
Abstract
Prior researchers have established the association between Health Human Resources (HHR) and children’s healthcare outcomes. However, there has been limited focus on the distribution of both professional and non-professional healthcare workers, as well as their impact on under-five mortality, in the context of environmental hygiene, along with the influence of maternal education as a moderator. Our research applied the data from the Pakistan Demographic and Health Survey (PDHS) 2018, having observations (N = 8022). The outcome comprises the risk of a child’s death before 0–59 months. A multivariate examination was conducted using Cox proportional hazards and regression models. The approximation of under-five deaths was achieved using generalized structural equation modeling (GSEM) and the 5000-bootstrap technique. A total of 4.09% of children died. The normal distribution of the healthcare workforce was professionals (83.34%), non-professionals (1.41%), and those who received no care (15.24%). The average maternal age and education are 29.55 and 4.52 years, respectively. The combined score for environmental hygiene was −0.00 (SD = 1.23). Multivariate regression results show that a one-unit increase in healthcare professional healthcare providers was associated with a 73% lower likelihood of under-five mortality (p < 0.01). Moreover, a one-unit increase in the number of professional healthcare providers was associated with a 30% increase in the likelihood of having a high environmental hygiene score (p < 0.001). The interaction of maternal education in the relationship between environmental hygiene and under-five mortality significantly contributes to the model’s predictive power, with 0.77 at (p < 0.001). Furthermore, professional healthcare providers were positively and significantly associated with under-five mortality (exp(β) = −0.178, 95% BCCI = −0.3585, −0.0017; P < 0.01). Additionally, a reduction in maternal education is associated with an increase in under-five deaths (exp(β) = 0.178, 95% BCCI: 0.0876, 0.2687; P < 0.001). Our findings suggest that environmental hygiene and maternal education play a critical role in reducing overall under-five deaths. Enhancing maternal and household head education, as well as improving environmental hygiene (access to clean water, toilets, and cooking fuel), will aid in addressing the issue of under-five mortality.
Similar content being viewed by others

Introduction
Over 90% of the seven million deaths of children under five take place in 40 nations, mainly concentrated in South Asian and sub-Saharan African countries (Black et al. 2010). Despite considerable development in the past few decades, child health outcomes remain a major issue worldwide, and few nations are on track to accomplish the Millennium Development Goals (MDGs) addressing maternal and under-five deaths (Goals four and five) (UNICEF, 2012; Victora et al. 2016).
In most developing and even developed countries, the standard of HRH is below the minimum required level to deliver effective healthcare services (World Health Organization 2006; Cometto et al. 2019). HRHs are more concentrated in economically developed areas, where they limit access to healthcare delivery to a particular population cluster (Cometto et al. 2019; Anand, 2010; Wiseman et al. 2017; Zhou et al. 2015; Nawaz et al. 2021). The distribution of the health workforce, particularly skilled professionals such as doctors, nurses, and midwives, may contribute to variations in under-five mortality. Prior literature demonstrates that improving the circulation and availability of qualified professionals is positively linked to better healthcare outcomes in children (Anand, Bärnighausen (2007); Li et al. 2021; Rana et al. 2018; Cometto et al. 2019). Nevertheless, limited research has been conducted on the relationship between the distribution of healthcare professionals and child healthcare outcomes, resulting in inconsistent findings on whether the number of healthcare providers results in reductions in infant and under-five mortality rates (Anand, 2010; Rana et al. 2018; Anand, Bärnighausen (2004); Sakai et al. 2016). While the quantity of healthcare providers is the fundamental factor in the health system, it is not enough to ensure access to healthcare services. Healthcare professionals must be distributed appropriately and accessible to the population to deliver quality care (Haakenstad et al. 2022; World Health Organization, 2015). The effective distribution of healthcare providers is essential for improving child healthcare outcomes. Despite this, evidence linking Professionals and non-professional healthcare providers to under-five deaths remains insufficient.
The disparity in the distribution of healthcare professionals remains a significant barrier to healthcare access for children worldwide. Pakistan is among those countries that face the challenge of unequal distribution of healthcare providers. Pakistan faces geographical variations in the availability of local healthcare providers (Nawaz et al. 2021). Studies from Pakistan have illustrated that the province of Sindh has a higher number of doctors compared to Khyber Pakhtunkhwa (KPK), whereas KPK has a greater number of nurses. The province of Punjab is also suffering from a lower number of nurses, hindering the accomplishment of SDGs (Nishtar et al. 2013). Moreover, in Pakistan, around 32,879 medical doctors graduate each year, and 40% of them decide to migrate to foreign countries to pursue superior opportunities due to low income, extended duty hours, and inadequate distribution (Nadir et al. 2023). These aspects collectively contribute to the reasons affecting child healthcare outcomes in Pakistan.
Globally, children are broadly recognized as a nation’s future workforce (Allen, Martinez (2005)). Therefore, ensuring the better health of the children is essential for the progress of any country. Despite substantial innovations in medical technology and healthcare systems, many countries continue to face challenges in reducing child mortality and morbidity rates, as published by the Government of Pakistan (2020). Researchers, policymakers, and humanitarians have emphasized the importance of quality of life and its impact on human health, which is directly related to child mortality (Brinda et al. 2015). Among the top ten predictors, five were associated with child mortality characteristics, including the household atmosphere, the household wealth index score, the type of fuel used for cooking and sanitary services, and the availability of cooling and drinking water (Fink et al. 2011; Headey, Palloni (2019)). Since the early twentieth century, environmental hygiene (water source, toilet, and cooking fuel) has been a public health priority, particularly concerning the health of infants and young children (Hutton, Chase (2018)). According to the World Health Organization (WHO) and United Nations Children’s Fund (UNICEF), inadequate water and poor hygiene or sanitation are likely key factors contributing to maternal and child mortality, as they can lead to direct or indirect health risks (Headey, Palloni (2019)). Global estimates indicate that sepsis is responsible for 8.5% of all maternal and child deaths (WHO/UNICEF Joint Water Supply, Sanitation Monitoring Program (2014); Bain et al. 2018). Recent estimates suggest that contaminated water, inadequate hygiene, and insufficient sanitation practices contribute to 50% of malnutrition, alongside regular cases of diarrhea or intestinal worm infections (Nadeem et al. 2024). The absence of hygiene results in numerous health risks, particularly for children, including parasitic illnesses like diarrhea and severe respiratory infections, which become the main reason for death in children under 5 years (Shrestha et al. 2020; Villavicencio et al. 2024). These illnesses can lead to additional complications such as anemia, respiratory infections, stunted physical growth, and impaired cognitive development, ultimately contributing to under-five mortality (Or et al. 2020; Brooker et al. 2008).
Wood smoke exposure in infants, due to poor ventilation, increases the risk of asthma, respiratory infections, and allergies. In rural areas, where over 2.3 billion individuals rely on biomass fuels for cooking, inadequate waste management contributes to child mortality (World Health Organization, 2014; Bradley, Putnick (2012)). Less than half of the rural population has access to proper hygiene services (World Health Organization, United Nations Children’s Fund (2021)).
According to a report by UNICEF (2016), around 53,000 children under 5 years die yearly from diarrhea, dirty water, and deprived hygiene. According to an estimate, 70% of families currently consume contaminated water, and around 25 million individuals continue to practice open defecation. Moreover, Cooper (2018) found that only 60% of the population can use soap and water for washing their hands. Furthermore, 57.6% of children in Pakistan face higher hazards due to inadequate environmental hygiene (Murtaza et al. 2021).
Herd et al. (2007) propose that maternal education is vital to improving child healthcare outcomes. Studies have also shown that mothers with advanced education tend to have more information and are more concerned about their children’s health (Pawlinska-Chmara, Wronka (2007)). Additionally, the higher educational levels of both parents were associated with a lower likelihood of their children developing diseases, infections, and malnutrition (Mooi-Reci, Wooden (2022)). Under-five mortality is twice as high in those children whose parents, especially mothers, have no formal schooling (112/1000 live births) as compared to those mothers who have secondary-level education (57/1000 live births). Moreover, according to Liu et al. (2015), child mortality is three times greater compared to that of children whose mothers are educated beyond the secondary level (36/1000 childbirths).
Pakistan currently ranks 25th out of 225 nations, based on child mortality statistics (Brinda et al. 2015). However, child mortality has decreased from 141/1000 to 67.4/1000 live births between 1990 and 2019, respectively (UNICEF, 2019). The progress remains slower than the target fixed for achieving the MDGs, which aim to minimize child deaths to 46/1000 live births by 2030 (Brinda et al. 2015; Bhutta et al. 2013). As per recent estimates, 26% of pneumonia and 27% of diarrhea are the primary causes of child mortality and are closely related to lack of resources, undernutrition, and deprived hygiene and sanitation (Bhutta et al. 2013; National Institute of Population Studies, 2018). Compared to maternal deaths, under-five deaths also have rural and urban disparities. According to Bhutta et al. 2013, deaths under the age of five are 2.5 times greater (118/1000 live births) in poor households than in wealthier households (49/1000). Additionally, the deaths of children less than 5 years old are on the upper side in Baluchistan (112/1000) than in Khyber Pakhtunkhwa (71/1000).
The relationship between the distribution of healthcare professionals and under-five deaths has not been well examined within the Pakistani context. Firstly, there are limited studies investigating the association between the health workforce and child health outcomes. Existing studies have considered access to clean water and sanitation as determinants of children’s well-being indicators. Secondly, prior researchers did not examine the association between both professional and non-professional healthcare provider distribution and under-five deaths. Finally, based on available information, previous researchers have not explored environmental hygiene as a mediator and maternal education as a moderator in relation to healthcare provider distribution and under-five mortality. Moreover, environmental hygiene and maternal education are important predictors, as the current study applies the population-attributable function to assess their roles in preventing under-five mortality. Therefore, this research aims to inspect the healthcare provider distribution effects on under-five deaths in Pakistan. Precisely, using the Pakistan DHS 2018 and GSEM, our objectives are to (a) examine the relationship between healthcare professional distribution and under-five deaths, (b) explore how the environmental hygiene index intervenes in the association between healthcare professional distribution and under-five deaths, and finally (c) to investigate how maternal education moderates this association. The results of the current research would be beneficial for developing strategies and plans to enhance healthcare professional accessibility, improve environmental hygiene, and promote maternal education, ultimately contributing to a reduction in child death rates under five years of age.
Theoretical perspective
Under-five years of death remains a most important worldwide health issue, particularly in underdeveloped nations (Aheto (2019); Sarkodie, 2021; Sharrow et al. 2022). A contributing factor to this problem is environmental hygiene (including water sources, sanitation, and cooking fuel), which causes infectious diseases and breathing problems (Nadeem et al. 2024; Shrestha et al. 2020; Villavicencio et al. 2024). This research examines the association among healthcare professional distribution and under-five mortality, focusing on environmental hygiene as a mediator and maternal education as a moderator while controlling for covariates. The current research framework is also guided by key theories that help explain the relationship between healthcare providers and under-five mortality.
The theory of Social Determinants of Health (SDH) emphasizes that healthcare results are influenced by a variety of societal, economic, and environmental variables (Watt, 2002; Thimm-Kaiser et al. 2023). In current research, the environmental factors associated with water sources, toilets, and cooking fuels used by households are considered important. Pure water, proper cleanliness, and adequate sanitation practices help reduce diarrhea and related worm infections, ultimately preventing malnutrition in children (Nadeem et al. 2024; Shrestha et al. 2020; Villavicencio et al. 2024). Similarly, using clean cooking fuel results in less pollution compared to solid fuels such as wood, charcoal, or dung cakes (Or et al. 2020; Yang et al. 2024; Puzzolo et al., (2016)). This pollution reduction can lead to fewer respiratory infections and a decrease in under-five mortality rates. Additionally, factors such as wealth, maternal education, the accessibility and availability of healthcare providers, and the quality of healthcare services significantly contribute to minimizing under-five mortality (Akinyemi et al., (2015); Adedini et al., (2015); Adebowale et al. 2012; Franics, Olalere (2014); Ezeh et al., (2015)).
The Health Belief Model (HBM) enlightens how public views and attitudes affect their well-being (Snetselaar, Delahanty (2017)). In the present research, maternal education is associated with more informed healthcare decisions regarding access to clean water, adherence to adequate hygiene practices, and the use of cleaner cooking fuels. Educated mothers can identify the well-being hazards associated with unclean water, poor hygiene practices, and dirty cooking fuels, as well as their benefits (Nadeem et al. 2024; Shrestha et al. 2020; Villavicencio et al. 2024; Or et al. 2020; Gould et al. 2020). This knowledge can enhance environmental hygiene and improve child health outcomes. The HBM also suggests that factors, such as the cost or availability of clean water and fuel can influence choices, which are affected by household socio-economic status (Haider et al. 2024).
Elder (1998) proposed that the Life Course Theory focuses on how early life experiences impact long-term health outcomes. Exposure to unclean water, poor hygiene, inadequate sanitation, and impurities in cooking fuel, such as dung cakes, during early childhood has a detrimental effect on health and increases the risk of death before the age of five (Liang et al. 2020). The Life Course Theory emphasizes the importance of timely policies and programs, such as promoting proper environmental hygiene, to improve children’s healthcare outcomes over time.
Using these theories together creates a strong foundation for the present research, connecting healthcare providers, environmental hygiene, and maternal education to under-five mortality. Additional variables, such as socio-economic status and access to healthcare services, influence environmental hygiene choices and their relationship with under-five mortality rates. This research explores these relationships to develop effective strategies for reducing under-five mortality and improving child health.
Methodology and process
This research derived data from the 2018 Pakistan Demographic and Health Survey (PDHS). The DHS is a nationwide representative survey using multistage sampling, gathered after five years across various nations. Our research used the data from the fifth wave of PDHS, which took place from November 2017 to 30th April 2018. The 2018 PDHS was initiated by the National Institute of Population Studies (NIPS) with support from the United States Agency for International Development (USAID) (National Institute of Population Studies, 2018). The survey employed a two-stage stratified sampling method across the four provinces, Islamabad, and FATA, categorizing regions as either urban or rural. Females between the ages of 15–49 in households were invited to participate in the interviews. Additional details regarding the survey and the data collection process are presented in the concluding document (National Population Health Survey, 2018).
Sample selection
The analysis focused on children born five years prior to the 2018 Pakistan DHS. This study population consisted of children with comprehensive information on survival status and mothers who resided with partners. The total number of births was 12708. Mothers’ previous marriages and their children were excluded, as past marriages affect their current marriage. This survey also collected environmental hygiene index information only for the most recent child, so our investigation was additionally limited to the last-born child. Around 265 twin births were recorded in the survey, which was subsequently reduced to a final sample of 8022. Missing data for key variables was minimal, with a maximum of 3.4%. The process used for selecting the sample is illustrated in Fig. 1.
Measurement of variables
Dependent variable
The outcome of the current research is the risk of under-five deaths. For the women’s questionnaires, the defendants were asked to provide information on how many children they had had in the past five years and how many of those children had survived. If a child had died, the interviewers asked for the age of the child when he died. The children’s survival status and their age (or age at death) were used as the dependent variable for the current investigation. Children who died were counted as cases, while those who were alive at the time of the interview were considered right-censored.
Independent variable
The independent variable in this analysis was the type of healthcare providers (Professionals and non-professionals). The defendants who received medical attention from non-professionals (pharmacists/chemists, traditional healthcare providers, etc.) were categorized as non-professionals = 0. In contrast, the defendants who acquired medical attention from trained professionals (Doctors, Nurses, and Midwives) were classified as professionals = 1 (Nawaz et al. 2021; Stephens et al. 2013). To enable a strong examination, non-professionals = 0 were designated as a baseline group.
Mediating variable
Environmental hygiene acts as the mediator in the current analysis. A composite index was created that includes three components of environmental hygiene. 1) water source, 2) toilet, 3) cooking fuel. The present selection highlights environmental hygiene in relation to under-five mortality. We first standardized the three variables to create the composite index, with each variable assessed using distinct scales. Moreover, we utilized principal component analysis (PCA) to merge them into a single composite index
Moderating variable
We used maternal education as a moderator for the current analysis, operationalized as a continuous variable.
Covariates
Various indicators at the children, maternal, home-based, and community levels, designated as determining factors of under-five deaths, were comprised as control variables (Akinyemi et al., (2015); Adedini et al., (2015); Adebowale et al. 2012; Franics, Olalere (2014); Ezeh et al., (2015)). At the child level, factors, such as the child’s sex, weight at birth, and birth type were considered. Factors related to the maternal level are the age of the mother in years, the mother’s employment in the previous year (binary), the number of children born (Continuous), and media exposure with categories of 0 = None, 1 = Less than once, and 2 = Once a week. Domestic variables were chosen, including the schooling of the husband, wealth index, remoteness of medical facilities (big issue = 0, not a big issue = 1), and the type of water to drink, which was categorized as follows: (0 = unimproved water, 1 = improved water). Furthermore, communal-level variables encompassed the place of residence, categorized as rural (Rural = 2) or urban (Urban = 1). The variable’s coding, as well as its description, is presented in Table 1.
Analytical strategy
Descriptive statistics were used to characterize the analysis. This includes percentages with weights to adjust for sampling bias (like over- and undersampling), along with means and standard deviations.
Multivariate analysis
Bivariate regression analysis was used to identify the variables that influence the mediator and outcome variables. Only variables with a t-statistic falling outside the range of +2 and ˗2, or those having a p-value below 0.1, were encompassed in the generalized structural equation model (GSEM) for further investigation. According to standard practice, predictor variables with t-statistics above 2 or below −2 are considered to significantly influence the dependent variable (Linden et al., 2021).
Using the Weibull proportional hazard models, we applied Seemingly Unrelated Regression (SUR) analysis to define the relationship between healthcare providers, environmental hygiene, and under-five deaths, after adjusting the control variables only. The SUR analysis is a traditional generalized regression model that offers the advantage of uncovering hidden associations between multiple variables and potentially revealing mediating and moderating effects.
The investigation contains four models. The model one depicts the regression of healthcare providers (independent variable) on the dependent variable (under-five deaths), after adjusting for the control factors. Model two predicts healthcare providers (independent variable) on environmental hygiene (mediator variable). Model three regressed the healthcare providers (independent variable) and the environmental hygiene (mediator variable) on the independent variable. The Weibull log function was used for the survival outcome, while the Gaussian identity function was employed for the environmental hygiene (mediator variable).
Moderation-mediation analysis
We executed the moderation-mediation analysis using GSEM and bootstrap techniques to examine the different paths of the relationship. The GSEM was adopted because it offers the advantage of analyzing path associations and can model different variables. The bootstrap technique, with 5,000 samplings, was also adopted because it has higher statistical power and can help avoid Type I errors (Hayes et al. 2012; Preacher et al. 2007). Given that other analytical tests assume a standard distribution, bias-corrected bootstrap confidence intervals (BCCI) are utilized to measure the statistical influence of intermediary relationship due to their non-symmetric assumptions. Estimations are generally regarded as methodologically sound when the BCCI does not contain a zero (Valente et al. 2020; MacKinnon et al. 2004).
Built based on the characteristics of the factors, the (Gaussian identity) function for the mediating variable and the (Weibull logit) function family of independent variable indicated a survival measure. Since the estimation effect on the dependent variable was a survival measure, the coefficients were reported as exponential.
Let Y symbolize under-five deaths, X represent healthcare professionals, M signify environmental hygiene, and W represent maternal education. Figure 2 illustrates the statistical analytical diagram.

Flow chart of the sample selection process.
Focused on Fig. 2 of the moderation-meditation outcomes of X on Y, the design of the track M is written as:
Where a represents the estimate from X to M, b describes the estimates from M to Y, and \(b2\) represents the moderating effect of W on Y. The Weibull hazard function can be written as
Where p describes the shape of the parameter, which is greater than zero. When p > 1, the hazard function rises over time. Whereas, when p < 1, it declines over time. However, when p = 1, the hazard function remains constant, and the Weibull model simplifies to an exponential distribution, as proposed by Allen (1997) and Hayes et al. 2012).
where \({\rm{\lambda }}\)
Then, the hazard ratio (HR)
Results
Overview of the sample investigated
The characteristics of the inspected sample are outlined in Table 2. Around 4.09% of children have died during the first five years of their birth. The survey found that children born alive were predominantly males (52.08%) and females (47.92%). The average maternal age was 29.55%, with an SD of 6.4 years. The average maternal education is 4.52 with an SD of 5.3 years. Additionally, the survey gathered information from 54.82% rural and 45.18% urban populations. The mean family wealth index was stated as -0.09 with an SD of 0.98. These results found that most households in the sample were poor. Healthcare professionals were categorized into three groups: professionals (83.34%), non-professionals (1.41%), and no care taken (15.24%). The combined mean environmental hygiene score was -0.00 with an SD of 1.23.
Bivariate regression examination
Table 3 shows the results of the bivariate regression. Our results indicate that children’s sex is not significantly related to under-five mortality (p > 0.1). The mother’s age (in years) was not associated with environmental hygiene (p > 0.1). Additionally, the sex of the child has not been linked to the mediating variable of environmental hygiene (p > 0.1). The t-statistics for the variables also did not exceed the ±2 range. Therefore, these variables were excluded from the multivariate SUR regression analysis. Before the analysis, a multicollinearity test was performed to identify potential issues. The test showed no problems, as all variance inflation factors (VIF) were below 5, with a mean VIF value of 1.58.
Multivariate Regression Analysis
The outcomes of the multivariate analysis are described in Table 4. Model one explains the outcomes, demonstrating a statistically significant relationship. The hazard ratios suggest that a unit increase in healthcare professionals’ distribution compared to non-professionals is associated with a nearly 73% decrease in the probability of under-five deaths (p < 0.05). In Model 2, when healthcare professionals were analyzed in terms of environmental hygiene, the mediator variable was included. Our study outcomes discovered a significant positive relationship between healthcare professionals and environmental hygiene. Specifically, an increase in one unit of healthcare professionals leads to a 30% increase in environmental hygiene scores (p < 0.05) when compared with non-professionals.
Furthermore, in Model 3, the distribution of healthcare professionals and environmental hygiene was investigated in relation to under-five deaths. The hazard proportion for the relationship among healthcare professionals and under-five deaths decreased in magnitude compared with Model 1. Additionally, although the relationship between environmental hygiene and under-five mortality is positive and significant, the hazard ratio illustrates that a unit increase in healthcare professionals, compared to non-professionals, reduces under-five mortality by 75% (p < 0.05). Finally, in model 4, we run the overall model by including maternal education as a moderator. The interaction of maternal education in the relationship between environmental hygiene and under-five mortality significantly contributes to the model’s predictive ability, with 0.77 at (p < 0.001). The likelihood-ratio test information emphasized that Model four will offer a more accurate fit compared to Model one, Chi2 (4) = 219.10 (p < 0.001).
Considering the observations mentioned earlier, it was observed that there may be a possible case of a moderated-mediation association among healthcare professionals and under-five mortality through environmental hygiene and maternal education. Nevertheless, it still tolerates the weight for further examination.
Decomposition of the coefficient magnitude
The decomposition of the coefficient magnitude of the relationship was achieved through 5000 bootstrap repetitions, along with a 95% bias-corrected bootstrap confidence interval (BCCI), where each path was estimated while holding all other variables constant, as shown in Table 5. The effect sizes are generally considered significant if the bias-corrected bootstrap confidence interval (BCCI) does not include 0 (Allen, 1997; Hayes et al. 2012). The findings indicate that the path from healthcare providers to under-five mortality is statistically significant (p < 0.01). The exponential coefficient, which represents the hazard proportion, suggests that a one-unit increase in healthcare professionals is associated with a reduced likelihood of under-five mortality. These results imply that the connection between healthcare professionals and under-five deaths may be evident in three patterns: direct, mediated, and moderated mediation. The direct relationship was statistically significant, with an exponential coefficient exp(β) = -0.178 and a 95% bias-corrected bootstrap confidence interval [BCCI = −0.3585, −0.0017]. The coefficient for the mediation path is minimal, indicating that a one-unit increase in healthcare professionals, compared to non-professionals, has a minimal effect on under-five mortality (exp(β) = 0.005). However, the moderation-mediation analysis suggests that maternal education is linked with a decrease in under-five mortality, with an effect size of exp(β) = 0.002.
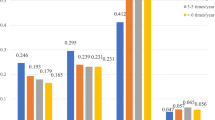
Table 5 also presents the prediction of effect sizes based on the BBCIs. The results indicated that maternal education has varying effects on under-five mortality depending on its level. At one standard deviation below the mean (Mean - 1 SD), the predicted value is 0.178 (SE = 0.0463, BBCI [0.0876, 0.2687]), which is statistically significant at (P < 0.001). At the mean level, the predicted value is 0.070 (SE = 0.0414, BBCI [-0.0106, 0.1517]), showing a marginally significant effect (P = 0.089). However, at one standard deviation above the mean (mean +1 SD), the predicted value is -0.037 (SE = 0.0754, BBCI [-0.1849, 0.1107]), which is not statistically significant (P = 0.623). These results suggest that maternal education is significantly associated with lower levels, but this association weakens and becomes statistically insignificant at higher levels. Additionally, Fig. 3 shows the estimation of the path coefficient derived from 5000 bootstrap repetitions in the mediation analysis involving healthcare professionals and under-five deaths.

This conceptual model illustrates the moderated-mediation association among healthcare professionals and under-five mortality.
Discussion
The current study utilized data from the 2018 Pakistan DHS survey to investigate the association among the distribution of healthcare professionals and under-five mortality, aiming to understand the fauna of this relationship. The current research also examined the patterns in the relationship between healthcare professionals by analyzing and decomposing the structure of association by using environmental hygiene as a mediator and maternal education as a moderator. The outcomes from the moderation-mediation analysis were conducted using a bootstrap technique with 5000 repetitions.

Framework for the estimation of the path coefficient from 5000 bootstrap repetitions of the moderated-mediation relationship between healthcare professionals and under-five mortality.
The results demonstrate a significant relationship between healthcare professionals and under-five death rates compared to those of non-professionals. Furthermore, when healthcare professionals were regressed on environmental hygiene, the mediator variable was taken into consideration. Our study’s outcomes revealed a positive and significant relationship between healthcare professionals and the environmental hygiene index, compared to non-professionals.
In addition, healthcare provider distribution and environmental hygiene were regressed on under-five mortality. We also found a positive and significant connection between healthcare professionals and under-five deaths compared to non-professionals. These results are concurrent with studies of (Adjiwanou, Engdaw (2017); Sheikh et al. 2021; Liang et al. 2019; Sutarto et al. 2024). Finally, the overall model includes maternal education as a moderator. The interaction between maternal education and environmental hygiene significantly contributes to the model’s predictive ability in the relationship with under-five mortality. Considering the observations mentioned above, it is suggested that there may be a possible association between the mediation and moderation of healthcare professionals and under-five mortality through environmental hygiene. Nevertheless, it still tolerates the weight for further examination. These outcomes of our research showed similarities with those of (Nadeem et al. 2024) and Yemane (2022), which confirmed that children whose household head has less education have higher rates of under-five mortality.
Likewise, our findings also revealed that the direct relationship among between healthcare professionals and under-five deaths compared to non-professionals was statistically significant, with an exponential coefficient of exp(β) = −0.178 and a 95% bias-corrected bootstrap confidence interval [BCCI = −0.3585, −0.0017]. The coefficient for the non-conditional indirect (mediation) path is minimal, indicating that an increment of one unit in healthcare professionals, compared to non-professionals, has a minimal effect on the risk of under-five deaths (exp(β) = 0.005). The outcomes of our research were consistent with existing research, which demonstrated that household well-being hazards were linked to higher child mortality in nine out of 12 countries; however, this association was only observed in four countries after adjustment. However, when considering age and household health hazards together, higher household well-being risks are connected to greater deaths between 24 and 59 months in eight countries (Adjiwanou, Engdaw (2017)). Another study illustrated that improved hygiene and sanitation are linked to better child health in Cameroon, with maternal education, father age, and urban residence being key factors for environmental hygiene (Tambi, Atemnkeng (2018)). A systematic review and meta-analysis illustrated that environmental hygiene interventions were linked to a 17% decrease in the probabilities of all causes of under-five mortality (OR = 0.55, 95% CI = 0.35,0.48), and a 45% decrease in diarrheal deaths (OR = 0.56, 95% CI = 0.35,0.48) across 38 and 10 interventions, respectively (Sharma Waddington et al., (2023)).
Finally, our results indicate that maternal education has varying effects on under-five mortality depending on its level. At one standard deviation below the mean (Mean -1SD), the predicted value is 0.178 (SE = 0.0463, BBCI [0.0876, 0.2687]), which is statistically significant at (P < 0.001). At the mean level, the predicted value is 0.070 (SE = 0.0414, BBCI [−0.0106, 0.1517]), showing a marginally significant effect (P = 0.089). However, at one standard deviation above the mean (mean +1 SD), the predicted value is −0.037 (SE = 0.0754, BBCI [−0.1849, 0.1107]), which is not statistically significant (P = 0.623). These findings suggest diminishing returns, where the effect of maternal education on under-five mortality decreases at higher levels, potentially due to the influence of other factors, such as socio-economic status or healthcare access. These findings are consistent with those of Wu (2022), which demonstrated that maternal education decreases under-five deaths through factors, such as wealth index, health literacy, and knowledge, but not through the mother’s employment. Another study of Nguyen-Phung (2023) and (Mandal et al. 2021) from Vietnam revealed that a decrease in one year of mother education increased newborn death, infant, and under-five deaths by around 2.4, 3.0, and 3.4%, respectively.
The current research outcomes emphasize the importance of equitably distributing healthcare providers in Pakistan, particularly in underdeveloped and remote areas, to reduce under-five mortality rates. Policies and program initiatives should focus on achieving “Health for All” and improving female education, consistent with the 4th SDG. Enhancing maternal and household head education, increasing household wealth, and improving environmental hygiene (access to clean water, toilets, and cooking fuel) are the critical factors in reducing under-five mortality. Additionally, raising public awareness campaigns regarding the effects of maternal age, education, and household environmental hygiene is vital for reducing child deaths and enhancing both mother and child health outcomes in Pakistan.
Limitations and strengths
Using PDHS data provides valuable insights into the association between healthcare providers, environmental hygiene, maternal education, and under-five mortality; several limitations must be considered. The use of cross-sectional data limits the ability to establish connections, and potential recall bias in self-reported information may impact data accuracy. However, this study employed statistical techniques to minimize this, such as those related to discriminating validity. Another significant limitation is that the data is collected from a single country, namely Pakistan, and from only one sector, specifically the healthcare sector, which is part of the service sector. To generalize results, future studies should collect data more than once. In addition, future studies should also focus on using other probability sampling techniques to collect data. It is also proposed that future studies consider qualitative methods, such as interviews, which can be conducted with policymakers, Directors of Health, and District Health Officers (DHOs) to validate the concept of this study. It is also proposed that future studies collect data using the same variables from other countries to gain a deeper understanding and enhance the generalizability of current research.
Conclusions
The current research highlights the significant influence of healthcare professionals and environmental hygiene, maternal education, on influencing under-five mortality in Pakistan. Our findings suggest that the equitable distribution of healthcare providers, enhanced environmental hygiene (including access to water, toilets, and cooking fuel), and improved maternal education are crucial for reducing under-five mortality. While maternal education is a key factor, its impact diminishes with higher levels of education, underscoring the importance of addressing basic education for women. The mediating role of environmental hygiene further emphasizes the need for infrastructure improvements to promote child healthcare outcomes. To effectively minimize under-five mortality, strategies and interventions should focus on improving healthcare access, expanding free maternal and child healthcare services, empowering women through education, and enhancing household environments, particularly in underdeveloped and remote regions.
Data availability
The datasets used for analysis and to reach the conclusions of this study are available online at MEASURE DHS (https://www.dhsprogram.com/data/available-datasets.cfm). They are released upon request and subject to approval. Additionally, direct access to the specific raw and curated datasets used in this research can be obtained through the following secure link (https://drive.google.com/file/d/1Zt-cw5DkjhatZbVOVPu0a8w9BbpomXcu/view?usp=drive_link). This link provides access to the exact datasets analyzed in the current study, ensuring transparency and reproducibility.
References
Adebowale AS, Yusuf BO, Fagbamigbe AF (2012) Survival probability and predictors for woman experience childhood death in Nigeria: analysis of north–south differentials. BMC Public Health 12:430
Adedini SA, Odimegwu C, Imasiku EN et al. (2015) Regional variations in infant and child mortality in Nigeria: a multilevel analysis. J Biosoc Sci 47:165–187
Adjiwanou V, Engdaw AW (2017) Household environmental health hazards’ effect on under-five mortality in sub-Saharan Africa: what can we learn from the Demographic and Health Survey? Glob Public Health 12:780–794
Aheto JM (2019) Predictive model and determinants of under-five child mortality: evidence from the 2014 Ghana demographic and health survey. BMC Public Health 19:64
Akinyemi JO, Bamgboye EA, Ayeni O (2015) Trends in neonatal mortality in Nigeria and effects of bio-demographic and maternal characteristics. BMC Pediatr 15:36
Allen M, Martinez S (2005) The politics of children’s issues: challenges and opportunities for advancing a children’s agenda. In: Applied Developmental Science: An Advanced Textbook, pp 325
Allen MP (1997) Understanding regression analysis. Springer US, Boston, MA
Anand S (2010) Measuring health workforce inequalities: methods and application to China and India. World Health Organization, Geneva
Anand S, Bärnighausen T (2004) Human resources and health outcomes: cross-country econometric study. Lancet 364(9445):1603–1609
Anand S, Bärnighausen T (2007) Health workers and vaccination coverage in developing countries: an econometric analysis. Lancet 369(9569):1277–1285
Bain R, Johnston R, Mitis F, Chatterley C, Slaymaker T (2018) Establishing sustainable development goal baselines for household drinking water, sanitation and hygiene services. Water 10(12):1711
Bhutta ZA, Hafeez A, Rizvi A et al. (2013) Reproductive, maternal, newborn, and child health in Pakistan: challenges and opportunities. Lancet 381:2207–2218
Black RE, Cousens S, Johnson HL et al. (2010) Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet 375:1969–1987
Bradley RH, Putnick DL (2012) Housing quality and access to material and learning resources within the home environment in developing countries. Child Dev 83(1):76–91
Brinda EM, Rajkumar AP, Enemark U (2015) Association between gender inequality index and child mortality rates: a cross-national study of 138 countries. BMC Public Health 15(1):97
Brooker S, Hotez PJ, Bundy DA (2008) Hookworm-related anaemia among pregnant women: a systematic review. PLoS Negl Trop Dis 2(9):e291
Cometto G, Buchan J, Dussault G (2019) Developing the health workforce for universal health coverage. Bull World Health Organ 98(2):109
Cometto G, Buchan J, Dussault G (2019) Developing the health workforce for universal health coverage. Bull World Health Or gan 98(2):109
Cooper R (2018) Water management/governance systems in Pakistan. K4D Helpdesk Report
Elder Jr GH (1998) The life course as developmental theory. Child Dev 69:1–2
Ezeh OK, Agho KE, Dibley MJ et al. (2015) Risk factors for postneonatal, infant, child and under-5 mortality in Nigeria: a pooled cross-sectional analysis. BMJ Open 5:e006779
Fink G, Günther I, Hill K (2011) The effect of water and sanitation on child health: evidence from the demographic and health surveys 1986–2007. Int J Epidemiol 40(5):1196–1204
Franics FA, Olalere A (2014) Differentials and correlates of infants mortality in Nigeria: a comparative survival analysis between North East and South West Nigeria. Int J Trop Dis Health 4(8):869–886
Gould CF, Urpelainen J, Sais JH (2020) The role of education and attitudes in cooking fuel choice: evidence from two states in India. Energy Sustain Dev 54:36–50
Government of Pakistan (2020) Economic Survey of Pakistan 2019–2020. Islamabad: Ministry of Finance
Haakenstad A, Irvine CM, Knight M et al. (2022) Measuring the availability of human resources for health and its relationship to universal health coverage for 204 countries and territories from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 399:2129–2154
Haider S, Mahapatra B, Mohammad S et al. (2024) Understanding the socioeconomic determinants of cooking fuel expenditure in Uttar Pradesh, India. Discov Sustain 5:182
Hayes AF, Glynn CJ, Huge ME (2012) Cautions regarding the interpretation of regression coefficients and hypothesis tests in linear models with interactions. Commun Methods Meas 6:1–1
Headey D, Palloni G (2019) Water, sanitation, and child health: evidence from subnational panel data in 59 countries. Demography 56(2):729–752
Herd P, Goesling B, House JS (2007) Socioeconomic position and health: the differential effects of education versus income on the onset versus progression of health problems. J Health Soc Behav 48(3):223–238
Hutton G, Chase C (2018) Water supply, sanitation, and hygiene
Li X, Mukandavire C, Cucunubá ZM et al. (2021) Estimating the health impact of vaccination against ten pathogens in 98 low-income and middle-income countries from 2000 to 2030: a modelling study. Lancet 397:398–408
Liang S, Macinko J, Yue D et al. (2019) The impact of the health care workforce on under-five mortality in rural China. Hum Resour Health 17:21
Liang W, Wang B, Shen G et al. (2020) Association of solid fuel use with risk of stunting in children living in China. Indoor Air 30:264–274
Linden A, Huber C, Wodtke GT (2021) A regression-with-residuals method for analyzing causal mediation: the rwrmed package. Stata J 21:559–574
Liu L, Oza S, Hogan D et al. (2015) Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet 385:430–440
MacKinnon DP, Lockwood CM, Williams J (2004) Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivar Behav Res 39:99–128
Mandal S, Paul P, Chouhan P (2021) Impact of maternal education on under-five mortality of children in India: insights from the National Family Health Survey, 2005–2006 and 2015–2016. Death Stud 45:788–794
Mooi-Reci I, Wooden M (2022) Jobless parents, unhealthy children? How past exposure to parental joblessness influences children’s future health. SSM Popul Health 19:101144
Murtaza F, Muzaffar M, Mustafa T, Anwer J (2021) Water and sanitation risk exposure in children under-five in Pakistan. J Fam Community Med 28(2):103–109
Nadeem M, Anwar M, Adil S et al. (2024) The association between water, sanitation, hygiene, and child underweight in Punjab, Pakistan: an application of population attributable fraction. J Multidiscip Health 17:2475–2487
Nadir F, Sardar H, Ahmad H (2023) Perceptions of medical students regarding brain drain and its effects on Pakistan’s socio-medical conditions: a cross-sectional study. Pak J Med Sci 39(2):401
National Institute of Population Studies, Macro International. Institute for Resource Development. Demographic, & Health Surveys (2018) Pakistan demographic and health survey. Islamabad: National Institute of Population Studies
National Population Health Survey (2017–18) National Institute of Population Studies
Nawaz R, Zhou Z, Khalid N et al. (2021) Income-related inequality in distribution of health human resources among districts of Pakistan. BMC Health Serv Res 21:142
Nguyen-Phung HT (2023) The impact of maternal education on child mortality: evidence from an increase tuition fee policy in Vietnam. Int J Educ Dev 96:102704
Nishtar S, Boerma T, Amjad S et al. (2013) Pakistan’s health system: performance and prospects after the 18th Constitutional Amendment. Lancet 381:2193–2206
Or PP, Wong BY, Chung JW (2020) To investigate the association between the health literacy and hand hygiene practices of the older adults to help them fight against infectious diseases in Hong Kong. Am J Infect Control 48(5):485–489
Pawlinska-Chmara R, Wronka I (2007) Assessment of the effect of socioeconomic factors on the prevalence of respiratory disorders in children. J Physiol Pharm 58(5):523–529
Preacher KJ, Rucker DD, Hayes AF (2007) Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivar Behav Res 42:185–227
Puzzolo E, Pope D, Stanistreet D et al. (2016) Clean fuels for resource-poor settings: a systematic review of barriers and enablers to adoption and sustained use. Environ Res 146:218–234
Rana RH, Alam K, Gow J (2018) Health expenditure, child and maternal mortality nexus: a comparative global analysis. BMC Int Health Hum Rights 18(1):29
Sakai R, Fink G, Kumamaru H, Kawachi I (2016) The impact of pediatrician supply on child health outcomes: longitudinal evidence from Japan. Health Serv Res 51(2):530–549
Sarkodie AO (2021) Factors influencing under-five mortality in rural-urban Ghana: an applied survival analysis. Soc Sci Med 284:114185
Sharma Waddington H, Masset E, Bick S et al. (2023) Impact on childhood mortality of interventions to improve drinking water, sanitation, and hygiene (WASH) to households: systematic review and meta-analysis. PLoS Med 20:e1004215
Sharrow D, Hug L, You D et al. (2022) Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet Glob Health 10:e195–e206
Sheikh W, Ahmed MB, Parulkar A et al. (2021) Association between the Hospital Readmissions Reduction Program and heart failure subtype readmissions and mortality in the USA. Cardiology 57:57
Shrestha SK, Vicendese D, Erbas B (2020) Water, sanitation and hygiene practices associated with improved height-for-age, weight-for-height and weight-for-age z-scores among under-five children in Nepal. BMC Pediatr 20(1):134
Snetselaar LG, Delahanty LM (2017) Nutrition intervention: lessons from clinical trials. In: Nutrition in the prevention and treatment of disease. Academic Press, pp 203–216
Stephens C, Crivelli V, Hautecouer J et al. (2013) Improving indigenous maternal and child health
Sutarto S, Puspitasari RD, Utama WT et al. (2024) The role of health services in improving the health status of children under five in Way Kanan District, Lampung Province. In: International Conference on Medical Science and Health (ICOMESH 2024). Atlantis Press, pp 215–242
Tambi MD, Atemnkeng JT (2018) Measuring the effect of environmental hygiene on child health outcomes in Cameroon. J Econ Manag 32:118–137
Thimm-Kaiser M, Benzekri A, Guilamo-Ramos V (2023) Conceptualizing the mechanisms of social determinants of health: a heuristic framework to inform future directions for mitigation. Milbank Q 101:486–526
UNICEF (2016) Strategy for water, sanitation and hygiene 2016–2030
UNICEF (2019) Committing to child survival: a promise renewed; progress report 2018. UNICEF, New York
Valente MJ, Rijnhart JJ, Smyth HL et al. (2020) Causal mediation programs in R, M plus, SAS, SPSS, and Stata. Struct Equ Modeling 27:975–984
Victora CG, Requejo JH, Barros AJ et al. (2016) Countdown to 2015: a decade of tracking progress for maternal, newborn, and child survival. Lancet 387:2049–2059
Villavicencio F, Perin J, Eilerts-Spinelli H et al. (2024) Global, regional, and national causes of death in children and adolescents younger than 20 years: an open data portal with estimates for 2000–21. Lancet Glob Health 12:e16–e17
Watt RG (2002) Emerging theories into the social determinants of health: implications for oral health promotion. Community Dent Oral Epidemiol 30:241–247
WHO/UNICEF Joint Water Supply, Sanitation Monitoring Programme (2014) Progress on drinking water and sanitation: 2014 update. World Health Organization, Geneva
Wiseman V, Lagarde M, Batura N et al. (2017) Measuring inequalities in the distribution of the Fiji health workforce. Int J Equity Health 16:115
World Health Organization (2006) The world health report 2006: working together for health. World Health Organization, Geneva
World Health Organization (2014) WHO guidelines for indoor air quality: household fuel combustion. World Health Organization, Geneva
World Health Organization (2015) Health workforce 2030: towards a global strategy on human resources for health. World Health Organization, Geneva
World Health Organization, UNICEF (2012) Building a future for women and children: the 2012 report. World Health Organization and UNICEF, Washington, DC
World Health Organization, United Nations Children’s Fund (2021) Progress on household drinking water, sanitation and hygiene 2000–2020: five years into the SDGs. World Health Organization, Geneva
Wu H (2022) The effect of maternal education on child mortality in Bangladesh. Popul Dev Rev 48:475–503
Yang R, He J, Zhong KK et al. (2024) Relationship of solid fuels use with cognitive function and efficacy of switching to cleaner fuels or using ventilation: a systematic review and meta-analysis. Environ Res 249:118314
Yemane GD (2022) The factors associated with under-five mortality in Ethiopia. Ann Med Surg 79:104063
Zhou K, Zhang X, Ding Y et al. (2015) Inequality trends of health workforce in different stages of medical system reform (1985–2011) in China. Hum Resour Health 13:94
Acknowledgements
The authors thank the Demographic and Health Surveys (DHS) for permission to utilize the Pakistan DHS data for the current research. This study was funded by the National Natural Science Foundation of China (Grant No. 72374169). However, the foundation was not involved in the research design or activities related to data collection, analysis, or manuscript writing.
Author information
Authors and Affiliations
Contributions
R.N.: Writing (Review & Editing, Original Draft), Visualization, Supervision, Software, Resources, Project Administration, Methodology, Investigation, Funding Acquisition, Formal Analysis, Data Curation, Conceptualization. N.K.: Review & Editing, Visualization, Software, Resources, Methodology, Investigation, Formal Analysis, Data Curation. Z.Z.: Writing (Review & Editing), Visualization, Supervision, Software, Resources, Investigation, Formal Analysis, Data Curation. S.G.: Review & Editing, Visualization, Supervision, Software, Resources, Project Administration, Methodology, Investigation, Funding Acquisition, Formal Analysis, Data Curation. M.F.A.: Investigation, Formal Analysis, Review & Editing. All authors have approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
Ethical considerations were strictly observed in this study, which is based on secondary data from the Pakistan Demographic and Health Survey (PDHS) 2017–18. The PDHS 2017–18 protocol was reviewed and approved by both the ICF Institutional Review Board (IRB) and the National Bioethics Committee (NBC) of the Pakistan Health Research Council. The ICF IRB approval (FWA00000845) was granted on October 19, 2017, and the NBC approval (Reference No. 4-87/NBC-285//17/1438) was granted on November 17, 2017. The ICF IRB ensured compliance with the U.S. Department of Health and Human Services regulations (45 CFR 46), while the NBC ensured adherence to national ethical standards. The study was conducted in accordance with the principles of the Declaration of Helsinki. Data collection for the PDHS 2017–18 occurred between November 22, 2017, and April 30, 2018. As this research involved secondary analysis of publicly available data, no additional ethical approval was required.
Informed consent
Prior to participation, informed consent was obtained from all respondents by the PDHS survey teams. Respondents were informed about the purpose of the study, the voluntary nature of their participation, procedures for maintaining confidentiality, and their right to withdraw at any stage without consequences. For minors, consent was obtained from a parent or legal guardian in addition to assent from the child when appropriate. All consent procedures were approved by the ICF IRB and the National Bioethics Committee of the Pakistan Health Research Council, in compliance with international and national ethical guidelines.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Nawaz, R., Khalid, N., Zhou, Z. et al. The relationship between healthcare professionals and under-five mortality: the mediating role of environmental hygiene and the moderating effect of maternal education. Humanit Soc Sci Commun 12, 1788 (2025). https://doi.org/10.1057/s41599-025-06037-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-025-06037-7
