
Abstract
IDH-mutant gliomas show prognostic heterogeneity despite favorable overall outcomes, necessitating refined molecular classification. While the extracellular matrix (ECM) critically regulates tumor progression, immunity, and EMT, its prognostic significance in IDH-mutant gliomas remains largely unexplored. Here, we employed unsupervised clustering of ECM-related genes across multiple glioma cohorts, identifying two distinct molecular subtypes: ECM1 and ECM2. ECM1 correlated with worse prognosis, characterized by heightened immune infiltration, elevated EMT activity, aggressive radiological features (peritumoral edema/necrosis), and enhanced proliferation, angiogenesis, stemness, and matrix remodeling capacities. A four-gene signature (CLCF1, COL11A1, CSPG5, and SULF1) robustly stratified patient risk in validation cohorts. Subtype-specific analyses revealed divergent metabolic pathways and predicted differential drug sensitivities, highlighting therapeutic opportunities. Our findings establish ECM-driven heterogeneity as a key determinant of IDH-mutant glioma behavior, offering a novel molecular taxonomy to guide precision oncology through targeted ECM-related biomarkers and therapies.
Similar content being viewed by others


Introduction
Gliomas are the most common malignant tumors of the central nervous system1. Despite advancements in molecular diagnostic technologies, the overall prognosis for patients remains poor, particularly for high-grade gliomas2. According to the 2021 WHO classification of central nervous system tumors, IDH-mutant gliomas exhibit distinct molecular characteristics3. Compared to IDH-wildtype gliomas, IDH-mutant gliomas grow more slowly and have relatively longer survival times2. However, some IDH-mutant gliomas undergo significant malignant progression during their clinical course, leading to treatment failure. Recent research has shown that the malignant progression of IDH-mutant gliomas is not solely dependent on genetic alterations but is also heavily influenced by the tumor microenvironment (TME)4, a complex system composed of tumor cells, immune cells, stromal cells, and the extracellular matrix (ECM). Among these components, the ECM has a particularly significant impact5.
The ECM serves not only as a structural scaffold for tumor tissues but also as a key regulator of cellular behavior and signaling pathways6 in tumors. Its dynamic remodeling affects cell migration, proliferation, differentiation, and the immune microenvironment, making it a critical driver of tumor invasion and metastasis7. Through interactions with integrins, glycoproteins (e.g., laminin), and proteases (e.g., MMPs) on tumor cells, the ECM directly influences tumor biology and further drives tumor progression toward malignancy8. Additionally, ECM heterogeneity is closely associated with therapeutic resistance, immune suppression, and epithelial-mesenchymal transition (EMT)9.
EMT, a process in which cells transition from a polarized epithelial phenotype to a migratory and invasive mesenchymal phenotype, is a key mechanism in tumor progression10. Different EMT stages (e.g., EPI, hybrid EMT [hEMT], and mesenchymal [MES]) reflect varying levels of tumor cell invasiveness11,12. The ECM plays a critical regulatory role in EMT, for instance, inducing EMT through classical signaling pathways such as TGF-β and Wnt, thereby promoting the transition from low-invasive to high-invasive phenotypes13. Despite its well-established role in other cancer types, the relationship between ECM and EMT in IDH-mutant gliomas remains unexplored, leaving a significant gap in understanding the regulatory mechanisms underlying their malignant progression.
In this study, we identified two ECM-based subtypes of IDH-mutant gliomas, ECM1 and ECM2, through unsupervised clustering analysis. ECM1 was associated with worse prognosis, higher expression of immune- and metabolism-related genes, and a strong correlation with the MES and hEMT states, reflecting higher invasiveness. In contrast, ECM2 was linked to better prognosis and predominantly correlated with the EPI state. These findings suggest that ECM plays a pivotal role in regulating EMT and driving malignant progression in IDH-mutant gliomas. This research not only enhances our understanding of the mechanisms underlying glioma progression but also provides a foundation for developing ECM-targeted therapeutic strategies to improve patient outcomes.
Results
Identification of consensus clustering ECM-based subgroups in IDH mutant gliomas
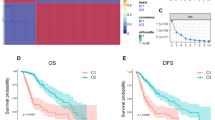
To elucidate the role of the ECM in IDH-mutant gliomas, we conducted unsupervised clustering analysis using 1026 ECM-related genes. The workflow of this analysis is illustrated in Fig. 1a. Initially, Cox regression analysis was performed on the CGGA 325 dataset (training cohort), CGGA 693, TCGA dataset, and GLASS dataset (validation cohort, Supplementary Fig. S1) to identify ECM-related genes significantly associated with overall survival (OS), resulting in the selection of 845 prognostic ECM-related genes. Consensus clustering based on the expression profiles of these genes stratified the tumors into two distinct molecular subtypes, termed ECM1 and ECM2, respectively (Fig. 1b, c). Notably, these subtypes exhibited significant differences in clinical characteristics, including WHO grades, 1p/19q co-deletion status, and MGMT promoter methylation, etc (Fig. 1d). Kaplan–Meier survival analysis demonstrated that patients in the ECM1 group had significantly worse OS compared to those in the ECM2 group (Fig. 1e). To investigate the potential mechanisms underlying this prognostic difference, we performed differential gene expression analysis between the two subtypes (Fig. 1f and Supplementary Fig. S2a, c, e). Subsequent pathway enrichment analysis of the differentially expressed genes (DEGs) revealed significant enrichment in pathways related to cell division and immune response (Fig. 1g and Supplementary Fig. S2b, d, f), suggesting that ECM heterogeneity may contribute to malignant progression through these biological processes.

a Flowchart of this study. b Consensus clustering of the ECM1 and ECM2 subtypes based on gene expression profiles, showing distinct clustering patterns. c Principal component analysis (PCA) of ECM1 and ECM2 subtypes, with 34.66% and 8.77% of the variance explained by PC1 and PC2, respectively. d Heatmap displaying gene expression patterns for ECM1 and ECM2 subtypes, with clinical features such as age, histology, tumor grade, gender, 1p/19q status, and MGMT promoter methylation status shown at the top. e Kaplan–Meier survival analysis comparing OS between ECM1 and ECM2 subtypes, with a significant difference (P < 0.0001), indicating worse prognosis for ECM1. f Volcano plot showing DEGs between ECM1 and ECM2 subtypes, with upregulated genes in ECM1 shown in red and downregulated genes in blue. g KEGG pathway analysis highlighting significantly enriched biological processes in ECM1 compared to ECM2, with the most enriched processes including cell division, immune response, and mitotic cell cycle.
Distinct somatic variations were divided between two ECM subgroups in IDH mutant gliomas
Genetic alterations such as TP53 mutations and CDKN2A/2B deletions are directly linked to poor prognosis in IDH-mutant gliomas, we therefore further analyzed somatic mutation profiles to investigate their association with ECM subtypes. Somatic mutation data from the CGGA 325 cohort were examined, and the distribution of key genetic alterations across ECM1 and ECM2 subtypes was assessed. The mutation landscape is presented in Fig. 2. Detailly speaking, the ECM1 subtype was significantly enriched for mutations and deletions commonly associated with aggressive tumor behavior, including TP53 mutations, co-deletions of CDKN2A and CDKN2B, NF1 mutations, and EGFR mutations (Fig. 2, left). In contrast, the ECM2 subtype exhibited a higher frequency of CIC and FUBP1 mutations, genetic alterations typically associated with more favorable clinical outcomes (Fig. 2, right). These findings suggest that distinct somatic alterations may contribute to the differential prognoses observed between ECM1 and ECM2 subtypes.

Mutation profiles of key genes in the ECM1 and ECM2 subtypes. On the left, ECM1 shows a higher frequency of mutations in IDH1 (94%), TP53 (64%), ATRX (52%), and CDKN2A (8%) compared to ECM2. The ECM2 subtype has a relatively lower mutation frequency, with IDH1 (94%) being the most frequent mutation, followed by TP53 (46%) and ATRX (42%). Mutation types are color-coded as follows: inframe mutations (putative driver) in red, missense mutations (putative driver) in green, inframe mutations (unknown significance) in light brown, missense mutations (unknown significance) in blue, splice mutations (putative driver) in orange, truncating mutations (putative driver) in purple, amplifications in dark green, and deep deletions in dark blue, red-labeled genes represent driver mutation, black-labeled genes represent passenger mutation. The bars next to each mutation denote the frequency of each mutation in the respective subtype.
Immune infiltration and metabolic variation of ECM subgroups in IDH mutant gliomas
Given the significant enrichment of immune-related pathways between ECM1 and ECM2 subtypes, we further investigated the differences in immune infiltration between these two groups. Using the ESTIMATE algorithm, we calculated the estimate score, immune score, stromal score, and tumor purity for both subtypes in the CGGA325 dataset. As shown in Fig. 3a, b, the ECM1 subtype exhibited significantly higher estimate, immune, and stromal scores compared to the ECM2 subtype, whereas tumor purity was markedly higher in the ECM2 group. To further dissect immune cell composition, CIBERSORT analysis revealed that ECM1 tumors were enriched in resting dendritic cells, M0, M1, and M2 macrophages, plasma cells, and CD8 + T cells (Fig. 3c). Conversely, the ECM2 subtype showed higher infiltration of activated mast cells, monocytes, resting NK cells, and naïve CD4 + T cells. Additionally, ssGSEA analysis demonstrated that the ECM1 subtype had elevated levels of most immune cell populations, including activated dendritic cells (aDCs), CD8 + T cells, dendritic cells (DCs), immature dendritic cells (iDCs), macrophages, mast cells, NK cells, plasmacytoid dendritic cells (pDCs), T helper cells, Th2 cells, tumor-infiltrating lymphocytes (TILs), and regulatory T cells (Tregs). In contrast, the ECM2 subtype was characterized by a significant increase in neutrophils and Th1 cells (Fig. 3d). In addition, types of regulatory mechanisms of the immune system and molecular interactions were almost markedly enriched in ECM1 subtype except the APC-co-inhibition (Fig. 3e). Moreover, the expression of immune checkpoint-related genes, such as CD160, CD200R1, CD27, CD274 (PD-L1), CD276, CD28, CD44, CD48, CD70, CD80, and CD86, were significantly upregulated in the ECM1 group (Fig. 3f). To validate these findings, we analyzed the CGGA693 dataset and TCGA cohort as independent validation datasets, both of which confirmed the consistency of our results (Supplementary Figs. S3 and S4).

a Comparison of the ESTIMATE score, immune score, and stromal score between ECM1 and ECM2 subtypes. ECM1 shows significantly higher immune and stromal scores. b Comparison of tumor purity between ECM1 and ECM2 subtypes, with ECM2 exhibiting significantly higher tumor purity. c Boxplots showing the estimated proportions of various immune cell types in ECM1 and ECM2 subtypes, with ECM1 enriched in B cells, DCs, Macrophages, Mast cells, and T cells. Significant differences are marked with P-values. d GSVA analysis of immune signatures across ECM1 and ECM2 subtypes, highlighting significantly higher immune activation in ECM1, including enriched signatures for aDCs, B cells, Macrophages, NK cells, and T helper cells. e GSVA analysis of immune-related pathways, showing significant enrichment of immune-related functions in ECM1, including T cell co-stimulation, HLA, APC co-inhibition, and inflammation-promoting pathways. f Boxplots showing the expression of key immune-related genes, with significant upregulation in ECM1 for genes such as CD80, CD44, TNFRSF1A, and ICOS, indicating stronger immune activation in ECM1. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001.
Isocitrate dehydrogenase (IDH) is a key enzyme in the tricarboxylic acid (TCA) cycle, and somatic variation in IDH-mutant gliomas suggests potential metabolic differences between ECM1 and ECM2 subtypes. We performed pathway enrichment analysis to investigate metabolism-related signatures. As shown in Supplementary Fig. S5a, in the CGGA325 cohort, ECM1 exhibited significantly higher enrichment in pathways associated with amino acid metabolism, including Kynurenine Metabolism and Valine, Leucine, and Isoleucine Biosynthesis. Similarly, ECM1 was also enriched in pathways related to lipid metabolism, such as Aldosterone Biosynthesis and Retinol Metabolism, suggesting enhanced lipid metabolic activity. Furthermore, ECM1 demonstrated significant enrichment in other metabolic pathways, including pentose and glucuronate interconversions, retinoic acid metabolism, and vitamin K.
These findings were consistently validated in the CGGA693 cohort and TCGA cohort (Supplementary Fig. S5b, c), where ECM1 also showed higher enrichment in similar amino acid, lipid, and other metabolic pathways compared to ECM2. The observed metabolic differences between ECM1 and ECM2 subtypes further highlight the potential role of metabolic reprogramming in driving the biological and clinical heterogeneity of IDH-mutant gliomas.
Identification of an ECM signature with prognostic significance
To achieve a more accurate quantification of ECM levels, we developed an ECM-based prognostic signature. DEGs between the ECM1 and ECM2 subtypes were identified at the whole-transcriptome level in the CGGA325 cohort. Among these DEGs, 120 genes overlapped with the ECM gene set. Using LASSO Cox regression analysis (Fig. 4a), we identified a four-gene signature consisting of CLCF1, COL11A1, CSPG5, and SULF1. A risk score was then constructed based on the expression levels of these four genes, and a risk factor association plot was generated to stratify patients into high- and low-risk groups (Fig. 4b). Kaplan–Meier survival analysis demonstrated that patients in the high-risk group had significantly worse OS compared to those in the low-risk group (Fig. 4c). Furthermore, receiver operating characteristic (ROC) curve analysis revealed that the risk score exhibited a higher area under the curve (AUC) and concordance index compared to other clinical factors such as age, sex, and tumor grade, highlighting its superior prognostic performance (Fig. 4d, f). The ROC curves demonstrated that the ECM-based signature had excellent predictive accuracy for 1-, 3-, and 5-year OS, with AUC values of 0.809, 0.806, and 0.854, respectively (Fig. 4e). The nomogram demonstrated that the ECM-based risk score had the strongest predictive power for OS, outperforming traditional clinical factors such as age, gender, and tumor grade (Fig. 4g). The calibration curve demonstrated excellent agreement between the nomogram-predicted and observed OS rates at 1, 3, and 5 years, indicating that the ECM-based signature provides highly accurate and reliable prognostic predictions for patient survival (Fig. 4h).

a Partial likelihood deviance plot showing the optimal selection of ECM signature genes. b Distribution of risk scores and survival times for each patient, with high-risk patients shown in red and low-risk patients in blue. The expression levels of key genes (SULF1, CSPG5, COL11A1, and CLCF1) are also shown for each patient, with higher expression levels associated with the high-risk group. c Kaplan–Meier survival analysis comparing OS between high-risk and low-risk groups, with a significant difference (P < 0.0001) in survival probability. d ROC curves showing the predictive performance of age, gender, grade, and risk score for OS, with risk score exhibiting the highest AUC (AUC = 0.854). e ROC curves at 1, 3, and 5 years for risk score, demonstrating the robustness of the ECM signature in predicting long-term survival outcomes. f Concordance index (C-index) for risk score, age, gender, and grade over time, with risk score showing superior predictive accuracy. g Nomogram combining risk score, age, gender, and grade for predicting OS at 1, 3, and 5 years. The corresponding survival probabilities for each factor are displayed, with risk score and grade having the greatest impact on OS prediction. h Calibration plot comparing nomogram-predicted OS with observed OS at 1, 3, and 5 years, showing excellent agreement between predicted and observed outcomes.
To validate the robustness of this ECM-based signature, we applied it to independent validation cohorts, including the CGGA693, TCGA, and GLASS datasets. Consistent results were observed across all validation datasets, confirming the reliability and predictive power of the signature (Supplementary Fig. S6a–f).
To further investigate the distribution of ECM-related genes across single-cell subpopulations, we analyzed two IDH-mutant single-cell sequencing datasets (GSE7063014 and GSE8956715). First, t-SNE visualization revealed that cells were clustered into three primary subpopulations: tumor cells, TME, and normal oligodendrocytes (Supplementary Fig. S7a, f). Dot plots then showed the expression profiles of marker genes specific to each subpopulation (Supplementary Fig. S7b, g). Subsequently, we computed enrichment scores for three categories of ECM-related genes in single cells: (1) four prognostic ECM signature genes (predicted to be high- and low-risk), (2) ECM gene sets associated with prognosis, and (3) all ECM gene sets. The results demonstrated that the enrichment scores of these four ECM signatures exhibited marked heterogeneity in tumor cells, with both high and low scores observed (Supplementary Fig. S6c, h), which was consistent with bulk transcriptome-based prognostic model findings, where the four prognostic ECM predictor genes were shown to distinguish IDH-mutant gliomas into high-risk and low-risk groups. Notably, ECM gene sets linked to prognosis (Supplementary Fig. S6d, e) and all ECM gene sets (Supplementary Fig. S6i, j) displayed significant enrichment specifically in TME cells, suggesting that non-tumor cells are the primary drivers of ECM gene expression in this context.
To further validate the clinical implications of ECM subtyping, we performed radiological analysis to assess imaging differences between ECM1 and ECM2 tumors using a radiology dataset from the CGGA database. Representative magnetic resonance imaging (MRI) scans illustrated that ECM1 subtype tumors displayed more aggressive radiological features compared to ECM2 tumors (Fig. 5a). Quantitative analysis revealed that ECM1 tumors exhibited significantly higher proportions of peritumoral edema (P < 0.0001) and tumor necrosis (P = 0.0039), while enhancement patterns showed a trend towards increased prevalence in ECM1 tumors but did not reach statistical significance (P = 0.0567) (Fig. 5b). These imaging findings further support the more aggressive biological and clinical phenotype observed in ECM1 gliomas.

a Representative MRI scans (T1-weighted, contrast-enhanced T1-weighted, and T2-weighted sequences, from left to right) demonstrating distinct imaging characteristics of ECM1 and ECM2 subtypes. ECM1 tumors exhibited larger tumor volumes with pronounced enhancement, extensive peritumoral edema, and necrosis, compared to ECM2 tumors. b Quantitative analysis of radiological features showed significantly higher proportions of peritumoral edema (P < 0.0001) and necrosis (P = 0.0039) in the ECM1 subtype. Enhancement prevalence showed a trend toward being higher in ECM1 tumors but did not reach statistical significance (P = 0.0567). Statistical analysis was conducted using Fisher’s exact test. n.s. not significant; **P < 0.01, ***P < 0.001.
Insights into the relationship between ECM signature and EMT in IDH-mutant gliomas
The ECM regulates the EMT process of tumor cells through multiple mechanisms. To explore the specific regulatory mechanisms of ECM in IDH-mutant gliomas, we conducted further studies. First, we validated the accuracy of the constructed signature. As shown in Fig. 6a, the risk score was significantly higher in the ECM1 subtype compared to the ECM2 subtype (P < 0.0001), indicating a stronger association of ECM1 with poor prognosis. Based on the EMT signature constructed from our previous research, we analyzed the differences in EMT levels between ECM subtypes. The EMT score was significantly higher in the ECM1 subtype compared to the ECM2 subtype (Fig. 6b), suggesting that ECM1 is more strongly associated with EMT in IDH-mutant gliomas. Furthermore, a strong positive correlation was observed between the risk score and EMT score (R = 0.70, P < 2.2e-16), indicating that higher risk scores are closely associated with enhanced EMT in IDH-mutant gliomas (Fig. 6c). As shown in supplementary Fig. S8a–i, we validated the results using the CGGA 693 dataset, TCGA database, and GLASS database, and obtained consistent findings. As shown in Fig. 6d, KEGG pathway analysis of the overlapping genes between highly expressed ECM1 and EMT core genes revealed significant enrichment in several key biological pathways, including ECM-receptor interaction, cellular senescence, and focal adhesion. Additionally, pathways such as IL-17 signaling, and TNF signaling were also enriched. These findings suggest that ECM1-related gene expression is closely linked to processes that contribute to EMT and tumor progression in IDH-mutant gliomas. The gene interaction network highlights key molecules such as FN1, CD44, MMP9, and ITGB1 that are centrally connected, suggesting a complex network of interactions among genes involved in ECM remodeling, cell adhesion, and EMT processes in IDH-mutant gliomas, contributing to tumor progression (Fig. 6e).

a Comparison of risk scores between ECM1 and ECM2 subtypes, with ECM1 showing significantly higher risk scores than ECM2. b Comparison of EMT scores between ECM1 and ECM2 subtypes, with ECM1 exhibiting significantly higher EMT scores, suggesting stronger EMT in ECM1. c Strong positive correlation between risk scores and EMT scores (R = 0.70, P < 2.2e-16), indicating that higher risk is associated with more advanced EMT stages in IDH-mutant gliomas. d KEGG pathway analysis showing significant enrichment of pathways related to ECM-receptor interaction, cellular senescence, and proteoglycans in cancer in ECM1, suggesting ECM1 involvement in these processes. Pathways are colored by -log10(P-value), with larger circles indicating more enriched pathways. e Gene interaction network highlights key genes (FN1, CD44, MMP9, and ITGB1) central to the ECM1 signature, showing strong interconnections that suggest their critical roles in ECM remodeling and EMT processes in IDH-mutant gliomas. Genes involved in cell adhesion, cytokine signaling, and immune response are prominently featured in this network. ****P < 0.0001.
Prognostic differences in ECM subtypes are attributed to distinct distributions across EMT states
In order to further explore how ECM1 and ECM2 subtypes are influenced by or influence the EMT process to account for the prognostic differences observed between these two subgroups, we further evaluated the distribution of these subtypes across different stages of EMT, namely the EPI stage, hEMT stage, and MES stage. Consensus clustering analysis of EMT-related genes revealed distinct expression patterns between the two subtypes across these stages (Fig. 7a). The heatmap presents the genes associated with the EPI stage (Fig. 7b), where ECM1 is predominantly enriched in the EPI low group, accounting for 61%, compared to ECM2, which is more evenly distributed across both EPI high and EPI low categories (Fig. 7c). Furthermore, in the hEMT stage, ECM1 is more strongly associated with the hEMT high category (79%), while ECM2 predominantly falls into the hEMT low group (93%) (Fig. 7d–f). In the MES stage, ECM1 is significantly enriched in the MES high group (65%) compared to ECM2, which is predominantly in the MES low group (99%) (Fig. 7g–i). Finally, the quantification of these distributions confirms the significant differences between ECM1 and ECM2 subtypes, with ECM1 being more strongly associated with the later stages of EMT, including hEMT and MES (Fig. 7j–l). And the similar results can be obtained in the CGGA693 dataset (Supplementary Fig. S9). These findings suggest that ECM1 subtypes are linked to the more aggressive and advanced stages of EMT, which may contribute to their poorer prognostic outcomes compared to ECM2 subtypes.

a Unsupervised clustering analysis of ECM1 and ECM2 subtypes based on gene expression profiles, identifying distinct patterns across EPI, hEMT, and MES stages. b Heatmap showing the expression of key EPI markers in the EPI high and EPI low stages, with significant differences between ECM1 and ECM2. c Proportion of ECM1 and ECM2 samples in the EPI high1, EPI high 2, and EPI low categories, with ECM1 primarily enriched in the EPI low group (61%). d Unsupervised clustering of genes associated with the hEMT stage. e Heatmap showing the expression of hEMT markers, highlighting the significant difference between ECM1 and ECM2 subtypes. f Proportion of ECM1 and ECM2 samples in the hEMT high and hEMT low categories, with ECM1 being strongly enriched in the hEMT high group (79%). g Unsupervised clustering of genes related to the MES stage. h Heatmap of MES markers in the ECM1 and ECM2 subtypes, indicating distinct expression patterns. i Proportion of ECM1 and ECM2 samples in the MES high and MES low categories, with ECM1 enriched in the MES high group (65%) compared to ECM2 (1%). j Percentage of EPI high samples in ECM1 and ECM2 subtypes, showing no significant difference between the two subtypes. k Significant difference in the percentage of hEMT high samples between ECM1 and ECM2, with ECM1 showing a higher proportion (P < 0.01). l Significant difference in the percentage of MES high samples between ECM1 and ECM2, with ECM1 showing a higher proportion (P < 0.01). These findings suggest ECM1 is associated with later stages of EMT (hEMT and MES), which are linked to more aggressive tumor behavior.
We also compared the expression levels of characteristic markers for each EMT stage, these markers represent the EPI, hEMT, and MES stages, highlighting the differences in gene expression between ECM1 and ECM2 subtypes. The expression of EPI markers such as CDH1, DSP, OCLN, and CRB3 did not show significant differences between ECM1 and ECM2 subtypes (Fig. 8a–d). However, for hEMT markers, such as PDPN, ITGA5, P4HA2, and TNC, ECM1 showed significantly higher expression, with ITGA5 (P < 2.22e-16) and TNC (P = 2.7e-16) being particularly notable (Fig. 8e–h). Furthermore, in the MES phase, genes like VIM, SNAI1, SNAI2, and FN1 were significantly higher in ECM1, with VIM (P < 2.22e-16) and FN1 (P < 2.22e-16) exhibiting the most pronounced differences (Fig. 8i–l). These findings reinforce the association of ECM1 with later stages of EMT, characterized by higher expression of MES and hEMT markers, suggesting a more aggressive tumor phenotype.

a–l Comparison of gene expression for EPI, hEMT, and MES signature genes between ECM1 and ECM2 subtypes. Significant differences in expression levels are observed for key markers of EPI transition (CDH1, DSP, OCLN, and CRB3), hEMT (PDPN, ITGA5, P4HA2, and TNC), and MES transition (VIM, SNAI1, SNAI2, and FN1), with ECM1 showing significantly higher expression for most markers associated with hybrid and MES EMT, including ITGA5, TNC, VIM, SNAI1, SNAI2, and FN1 (P < 0.0001 for many comparisons). m–t Comparison of gene expression for proliferation, stemness, angiogenesis, and plasticity signatures. ECM1 subtypes show significantly higher expression of proliferation markers (e.g., MKI67, PCNA, P < 0.0001), stemness markers (SOX2, CD44, P < 0.01 to P < 0.0001), angiogenesis markers (VEGFA, VEGFB, P < 0.0001 for VEGFA, P < 0.05 for VEGFB), and plasticity markers (MMP2, MMP9, P < 0.0001). These findings indicate that ECM1 is associated with more aggressive tumor features such as increased proliferation, stemness, angiogenesis, and plasticity.
Additionally, we also compared key biological processes related to tumor malignancy and their association with EMT in the CGGA325 dataset, such as proliferation capacity, tumor stemness, angiogenesis potential, and tumor matrix remodeling. ECM1 and ECM2 subtypes displayed significant differences in these critical tumor biology processes. For proliferation, both MKI67 and PCNA expression levels were significantly higher in ECM1 compared to ECM2 (P < 0.0001 for MKI67 and P < 0.0001 for PCNA), indicating a stronger proliferative capacity in ECM1 tumors (Fig. 8m, n). Regarding stemness, markers like SOX2 and CD44 were also elevated in ECM1 compared to ECM2 (P = 0.004 for SOX2 and P < 0.0001 for CD44), suggesting a more stem-like, less differentiated state in ECM1 (Fig. 8o, p). In terms of angiogenesis, VEGFA expression was significantly higher in ECM1 (P < 0.0001) than in ECM2 (Fig. 8q). Furthermore, ECM1 showed increased VEGFB expression (P = 0.015) compared to ECM2, suggesting a higher angiogenic potential in ECM1 tumors (Fig. 8r). Finally, for plasticity, both MMP2 and MMP9, key markers involved in ECM remodeling, were significantly upregulated in ECM1 (P < 0.0001 for MMP2 and P < 0.0001 for MMP9), further highlighting the aggressive tumor nature of ECM1 and its enhanced ability to remodel the TME (Fig. 8s, t). And the similar results can be found in another two validation datasets, which are the CGGA693 dataset (Supplementary Fig. S10) and the TCGA dataset (Supplementary Fig. S11). These results collectively suggest that ECM1 is associated with more aggressive tumor characteristics, including higher proliferation, stemness, angiogenesis, and matrix remodeling, which may contribute to its poorer prognosis compared to ECM2.
ECM signatures demonstrate superior molecular docking compatibility with vinblastine, docetaxel, erlotinib, fedratinib, and vorasidenib
To further evaluate the potential drugs of ECM subgroups, we conducted the drug sensitivity analysis in the CGGA325 training dataset and another three validation datasets (CGGA693, TCGA, and GLASS). Venn diagram analysis identified 106 candidate drugs with statistically significant differential efficacy (IC50, P < 0.05), demonstrating subtype-specific drug sensitivity patterns between glioma subtypes. Specifically, 94 compounds exhibited inhibitory activity in the ECM1 subtype, while 12 drugs showed comparable potency in the ECM2 subtype. To prioritize therapeutically relevant candidates, we selected top five drugs with minimal P-values within each subtype, then four lead compounds—Vinblastine and Docetaxel (ECM1-predominant), as well as Erlotinib and Fedratinib (ECM2-predominant) for further mechanistic investigation (Fig. 9a). Vinblastine and Docetaxel illustrated uniform lower IC50 value in ECM1 compared to ECM2 in four datasets, and Erlotinib and Fedratinib showed lower IC50 value in ECM2 compared to ECM1 in all analyzed datasets (Supplementary Fig. S12).

a Venn diagram depicting the overlap of top-ranked drugs (IC50, P < 0.05) across four glioma datasets (CGGA693, CGGA325, TCGA, and GLASS). ECM1 subtype showed 94 drug candidates (e.g., Vinblastine and Docetaxel), while ECM2 identified 12 drugs (e.g., Erlotinib and Fedratinib). b Three-dimensional structures of selected drugs: Vinblastine (left-top), Docetaxel (right-top), Erlotinib (left-bottom), and Fedratinib (right-bottom). c–j Binding conformations of Vinblastine (c–f) and Docetaxel (g–j) with ECM clinically relevant key signatures.
The three-dimensional (3D) molecular architectures of the four candidate compounds were illustrated in Fig. 9b, revealing distinct structural features relevant to subtype-specific drug targeting. Structural modeling and molecular docking simulations further supported the potential interaction modalities between these compounds and the ECM signatures (Fig. 9c–j and Supplementary Fig. S13). These findings collectively demonstrate that Vinblastine, Docetaxel, Erlotinib, and Fedratinib emerge as promising therapeutic agents for ECM key clinically relevant signatures mediated molecular pathways in IDH-mutant gliomas, with potential implications for improving patient survival and overcoming chemoresistance through targeted pathway inhibition.
To potentially enhance the clinical relevance of the distinct ECM clusters of IDH-mutant gliomas, we conducted stratified analyses across multiple datasets (CGGA325, CGGA693, TCGA, and GLASS), and found that ECM risk scores were consistently higher in IDH-mutant astrocytomas (A) than in oligodendrogliomas (O) (Supplementary Fig. S14a–d). These results reinforce the notion that ECM remodeling is more active in astrocytic tumors, which typically exhibit more aggressive biological behavior. Vorasidenib (AG-881), an oral brain-penetrant inhibitor of mutant IDH enzymes, showed preliminary activity in IDH-mutant gliomas16, in silico docking analysis suggests potential binding interactions between Vorasidenib and these ECM signatures (SULF1, CSPG5, COL11A1, and CLCF1) (Supplementary Fig. S14e–h). This raises the hypothesis that ECM-related molecular components may modulate drug accessibility, metabolism, or downstream signaling pathways, and thus may influence the overall effectiveness of IDH inhibition.
Discussion
Although IDH-mutant gliomas, predominantly harboring the IDH1 R132H mutation, are generally considered a molecular subtype associated with a more favorable prognosis compared to IDH-wildtype gliomas, clinical reality often presents a more complex picture17. In our daily clinical practice, it is not uncommon to encounter patients with IDH-mutant gliomas who experience poor therapeutic responses and rapid disease progression, despite standard treatment regimens. As one of the most heterogeneous tumor types, gliomas harbor significant intertumoral and intratumoral variability within the TME, which may give rise to divergent clinical outcomes even within molecularly defined subtypes18. Among these factors, the ECM has emerged as a critical regulator of tumor behavior and treatment response19,20, yet remains underexplored in the context of IDH-mutant gliomas.
In our study, we performed unsupervised clustering based on ECM-related gene expression and identified two molecularly distinct subtypes in IDH mutant glioma, namely ECM1 and ECM2. These subtypes exhibited clear differences in clinical and molecular characteristics, including tumor grade, 1p/19q co-deletion status, and MGMT promoter methylation. More importantly, ECM1 tumors were associated with significantly worse OS, suggesting that ECM heterogeneity is an important determinant of prognosis in IDH-mutant gliomas. Differential expression and pathway enrichment analyses revealed that ECM1 tumors were characterized by increased activity in pathways related to cell division and immune response, highlighting the potential roles of malignant cell plasticity and immunological remodeling in driving poor outcomes.
The ECM is a complex and dynamic network composed of structural proteins such as laminins and fibronectins, which are also the major components of the Schwann cell basal lamina21. These components not only provide mechanical support but also actively participate in regulating cellular differentiation, intercellular communication, and immune modulation22,23. Thus, the ECM is increasingly recognized as an immunoregulatory scaffold that influences immune cell infiltration, spatial distribution, and functional state. Our findings revealed that ECM1 tumors exhibited higher immune and stromal scores, along with lower tumor purity. Immune profiling demonstrated that ECM1 tumors were enriched in DCs, macrophages, plasma cells, and CD8 + T cells, and showed increased expression of multiple immune checkpoint-related genes, suggesting a more complex and immunologically active, yet potentially immunosuppressive microenvironment. These results underscore the role of ECM heterogeneity in shaping the immune landscape, which may influence therapeutic response and clinical outcomes.
Moreover, our single-cell analysis revealed that ECM-related gene expression is primarily localized to non-tumor microenvironmental cell populations, consistent with a stromal or immune origin. However, we also observed moderate expression of the four-gene prognostic signature within subsets of tumor cells. This may reflect a MES-like or EMT-associated transcriptional state within the malignant compartment, suggesting that tumor-intrinsic and microenvironmental ECM programs may cooperate to shape glioma progression. These observations highlight the complex and non-exclusive cellular origin of ECM-based signatures and warrant future spatial and functional studies to delineate their precise sources and mechanistic roles.
Interestingly, our prior work24 demonstrated that IDH-mutant astrocytomas and oligodendrogliomas likely share a common developmental origin from oligodendrocyte precursor cells (OPCs), despite their divergent histological and clinical trajectories. We hypothesize that differences in the TME-particularly ECM composition, play a pivotal role in directing these tumors toward distinct lineage fates during malignant progression. Such divergence may underlie not only their transcriptomic and radiographic differences but also their variable prognostic outcomes. While this remains speculative, it raises the possibility that microenvironmental cues, including ECM remodeling, may act as instructive factors in glioma lineage bifurcation and evolution. Future investigations integrating spatial transcriptomics and functional models will be essential to test this hypothesis.
Besides, our findings that ECM1 tumors were enriched in cell division-related pathways may not only indicate increased proliferation, but also reflect malignant cellular differentiation potential, contributing to a more aggressive tumor phenotype. The bidirectional relationship between ECM and EPI–MES transition (EMT) has been a long-standing topic in cancer biology. ECM components such as fibronectin, collagen, and integrins are well-established inducers of EMT, while EMT itself contributes to ECM remodeling by increasing matrix stiffness and plasticity25. However, this interplay remains largely unexplored in IDH-mutant gliomas. In our study, we demonstrated that ECM1 tumors exhibited significantly higher EMT scores and a strong positive correlation between risk score and EMT activation. Enrichment of ECM-receptor interaction, cellular senescence, and adhesion-related pathways in ECM1 further supports the mechanistic link between ECM composition and EMT progression. A gene interaction network revealed central roles of FN1, CD44, and MMP9, classical mediators of both ECM remodeling and EMT regulation.
EMT is no longer viewed as a binary process but rather a dynamic and reversible spectrum of intermediate states, including EPI, hEMT, and MES stages11. Each state is characterized by specific molecular markers, some stably expressed throughout the EMT continuum (e.g., VIM and FN1), some transiently upregulated during intermediate states (e.g., PDPN, ITGA5, and TNC), and others primarily expressed in early EPI phases (e.g., CDH1, OCLN, and DSP)26. By profiling the expression of these markers, we found that ECM1 tumors were predominantly enriched in hEMT and MES stages, while ECM2 tumors were mostly confined to EPI or EMT-inactive states, indicating that ECM heterogeneity may drive tumors toward more advanced EMT phenotypes.
Importantly, these phenotypic transitions were accompanied by distinct biological behaviors. ECM1 tumors exhibited significantly higher proliferative capacity, stemness potential, angiogenesis activity, and ECM remodeling ability, as evidenced by increased expression of markers such as MKI67, SOX2, VEGFA, MMP2, and MMP9. These features collectively suggest that ECM1 represents a biologically aggressive subtype, associated with enhanced plasticity, invasive capacity, and treatment resistance.
Further supporting this notion, preliminary analysis of radiological data indicated that ECM1 tumors tend to present with more malignant imaging features, including more extensive enhancement, necrosis, and peritumoral edema, which are known correlates of poor clinical outcomes. This highlights the potential clinical utility of ECM-based classification in guiding radiological interpretation and therapeutic planning.
Given the distinct molecular and prognostic profiles of ECM subtypes in IDH-mutant gliomas, targeted therapeutic strategies based on ECM-associated molecular vulnerabilities could provide meaningful clinical benefits. To explore such opportunities, we performed an in silico drug sensitivity screening to identify small-molecule compounds specifically effective against ECM1 and ECM2 subtypes.
Our analyses revealed subtype-specific sensitivities: notably, the ECM1 subtype showed lower predicted IC50 values and enhanced sensitivity toward drugs including Vinblastine, Docetaxel, WZ-1-84, FTI-277, and Cyclopamine. In contrast, ECM2 subtype tumors were predicted to exhibit selective sensitivity to targeted kinase inhibitors such as Erlotinib and Fedratinib.
Vinblastine and Docetaxel, widely recognized microtubule-disrupting agents, have been clinically utilized to disrupt mitotic spindle assembly and inhibit tumor proliferation, aligning with the aggressive proliferative phenotype observed in ECM1 tumors. Additionally, ECM1 heightened EMT status and ECM remodeling capacity suggest that targeting cytoskeletal dynamics could indeed represent a feasible therapeutic strategy. Conversely, the sensitivity of ECM2 tumors toward kinase inhibitors, particularly Erlotinib (EGFR inhibitor)27,28 and Fedratinib (JAK2 inhibitor)29, corresponds well with their relatively less aggressive and potentially growth factor-dependent characteristics, suggesting targeted inhibition of signaling pathways may effectively attenuate tumor growth in this subset.
Together, our findings demonstrate the feasibility of subtype-specific pharmacological targeting based on ECM-associated molecular subtyping, offering a promising avenue for precision oncology in IDH-mutant gliomas. However, further preclinical validation in cell lines and animal models is warranted to substantiate the clinical applicability and efficacy of these identified candidate drugs. These findings offer new therapeutic possibilities and provide a foundation for future development of precision-targeted therapies tailored to ECM-defined tumor subtypes.
Despite the robust multi-omics design and cross-cohort validation, this study has several limitations. First, the lack of functional validation using glioma cell lines and in vivo models precludes direct mechanistic proof of ECM-EMT interactions. Second, the absence of single-cell transcriptomic data limits our ability to resolve the precise cellular sources of ECM components and dissect cell–cell communication networks. Third, spatial transcriptomics would be invaluable for mapping the co-localization of ECM signatures and EMT states, which remains unaddressed in the current study. These limitations will be addressed in future work through integrated spatial and single-cell profiling, as well as functional validation in experimental models, to more comprehensively elucidate the role of ECM heterogeneity in glioma progression.
Another limitation of the current study is the heterogeneity in sample annotation across different datasets. In particular, older designations such as “oligoastrocytoma” (AO) reflect outdated diagnostic criteria. Although these labels were retained in the original datasets, we attempted to mitigate their impact by cross-referencing 1p/19q codeletion and TP53 status when available. Moreover, the method used for 1p/19q assessment varied across datasets; while most recent cohorts rely on SNP-array or sequencing-based approaches, earlier datasets may have used FISH, which is now recognized to have a non-negligible false positive rate. This potential source of diagnostic ambiguity should be considered when interpreting ECM subtype associations with molecular features.
A further challenge lies in the temporal plasticity of the ECM and TME, which evolve during disease progression and in response to therapeutic interventions. Our current study is based on cross-sectional transcriptomic snapshots and thus cannot capture the dynamic remodeling of the ECM over time. Future studies leveraging longitudinal sampling (e.g., rebiopsies) or experimental models will be essential to dissect how ECM states change with treatment and how they influence clinical outcomes.
Methods
Samples and databases
This study contained 965 IDH-mutant gliomas from three public databases: Chinese Glioma Genome Atlas (CGGA, https://www.cgga.org.cn/download_other.jsp)30: RNA-seq data with clinical and survival information from 167 IDH-mutant glioma patients (CGGA325 dataset) and 333 IDH-mutant glioma patients (CGGA693 dataset), The Cancer Genome Atlas Program (TCGA, https://www.cancer.gov/tcga)31: 368 IDH-mutant glioma RNA-seq samples with clinical and survival information, and The Glioma Longitudinal Analysis Consortium (GLASS, http://synapse.org/glass)32: 97 IDH-mutant glioma RNA-seq patients with clinical and survival information. Single-cell sequencing data of IDH-mutant gliomas, along with their corresponding clinical information, were retrieved from the GEO database for the following datasets: GSE7063014 (n = 6; https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE70630) and GSE8956715 (n = 10; https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE89567).
Identification of ECM subtypes
The ECM-related gene signatures (collagens, proteoglycans, glycoproteins, matrisome regulators, secreted factors, and affiliated genes) were downloaded from The Human Molecular Signatures Database (MSigDB, https://www.gsea-msigdb.org/gsea/msigdb/human/collections.jsp) for the subsequent clustering analysis33,34,35. Survival-associated genes (p < 0.05) were identified using the “survival” and “survminer” R packages in the CGGA325 cohort. Genes with high median absolute deviation (MAD ≥ 0.5) were selected for consensus clustering via the “ConsensusClusterPlus” package36,37. To determine the ideal number of robust clusters, the cumulative distribution function (CDF) and consensus heatmap were adopted to assess the optimal K. And same analysis was repeated and validated in CGGA693, TCGA, and GLASS datasets, and the same K value was obtained in all three datasets.
Bioinformatic analysis
R package “princomp” was used for principal components analysis (PCA) to detect the expression difference between both subtypes38. Heatmaps displaying the survival-related ECM genes in two subgroups were created using with R package “pheatmap”. Significantly differentially expressed genes ((|log2fold-change (FC)| >1 and p < 0.05) between the ECM1 and ECM2 groups were identified with the R package “limma”39, and volcano plots were visualized by utilizing R software. Subsequently, to provide functional annotations for these genes, Gene Ontology (GO) terms were defined by using DAVID functional annotation bioinformatics microarray analysis40,41. Additionally, receiver-operating characteristic (ROC) curve analysis was performed to predict OS by using R package “survivalROC”42.
Mutation landscape assessment
To distinguish the mutation landscape of canonical genes and significant genes in two ECM groups, cBioPortal online software (version 6.0.24) was adopted, and oncoplots were mapped according to the mutation types and mutation frequency43,44.
Estimation of immune infiltration
To evaluate the immune infiltration in both ECM subtypes, the ESTIMATE R package was first used to evaluate the immune cell, stromal content, and tumor purity for each sample45. And CIBERSORT algorithm was adopted to estimate the relative fraction of 22 immune cell types46,47. Further, Single-sample gene-set enrichment analysis (ssGSEA) was performed to distinguish immune cells that infiltrated tumors for the two subgroups by utilizing the R package “GSVA”48,49.
Computation of metabolism-relevant gene signatures
Amino acid metabolism relevant signatures, lipid metabolism relevant signatures, and other metabolism signatures were acquired from previously published researches50,51. And the enrichment levels of metabolism-related signatures were quantified for each sample in two subgroups by using R package “GSVA”48,49.
Construction of a prognostic risk model
To construct an ECM-related prognostic risk model, we first overlapped the enriched genes in the ECM1 subgroup in the CGGA325 dataset with the ECM signatures. The Least Absolute Shrinkage and Selection Operator (LASSO) method was subsequently utilized to define a gene signature through R package “glmnet”52. The CGGA325 dataset was used as the training set, and CGGA693, TCGA, and GLASS were used as the validation sets.
Nomogram design and construction
Nomogram analysis was built to predict patients’ survival outcome in terms of OS for 1, 3, and 5-year periods in the CGGA325 IDH-mutant cohorts by using R packages “regplot”53 and “survival”. Then, the predictive accuracy of our nomogram survival models was assessed through calibration curves and C-Index values.
Analysis of single-cell RNA-seq data
The single cell expression matrix was analyzed using default parameters in Seurat (version 4.0.2, https://satijalab.org/seurat/articles/get_started.html)54,55 following a standardized workflow, which comprised the following key steps: data preprocessing and normalization, feature selection (nFeatures = 2000), data scaling, linear dimensionality reduction, identification of principal component dimensions based on a significance threshold (p < e⁻¹⁰), and t-SNE-based cell clustering with subsequent identification of cluster markers (SOX2 for malignant tumor cells56; PDGFRA, DLL3 and OLIG2 for IDH-mutant tumor cells57,58; CX3CR1, CD68 and P2RY12 for tumor microenvironmental cells (TME)15; KLK6, MAG and MOBP for oligodendrocytes14,58). Next, we used Seurat’s built-in “AddModuleScore” function to calculate the enrichment scores of relevant gene sets across different cell types.
Protein-protein interaction network construction
In CGGA325 dataset, to analyze the relationship of overlap genes between signatures enriched in ECM1 group and EMT signatures downloaded from EPI−MES Transition Gene Database (dbEMT2.0, http://dbemt.bioinfo-minzhao.org), protein-protein interaction network was created by utilizing STRING (version 12.0) online database59, the results with high confidence (0.700) were subsequently imported into Cytoscape software (version 3.9.0)60, and the degree was calculated and ranked for the protein-protein interaction network mapping.
Radiological analysis
Radiological data were obtained from the publicly available CGGA imaging dataset. MRI images were independently reviewed by three experienced neuroradiologists or neurosurgeons, blinded to clinical outcomes and molecular subtype information. Imaging features assessed included: (1) enhancement, defined as the presence of distinct contrast-enhancing lesions on T1-weighted contrast-enhanced sequences, with non-contrast T1-weighted sequences reviewed simultaneously to exclude confounding factors such as hemorrhage; (2) edema, defined as clearly delineated peritumoral hyperintense areas observed on T2-weighted MRI sequences; and (3) necrosis, defined as the presence of cystic or necrotic regions within the tumor mass, indicating necrotic liquefaction. Final radiological features were determined by consensus agreement among all reviewers.
Evaluation of therapeutic drug sensitivity and molecular docking
The prediction of therapeutic response for IDH-mutant glioma patients to chemotherapeutic and targeted agents was conducted based on half-maximal inhibitory concentration (IC50) values. Drug screening and sensitivity analyses were performed using integrated R packages (pRRophetic61, ggpubr, ggplot2, and tidyr), applying a statistical significance threshold (pFilter = 0.05). Compound structures (2D/3D configurations) were obtained from PubChem, while the predicted conformations of the SULF1, CSPG5, COL11A1, and CLCF1 proteins were acquired from the Protein Data Bank (PDB). Subsequently, molecular docking simulations were carried out to characterize potential binding interfaces between proteins and therapeutic compounds by utilizing AutoDock Vina, with spatial configurations visualized at atomic resolution.
Statistical analysis
For statistical analyses, means with standard deviation (SD) of the results were shown in dot plots, bar charts, and bar-and-scatter plots. A t-test was performed for comparisons between two groups. The statistical analyses were performed using GraphPad Prism software (version 8.0.2), and statistical significances at P < 0.05, P < 0.01, P < 0.001, and P < 0.0001 were labeled as *, **, ***, and ****, respectively. In addition, combined violin and box plots were obtained by using R software (version 4.0.3), and a t-test was used to compare the significance of the difference between the two groups.
Data availability
The datasets analyzed for bulk RNA-seq during the current study are available in TCGA (https://www.cancer.gov/tcga), GLASS (http://synapse.org/glass), and CGGA (https://www.cgga.org.cn/download_other.jsp) datasets, and datasets analyzed for single cell RNA-seq are available in the GEO database (https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE70630, and https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE89567).
Code availability
Data analysis was conducted using R4.0.3 and GraphPad Prism8.0.2, and all analyses were performed with conventional analysis codes, no new codes were generated.
References
Schaff, L. R. & Mellinghoff, I. K. Glioblastoma and other primary brain malignancies in adults: a review. JAMA 329, 574–587 (2023).
Weller, M. et al. Glioma. Nat. Rev. Dis. Prim. 10, 33 (2024).
Louis, D. N. et al. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol. 23, 1231–1251 (2021).
Bhatia, A. et al. Tumor volume growth rates and doubling times during active surveillance of IDH-mutant low-grade glioma. Clin. Cancer Res. 30, 106–115 (2024).
Jeon, H. M. et al. Tissue factor is a critical regulator of radiation therapy-induced glioblastoma remodeling. Cancer Cell 41, 1480–97 e9 (2023).
Pasupuleti, V., Vora, L., Prasad, R., Nandakumar, D. N. & Khatri, D. K. Glioblastoma preclinical models: strengths and weaknesses. Biochim. Biophys. Acta Rev. Cancer 1879, 189059 (2024).
Collado, J., Boland, L., Ahrendsen, J. T., Miska, J. & Lee-Chang, C. Understanding the glioblastoma tumor microenvironment: leveraging the extracellular matrix to increase immunotherapy efficacy. Front. Immunol. 15, 1336476 (2024).
Yuan, Z. et al. Extracellular matrix remodeling in tumor progression and immune escape: from mechanisms to treatments. Mol. Cancer 22, 48 (2023).
Peng, D., Fu, M., Wang, M., Wei, Y. & Wei, X. Targeting TGF-beta signal transduction for fibrosis and cancer therapy. Mol. Cancer 21, 104 (2022).
Nieto, M. A., Huang, R. Y., Jackson, R. A. & Thiery, J. P. Emt: 2016. Cell 166, 21–45 (2016).
Brabletz, S., Schuhwerk, H., Brabletz, T. & Stemmler, M. P. Dynamic EMT: a multi-tool for tumor progression. EMBO J. 40, e108647 (2021).
Simeonov, K. P. et al. Single-cell lineage tracing of metastatic cancer reveals selection of hybrid EMT states. Cancer Cell 39, 1150–62 e9 (2021).
Rigillo, G. et al. The NF-Y splicing signature controls hybrid EMT and ECM-related pathways to promote aggressiveness of colon cancer. Cancer Lett. 567, 216262 (2023).
Tirosh, I. et al. Single-cell RNA-seq supports a developmental hierarchy in human oligodendroglioma. Nature 539, 309–313 (2016).
Venteicher, A. S. et al. Decoupling genetics, lineages, and microenvironment in IDH-mutant gliomas by single-cell RNA-seq. Science 355, eaai8478 (2017).
Mellinghoff, I. K. et al. Vorasidenib in IDH1- or IDH2-mutant low-grade glioma. N. Engl. J. Med. 389, 589–601 (2023).
Blanco-Carmona, E. et al. Tumor heterogeneity and tumor-microglia interactions in primary and recurrent IDH1-mutant gliomas. Cell Rep. Med. 4, 101249 (2023).
Liu, J. et al. Multi-scale signaling and tumor evolution in high-grade gliomas. Cancer Cell 42, 1217–38.e19 (2024).
Ferrer, V. P., Moura Neto, V. & Mentlein, R. Glioma infiltration and extracellular matrix: key players and modulators. Glia 66, 1542–1565 (2018).
Cui, X. et al. RUNX1/NPM1/H3K4me3 complex contributes to extracellular matrix remodeling via enhancing FOSL2 transcriptional activation in glioblastoma. Cell Death Dis. 15, 98 (2024).
Giese, A. et al. Migration of human glioma cells on myelin. Neurosurgery 38, 755–764 (1996).
Monzo, P. et al. Adaptive mechanoproperties mediated by the formin FMN1 characterize glioblastoma fitness for invasion. Dev. Cell 56, 2841–55 e8 (2021).
Galbo, P. M. Jr. et al. Functional contribution and clinical implication of cancer-associated fibroblasts in glioblastoma. Clin. Cancer Res. 30, 865–876 (2024).
Wei, Y. et al. Stalled oligodendrocyte differentiation in IDH-mutant gliomas. Genome Med. 15, 24 (2023).
Marhuenda, E. et al. Glioma stem cells invasive phenotype at optimal stiffness is driven by MGAT5 dependent mechanosensing. J. Exp. Clin. Cancer Res. 40, 139 (2021).
Malagoli Tagliazucchi, G., Wiecek, A. J., Withnell, E. & Secrier, M. Genomic and microenvironmental heterogeneity shaping epithelial-to-mesenchymal trajectories in cancer. Nat. Commun. 14, 789 (2023).
Nathanson, D. A. et al. Targeted therapy resistance mediated by dynamic regulation of extrachromosomal mutant EGFR DNA. Science 343, 72–76 (2014).
Hayes, T. K. et al. Comprehensive mutational scanning of EGFR reveals TKI sensitivities of extracellular domain mutants. Nat. Commun. 15, 2742 (2024).
McLornan, D. P., Pope, J. E., Gotlib, J. & Harrison, C. N. Current and future status of JAK inhibitors. Lancet 398, 803–816 (2021).
Zhao, Z. et al. Chinese Glioma Genome Atlas (CGGA): a comprehensive resource with functional genomic data from Chinese glioma patients. Genomics Proteom. Bioinforma. 19, 1–12 (2021).
Ceccarelli, M. et al. Molecular profiling reveals biologically discrete subsets and pathways of progression in diffuse glioma. Cell 164, 550–563 (2016).
Malta, T. M. et al. The epigenetic evolution of glioma is determined by the IDH1 mutation status and treatment regimen. Cancer Res. 84, 741–756 (2024).
Subramanian, A. et al. Gene set enrichment analysis: a knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. USA 102, 15545–15550 (2005).
Liberzon, A. et al. Molecular signatures database (MSigDB) 3.0. Bioinformatics 27, 1739–1740 (2011).
Liberzon, A. et al. The molecular signatures database (MSigDB) hallmark gene set collection. Cell Syst. 1, 417–425 (2015).
Wilkerson, M. D. & Hayes, D. N. ConsensusClusterPlus: a class discovery tool with confidence assessments and item tracking. Bioinformatics 26, 1572–1573 (2010).
Wu, F. et al. Molecular classification of IDH-mutant glioblastomas based on gene expression profiles. Carcinogenesis 40, 853–860 (2019).
Huang, R. et al. Identification of an ATP metabolism-related signature associated with prognosis and immune microenvironment in gliomas. Cancer Sci. 111, 2325–2335 (2020).
Ritchie, M. E. et al. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 43, e47 (2015).
Sherman, B. T. et al. DAVID: a web server for functional enrichment analysis and functional annotation of gene lists (2021 update). Nucleic Acids Res. 50, W216–w21 (2022).
Huang da, W., Sherman, B. T. & Lempicki, R. A. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat. Protoc. 4, 44–57 (2009).
Heagerty, P. J., Lumley, T. & Pepe, M. S. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics 56, 337–344 (2000).
Cerami, E. et al. The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2, 401–404 (2012).
Gao, J. et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci. Signal. 6, pl1 (2013).
Yoshihara, K. et al. Inferring tumour purity and stromal and immune cell admixture from expression data. Nat. Commun. 4, 2612 (2013).
Newman, A. M. et al. Robust enumeration of cell subsets from tissue expression profiles. Nat. methods 12, 453–457 (2015).
Wu, F. et al. Molecular subtyping reveals immune alterations in IDH wild-type lower-grade diffuse glioma. J. Pathol. 251, 272–283 (2020).
He, Y., Jiang, Z., Chen, C. & Wang, X. Classification of triple-negative breast cancers based on Immunogenomic profiling. J. Exp. Clin. cancer Res. CR 37, 327 (2018).
Hänzelmann, S., Castelo, R. & Guinney, J. GSVA: gene set variation analysis for microarray and RNA-seq data. BMC Bioinforma. 14, 7 (2013).
Yang, C., Huang, X., Liu, Z., Qin, W. & Wang, C. Metabolism-associated molecular classification of hepatocellular carcinoma. Mol. Oncol. 14, 896–913 (2020).
Rosario, S. R. et al. Pan-cancer analysis of transcriptional metabolic dysregulation using The Cancer Genome Atlas. Nat. Commun. 9, 5330 (2018).
Friedman, J., Hastie, T. & Tibshirani, R. Regularization paths for generalized linear models via coordinate descent. J. Stat. Softw. 33, 1–22 (2010).
Erady, C. et al. Pan-cancer analysis of transcripts encoding novel open-reading frames (nORFs) and their potential biological functions. NPJ Genom. Med. 6, 4 (2021).
Butler, A., Hoffman, P., Smibert, P., Papalexi, E. & Satija, R. Integrating single-cell transcriptomic data across different conditions, technologies, and species. Nat. Biotechnol. 36, 411–420 (2018).
Stuart, T. et al. Comprehensive integration of single-cell data. Cell 177, 1888–902.e21 (2019).
Yuan, J. et al. Single-cell transcriptome analysis of lineage diversity in high-grade glioma. Genome Med. 10, 57 (2018).
Weng, Q. et al. Single-cell transcriptomics uncovers glial progenitor diversity and cell fate determinants during development and gliomagenesis. Cell Stem Cell 24, 707–23.e8 (2019).
Marques, S. et al. Oligodendrocyte heterogeneity in the mouse juvenile and adult central nervous system. Science 352, 1326–1329 (2016).
Szklarczyk, D. et al. The STRING database in 2023: protein-protein association networks and functional enrichment analyses for any sequenced genome of interest. Nucleic Acids Res. 51, D638–d46 (2023).
Shannon, P. et al. Cytoscape: a software environment for integrated models of biomolecular interaction networks. Genome Res. 13, 2498–2504 (2003).
Geeleher, P., Cox, N. & Huang, R. S. pRRophetic: an R package for prediction of clinical chemotherapeutic response from tumor gene expression levels. PLoS One 9, e107468 (2014).
Acknowledgements
We sincerely thank the radiologists and neurosurgeons from the Department of Radiology and the Department of Neurosurgery at Sanbo Brain Hospital for their invaluable assistance in data processing, imaging assessment, and expert review of radiological data. Their professional input greatly facilitated the completion of this research. And this work was supported by the Fund of International Cooperation of Science and Technology of Henan Province (no. 242102521016), the National Key R&D Program of China (2023YFC2510000), the Start-up Fund of Henan Academy of Sciences (no. 241828051), the National Natural Science Foundation of China (82002653), the Laboratory for Clinical Medicine, Capital Medical University (no. 2024LCMCMU05), and the Start-up Fund of Henan Academy of Sciences (no. 231816047).
Author information
Authors and Affiliations
Contributions
Y.W. proposed the concept and performed data processing and bioinformatics analysis. D.C. and Y. F. performed molecular docking analysis and visualization. Q.Z., F.Y., L.Z., L.Z. and N.Z. participated in data analysis and interpretation. Y.W., G.L., J.Y. and X.F. contributed to the study design, drafted and revised the manuscript. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wei, Y., Chen, D., Zhang, Q. et al. ECM-based molecular subtypes define prognostic, EMT status, and therapeutic diversity in IDH-mutant gliomas. npj Precis. Onc. 9, 301 (2025). https://doi.org/10.1038/s41698-025-01100-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41698-025-01100-7
