The blood samples were centrifuged at 3,000 × g for 10 min at 4 °C to obtain plasma, which was then centrifuged at 12,000 × g for 10 min at 4 °C to acquire cell-free serum. The serum was aliquoted and stored at −80 °C until analysis. In parallel, TIB-71 macrophages (ATCC) were seeded into 24-well plates at a density of 2 × 10⁵ cells per well and cultured for 12 h. The cells were then stimulated by replacing the medium with serum-free DMEM containing 50 µg/mL TNF-α. After 24 h of incubation, the culture supernatant was collected and centrifuged at 3,000 × g for 5 min at 4 °C to remove cellular debris. The clarified supernatant was aliquoted and stored at −80 °C. Cytokine levels (TNF-α, IL-6, IL-1β, IL-17 A) in both serum and cell culture supernatant were quantified using commercial ELISA kits (Lianke Biotech, Hangzhou, China) according to the manufacturer’s instructions. Briefly, 100 µL of each standard or sample was added to the coated wells and incubated for 2 h at 37 °C. After washing, a detection antibody was added and incubated, followed by the addition of a substrate solution after a second wash. The reaction was stopped, and the absorbance was measured at 450 nm. All samples were analyzed in duplicate. Statistical analysis was performed with n = 3 biological replicates (serum samples from 3 mice per group) for in vivo data, and n = 3 independent cell culture experiments for in vitro data.
Gene level detection (RT‒qPCR)
HaCaT cells were harvested, and total RNA was extracted using TRIzol Reagent (Invitrogen). The RNA concentration and purity were verified by measuring the A260/A280 ratio. Subsequently, 1 µg of total RNA was reverse-transcribed into cDNA using the PrimeScript RT Master Mix (Takara). Quantitative PCR (qPCR) was performed using SYBR Green Premix Pro Taq HS (Accurate Biology) on a QuantStudio 5 Real-Time PCR System (Applied Biosystems). The reaction mixture (20 µL total volume) consisted of 10 µL of SYBR Green Premix, 0.8 µL each of forward and reverse primers (10 µM), 2 µL of cDNA template, and 6.4 µL of nuclease-free water. The thermal cycling conditions were as follows: initial denaturation at 95 °C for 30 s, followed by 40 cycles of 95 °C for 5 s and 60 °C for 30 s. The relative mRNA expression levels of TNF-α, Arg-1, CD86, and CD206 were determined, normalized to GAPDH as an endogenous control. Each sample was analyzed in technical duplicate across three independent biological replicates (n = 3). The primer sequences are listed in Table 1.
Transcriptome analysis of skin tissue
Skin samples from three independent mice in each model group and treatment group. All samples are sourced from the same developmental stage/tissue site and collected at the same time point to minimize batch effects.Grouping method: Both model and treatment groups are randomly assigned to avoid systematic bias. Send samples (shipped with dry ice) to Novogene Co., Ltd. in Beijing. Novogene will complete subsequent experiments according to standard procedures.
Data analysis
All statistical analyses were conducted using GraphPad Prism 10. The data are presented as the mean ± SEM. One-way ANOVA with Tukey’s multiple comparison test was used. A P value < 0.05 was considered to indicate statistical significance.
Results
MTX@DXM-MN Preparation and FTIR characterization
To codeliver MTX and DXM for psoriasis therapy, we engineered a dissolving bilayered microneedle array (MTX@DXM-MNs). The outer layer was a Gel-PVA hydrogel loaded with DXM, and the inner layer was a MeHA-NH2 hydrogel loaded with MTX. To prepare the inner hydrogel, we first grafted -NH2 with HA to generate HA-NH2, which reacted with methacrylic anhydride to form MeHA-NH2, and then loaded MTX into MeHA-NH2 by an amide reaction. To prepare the outer hydrogel, we mixed Gel and PVA at a specific ratio to make a hydrogel and then added DXM and mixed it to make the outer layer. Then, the prepared hydrogels were filled sequentially into the microneedle array mould (Fig. 2A).
Fourier transform infrared spectroscopy (FTIR) analysis revealed the following characteristic peaks: as shown in Fig. 2B, the FTIR spectrum of pure PVA showed a broadband peak at 3330 cm−1, which was attributed to O-H stretching, likely resulting from inter- and intramolecular hydrogen bonding. The peak at 2939 cm−1 was ascribed to vibrational bending from alkyl C-H bonding. The peak at 1485 cm−1 was attributed to alkyl C-H bonding; and the peak at 1485 cm−1 was attributed to vibrational bending due to the stretching of alkyl C-H bonds. The peaks at 1485 cm−1 and 1342 cm−1 represent the shear motion of -CH2 groups and the vibrational bending of -OH groups, respectively. On the infrared spectra of Gel, the peak at 3280 cm−1 represents the synergistic stretching vibration of the amide N-H and the amide O-H in the gelatine; 2930 cm−1 is representative of the stretching vibration of aliphatic C-H bonds, namely -CH₂-. The absorption peak at 1650 cm−1 is caused by the stretching vibration of C = O in the amide bond on the main chain. The FTIR peaks of the Gel-PVA hydrogel are at 3280 cm−1 (O-H/N-H), 1650 cm−1 (amide I) and 1093 cm−1(C-O). The spectra of DXM exhibited a distinctive peak at 3473 cm−1 for the 11-position hydroxyl O-H stretching vibration, 2942 cm−1 for the aliphatic C-H stretching vibration, and 1618 cm−1 for the C = C stretching vibration (conjugated double bond). The infrared absorption at 1451 cm−1 can be attributed to the shear bending vibration of aliphatic C-H. After loading DXM on the Gel-PVA hydrogel, the O-H stretching peak (near 3300 cm−1) clearly broadened, reflecting the generation of hydrogen bonds linking PVA, gelatine, and DXM; the amide I band of gelatine (1650 cm−1) overlapped with the C = O peak of DXM, and the peak shape was broadened.
As shown in Fig. 2C, the infrared spectrum of HA showed a peak at 3434 cm−1 for hydroxyl group stretching vibration, 3080 cm−1 for amide N-H stretching vibration, 1638 cm−1 for the C = O stretching vibration of carboxylate/amide I, and 1066 cm−1 for the C-O stretching vibration of the glycocyclic C-OH. The infrared spectrum of HA-NH2 showed a sharp N-H stretching vibration peak at 3301 cm−1 compared with that of HA, which proves the successful modification of hyaluronic acid with amino groups and MeHA. The FTIR spectrum of MeHA showed a characteristic peak at 1720 cm-1, which may be attributed to the C = O stretching vibration of a methacrylate ester, suggesting a potential minor side reaction with hydroxyl groups. However, the dominant absorption bands at 1634 cm-1 and 1546 cm-1, corresponding to the amide I and II bands respectively, provide clear evidence that the primary reaction pathway was the formation of amide bonds via the reaction between the amine groups of HA-NH₂ and methacrylic anhydride. The infrared spectra of MTX showed a peak at 3361 cm−1 for N-H stretching vibration (amide/amido group); 2958 cm−1 for aliphatic C-H stretching vibration (CH₃/CH₂); 1680 cm−1 for carboxylic acid C = O stretching vibration (-COOH); 1600 cm−1 for aromatic ring C = C skeleton vibration; and 1445 cm−1 for CH₃ bending vibration. Successful conjugation to form MTX@MeHA-NH₂ was confirmed by the emergence and intensification of the amide I and II bands (1634 cm-1 and 1546 cm-1) in the conjugate’s spectrum.

Preparation and structural characterization of MTX@DXM-MN Double-Layer Microneedles. (A) Demonstration of the preparation process of MTX@DXM-MN. (B)FT-IR spectra of the outer layer components (Gel-PVA and DXM@Gel-PVA). (C)FT-IR spectra of the inner layer components (MeHA-NH₂ and MTX@MeHA-NH₂).
Multimodal performance characterization of MTX@DXM-MNs
The cross-sectional CLSM image of MTX@DXM-MNs (Fig. 3A) distinctly reveals the successful fabrication of a bilayer structure. The green fluorescence (FITC-labeled DXM) is predominantly localized within the needle’s outer layer, whereas the red fluorescence (Rhodamine B-labeled MTX) is exclusively confined to the inner core. The clear spatial segregation between the two fluorescent signals, with minimal overlap, provides direct visual evidence for the compartmentalized loading of the two drugs. The microneedle arrays exhibited a 12 × 12 arrangement, and each needle was tapered to a height of 800 μm, a diameter of 420 μm at the base, and a tip radius of curvature of less than 10 μm, which is sufficient to efficiently penetrate the stratum corneum (Fig. 3B). SEM and fluorescence imaging revealed that the microneedles had smooth surfaces, intact morphologies, and sharp tips (Fig. 3C). Previous studies have suggested that the critical load required for a single microneedle to break through the stratum corneum is approximately 0.058 N26, and the results of the force‒displacement test confirmed that the maximum force that the microneedles could withstand was 187.15 N, and the average maximum force per needle was 1.30 N, indicating that the microneedles possessed sufficient mechanical strength to penetrate the skin smoothly without fracture or collapse (Fig. 3D).In addition, the microneedle-induced pores vanished within 30 min, underscoring the minimal invasiveness of the system (Fig. 3E). The penetration of the rhodamine B-labelled MTX@DXM-MNs was subsequently imaged by fluorescence microscopy to validate the epidermal puncture ability of the microneedle as well as the diffusion of the matrix (Fig. 3F). Significant fluorescence accumulation was observed after 30 min of transdermal delivery, and microporous channels were visible, confirming the efficient penetration of the microneedles.
The efficacy of microneedles is closely related to drug release kinetics. Psoriatic lesions are weakly acidic (pH ≈ 5) and have a low temperature (≈ 32 °C), which is significantly different from that of normal skin27,28. Therefore, we compared the release behaviour of MTX@DXM-MNs in two environments: under simulated lesion conditions, DXM release at 1 h was about 54%. Compared to DXM release, the release behavior of pre-MTX was relatively slow at about 12%, and then both remained relatively slow for the next 48 h, working together to exert therapeutic effects, whereas in normal physiological environments, the release rate of both drugs was significantly reduced (Fig. 3G, H).

Characterization of MTX@DXM-MN bilayer microneedles. (A) Dual-layer fluorescence image of MTX@DXM-MN. (B) Full image display of MTX@DXM-MN. (C) SEM image of MTX@DXM-MN, scale bars: 30, 200 and 100 μm. (D) Mechanical testing of MTX@DXM-MN. (E) Penetration force of MTX@DXM-MN into skin. (F) Fluorescence microscopic image of Rho B-labeled MTX@DXM-MN penetrating mouse skin. (G-H) In vitro drug release curves of MTX@DXM-MN. Data represent three independent experiments.
MTX@DXM-MNs inhibit the proliferation and migration of TNF-α-treated HaCaT cells
To evaluate the in vitro effects of MTX@DXM-MNs, a gradient concentration was used to test toxicity to HaCaT cells. Different concentrations of MTX@DXM-MNs and blank microneedles (MNs) were aseptically extracted in DMEM for 5 days, and the extracts were filtered and collected to treat HaCaT cells, which revealed > 85% cell viability when the cells were treated with 1 µg/mL MTX@DXM-MN extract (Fig. 4A); therefore, this concentration was used for subsequent experiments. After 24 h, calcein-AM/PI double staining revealed that the cell morphology in each group was intact and clear, and the proportion of viable cells remained comparable to that in the control group (Fig. 4B). Moreover, a haemolysis assay using mouse erythrocytes revealed no appreciable lysis after exposure to graded concentrations of MTX@DXM-MN extract, in sharp contrast to the complete haemolysis observed in the ultrapure-water positive control, confirming that the microneedle patch had low toxicity and excellent biocompatibility (Fig. 4C). To evaluate the effect of MTX@DXM-MNs on keratinocyte behaviour under psoriatic conditions, an inflammatory microenvironment was simulated using TNF-α, and stimulated cells were cocultured with microneedle extract for 3 days. EdU proliferation and scratch assays demonstrated that compared with TNF-α alone, treatment with MTX@DXM-MN extract significantly inhibited both HaCaT cell proliferation and migration, whereas no differences were observed between the blank MN group and the TNF-α alone group (Fig. 4D-G).

The inhibitory effect of MTX@DXM-MN on TNF-α-induced HaCaT cells in vitro. (A)Cell viability after 48 h after co-culture of various patch with HaCaT cells. (B) Calcein-AM/PI staining results after co-culture of various patch with HaCaT cells. Scale bar: 50 μm. (C) Hemolysis test of different concentrations of MTX@DXM-MN. The positive control was water, and the negative control was PBS. (D-E) Representative EDU cell images and positive value-added rate after 3 days of co-culture of various patch with HaCaT cells. Scale bar: 50 μm. (F-G) Representative HaCaT cell images and migration rate after 24 h of co-culture of various patch with HaCaT cells. Scale bar: 50 μm. Data is presented as mean ± SEM. *p < 0.05; **p < 0.01; ***p < 0.001; ns, not significant. One-way ANOVA with Tukey’s multiple comparisons test in (E and G). Scale bars are indicated. Data are representative of three independent experiments.
MTX@DXM-MNs regulate macrophage polarization
Psoriasis is a chronic inflammatory dermatosis driven in large part by macrophage-mediated pathogenesis29. Given the clear anti-inflammatory properties of dexamethasone, we explored the effects of MTX@DXM-MNs on macrophage polarization in response to inflammatory TNF-α stimulation in vitro by coculturing MTX@DXM-MN extract with RAW264.7 macrophages stimulated with TNF-α. Compared with TNF-α stimulation alone, treatment with MTX@DXM-MN extract markedly decreased the expression of CD86 (an M1 polarization marker) and upregulated the expression of CD206 (an M2 marker). In contrast, the administration of MN extract after TNF-α challenge did not significantly affect the expression of either marker (Fig. 5A-B). RT‒PCR analysis further confirmed that MTX@DXM-MN extract treatment significantly decreased the mRNA levels of M1-associated proinflammatory cytokines (TNF-α and CD86) but significantly increased the mRNA levels of M2-associated anti-inflammatory cytokines (CD206 and Arg-1) (Fig. 5C-F).
In addition, an enzyme-linked immunosorbent assay of RAW264.7 cell culture supernatants revealed that compared with TNF-α stimulation alone, treatment with MN extract after TNF-α stimulation markedly suppressed the secretion of key inflammatory cytokines (TNF-α, IL-6, IL-1β, and IL-17 A) (Fig. 5G-J). In conclusion, MTX@DXM-MNs effectively suppressed macrophage polarization towards the proinflammatory M1 phenotype, promoted macrophage polarization towards the anti-inflammatory M2 phenotype under inflammatory conditions in vitro, and significantly suppressed the expression of inflammatory factors.

MTX@DXM-MN promotes the polarization of RAW264.7 cells towards the M2 phenotype thereby facilitating inflammation regulation. (A-B) Representative immunofluorescence images illustrating macrophage polarization markers. CD206 serves as an M2 macrophage marker, while CD86 represents the M1 macrophage marker. (C-F) Evaluation of the relative mRNA expression levels of TNF-α (C), Arg-1 (D), CD86 (E) and CD206 (F) in RAW264.7 cells under different conditions. (G-J) ELISA detection of TNF-α, IL-6, IL-1β, and IL-17 A expression in the supernatant of RAW24.7 cells from each group. Data is presented as mean ± SEM. *p < 0.05; **p < 0.01; ***p < 0.001; ns, not significant. One-way ANOVA with Tukey’s multiple comparisons test in (C-F). (G-J) analyzed using one-way ANOVA with Tukey’s post-hoc test. Scale bars are indicated. Data are representative of three independent experiments.
Therapeutic efficacy and biosafety evaluation of MTX@DXM-MNs in IMQ-induced psoriasis
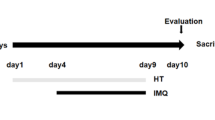
We assessed the efficacy of MTX@DXM-MNs using a murine model of IMQ-induced psoriasiform dermatitis. After the model was established by the continuous application of IMQ to the dorsum of BALB/c mice, microneedle patches were aseptically pressed onto the lesion areas daily (Fig. 6A). Daily monitoring of body weight revealed no significant difference between the groups (Fig. 6B), suggesting that the treatment did not cause significant systemic toxicity. Given the systemic nature of psoriasis, we further tested the splenic index to assess the systemic inflammatory response. Compared with the model group, both the MTX@DXM-MN group and the tacrolimus positive-control group showed significantly reduced splenic indexes and effectively suppressed splenomegaly, confirming the systemic anti-inflammatory effect of MTX@DXM-MNs (Fig. 6C). Macroscopic observation revealed that IMQ induced typical psoriasis-like lesions, including erythema, scaling, and dorsal skin thickening (Fig. 6D). MTX@DXM-MN treatment significantly improved these clinical signs compared with those in the untreated group or the model group treated only with blank MN patches. Histopathological (H&E staining) analysis further demonstrated that MTX@DXM-MNs attenuated IMQ-induced epidermal thickening and dermal inflammatory cell infiltration (Fig. 6D). Notably, compared with the blank, the MTX@DXM-MNs exhibited superior efficacy in mitigating erythema, scaling, and cutaneous thickening, with significantly lower cumulative PASI scores by day 7 (Fig. 6E).

Therapeutic effect of MTX@DXM-MN on IMQ-induced psoriasis in vivo. (A) Experimental timeline diagram illustrating imiquimod-induced psoriasis treatment. (B) Changes in mean body weight in each group. (C) Optical images of spleen and spleen index (spleen weight/body weight) in each group. (D) Images displaying mice treated with various patch and Representative sections of mice skin stained with Hematoxylin and Eosin (H&E). Normal mice (Normal); the untreated psoriasis mice (Model); the treated psoriasis mice (MN); the treated psoriasis mice (MTX@DXM-MN); the positive control (Tacrolimus). Scale bar: 100 μm&50 μm. (E-H) Psoriasis scores of mice after different treatments. Erythema, scale, thickness, and cumulative scores were assessed from day 0 to day 7. The PASI score on day 7 were used for statistical analysis. Data is presented as mean ± SEM. *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001; ns, not significant. One-way ANOVA with Tukey’s multiple comparisons test in (C and E-H). Scale bars are indicated. Data are representative of three independent experiments.
To elucidate the mechanism of action of MTX@DXM-MNs in the psoriasiform IMQ mouse model, we performed correlation analysis. Consistent with the previous results, immunohistochemical staining revealed that the expression of Ki67, a proliferation marker in skin lesion tissues, was significantly downregulated after treatment with MTX@DXM-MNs (Fig. 7A), suggesting that the treatment effectively inhibited the abnormal proliferation of keratinocytes, which coincided with the observed reduction in epidermal thickness. Further analysis of the local immune environment of the lesions revealed that MTX@DXM-MN treatment significantly reduced inflammatory cell infiltration and decreased the expression of local inflammatory cytokines, indicating favourable anti-inflammatory properties (Fig. 7A). This anti-inflammatory response was further confirmed systemically: circulating levels of the pivotal proinflammatory mediators TNF-α, IL-6, IL-1β, and IL-17 A were markedly diminished by MTX@DXM-MN treatment (Fig. 7B-E). In addition, H&E staining of important organs (heart, liver, spleen, lungs, and kidneys) did not reveal significant morphological abnormalities or inflammatory cell infiltration (Fig. 7F). In conclusion, MTX@DXM-MN patches have potential as a therapeutic strategy for psoriasis by inhibiting the hyperproliferation of keratinocytes and attenuating local and systemic inflammatory responses with a favourable safety profile.

Effect of MTX@DXM-MN on the expression of inflammatory factors in IMQ mice and Assessment of in vivo biosafety. (A) Immunohistochemical images of IL-17 A, IL-6, TNF-α, and Ki67 in psoriatic skin of each group. Scale bar: 50 μm. (B-E) ELISA assay for the expression of IL-1β, IL-17 A, IL-6 and TNF-α in serum of each group. (F) Representative H&E-stained sections of the heart, liver, spleen, lungs, and kidneys across various groups. Scale bar: 50 μm. Data is presented as mean ± SEM. *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001; ns, not significant. One-way ANOVA with Tukey’s multiple comparisons test in (B-E). Scale bars are indicated. Data are representative of three independent experiments.
Transcriptomic profiling to reveal the therapeutic mechanism of MTX@DXM-MNs in psoriasis
To corroborate the experimental findings from cellular and animal studies and elucidate the proposed mechanism of action, a comprehensive analysis of total transcriptome RNA sequencing was performed on six randomly selected skin samples, including those from the model group (model) and the MTX@DXM-MN treatment group (MN-drug). Principal component analysis (PCA) based on gene expression motifs was first performed, revealing differences in transcriptome segregation along the first principal component (PC1) between the model and MN-drug groups. This visualization effectively illustrated the marked divergence in the transcriptomes of the two cohorts (Fig. 8A). A Venn diagram revealed 13,039 coexpressed genes in the model and MN-drug groups (Fig. 8B). The violin plot demonstrated the gene expression distribution, suggesting that the MN-drug group may have reduced variability of gene expression (Fig. 8C). Compared with those from the model group, skin samples from the MTX@DXM-MN-treated group presented 617 differentially expressed genes (428 upregulated and 189 downregulated) (Fig. 8D-F).
KEGG enrichment analysis of the differentially expressed genes revealed significant involvement of cytokine‒cytokine receptor interactions, cell adhesion molecules, NOD-like receptor signalling, and chemokine signalling pathways (Fig. 8G). These pathways are primarily associated with inflammatory and proliferative processes, indicating their potential regulatory roles in response to MTX@DXM-MN treatment. GO term enrichment further highlighted significant terms related to epidermal development, tissue morphogenesis, and cytokine binding within the biological process and molecular function categories (Fig. 8H), suggesting that the modulation of inflammatory responses and skin regeneration are central to the therapeutic mechanism of MTX@DXM-MNs.

Transcriptome sequencing analysis of the MTX@DXM-MN group and the Model group. (A) Correlation coefficient graphs and 2D/3D clustering graphs of the MTX@DXM-MN group and the model group. (B)The Veen diagram shows the co-expressed genes in the MTX@DXM-MN treatment group and the model group. (C) The violin plot shows the distribution of gene expressions in the MTX@DXM-MN treatment group and the model group. (D)The volcano plot shows the differentially expressed genes (DEGs) in the MTX@DXM-MN treatment group and the model group. (E-F) This heatmap presents the union of DEGs in the MTX@DXM-MN treatment group and the model group, as well as the statistics of the number of differentially expressed genes. (G) Bubble plot showing the results of KEGG pathway enrichment analysis for differentially expressed genes. (H) Bubble plot showing the results of Gene Ontology (GO) enrichment analysis for differentially expressed genes. Data is presented as mean ± SEM. *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001; ns, not significant.
Discussion
Psoriasis is a chronic inflammatory dermatosis driven by persistent activation of TNF-α and IL-23/IL-17 and is characterized by unchecked keratinocyte hyperproliferation, compromised epidermal barrier integrity, and dysregulated immunity30,31. TNF-α, a key early mediator of inflammation, triggers the secretion of proinflammatory cytokines, including IL-1, IL-6, and CXCL10, and drives neutrophils and T cells to infiltrate the epidermis32, where along with IL-17, they promote dendritic cell maturation and Th17 expansion, forming a positive feedback of loop of inflammation and proliferation33,34,35. Keratinocytes, as the core target and source of inflammatory mediators/chemokines, can be activated by LL37-DNA/IFN-γ and secrete large amounts of type I interferon and chemokines, which continuously amplify local inflammation and lead to disease progression36,37,38.
Although the combination of MTX and DXM in clinical practice enhances anti-inflammatory efficacy and allows for lower individual drug doses, its oral administration remains constrained by pronounced first-pass effects, resulting in poor bioavailability and a potential risk of cumulative toxicity39. Topical administration is inefficient because of limited stratum corneum barrier penetration39. In this regard, we developed a MTX@DXM-MN patch that physically penetrates the stratum corneum in a painless and minimally invasive manner40,41 and targets drug delivery to dermal lesions, first with the rapid-acting anti-inflammatory DXM and then with the continuous immunosuppressant MTX. This approach significantly enhances drug bioavailability42,43, providing a new strategy for the safe and efficient topical treatment of psoriasis.
The core of the patch design is spatiotemporal programmed drug release: the outer layer of DXM is rapidly released within minutes44, directly inhibiting TNF-α/IL-6 signalling in keratinocytes and infiltrating immune cells for rapid relief of erythema and itching, whereas the inner layer of MTX is slowly released (> 24 h)43 to mediate long-lasting immunomodulation through the inhibition of folate metabolism and T-cell proliferation. The bilayered structure physically isolates the drugs44,45, circumvents compounding contraindications (e.g., pH incompatibility), and reduces focal loss of MTX from the inner layer because of inflammatory exudation by lowering local vascular permeability through the outer layer of DXM. The material is made of biodegradable polymers (e.g., hyaluronic acid), which completely dissolve within 10 min and reduce the risk of infection46.
Compared with traditional topical formulations, this double-layered microneedle patch has the following core advantages: (1) physical penetration of the stratum corneum, significantly increasing the amount of drug exposure at the lesion site47; (2) spatial and temporal sequential release of a rapid anti-inflammatory agent followed by an immunosuppressant to match the acute-chronic biphasic course of psoriasis48; and (3) physical isolation of each active ingredient by the bilayered architecture, which prevents incompatibility, enables rapid dissolution of the outer DXM layer, and preserves the sustained-release profile of the inner MTX core. The double-layered structure physically segregates the active ingredients, avoiding contraindications and ensuring that the rapid dissolution of DXM in the outer layer does not affect the slow-release kinetics of MTX in the inner layer49. However, the current design still has the following shortcomings: the methacrylation degree of the HA-based precursor was not determined by ¹H NMR analysis; limited drug loading (which needs to be enhanced by surface modification or optimization of carrier‒drug interactions)50; an insufficient in vivo period (7 days) for assessing skin tolerance, with the potential for microresidues under long-term repeated applications51; and a lack of human dermal Franz diffusion data and GLP toxicity studies48.
In conclusion, the MTX@DXM-MN patch provides a novel topical drug delivery strategy for psoriasis with clinical translational potential through the spatial and temporal synergy of the outer layer and inner layers; the patch breaks through the stratum corneum barrier, reduces systemic toxicity, and provides individualized treatment that is painless, convenient, and programmable.
Data availability
All data generated for this study are available from the corresponding authors upon reasonable request.
References
Ma, R. et al. Association between systemic immune inflammation index, systemic inflammation response index and adult psoriasis: evidence from NHANES[J]. Front. Immunol. 15, 1323174 (2024).
Chen, H. et al. Controlled delivery of MTX from thermosensitive hydrogels using Au nanorods for enhanced therapeutics of psoriasis via improving stratum corneum Penetration[J]. Small 21 (9), e2410566 (2025).
Bruni, M. et al. Psoriasis and cancer: the role of inflammation, immunosuppression, and cancer treatment[J]. Expert Opin. Biol. Ther. 25 (4), 395–411 (2025).
Orzan, O. A., Tutunaru, C. V. & Ianosi, S. L. Understanding the intricate pathophysiology of psoriasis and related skin Disorders[J]. Int. J. Mol. Sci. 26(2), 749 (2025).
Sbidian, E. et al. Systemic Pharmacological treatments for chronic plaque psoriasis: a network meta-analysis[J]. Cochrane Database Syst. Rev. 5 (5), CD011535 (2022).
Sobolev, V. V., Denisova, E. V., Chebysheva, S. N., Geppe, N. A. & Korsunskaya, I. M. IL-6 gene expression as a marker of pathological state in psoriasis and psoriatic Arthritis[J]. Bull. Exp. Biol. Med. 173 (1), 77–80 (2022).
Wu, S., Xu, Y., Yang, L., Guo, L. & Jiang, X. Short-term risk and long-term incidence rate of infection and malignancy with IL-17 and IL-23 inhibitors in adult patients with psoriasis and psoriatic arthritis: a systematic review and meta-analysis[J]. Front. Immunol. 14, 1294416 (2023).
Sugumaran, D., Yong, A. C. H. & Stanslas, J. Advances in psoriasis research: from pathogenesis to therapeutics[J]. Life Sci. 355, 122991 (2024).
Griffiths, C. E. M., Armstrong, A. W., Gudjonsson, J. E. & Barker, J. Psoriasis[J] Lancet, 397(10281):1301–1315. (2021).
Yang, F., Lv, J., Huang, Y., Ma, W. & Yang, Z. A supramolecular assembly strategy for the treatment of rheumatoid arthritis with ultrasound-augmented inflammatory microenvironment reprograming[J]. Biomaterials 316, 123006 (2025).
Chen, Z. et al. Dermal immune responses against Psoroptes Ovis in two cattle breeds and effects of anti-inflammatory dexamethasone treatment on the development of psoroptic mange[J]. Vet. Res. 52 (1), 1 (2021).
Shen, S. et al. Methotrexate-loaded hyaluronan-modified liposomes integrated into dissolving microneedles for the treatment of psoriasis[J]. Eur. J. Pharm. Sci. 195, 106711 (2024).
Sevilla, L. M. et al. Glucocorticoid receptor controls atopic dermatitis inflammation via functional interactions with P63 and autocrine signaling in epidermal keratinocytes[J]. Cell. Death Dis. 15 (7), 535 (2024).
Choonhakarn, C., Chaowattanapanit, S., Julanon, N. & Limpawattana, P. Comparison of the clinical efficacy of subcutaneous vs. oral administration of methotrexate in patients with psoriasis vulgaris: a randomized controlled trial[J]. Clin. Exp. Dermatol. 47 (5), 942–948 (2022).
Khaitan, B. K. & Gupta, S. Total cumulative dose of methotrexate is not the same as continuous cumulative dose: A clinician’s Perspective[J]. Indian Dermatol. Online J. 11 (3), 425–427 (2020).
Zeng, S., Zhang, J., Zu, G. & Huang, J. Transparent, flexible, and multifunctional starch-based double-network hydrogels as high-performance wearable electronics[J]. Carbohydr. Polym. 267, 118198 (2021).
Yu, Y. Q., Yang, X., Wu, X. F. & Fan, Y. B. Enhancing Permeation of Drug Molecules across the Skin Via Delivery in Nanocarriers: Novel Strategies for Effective Transdermal Applications[J] Vol. 9, 646554 (Front Bioeng Biotechnol, 2021).
Wollina, U., Tirant, M., Vojvodic, A. & Lotti, T. Treatment of psoriasis: novel approaches to topical Delivery[J]. Open. Access. Maced J. Med. Sci. 7 (18), 3018–3025 (2019).
Wang, C. et al. Enhancing Deep-Seated melanoma therapy through wearable Self-Powered microneedle Patch[J]. Adv. Mater. 36 (11), e2311246 (2024).
Prabhu, A., Baliga, V., Shenoy, R., Dessai, A. D. & Nayak, U. Y. 3D printed microneedles: revamping transdermal drug delivery systems[J]. Drug Deliv Transl Res. 15 (2), 436–454 (2025).
Huang, L. et al. An approach for psoriasis of microneedle patch simultaneously targeting multiple inflammatory cytokines and relapse related T cells[J]. Biomaterials 318, 123120 (2025).
Qu, F., Geng, R., Liu, Y. & Zhu, J. Advanced nanocarrier- and microneedle-based transdermal drug delivery strategies for skin diseases treatment[J]. Theranostics 12 (7), 3372–3406 (2022).
Li, M. et al. Cannabidiol-loaded hydrogel microneedle patches inhibit TRIM14/TRAF3/ NF-kappaB axis for the treatment of psoriasis[J]. Int. J. Biol. Macromol. 304 (Pt 2), 140825 (2025).
Xu, Y., Yang, H., Zhu, H., Jiang, L. & Yang, H. Self-healing gelatin-based shape memory hydrogels via quadruple hydrogen bonding and coordination crosslinking for controlled delivery of 5-fluorouracil[J]. J. Biomater. Sci. Polym. Ed. 31 (6), 712–728 (2020).
Nedunchezian, S. et al. Characteristic and chondrogenic differentiation analysis of hybrid hydrogels comprised of hyaluronic acid methacryloyl (HAMA), gelatin methacryloyl (GelMA), and the Acrylate-Functionalized Nano-Silica Crosslinker[J]. Polymers (Basel), 14(10) (2022).
Bi, D. et al. Reactive oxygen Species-Responsive Gel-Based microneedle patches for prolonged and intelligent psoriasis Management[J]. ACS Nano. 17 (5), 4346–4357 (2023).
Jing, Q. et al. Keratinocyte membrane-mediated nanodelivery system with dissolving microneedles for targeted therapy of skin diseases[J]. Biomaterials 278, 121142 (2021).
Gao, X. et al. Site-Specifically launched microneedles for the combined treatment of Psoriasis-Diabetic Comorbidity[J]. ACS Appl. Mater. Interfaces. 15 (40), 46613–46625 (2023).
Lu, Y. et al. Adenosine A2A receptor activation regulates the M1 macrophages activation to initiate innate and adaptive immunity in psoriasis[J]. Clin. Immunol. 266, 110309 (2024).
Fadel, A. et al. Erythrodermic psoriasis in the context of emerging triggers: insights into Dupilumab-Associated and COVID-19-Induced psoriatic Disease[J]. Dermatopathology (Basel), 12(2), (2025).
Potestio, L. et al. The role of Interleukin 23/17 axis in psoriasis management: A comprehensive review of clinical Trials[J]. Clin. Cosmet. Investig Dermatol. 17, 829–842 (2024).
Zhao, H. et al. Inflammation and tumor progression: signaling pathways and targeted intervention[J]. Signal. Transduct. Target. Ther. 6 (1), 263 (2021).
Ehst, B. et al. Synergistic induction of IL-23 by TNFalpha, IL-17A, and EGF in keratinocytes[J]. Cytokine 138, 155357 (2021).
Bunte, K. & Beikler, T. Th17 cells and the IL-23/IL-17 axis in the pathogenesis of periodontitis and Immune-Mediated inflammatory Diseases[J]. Int. J. Mol. Sci. 20(14), 3394 (2019).
Ben Abdallah, H., Johansen, C. & Iversen, L. Key signaling pathways in psoriasis: recent insights from antipsoriatic Therapeutics[J]. Psoriasis (Auckl). 11, 83–97 (2021).
Yang, B. et al. Significance of LL-37 on Immunomodulation and Disease Outcome[J]. Biomed. Res. Int., 2020, 8349712 (2020).
Armstrong, A. W. et al. Psoriasis[J]. Nat. Rev. Dis. Primers. 11 (1), 45 (2025).
Armstrong, A. W., Read, C. & Pathophysiology Clinical Presentation, and treatment of psoriasis: A Review[J]. JAMA 323 (19), 1945–1960 (2020).
Pucek, A., Tokarek, B., Waglewska, E. & Bazylinska, U. Recent advances in the structural design of photosensitive agent formulations using soft colloidal Nanocarriers[J]. Pharmaceutics 12(6), 587 (2020).
Jung, J. H. & Jin, S. G. Microneedle for transdermal drug delivery: current trends and fabrication[J]. J. Pharm. Investig. 51 (5), 503–517 (2021).
Zheng, B. et al. Microorganism microneedle micro-engine depth drug delivery[J]. Nat. Commun. 15 (1), 8947 (2024).
Shinde, S., Singh, A. K., Chidrawar, V. R., Rajput, A. & Singh, S. Enhanced topical delivery of methotrexate via Transferosome-Loaded microneedle array patch: Formulation, Optimization, and in Vitro-In vivo Assessment[J]. Pharmaceuticals (Basel) 18(4), 594 (2025).
Wang, J. et al. Promising strategies for transdermal delivery of arthritis drugs. Microneedle Systems[J] Pharm. 14(8), 1736 (2022).
Zhang, B. et al. Double-Layer Nucleoside-Microneedles Co-Delivering dexamethasone vesicles and adenosine overcome pseudomembrane barriers for the treatment of oral Ulcer[J]. ACS Nano. 19 (27), 25204–25227 (2025).
Xu, B. et al. Novel double-layered PLGA microparticles-dissolving microneedle (MPs-DMN) system for peptide drugs sustained release by transdermal delivery[J]. Int. J. Pharm. 670, 125128 (2025).
Du, H. et al. Hyaluronic Acid-Based dissolving microneedle patch loaded with methotrexate for improved treatment of Psoriasis[J]. ACS Appl. Mater. Interfaces. 11 (46), 43588–43598 (2019).
Zhang, W. et al. Double-Layered microneedle patch integrated with multifunctional nanoparticles and live bacteria for Long-Term treatment of atopic Dermatitis[J]. Small 21 (3), e2409121 (2025).
Meng, Y. et al. Novel Double-Layer dissolving microneedles for transmucosal sequential delivery of multiple drugs in the treatment of oral mucosa Diseases[J]. ACS Appl. Mater. Interfaces. 15 (11), 13892–13906 (2023).
Than, A. et al. Self-implantable double-layered micro-drug-reservoirs for efficient and controlled ocular drug delivery[J]. Nat. Commun. 9 (1), 4433 (2018).
Du, H. et al. Microneedle-assisted percutaneous delivery of methotrexate-loaded nanoparticles enabling sustained anti-inflammatory effects in psoriasis therapy[J]. J. Mater. Chem. B. 12 (10), 2618–2627 (2024).
Xu, Y. et al. Single-dose of integrated bilayer microneedles for enhanced hypertrophic Scar therapy with rapid anti-inflammatory and sustained Inhibition of myofibroblasts[J]. Biomaterials 312, 122742 (2025).
Funding
This study was supported by the Yunnan Fundamental Research Projects (202201AS070079), the National Natural Science Foundation of China (82360447, 82560625), the First-Class Discipline Team of Kunming Medical University (2024XKTDYS01), the NHC Key Lab of Drug Addiction Medicine (Kunming Medical University) Open Projects Fund (KN202421), Yunnan health training project of high level talents (L-2025016), Yunnan Fundamental Research Projects (202501AU070010) and 2024 Yunnan Province Caiyun Postdoctoral Fellowship Project.
Author information
Authors and Affiliations
Contributions
Ting Wang : Writing – original draft, Project administration, Methodology, Formal analysis, Data curation, Conceptualization. Die Li : Writing – original draft, Methodology, Formal analysis, Data curation, Conceptualization. Haojie Bi : Methodology, Formal analysis, Data curation. Yi Liu : Formal analysis, Data curation. Xuan Xu : Project administration, Methodology. Hanying Wang : Project administration, Methodology. Qianwei Jin : Methodology, Data curation. Shaochun Chen : Writing – review & editing. Lechun Lyu : Writing – review & editing, Funding acquisition. Jingpei Shi : Writing – review & editing, Funding acquisition.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
All animal experiments in this study were performed in accordance with institutional guidelines and approved by the Ethical Review Committee for Animal Experiments of Kunming Medical University (KMMUX2025070048), This study was reported in accordance with the ARRIVE guidelines.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wang, T., Li, D., Bi, H. et al. A bilayered microneedle patch loaded with methotrexate and dexamethasone for transdermal treatment of psoriasis. Sci Rep 16, 7604 (2026). https://doi.org/10.1038/s41598-026-38216-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-38216-0
