
Abstract
Background
Older adults are vulnerable to mistimed food intake due to health and environmental changes; characterizing meal timing may inform strategies to promote healthy aging. We investigated longitudinal trajectories of self-reported meal timing in older adults and their associations with morbidity, genetic profiles, and all-cause mortality.
Methods
We analyzed data from 2945 community-dwelling older adults from the University of Manchester Longitudinal Study of Cognition in Normal Healthy Old Age, with up to five repeated assessments of meal timing and health behaviors conducted between 1983 and 2017. Linear mixed-effects models, latent class analysis, and Cox regression were used to examine relationships between meal timing with illness and behavioral factors, genetic scores for chronotype and obesity, and mortality.
Results
Here we show older age is associated with later breakfast and dinner times, a later eating midpoint, and a shorter daily eating window. Physical and psychological illnesses, including fatigue, oral health problems, depression, anxiety, and multimorbidity, are primarily associated with later breakfast. Genetic profiles related to an evening chronotype, but not obesity, are linked to later meals. Later breakfast timing is also associated with increased mortality. Latent class analysis of meal timing trajectories identify early and late eating groups, with 10-year survival rates of 86.7% in the late eating group compared to 89.5% in the early eating group.
Conclusions
Meal timing, particularly later breakfast, shifts with age and may reflect broader health changes in older adults, with implications for morbidity and longevity.
Plain language summary
As people get older, changes in health and daily routines can affect when they eat their meals. This study followed nearly 3000 older adults in the UK over several decades to understand how meal timing changes with age and how it relates to health and longevity. Participants reported the times they ate meals and completed health and lifestyle surveys across multiple years. We found that as people aged, they tended to eat breakfast and dinner later, and those with more health problems or a genetic tendency to stay up late also tended to eat later. Importantly, eating breakfast later with aging was linked to a higher risk of death. Our findings suggest that later meal timing, especially breakfast, could serve as a simple marker of health in older adults and may guide future strategies for healthy aging.
Similar content being viewed by others
Introduction
Chrononutrition, the study of the timing of eating, has emerged as a modifiable risk factor for adverse health outcomes1,2. The relevance of the timing of dietary intake on health and mortality was initially demonstrated in animal and human studies in the late 1970s3. Recent studies in rodents indicating greater fat mass accumulation when high-fat diets are consumed during atypical periods (i.e., inactive phases) compared to typical times (i.e., active phases), have renewed interest in this area4. Subsequent human studies showed that later meal times may diminish the efficacy of behavioral weight loss interventions and that late eating is associated with metabolic changes leading to higher body mass index (BMI) and body fat accumulation5,6,7,8. In addition, experimental studies showed that endogenous melatonin in circulation in the evening impairs glucose tolerance9. The role of eating schedules is biologically relevant as dietary intake acts as an environmental cue influencing the circadian clocks of peripheral metabolic tissues and therefore can contribute to circadian misalignment and internal desynchrony2,10. The emerging evidence largely suggests that later meal times, particularly eating during the biological evening, is detrimental to health, and that eating at night is expected to be among the leading factors mediating the link between night shift work and higher risk of disease2,11. However, the role of chrononutrition in older adults remains underexplored1,12.
Older adults constitute a vulnerable population for mistimed food intake because of the onset of multimorbidity and the environmental changes that often accompany aging. Current chrononutrition studies in older adults are limited to cross-sectional analyses comparing older to younger adults13,14,15,16,17. Eating times are expected to shift in older adulthood, partly because of documented behavioral changes, such as earlier bed and wake times18,19. In addition, older adults are at risk of dysphagia, dehydration, impaired swallowing and declining oral health, all of which can negatively impact overall diet and increase the risk of malnutrition20. Transitioning to retirement or assisted living facilities can further affect nutritional status21. A key priority of the NIH Common Fund’s Nutrition for Precision Health, the NHLBI nutrition research priorities, and the NIH Sleep Research Plan is to advocate for meal times that align with the circadian system1,22. Carefully characterizing meal timing in older adults can inform relevant food timing countermeasures to support healthy aging.
No longitudinal study has yet described lifetime trajectories of mealtime patterns in older adults, and few studies have explored the broader factors influencing meal timing in this population23. Existing research on meal timing has disproportionately focused on younger healthy adults and night shift workers2. Key factors known to influence meal timing include intrinsic elements, such as medication use, sleep disorders, genetics, and chronotype, as well as extrinsic factors like cultural practices, environmental conditions, food availability, and work schedules23. This longitudinal analysis aims to characterize meal timing trajectories in older adults and investigate their associations with morbidity, behaviors, genetic profiles, and all-cause mortality, utilizing data from the University of Manchester Longitudinal Study of Cognition in Normal Healthy Old Age (UMLCHA) cohort.
The study shows that meal timing shifts with older age, particularly toward later breakfast and dinner, a delayed eating midpoint, and a shorter eating window. Later breakfast timing is associated with greater physical and psychological illness, multimorbidity, evening chronotype genetic profiles, and increased mortality risk. These findings suggest that shifts in meal timing may reflect underlying health and aging processes in older adults.
Methods
University of Manchester Longitudinal Study of Cognition in Normal Healthy Old Age
The University of Manchester Longitudinal Study of Cognition in Normal Healthy Old Age (UMLCHA) recruited 6375 individuals aged 42–94 years old from Newcastle and Manchester, UK, starting in 1983 through 199324. All participants were followed until 2017, and therefore follow-up durations varying based on each participant’s enrollment date. Over the course of the study, participants were invited to complete optional questionnaires including those on sociodemographic, health status, and lifestyle19. Between 1999 and 2004, a subset of participants also provided whole blood samples. The study was approved by the University Research Ethics Committee at the University of Manchester (Ref: 2021-11274-17829), and all participants gave written informed consent prior to study procedures.
Assessment of meal timing and sleep habits
The Personal Details Questionnaire, a cohort-specific survey that included questions on meal and sleep habits, sociodemographics, occupation, and subjective health, consistent with those used in other cohorts, was administered to participants up to five times. The initial administration occurred in person at enrollment, beginning in 1983 (baseline). The questionnaire was subsequently readministered to enrolled participants by mail at multiple points during the study: between 1984 and 1996 (second administration), 2001 and 2003 (third administration), 2007 (fourth administration), and 2010 (fifth and final administration). Due to variation in enrollment dates and follow-up participation, not all participants completed every questionnaire.
In the Personal Details Questionnaire, participants responded to questions pertaining to the timing of meals and sleep. Participants responded to the question, “What time do you eat [breakfast/lunch/dinner]?” In addition, participants responded to the questions, “Generally, at what time do you [go to bed at night/get up in the morning]?” and “On average, how many hours of sleep do you get every night?” Responses were used to calculate the time interval between waking and breakfast, the time interval between dinner and bed, the time interval between breakfast and dinner (i.e., daily eating window), and the midpoint between breakfast and dinner (i.e., eating midpoint).
Mortality and other measures
Mortality data were obtained from the England NHS Digital death registry from the NHS England’s Secure Data Environment service for England (https://digital.nhs.uk/services/secure-data-environment-service). Access to the data was granted following approval of a data access request in adherence to the NHS Digital’s data governance and security protocols. The record data included information on the date of death up until August 2017.
At baseline, participants reported demographic information such as birth year, sex, socioeconomic status (based on the Standard Occupational Classification 2000), and education level (categorized using the International Standard Classification of Education 1997). On each of the five assessment occasions, participants also provided updates on their employment status (full-time, part-time, or unemployed/retired), smoking status, marital status, alcohol consumption, and subjective health status (rated on a scale from 1 (very bad) to 5 (very good)). Clinical measurements, including height and weight, were collected in-person for a subset of participants (n = 493 of the analytical sample). Through the repeated Personal Details Questionnaire, participants also reported daily cumulative time spent preparing meals (in hours) and whether they experienced any difficulty in meal preparation (yes/no). In addition, during their enrollment, participants completed the Pittsburgh Sleep Quality Index (PSQI) once and responses to the survey were used to compute scores reflecting sleep quality based on accepted thresholds25.
To assess symptoms of physical and psychological illness (i.e., morbidity), the Cornell Medical Index (CMI) was administered on four occasions, covering 19 general areas of symptomatology26. A participant was considered to have a health problem if they responded “yes” to any question corresponding to a specific health category within the CMI. A multimorbidity index was calculated by summing the number of health conditions reported by participants at each assessment.
Polygenic scores
In a subset of participants, DNA was extracted from blood samples collected between 1999 and 2004, and genotyping was performed at the Wellcome Trust Clinical Research Facility Genetics Core, Western General Hospital, Edinburgh, using the Illumina610-Quadv1 chip (Illumina, San Diego, CA). Imputation was performed using the Haplotype Reference Consortium panel (GRCh37-hg19 genome assembly)7. Standard quality control was conducted: variants with >20% missing genotypes, variants not in Hardy-Weinberg Equilibrium, and individuals with a SNP call rate <80% were removed. Variants with frequency <0.1% were further excluded24. Population substructure correction was performed by calculating the principal components of ancestry using TRACE and the Human Genome Diversity Project27,28.
Genome-wide polygenic scores for eveningness (i.e., later chronotype) and obesity (i.e., higher BMI), scores with known associations with meal timing29,30, were calculated for each participant using PRS-CS (Polygenic Risk Score–Continuous Shrinkage), a Bayesian regression framework that places a continuous shrinkage prior on SNP effect sizes31. The UK Biobank EUR-ancestry linkage disequilibrium (LD) panel was used as the reference. The publicly available UK Biobank linkage disequilibrium matrices were obtained from Broad Institute’s Amazon repository (s3://broad-alkesgroup-ukbb-ld/UKBB_LD/). Effect estimates for the polygenic score were derived from the large genome-wide association study for evening preference in UK Biobank participants of European ancestry and the meta-analysis of genome-wide association studies for BMI in approximately 700,000 individuals of European ancestry by the Genetic Investigation of ANthropometric Traits (GIANT) consortium32,33. Each polygenic score was standardized to have a mean of 0 and a standard deviation of 1.
Statistics and reproducibility
Participants who provided responses to all meal and sleep timing questions at baseline and had at least one additional meal timing response at any of the four subsequent occasions were included in the analysis. Descriptive statistics are presented as mean and standard deviations for continuous variables and frequency and percentages for categorical variables.
Changes in meal timing variables (dependent variables) with age (time-varying predictor) were assessed using linear mixed-effects models, as conducted previously34. An interaction term between age and wave was included to account for varying effects of age across different waves. Participant ID was also included as a random intercept to account for repeated measurements. The basic model (Model 1) adjusted for sex as a time-independent variable. The full model (Model 2) included additional time-independent variables such as socioeconomic status and education level, and time-dependent variables including sleep duration, employment status, smoking status, marital status, alcohol consumption, and subjective health status. Effects are reported per 10-years increase in age, with corresponding regression coefficients and 95% confidence intervals. For time-dependent variables with missing data in later cycles, values were carried forward once from previous cycles using the last observation carried forward approach. If still missing after the first carry-forward, the data were treated as missing (<5% missingness).
Latent class analysis was performed for meal timing to identify subgroups with distinct meal timing trajectories using LatentGOLD 5.1 (Statistical Innovations, Belmont, MA). The best-fitting model was determined by evaluating the average latent class posterior probability, Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) with each added subgroup, ensuring that each subgroup included at least 5% of participants, and demonstrated meaningful distinction between subgroups (Supplementary Table 1). A two-cluster model was identified as the best fit. Meal timing variables were compared between the latent classes. The associations between the latent classes with the meal timing variables were also assessed using linear mixed-effects models as previously described.
The associations between physical and psychological illness (derived from the CMI) and meal-related behaviors (daily cumulative hours spent preparing meals and difficulty in meal preparation) with meal timing variables were analyzed using linear mixed-effects models, accounting for the covariates mentioned earlier with the inclusion of the age by wave interaction term in both models 1 and 2. Associations between PSQI score (sleep quality) with meal timing variables were analyzed using linear regression models, accounting for the same covariates. Linear mixed-effects models were also used to quantify the relationship between the scaled polygenic scores and meal timing variables accounting for the covariates mentioned above in the subset of 1226 participants with genetic data and 5 principal components of ancestry to account for population substructure. As confirmatory analyses, the polygenic score for evening chronotype was tested for associations with sleep midpoint, previously described as the midpoint between bed and wake times19, and the polygenic score for obesity was tested for associations with measured BMI. In sensitivity analyses, all model 1 analyses were further adjusted for the polygenic score for evening chronotype.
Meal timing trajectories and their associations with all-cause mortality were assessed using mixed-effects Cox regression models. For participants who died during follow-up, the time variable was defined as the period from recruitment to the date of death. For surviving participants, the time variable was defined as the period from recruitment to August 2017. The basic model (Model 1) only adjusted for sex as a time-independent variable and age as a time-dependent variable, whereas the full model (Model 2) additionally included time-independent variables such as socioeconomic status and education level, and time-dependent variables such as sleep duration, smoking status, and alcohol consumption. Results are presented as hazard ratios and 95% confidence intervals. For the meal timing clusters, Kaplan-Meier survival curves were generated, and log-rank tests were performed.
Associations with a two-sided p value < 0.05 were considered statistically significant. All analyses were two-tailed and performed using R version 4.3.1 (The R Foundation for Statistical Computing Platform, 2023) and the latest version of RStudio (Posit Software, PBC, Boston, MA).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Results
Meal timing trajectories across the older adult lifespan
A total of 2945 community-dwelling older adults recruited from Manchester and Newcastle, United Kingdom were included and had available self-reported meal timing data upon enrollment (baseline) and at least one additional repeat assessment (n = 2181 / 272 / 316 / 176 with 2 / 3 / 4 / 5 responses, respectively). At baseline, participants had a mean age of 64.0 years (standard deviation (SD) = 6.6; range = 42—94), 71.5% were female, and 83.3% were unemployed (Table 1). Participants reported average times for breakfast, lunch, and dinner of 8:22 (SD 0:43), 12:38 (SD 0:30), and 17:51 (SD 0:53), respectively. On average, participants had breakfast 31 min (SD 29) after waking up and had dinner 5.38 h (SD 1.07) before going to bed.
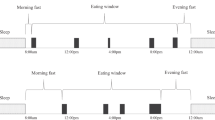
Older age was associated with later timing for breakfast in model 1 (Fig. 1a and Table 2). Each additional decade of aging was associated with a delay in breakfast of 7.94 min (95% CI: 5.56, 10.31). In model 2, the association remained significant, where each additional decade was associated with a delay in breakfast of 2.89 min (95% CI: 0.31, 5.46). Age trajectories were also evident for later midpoint of eating, shorter intervals from dinner to bed, and, in model 1 only, a shorter daily eating window. Lastly, an association with later dinner timing was observed only in model 2, where each additional decade of aging was associated with a delay in dinner of 3.67 min (95% CI: 0.6, 6.75).

Age-related changes in meal and bed times (a), and latent class differences in meal times and trajectory (b). The lines display model-predicted values from the linear mixed-effect models, with the shaded region indicating the 95% confidence interval of the estimates.
Latent class analysis of meal timing trajectories indicated heterogeneity in age-related changes in meal timing among older adults (Supplementary Tables 1 and 2). The analysis identified a two-cluster model as the best fit to capture the distinct meal timing patterns. The two clusters exhibited notable differences in their meal timing trajectories (Fig. 1b). The early eating subgroup (n = 1391) had consistently earlier meal times with aging, whereas the late eating subgroup (n = 1554) displayed generally later meal times with aging (Supplementary Table 3).
Longitudinal associations of physical and psychological illness, behaviors, and genetic profiles with changes in meal timing
To assess morbidity, participants were administered the Cornell Medical Index (CMI) on four occasions to report symptoms of physical and psychological illness26. Significant associations with meal timing were observed for both physical and psychological illnesses in linear mixed-effects models (Fig. 2, Supplementary Data 1 and 2). Among physical illnesses, associations were observed between having fatigue with both later breakfast timing and a shorter daily eating window. Having oral health problems was also linked to earlier dinner timing and a shorter daily eating window. Among psychological illnesses, associations were evident between depression and later breakfast time and a later eating midpoint, and between anxiety and a shorter daily eating window. Greater frequency of illness (i.e., hypochondria) was associated with later breakfast timing, a later eating midpoint, and a shorter eating window. Lastly, multimorbidity was also associated with later breakfast time, a later eating midpoint, and a shorter daily eating window. The associations remained largely unchanged after adjusting for lifestyle factors in model 2 (Supplementary Data 2) and the polygenic score for evening chronotype in sensitivity analysis (Supplementary Data 3).

Results are reported as regression coefficient (95% confidence interval) in minutes from model 1 adjusted for sex only. Positive coefficients indicate later meals; negative coefficients indicate earlier meals. Full association results are shown in tabular format in Supplementary Data 1.
Self-reported data on meal preparation behaviors and survey-derived sleep quality provided insight into additional lifestyle factors associated with meal timing trajectories. In linear mixed-effects models, longer meal preparation times were associated with a later dinner, a later eating midpoint, and a longer interval between waking and breakfast (model 2 only) (Supplementary Data 4). In addition, having difficulty preparing meals was associated with a later breakfast, a later eating midpoint, and a shorter daily eating window. In model 2, only the association with later breakfast remained significant. Lastly, higher PSQI score reflecting worse sleep quality was associated with a later breakfast and a shorter daily eating window in model 2 only (Supplementary Data 4).
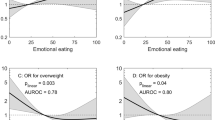
To further identify determinants of meal timing, the role of polygenic scores for evening chronotype and obesity, which have previously been linked to eating times in younger populations29,30, were further examined in a subset of 1226 participants with genetic data. In confirmatory analyses, there were associations between polygenic scores for evening chronotype with later sleep midpoint (Beta (95% CI) = 6.65 (4.84, 8.47) minutes per SD) and for obesity with higher BMI (Beta (95% CI) = 1.54 (1.18, 1.91) kg/m2 per SD) (Supplementary Data 5). The polygenic score for evening chronotype was associated with later meals and eating midpoint (Fig. 3 and Supplementary Data 5). Specifically, each standard deviation increase in the polygenic score for eveningness was associated with later meal times: breakfast was later by 7.20 min (95% CI: 5.07, 9.34), lunch by 3.10 min (95% CI: 1.72, 4.47), and dinner by 3.88 min (95% CI: 1.61, 6.15). The polygenic score for evening chronotype and obesity were both associated with shorter daily eating windows.

Associations are adjusted beta values reflecting difference in meal timing in minutes per standard deviation of the polygenic scores. Model 1 is only adjusted for sex and 5 principal components of ancestry to account for population substructure as a time-independent variable and age as a time-dependent variable; model 2 additionally included time-independent variables such as socioeconomic status and education level, and time-dependent variables such as sleep duration, employment status, smoking status, marital status, alcohol consumption, and subjective health status. Association results are shown in tabular format in Supplementary Data 5.
Meal timing and all-cause mortality
During a mean follow-up of 22.0 years (SD 8.4), 2361 deaths were recorded over a total of 63,388 participant-years based on survival data from the National Health Service (NHS) Digital death register. The 10-year survival rate was 86.7% for the late group compared to 89.5% for the early group. Kaplan–Meier survival estimates indicated that individuals with later eating had a shorter survival compared to those with early eating (Fig. 4). Meal timing trajectories and their relationship with all-cause mortality were assessed using mixed-effects Cox regression models (Table 3 and Supplementary Table 4). Each additional hour of later breakfast timing was associated with a 1.11 (95% CI: 1.03, 1.18) increase in odds of mortality in model 1, and a 1.08 (95% CI: 1.00, 1.17) increase in model 2 (Table 3).

Kaplan–Meier survival estimates are shown as solid lines, with shaded regions representing the 95% confidence intervals at each time point.
Discussion
Longitudinal data from a large cohort of community-dwelling older adults, followed for over 20 years, showed gradual shifts in meal timing with aging, specifically toward later breakfast, dinner, and eating midpoint and a shorter interval between dinner and sleep. The onset of physical and psychological illnesses including multimorbidity, challenges with meal preparation and worse sleep, and genetic predispositions partly contributed to the observed shifts in meal timing. Distinct meal timing trajectories, particularly those characterized by later breakfast, were associated with increased mortality risk.
There is growing evidence to suggest that eating behaviors, including eating times, shift with aging13,14,15,16,17. Few cross-sectional studies compared meal timing in older and younger adults, although with mixed results. For example, data from the National Health and Nutrition Examination Survey (NHANES) suggest that older adults skip breakfast less frequently and have a later eating midpoint compared to younger individuals14. Conversely, other studies from the US and Japan report earlier meal times in older adults compared to younger adults16,17. The present study extends these findings by providing longitudinal data with repeat assessments of meal timing showing that meal timing continues to change throughout older adulthood. Specifically, the data suggest later breakfast and dinner times and a later eating midpoint with age, while lunch timing remains stable likely due to limited variability in lunch schedules across participants35. Although the per-decade shifts in meal timing were modest, they accumulate to a more substantial difference (approximately 45 min for breakfast timing) when considered across the full age range of participants spanning over five decades. The concurrent assessment of bed and wake times with the timing of traditional meals allowed for other relevant meal timing measures to be examined in this study, such as the interval from wake-up to breakfast and from dinner to bedtime. Consistent with prior studies, the data suggest shorter intervals between dinner and bed with aging independent of sleep changes16.
Morbidity may contribute to changes in meal timing among older adults. The systematic analysis of 19 illnesses indicated notable associations for depression, anxiety, and fatigue, and declining oral health with later meals. Furthermore, multimorbidity is also associated with later eating. Late eating in younger and older adults has previously been implicated in obesity and other metabolic disorders such as diabetes8,15,36. Limited evidence also suggests that meal timing also impacts physical health in older adults. For example, in a larger observational study of older adults, later eating was associated with lower grip strength, and a shorter eating interval was associated with lower muscle mass12. In another study, short-term time-restricted eating in older adults did not lead to physical or mental fatigue37. Although the observational design cannot establish directionality, it is more likely that the onset of disease leads to shifts in meal timing rather than shifts in meal timing contributing to the onset of disease. Overall, the results suggest that age-related physical and psychological health factors, including worse sleep, may play a role in shaping meal timing in aging populations, with multimorbidity potentially exacerbating these changes.
Genetic profiles for evening chronotype and obesity have been previously implicated with meal timing including later breakfast and breakfast skipping29,30,38. The present findings are consistent with findings in younger adults, demonstrating robust associations between evening chronotype genetic profiles and later meal times. The genetic analyses also corroborates epidemiological data indicating later eating among evening-type older adults39. The findings do not suggest that obesity-implicated genetic variants that are known to influence eating behaviors such as satiety and taste preferences further influence eating times in older adults29. Associations between both evening chronotype and obesity genetic risks with shorter eating windows may indicate post-meal snacking behavior among individuals at higher genetic risk. Overall, these findings suggest that individuals with genetic predispositions toward evening chronotype may be at the highest risk for late eating behaviors.
In the present study, later breakfast is associated with an increased risk of mortality, although the association was attenuated when considering the effects of important confounders. This finding is consistent with a previous study showing associations between breakfast skipping and increased mortality in older adults40. No associations with mortality were evident for the timing of lunch or dinner, length of the eating window, or the proximity of meals to sleep. In addition, the late eating cluster was associated with a lower survival rate compared to the early eating cluster. Age-related changes in the microbiome are known to influence energy utilization and appetite, which may partially mediate the observed associations41.
Anorexia of aging is a prevalent geriatric syndrome, characterized by a loss of appetite and reduced food intake, and is associated with undernutrition42,43. Established causes of anorexia of aging are changes in oral health, alterations in chemosensory and gastrointestinal functions such as swallowing disorders, cognitive decline and dementia, social factors, and medication side effects that may alter taste and smell or induce dryness and constipation42,43. The present findings suggest that the onset of anorexia of aging may be also accompanied by shifts toward later meal times, particularly breakfast. However, given the modest effect sizes observed, established screening approaches for anorexia of aging, such as regular weight monitoring and dietary assessment, remain essential for tracking overall health decline in older adults. Aging is known to dampen the entraining effects of behavioral cues, such as meal timing, thereby reducing the sensitivity of peripheral tissues to nutrients44. Based on the present findings, gradual delays in meal timing with age may mediate the observed effect. The results support the hypothesis that maintaining consistent eating schedules, including breakfast times, could restore circadian rhythms in older adults45. Addressing the onset of pathologies such as depression and fatigue that may lead to meal delays may support robust rhythms in older adults.
A major strength of this study is the repeated assessment of meal timing in a large cohort of community-dwelling older adults (though most participants had only two assessments given the aging nature of this older adult cohort) allowing for the consideration of both inter- and intra-individual variation in meal timing patterns.
Additionally, the concurrent assessment of sleep and relevant sociodemographic factors allowed for the inclusion of other meal timing variables in the longitudinal analyses. However, several limitations should be noted. Currently, there are no standard methodologies or established variables for chrononutrition, making it difficult to compare results across studies and cohorts46. Furthermore, the study was unable to derive other common meal timing variables, such as eating frequency, meal timing variability, and the first and last eating occasions, which may capture snack consumption outside traditional meal times12. However, previous studies using 24-h recalls in older adults indicate that most tend to consume three primary meals, justifying the focus on the traditional meals in the analysis47. In addition, while some research suggests considerable day-to-day variation in meal timing among older adults48, others have not17. Therefore, the questions on mealtimes and bedtime routines may not accurately reflect participants’ actual behavioral patterns, and assumptions about typical eating habits based on other populations may not apply to the present sample. Additionally, meal frequency and skipping behaviors, areas of interest in older adults and chrononutrition, were not examined as missing meal timing data could have been misinterpreted as skipped meals. Moreover, the timing of specific nutrients, including protein content, which has been shown to associate with skeletal muscle mass in older adults when ingested before sleep, was not evaluated in this study49,50. Another limitation is the reliance on the CMI for capturing morbidity, which, although correlated with clinical diagnoses, may not identify asymptomatic conditions that could only be detected through laboratory tests or physical examinations51. The cohort recruited healthy, community-dwelling older adults of British European ancestry, which may limit the generalizability of the findings. Non-random attrition and dropout effects in this older adult population may have introduced bias because participants with poorer health may have fewer repeated assessments52. Lastly, although our models accounted for several potential confounders, they did not include physical activity, and residual confounding remains possible.
In summary, the findings suggest that meal timing shifts with aging and is associated with morbidity and mortality in older adults. Future research, including randomized controlled trials, is needed to explore the potential of meal timing as a strategy to promote longevity in aging populations.
Data availability
The data used in this manuscript from the Manchester Longitudinal Cognitive Ageing Cohort are not publicly available. However, they may be shared upon reasonable request and the completion of a Material Transfer Agreement. England NHS Digital death registry data used in this study are available in NHS England’s Secure Data Environment service for England, but as restrictions apply are not publicly available (https://digital.nhs.uk/services/secure-data-environment-service). Access to the NHS registry data can be requested by completing the Data Access Request application form via https://dataaccessrequest.hscic.gov.uk/. UK Biobank linkage disequilibrium matrices are publicly available at s3://broad-alkesgroup-ukbb-ld/UKBB_LD/. The Source data for Fig. 2 is in Supplementary Data 1 and the Source data for Fig. 3 is in Supplementary Data 5.
Code availability
The code used in this manuscript from the Manchester Longitudinal Cognitive Ageing Cohort are not publicly available. However, they may be shared upon reasonable request and the completion of a Material Transfer Agreement.
References
Dashti, H. S. et al. Advancing chrononutrition for Cardiometabolic Health: a 2023 National Heart, Lung, and Blood Institute Workshop report. J. Am. Heart Assoc. 14, e039373 (2025).
Johnston, J. D., Ordovás, J. M., Scheer, F. A. & Turek, F. W. Circadian rhythms, metabolism, and chrononutrition in rodents and humans. Adv. Nutr. 7, 399–406 (2016).
Cornelissen, G. When you eat matters: 60 years of Franz halberg’s nutrition chronomics. Open Nutraceuticals J. 5, 16–44 (2012).
Arble, D. M., Bass, J., Laposky, A. D., Vitaterna, M. H. & Turek, F. W. Circadian timing of food intake contributes to weight gain. Obesity 17, 2100–2102 (2009).
Dashti, H. S. et al. Late eating is associated with cardiometabolic risk traits, obesogenic behaviors, and impaired weight loss. Am. J. Clin. Nutr. 113, 154–161 (2021).
McHill, A. W. et al. Later circadian timing of food intake is associated with increased body fat. Am. J. Clin. Nutr. 106, 1213–1219 (2017).
Garaulet, M. et al. Timing of food intake predicts weight loss effectiveness. Int. J. Obes. 37, 604–611 (2013).
Vujović, N. et al. Late isocaloric eating increases hunger, decreases energy expenditure, and modifies metabolic pathways in adults with overweight and obesity. Cell Metab. 34, 1486–1498.e7 (2022).
Garaulet, M. et al. Interplay of dinner timing and MTNR1B type 2 diabetes risk variant on glucose tolerance and insulin secretion: a randomized crossover trial. Diab. Care 45, 512–519 (2022).
Maywood, E. S. et al. Disruption of peripheral circadian timekeeping in a mouse model of Huntington’s disease and its restoration by temporally scheduled feeding. J. Neurosci. 30, 10199–10204 (2010).
St-Onge, M.-P. et al. Meal timing and frequency: implications for cardiovascular disease prevention: a scientific statement from the American Heart Association. Circulation 135, e96–e121 (2017).
Mao, Z. et al. The association between chrononutrition behaviors and muscle health among older adults: the study of muscle, mobility and aging. Aging Cell 23, e14059 (2024).
Almoosawi, S. et al. Chronotype: implications for epidemiologic studies on chrono-nutrition and cardiometabolic health. Adv. Nutr. 10, 30–42 (2019).
Kant, A. K. & Graubard, B. I. Within-person comparison of eating behaviors, time of eating, and dietary intake on days with and without breakfast: NHANES 2005-2010. Am. J. Clin. Nutr. 102, 661–670 (2015).
Bernardes da Cunha, N., Teixeira, G. P., Madalena Rinaldi, A. E., Azeredo, C. M. & Crispim, C. A. Late meal intake is associated with abdominal obesity and metabolic disorders related to metabolic syndrome: a chrononutrition approach using data from NHANES 2015-2018. Clin. Nutr. 42, 1798–1805 (2023).
Takahashi, M. et al. Association between circadian clock gene expressions and meal timing in young and older adults. Chronobiol. Int. 40, 1235–1243 (2023).
de Castro, J. M. Age-related changes in the social, psychological, and temporal influences on food intake in free-living, healthy, adult humans. J. Gerontol. A Biol. Sci. Med. Sci. 57, M368–77 (2002).
Fischer, D., Lombardi, D. A., Marucci-Wellman, H. & Roenneberg, T. Chronotypes in the US—influence of age and sex. PLoS ONE 12, e0178782 (2017).
Didikoglu, A., Maharani, A., Payton, A., Pendleton, N. & Canal, M. M. Longitudinal change of sleep timing: association between chronotype and longevity in older adults. Chronobiol. Int. 36, 1285–1300 (2019).
Fávaro-Moreira, N. C. et al. Risk factors for malnutrition in older adults: a systematic review of the literature based on longitudinal data. Adv. Nutr. 7, 507–522 (2016).
Si Hassen, W. et al. Associations between transition to retirement and changes in dietary intakes in French adults (NutriNet-Santé cohort study). Int. J. Behav. Nutr. Phys. Act. 14, 71 (2017).
Lee, B. Y. et al. Research gaps and opportunities in precision nutrition: an NIH workshop report. Am. J. Clin. Nutr. 116, 1877–1900 (2022).
Dashti, H. S., Scheer, F. A. J. L., Saxena, R. & Garaulet, M. Timing of food intake: identifying contributing factors to design effective interventions. Adv. Nutr. 10, 606–620 (2019).
Didikoglu, A. et al. Associations between chronotype and employment status in a longitudinal study of an elderly population. Chronobiol. Int. 39, 1118–1131 (2022).
Buysse, D. J., Reynolds, C. F. 3rd, Monk, T. H., Berman, S. R. & Kupfer, D. J. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 28, 193–213 (1989).
Brodman, K. & Erdmann, A. J. Jr. The Cornell medical index; a adjunct to medical interview. J. Am. Med. Assoc. 140, 530–534 (1949).
Wang, C., Zhan, X., Liang, L., Abecasis, G. R. & Lin, X. Improved ancestry estimation for both genotyping and sequencing data using projection procrustes analysis and genotype imputation. Am. J. Hum. Genet. 96, 926–937 (2015).
Cann, H. M. et al. A human genome diversity cell line panel. Science 296, 261–262 (2002).
Dashti, H. S. et al. Polygenic risk score for obesity and the quality, quantity, and timing of workplace food purchases: a secondary analysis from the ChooseWell 365 randomized trial. PLoS Med. 17, e1003219 (2020).
Dashti, H. S. et al. Chronotype polygenic score and the timing and quality of workplace cafeteria purchases: secondary analysis of the ChooseWell 365 randomized controlled trial. Curr. Dev. Nutr. 7, 100048 (2023).
Ge, T., Chen, C.-Y., Ni, Y., Feng, Y.-C. A. & Smoller, J. W. Polygenic prediction via Bayesian regression and continuous shrinkage priors. Nat. Commun. 10, 1776 (2019).
Jones, S. E. et al. Genome-wide association analyses of chronotype in 697,828 individuals provides insights into circadian rhythms. Nat. Commun. 10, 343 (2019).
Yengo, L. et al. Meta-analysis of genome-wide association studies for height and body mass index in ∼700000 individuals of European ancestry. Hum. Mol. Genet. 27, 3641–3649 (2018).
Didikoglu, A. et al. Longitudinal sleep efficiency in the elderly and its association with health. J. Sleep. Res. 29, e12898 (2020).
Huseinovic, E. et al. Timing of eating across ten European countries—results from the European Prospective Investigation into Cancer and Nutrition (EPIC) calibration study. Public Health Nutr. 22, 324–335 (2019).
Carew, A. S. et al. Prospective study of breakfast frequency and timing and the risk of incident type 2 diabetes in community-dwelling older adults: the Cardiovascular Health Study. Am. J. Clin. Nutr. 116, 325–334 (2022).
Anton, S. D. et al. The effects of time restricted feeding on overweight, older adults: a pilot study. Nutrients 11, 1500 (2019).
Lopez-Minguez, J. et al. Heritability of the timing of food intake. Clin. Nutr. 38, 767–773 (2019).
Suh, S. et al. Chronotype differences in health behaviors and health-related quality of life: a population-based study among aged and older adults. Behav. Sleep. Med. 15, 361–376 (2017).
King, D. E. & Xiang, J. A relationship between mortality and eating breakfast and fiber. J. Am. Board Fam. Med. 34, 678–687 (2021).
Ghosh, T. S., Shanahan, F. & O’Toole, P. W. The gut microbiome as a modulator of healthy ageing. Nat. Rev. Gastroenterol. Hepatol. 19, 565–584 (2022).
Aprahamian, I. et al. Anorexia of aging: an international assessment of healthcare providers’ knowledge and practice gaps. J. Cachexia Sarcopenia Muscle 14, 2779–2792 (2023).
Volkert, D. et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 38, 10–47 (2019).
Mattis, J. & Sehgal, A. Circadian rhythms, sleep, and disorders of aging. Trends Endocrinol. Metab. 27, 192–203 (2016).
Kessler, K. & Pivovarova-Ramich, O. Meal timing, aging, and metabolic health. Int. J. Mol. Sci. 20, 1911 (2019).
Gioia, S. C. et al. How accurately can we recall the timing of food intake? A comparison of food times from recall-based survey questions and daily food records. Curr. Dev. Nutr. 6, nzac002 (2022).
Engelheart, S., Brummer, R. J. & Bertéus Forslund, H. Meal patterns in relation to energy and protein intake in older adults in home health care. Clin. Nutr. ESPEN 35, 180–187 (2020).
van Egmond, L. T., C Moulin, T., Schiöth, H. B., Cederholm, T. & Benedict, C. Meal timing and subjective sleep disturbances in older men. Exp. Gerontol. 141, 111089 (2020).
Kouw, I. W. et al. Protein ingestion before sleep increases overnight muscle protein synthesis rates in healthy older men: a randomized controlled trial. J. Nutr. 147, 2252–2261 (2017).
Farsijani, S. et al. Relation between mealtime distribution of protein intake and lean mass loss in free-living older adults of the NuAge study. Am. J. Clin. Nutr. 104, 694–703 (2016).
Brodman, K., Erdmann, A. J. Jr, Lorge, I. & Wolff, H. G. Cornell Medical Index-Health Questionnaire. J. Abnorm. Psychol. https://doi.org/10.1037/t02140-000 (1949).
Rabbitt, P., Diggle, P., Holland, F. & McInnes, L. Practice and drop-out effects during a 17-year longitudinal study of cognitive aging. J. Gerontol. B Psychol. Sci. Soc. Sci. 59, P84–97 (2004).
Acknowledgements
This work was supported by the National Institute of Health [grant number R00HL153795 to H.S.D.]. The authors thank the research participants who contributed to this research.
Author information
Authors and Affiliations
Contributions
H.S.D. and A.D. contributed to the conception/design of the research; H.S.D., C.L., H.D., A.S., A.P., A.M., and A.D. contributed to the acquisition, analysis, and interpretation of the data; H.S.D., C.L., and A.D. drafted the manuscript; all authors critically revised the manuscript; and H.S.D. agrees to be fully responsible for ensuring the integrity and accuracy of the work. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Medicine thanks Rodrigo Chamorro and the other anonymous reviewers for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dashti, H.S., Liu, C., Deng, H. et al. Meal timing trajectories in older adults and their associations with morbidity, genetic profiles, and mortality. Commun Med 5, 385 (2025). https://doi.org/10.1038/s43856-025-01035-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-025-01035-x
