
Abstract
Chronic hepatitis B (CHB) infection and metabolic dysfunction-associated steatotic liver disease (MASLD) are important contributors to the growing worldwide burden of liver disease. There is limited understanding regarding the interaction between CHB and MASLD. This is a consequence of the changing terminology for liver disease, inconsistent application of diagnostic tools, and poor understanding of global populations. In this review, we collate data on the use of diagnostic tests for identifying MASLD and associated liver inflammation or fibrosis in people living with CHB. We advocate for improved consensus on diagnosis, evidence-based monitoring and risk stratification, enhanced access to interventions and reduced health inequity.
Similar content being viewed by others


Introduction
Epidemiology and disease burden
Chronic liver disease is a substantial contributor to global mortality, with causes that include viral hepatitis infection and metabolic liver disease1. Chronic hepatitis B (CHB) is responsible for an estimated 1.1 million deaths per year2, despite the long-standing availability of a cheap, safe, robust vaccine and generic suppressive antiviral treatment. For people living with CHB, the cumulative lifetime incidence of primary hepatocellular carcinoma (HCC) is ~20% and for cirrhosis is ~40%, but with substantial heterogeneity3,4.
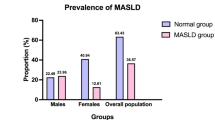
The contribution of metabolic dysfunction-associated liver disease (MASLD) to morbidity and mortality is also increasing worldwide, with over one billion people now living with overweight and obesity, and >800 million with diabetes5,6. As the impact of metabolic disease on liver outcomes is emerging, it is estimated that 3% of people living with MASLD will develop major liver-related complications over 20 years7. MASLD is also associated with ~1.5-fold increased risk of fatal and non-fatal cardiovascular events, 3-fold higher risk of developing chronic kidney disease, and increased risk of extrahepatic cancers5. Importantly, the prevalence of metabolic conditions is climbing in regions with high CHB endemicity, for example, in African, eastern Mediterranean, and western Pacific regions8. This critical nexus between CHB and MASLD will undoubtedly alter the epidemiology and morbidity of these conditions worldwide (Fig. 1).

Terminology and definitions
The term MASLD was introduced in 20239 to replace potentially pejorative or stigmatising language in previous definitions, which included reference to ‘alcoholic’ and ‘fatty’ liver disease. Diagnosis of MASLD requires identification of steatotic liver disease together with at least one cardiometabolic factor (hypertension, diabetes, dyslipidaemia, or obesity). Relevant thresholds for the use of cardiometabolic factors in the diagnosis of MASLD were agreed via a Delphi consensus process, largely based on the existing definition of metabolic syndrome9,10 (Fig. 2). This standardisation of terminology simplifies approaches to diagnosis and management and improves consistency of data collection as new therapeutics emerge. For consistency, we use the term MASLD throughout this review, even when referencing literature published prior to 2023, which uses older terminology (in contrast, in the Supplementary Tables 1−5, we use the original terms used by each article). In parallel with shifts in the MASLD field, the CHB landscape is changing, as there has been a move away from complicated classification systems and definitions, aiming to develop simplified practical approaches to diagnosis and risk-assessment, which will support more equitable access to interventions and treatment2. CHB refers to hepatitis B virus (HBV) infection, which has persisted for longer than six months, based on the presence of HBV surface antigen, HBsAg, and/or HBV DNA in peripheral blood. The term ‘‘person/people living with HBV’’ (PLWHB) is used where possible to emphasise person-centred language. Clearance of hepatitis B surface antigen (HBsAg) in the context of CHB is termed ‘functional cure’.

Metabolic dysfunction Associated Steatotic Liver Disease (MASLD) replaces prior terminology of ‘metabolic dysfunction-associated fatty liver disease’ (MAFLD) and ‘non-alcoholic fatty liver disease’ (NAFLD)9. Although definitions have changed, there is high concordance between MASLD and NAFLD107. Metabolic dysfunction-associated steatohepatitis (‘MASH’) is defined as MASLD with liver inflammation and/or fibrosis. Created in BioRender. Martyn, E. (2026) https://BioRender.com/yv9c4yy. BMI body mass index, CRP C-reactive protein, FPG fasting plasma glucose, HAART highly active antiretroviral therapy, HbA1c haemoglobin A1c, HDL high density lipoprotein, HBV hepatitis B virus, HOMA-IR homeostasis model assessment of insulin resistance score, MetALD metabolic dysfunction-associated steatotic liver disease with moderate alcohol consumption, OGTT oral glucose tolerance test, WC waist circumference. MAFLD cut-offs: BMI ≥ 25 kg/m2 (WC ≥ 25 kg/m2 Asian population); Type 2 diabetes diagnosed ‘‘according to widely accepted international criteria’’; WC Caucasian: ≥102 cm (male)/88 cm (female), Asian: ≥90 cm (male)/80 cm (female); BP ≥ 130/85 or treatment for hypertension; Prediabetes HbA1c 39–47 mmol/mol; Triglycerides ≥1.7 mmol/L; HDL-cholesterol ≤ 1.0 mmol/L (male), ≤1.3 mmol/L (female); HOMA-IR ≥ 2.5; CRP > 2 mg/L9,47,108.
Challenges for the field
To date, algorithms for the classification of hepatic steatosis may lead to inconsistencies, due to high population heterogeneity and complex overlapping risk factors for the evolution of liver disease, which include genetics, environment, diet, socioeconomic factors, and the influence of migration on risk11. It is also notable that the evidence used to establish thresholds is not representative of all populations, with different tools used according to location and resources, and scarce data from World Health Organization (WHO)Africa and Eastern Mediterranean regions (where MASLD and CHB are significant public health threats) (Supplementary Table 1). Insufficient data from resource-constrained settings reflecting key populations contributes to gaps in our understanding of epidemiology, clinical impact, and public health implications of the MASLD/CHB interplay12,13. Thus, the field is complicated by heterogeneous (and in some cases, conflicting) data. Despite increasing evidence informing diagnosis, treatment, and public health interventions for both CHB and MASLD, profound health inequities persist.
Aims of the review
In this narrative review, we consider the diagnosis and risk assessment of MASLD in PLWHB. Our aim is to summarise existing tools and evidence, and to highlight the need for concordance in the use and interpretation of diagnostic tests, with special emphasis on those that can be made accessible across diverse settings to facilitate better assessment and provision of evidence-based healthcare. By unifying classification and improving understanding of the intersection of these two important conditions, we can advance an understanding of the biology, clinical implications and treatment pathways, tackle health inequities, and identify areas for specific action.
Evidence for diverse outcomes in PLWHB and MASLD
To date, the impact of MASLD on liver disease and viral outcomes in PLWHB has been explored in 12 systematic reviews14,15,16,17,18,19,20,21,22,23,24, which collectively incorporate data from 178 studies (Table 1). Despite the increasing body of data, conflicting evidence associates MASLD with either increased or decreased risk of the development of chronic liver disease, cirrhosis, HCC, and poor treatment responses in PLWHB (Table 1, Fig. 3). The reasons behind these conflicting findings are likely to be multifactorial. One possible contributing factor is the heterogeneity of studies included in the meta-analyses. For example, older definitions of metabolic or fatty liver disease (Fig. 2), different methods of MASLD diagnosis (e.g., imaging, biopsy, non-invasive serum-based scores), different populations, and varied study designs (e.g., cohort vs. cross-sectional) (Table 1). Another possible explanation is that risk factors have a differential impact on outcomes in CHB, with cardiometabolic factors having a dose-dependent adverse effect, while steatotic liver disease may have a protective effect25,26,27. The challenge of accurately estimating the individual causal effect estimates of these interrelated factors using routinely collected clinical data likely contributes to current ambiguity in the literature.

-- No impact on outcome, ↑ outcome increased in people living with CHB and MASLD compared to CHB alone, ↓ outcome decreased in people living with CHB and MASLD compared to CHB alone. The first author of the meta-analysis and the year published are stated. A list of these meta-analyses is presented linked to full citations in Table 1.
One consistent (albeit perhaps unexpected) observation is that functional cure occurs more frequently in the presence of MASLD17,19. Hypothesised mechanisms for this increased chance of HBsAg loss include apoptosis of steatotic HBV-infected hepatocytes, fatty acid inhibition of HBsAg secretion, and increased MASLD-related inflammation boosting immune-related HBsAg seroclearance28,29,30,31. However, these mechanisms are speculative, and more robust experimental evidence is required.
Outcomes of CHB are known to be influenced by individual attributes (age at infection, sex, genetics), infection attributes (HBV genotype, e-Antigen status, viral load), comorbidity including coinfections (HIV, hepatitis D virus), and antiviral treatment, all of which are reflected in clinical practice guidelines2,32,33. New nomenclature recognises the need to identify liver inflammation in the presence of MASLD (termed metabolic dysfunction-associated steatohepatitis, ‘MASH’; Fig. 2)34,35, irrespective of the presence or absence of CHB, although it is the severity of fibrosis rather than inflammation that is associated with long-term outcomes36. On these grounds, there is particular focus on identifying MASH with fibrosis (‘at-risk MASH’), to inform earlier intervention or enhanced monitoring, and to identify a population of interest for clinical trials.
Assessment of MASLD in PLWHB
The conventional gold standard for diagnosis of steatotic liver disease (SLD) and fibrosis/cirrhosis is histopathological examination of a liver biopsy (Supplementary Table 2), with steatotic liver disease defined by >5% of hepatocytes containing fat deposition, and graded as S1, S2 or S3 based on fat deposition in 5–33%, 34–66%, and >66% of hepatocytes, respectively37. However, a biopsy samples only a tiny fragment of liver tissue, requires expert operators, is costly, and associated with rare but important complications, which means it should be undertaken in a specialist centre with clinical expertise on site.
To reduce risk and improve access, there is a move towards non-invasive tests (NITs), which can be made safely and universally accessible12,38. NIT results can be incorporated into algorithms to identify individuals at the highest risk of complications (including identifying selected individuals who may benefit from biopsy, in situations where this can be accessed). However, the coexistence of CHB and MASLD may affect NIT performance, and many MASLD NITs were developed and validated in studies that excluded CHB.
Imaging modalities that detect fibrosis and steatosis
Ultrasound and magnetic resonance imaging (MRI) are the two main modalities used to assess liver steatosis and fibrosis (Table 2). To assess steatosis, the echogenicity of the liver and renal parenchyma can be compared, with increased hepatic echogenicity corresponding to steatosis. Quantitative scores can be derived based on attenuation of the ultrasound beam as it passes through liver tissue, for example, by controlled attenuation parameter (CAP), which was first validated in humans in 201039. The most widely used ultrasound technology for liver stiffness measurement uses vibration-controlled transient elastography (VCTE). To measure VCTE, a mechanical pulse is transmitted through the liver, producing a shear wave that is converted into a quantitative value40, which is used to quantify and grade fibrosis. This shear wave is also influenced by the presence of inflammation. Both CAP and VCTE are most widely available through hardware produced by FibroscanTM (Echosens, France), although new tools are coming onto the market.
CAP/VCTE measurements of steatosis and liver stiffness have moderate-good accuracy compared to biopsy, and can be collected as quick, mobile, point-of-care tests by a wide range of personnel, as these measures require simple training and are not limited to expert healthcare workers. Despite these advantages, the global community is far from achieving equitable access, due to the high costs associated with procurement and maintenance of equipment, running expenses for annual recalibration, equipment upgrades, insurance, and employment and training of staff. Other limitations include reduced accuracy caused by factors which affect the elastic properties of the liver (e.g., transaminitis, congestive heart failure, post-prandial hyperaemia, cholestasis) and impede the transmission of shear waves (e.g., ascites)41. The standard M probe may not perform well in the context of overweight/obesity; therefore, FibroscanTM introduced the XL probe for use when the skin-to-capsule distance is >25 mm42.
Magnetic resonance spectroscopy - proton density fat fraction (MRS-PDFF) measures the different resonance frequencies between water and fat proton signals to calculate the proton density fat fraction, defined as the fraction of mobile protons in the liver attributable to fat43. MRS-PDFF is regarded as the non-invasive gold standard tool for fat quantification, but requires intensive data post-processing43,44. Magnetic resonance imaging - proton density fat fraction (MRI-PDFF) has been developed over the last 15 years and is based on the same underlying physics concepts as MRS-PDFF, but is more practical to measure in a clinical setting43. Magnetic resonance elastography (MRE) provides the benefit of assessing fibrosis across the whole liver45. To date, there is no evidence for the use of MRS/MRI-PDFF or MRE specifically for diagnosis of MASLD in PLWHB, and since this approach is not widely available or affordable, it remains in the research domain and is unlikely to move to routine clinical practice in the short-to-medium term.
Clinical and public health applications of CAP are currently limited by lack of consistency for CAP thresholds in comparison to assessment by biopsy (Fig. 4). European MASLD guidelines suggest distinct thresholds for distinguishing between steatosis grades (with cut-offs to distinguish S0/1, S1/2 and S2/3 thresholds), based on individual patient data meta-analysis including almost 4000 individuals with multi-aetiology liver disease, including >1000 PLWHB. In contrast, American guidelines advocate for a single rule-in CAP threshold, which sits in the European S3 category (based on a single-centre study with 119 participants, excluding PLWHB)46,47,48,49. The decision to select a single binary threshold recognises the limited accuracy of CAP to distinguish between steatosis grades, in particular S2–S350,51.

Criteria are shown using A histopathology and B non-invasive assessment by controlled attenuation parameter (CAP) measurement, based on (i) American guidelines (based on a single centre study with 119 patients, excluding people living with chronic hepatitis B (PLWHB)47,49, (ii) European guidelines (based on meta-analysis data including multi-aetiology liver disease, including over 1000 PLWHB52), and (iii) by meta-analysis data with viral-hepatitis specific thresholds49. Colours indicate grades of steatosis: Green—S0, Yellow—S1, Light red—S2, Dark red—S3. AUC area under the receiver operator curve, CAP controlled attenuation parameter, CHB chronic hepatitis B, CHC chronic hepatitis C, S1 mild hepatic steatosis (consistent with fat deposition in 5–33% of hepatocytes); S2—moderate hepatic steatosis (fat deposition in 34–66% of hepatocytes), S3—severe steatosis (fat depostion in >66% of hepatocytes).
Neither European nor American guidelines acknowledge the potential influence of CHB on CAP thresholds, although meta-analysis suggests that CHB independently lowers CAP scores when compared to other factors that influence liver pathology: −10 dB/M (95% confidence interval −17 to −3.6) compared to steatosis alone and −17.2 dB/M (95% CI −34.8 to 0.2) compared to alcohol-related liver disease49,52. When considering viral hepatitis alone (either CHB or chronic hepatitis C (CHC)), optimal CAP thresholds were lower than in studies considering mixed liver disease or MASLD alone (Fig. 4; Table 2; Supplementary Table 3).
A systematic review and meta-analysis conducted by the WHO led to a recommendation of elastography scores >7 kPa to detect liver fibrosis (≥F2) and >12.5 kPa to detect cirrhosis (F4) in CHB2. Some studies of MASLD in the context of CHB report that there is a higher elastography threshold to diagnose advanced fibrosis in people with CAP ≥ 268 dB/m compared to those with lower CAP scores (<268 dB/m) (8.8 vs. 7.0 kPa, respectively)53,54,55,56,57. This remains a topic of debate; while studies reaching this conclusion used only M probes to measure CAP, and excluded obesity, the use of the correct probe size may influence conclusions, and other studies have found no such relationship between CAP score and fibrosis threshold58.
While data to suggest variation in CAP and VCTE values according to disease threshold may create confusion, especially as there are global efforts to simplify CHB treatment guidelines, it is not possible to suggest a single cutoff threshold based on current data. Further research is needed to understand optimal thresholds for use in clinical practice.
Clinical and laboratory-based scores to identify liver disease
Simple scoring systems are based on routine laboratory parameters, typically using alanine transaminase (ALT), aspartate aminotransferase (AST), and platelet counts, with or without other demographic or biometric data. These approaches provide an assessment of liver health, aiming to identify and risk-stratify steatosis and/or fibrosis. However, there is variable data for the influence of CHB on the performance of these scores.
Steatosis scores are based on laboratory tests, anthropometric measurements, and cardiometabolic risk factors, e.g., NAFLD-liver fat score (NAFLD-LFS), fatty liver index (FLI), hepatic steatosis index (HSI), and others (summarised in Table 3; Supplementary Table 3). Most of these approaches have not been assessed in the context of CHB, which has been justified because CHB infection is not steatogenic. However, some validation has been undertaken in small studies of CHB59,60, and one score has been specifically proposed for use in the setting of CHB, the ‘steatosis index in patients with HBV’ (SIHBV). SIHBV was derived from a cohort of 182 Chinese individuals evaluated with liver biopsy, among whom 59 had >5% steatosis histologically60. In a validation cohort that incorporated liver biopsies, SIHBV outperformed other NITs and had a better sensitivity for diagnosing mild steatosis (<20%) than ultrasound. This approach was published in 2016, but has yet to be validated in larger cohorts, presumably reflecting the practical difficulty, cost, and ethical implications of undertaking a biopsy.
Fibrosis scores are summarised in Table 4. AST to platelet ratio index (APRI) > 0.5 is endorsed by WHO CHB treatment guidelines for the identification of individuals with ≥F2 fibrosis2, and Fibrosis-4 (Fib4) is recommended for use by primary care in European MASLD guidelines to identify F3 fibrosis47; in the presence of cardiometabolic risk factors, individuals with Fib4 > 1.3 require further non-invasive fibrosis testing while those with >2.67 may benefit from specialist hepatology assessment47. Enhanced liver fibrosis (ELF) is endorsed as an alternative to VCTE to assess for fibrosis in MASLD, and several studies have demonstrated good diagnostic performance in CHB; however, no studies have investigated accuracy for individuals living with concomitant MASLD/CHB47,61.
In studies that have compared serum-based fibrosis scores in PLWHB and MASLD, their performance is generally equivalent, even when compared across different metabolic liver disease definitions (NAFLD, MAFLD, and MASLD)53,62,63,64. One exception was in MASLD with moderate alcohol intake (MetALD), where gamma-glutamyl transpeptidase (GGT) to platelet ratio (GPR) and APRI had superior performance to Fib4 and VCTE64. In some datasets, GPR may perform better than other laboratory-based approaches in identifying advanced fibrosis (F3–F4)65. In a small Chinese study, GPR had a significantly higher AUC and negative predictive value to detect ≥F3 fibrosis compared to Fib-4 and APRI (Table 4, Supplementary Table 4)66. In some African cohorts, GPR has also outperformed other scores67,68. However, GPR remains understudied compared to other NITs and has poor performance in the setting of HBV/HIV coinfection, limiting widespread implementation69.
Approaches to combine appraisal of steatosis and fibrosis are required for diagnosis and evaluation of at-risk MASH (Supplementary Table 5). AGILE 3+ and AGILE 4 combine VCTE with sex, diabetes, ALT, AST, platelets ± age to detect advanced fibrosis and cirrhosis, respectively, in the context of suspected MASLD45. Real-world European studies find that AGILE 3+ and 4 scores have similar AUCs, but classify more people living with MASLD correctly (fewer indeterminate results) than VCTE alone, but this was not replicated in PLWHB70. However, in a Chinese cohort of PLWHB and MASLD, AGILE 3+ demonstrated better ability to correctly classify fibrosis (fewer indeterminates and higher proportion with advanced fibrosis ruled out) than VCTE alone63. The NAFLD fibrosis score (NFS), which aims to identify ≥F3 fibrosis, has been validated in multiple external cohorts71,72. The PPDHG Score was developed to detect fibrosis specifically in antiviral naïve PLWHB and MASLD to detect advanced fibrosis (≥F3). It had a higher AUC, sensitivity, and specificity than APRI, Fib4, and NFS in one multi-centre Chinese cohort73, but needs validation in other populations.
It must be recognised that many scores for assessment of fibrosis and/or steatosis may be specifically influenced by CHB due to their reliance on laboratory parameters which can be independently affected by HBV infection (e.g., liver enzymes and/or platelets). Other conditions that impact platelet count should also be considered, which vary widely by clinical population. Score performance can also potentially be negatively impacted as the number of cardiometabolic risk factors increases; this has been described for Fib4, APRI, and NFS54.
New technologies to diagnose MASLD
A machine learning approach, the ‘Gradient Boosting Classifier’ (GBC), has been trialled to predict MASH in a Chinese cohort of almost 2000 treatment-naïve PLWHB and biopsy-proven MASLD. This approach demonstrated a high AUC and negative predictive values across a training and two validation cohorts (Table 4)74. While these results are promising, vast data and computing requirements are likely to limit global application of the technique.
Other developing technologies, for example, metabolomics, can be applied to MASLD diagnosis75. The metabolomics-advanced steatohepatitis fibrosis score (MASEF) uses 12 lipids, together with BMI, AST and ALT to predict at-risk MASH (NAFLD Activity Score ≥4 and F ≥ 2 fibrosis) with an AUC 0.79 (95% CI 0.75–0.83), sensitivity 78%, specificity 65%, positive predictive value 48% and negative predictive value 73% in an international validation cohort76. However, this study did not assess MASEF performance in PLWHB. Similar to machine learning approaches, widespread roll-out of this technology is currently limited by the requirement for high-cost specialist equipment and expertise for data analysis, but the landscape is changing rapidly with a focus on delivery of more personalised risk stratification and management, supported by the potential for AI—approaches to analysis and interpretation of large ‘-omics’ data sets.
Refining diagnostic approach to the context and setting
The context in which clinical assessment takes place currently informs the choice of assessment strategy, for example, the extent to which imaging is available and affordable, both at individual and population levels in community settings, primary care, or through specialist services. MRI- and CT-based imaging techniques are the most accurate non-invasive methods to diagnose steatosis and fibrosis, with some arguing that MRI-PDFF should be the new gold standard for steatosis clinical trial endpoints77. However, most clinicians providing care for PLWHB will not have easy access to these imaging modalities, which are high-cost, available only in specialist centres, and reserved for specialist hepatology assessment.
Scores based on routinely collected clinical information are pragmatic and easy to use; however, they are limited by low specificity45. American and European guidelines suggest using serum-based NITs to screen for fibrosis in individuals at high-risk for MASLD in primary care47,78. To address the issue of diagnostic accuracy, two thresholds are adopted: a lower threshold with high specificity to rule-out fibrosis, and a higher threshold with greater sensitivity to rule-in fibrosis and qualify for immediate hepatology referral47. This leaves an “intermediate zone” of individuals, who should undergo a further NIT to risk-stratify them for hepatology referral or increased surveillance in primary care.
Although MASLD screening in the general population is not recommended47,78, there is an argument to screen for MASLD among PLWHB. Although only some studies suggest worse liver outcomes with concomitant MASLD and CHB, the 2024 WHO CHB treatment guidelines suggest MASLD as a potential antiviral criterion2. Extra-hepatic MASLD manifestations pose a significant health threat (e.g., increased risk of extra-hepatic cancer and cardiovascular events)5, and knowledge of a MASLD diagnosis presents an opportunity to optimise management of comorbidities and may help clinicians interpret persistently abnormal liver function tests. Moreover, ultrasound and FibroscanTM assessment are routine components of CHB monitoring in high-income settings; therefore, MASLD diagnosis will only require additional screening for cardiometabolic risk factors.
Access to ultrasound-based diagnostics is severely limited in low-income settings, and in this context, serum-based scores to screen for steatosis may be beneficial. Although specific tests to diagnose MASLD in PLWHB (e.g., SIHBV) show promising results, they have not been replicated outside a single study. Of all the serum-based NITs available to diagnose steatosis, HSI has the most evidence in CHB and uses commonly measured parameters; therefore, it may be a pragmatic suggestion in resource-constrained settings (Table 3, Supplementary Table 3). However, HSI still lacks validation outside of Asia and therefore must be interpreted with caution. Since APRI has been adopted by the WHO in HBV guidelines2, and has similar performance to Fib-4 in PLWHB/MASLD53,54,64,66,79,80,81, it is reasonable to use this to identify individuals at risk of fibrosis.
An example algorithm to screen for MASLD in viral hepatitis clinics, considering both high-income and resource-constrained settings, is suggested in Fig. 5. However, this is not intended to be a guideline for widespread adoption, rather an illustration of how NITs could be implemented based on the limited available evidence. Better evidence for the impact of MASLD on CHB outcomes and the cost-effectiveness of screening is required before implementation.

This is not intended to be a clinical guideline, as further evidence on the impact of MASLD on outcomes in PLWHB and cost-effectiveness analysis is required. Suggested controlled attenuated parameter (CAP) score thresholds are based on a large multi-aetiology analysis containing >1000 PLWHB52. The suggested hepatic steatosis index (HSI) threshold is based on a rule-in value from the original study109. The suggested aspartate transaminase-to-platelet-ratio (APRI) threshold based on World Health Organization (WHO) chronic hepatitis B (CHB) treatment guidelines2. The suggested vibration controlled transient elastography (VCTE) threshold based on European Association for the Study of the Liver (EASL) MASLD guidelines47. aThese tests may be more widely available alternatives in a resource-constrained setting. bCould also consider using Fibrosis-4 (Fib-4) instead of APRI, as they have similar diagnostic performance in PLWHB/MASLD. cConsider starting antiviral treatment. dPersistently elevated liver enzymes: alanine transaminase (ALT), gamma-glutamyl transferase (GGT), or aspartate transaminase (AST), e.g., above the upper limit of normal twice in 6 months, deteriorating fibrosis score, e.g., increase to >8 kPa or, if known fibrosis, increase >2 kPa since last fibroscan. Figure created in draw.io110. APRI aspartate aminotransferase to platelet ratio index, BMI body mass index, CAP controlled attenuation parameter, F female, GP general practitioner, HbA1c glycosylated haemoglobin, HDL high-density lipoprotein, HSI hepatic steatosis index, M male, MASLD metabolic dysfunction-associated steatotic liver disease, NIT non-invasive test, VCTE vibration controlled transient elastography.
A roadmap for the field
Establishing consistent thresholds and expanding data collection
Validating tests across different populations, and forming expert consensus on consistent approaches will help with understanding the epidemiology and identifying/grading MASLD in PLWHB. More work is needed to develop and validate consistent thresholds to standardise data collection, and evidence is needed to better represent diverse populations. Future studies will be enhanced by wider representation of different geographical settings, children and adolescents, and accounting for varied comorbidities and liver disease aetiologies, HBV genotype, diet/alcohol, host factors (e.g., genetics, immune response), and CHB treatment. Clinical studies have so far failed to elucidate a clear understanding of the MASLD/CHB relationship, and current in vivo and in vitro models for both CHB and MASLD have limitations to date. However, by harnessing the rapidly developing field of liver experimental models, for example, organoids using primary patient-derived hepatocytes, and precision-cut liver slices, there is increasing potential for more accurate models of disease.
Approaches to integrated healthcare modelled in other fields
The HIV field sets an example for holistic services that aim to integrate healthcare beyond the assessment and management of chronic viral infection, including long-term interventions to improve metabolic and cardiovascular health. This blueprint could be deployed by CHB services, following the mandate to ‘make every contact count’ and recognising the disadvantages and barriers some individuals may encounter in accessing consistent health care12,82. Basic management of cardiometabolic factors could be implemented through decentralised and multidisciplinary teams, for example, including dieticians, counsellors, and peer support workers. Acknowledging that such implementation comes with resource implications, cost-effectiveness analysis will be required to determine the optimum approaches in different settings, offsetting the fiscal investment in service provision against the costs saved in reducing long-term morbidity and mortality.
Changes in the therapeutic landscape
One major motivating factor for improved diagnostic assessment of liver disease due to CHB and MASLD is the rapidly transforming landscape of pharmacotherapy for both conditions. CHB management using long-term suppressive nucleos/tide analogue therapy is well established, overlapping with antiretroviral therapy and drawing on drugs with excellent safety profiles and a high genetic barrier to resistance. However, the landscape is fast changing, with the 2024 WHO CHB guidelines expanding and simplifying treatment criteria. For the first time, these include the presence of MASLD as a criterion for initiating antiviral therapy2, recognising the potential for enhanced risk. On this basis, many more PLWHB will be offered treatment, aligning with global targets for eliminating CHB as a public health threat. The field may change further as there is ongoing research to identify functional cure strategies83.
New therapies to treat people living with obesity and MASLD are licensed and being rapidly taken up. Semaglutide, a glucagon-like-peptide agonist (GLP-1 agonist), was recommended by the UK’s National Institute for Health and Clinical Excellence (NICE) in 2023 to treat people with a BMI ≥ 35 (or ≥30 with a weight-related co-morbidity)84. Resmetirom, the first pharmacological treatment for MASLD, was given accelerated approval by the United States Food and Drug Administration in March 2024 for at-risk MASH85. Although PLWHB are not currently eligible for this treatment, therapeutic recommendations will continue to change, and therefore, it is crucial to be able to diagnose MASLD accurately and consistently. The field will also be influenced according to the results of clinical trials exploring new drugs and combinations (e.g., dual GLP1/GL agonists, DGAT2i/ACCi combination86).
Recognising global disparities and advancing equitable solutions
There is a critical overlap between global regions with the biggest projected increase in obesity and diabetes, high CHB prevalence, and inequitable access to diagnostic methods and health infrastructure87,88. Although steatosis and fibrosis scores are useful and accessible tools, they are outperformed by imaging-based NITs. Therefore, there is a pressing need to address inequitable access to VCTE/CAP measurement. Approaches could include the introduction of subsidies that account for resource constraints, access to loan machines, sharing equipment between services, and/or between clinical and research programmes. New hardware that can measure CAP is emerging on the market, which should promote cost reductions and promise wider access, but may also bring challenges in quality and consistency.
In the light of the sudden, drastic withdrawal of US federal funding for overseas clinical and research programmes during 2025, coupled with significant cuts to foreign aid from several European countries, existing global health disparities are set to deepen89. This underscores the urgent need for healthcare and scientific communities to speak with a unified voice to retain global health funding and international research collaboration90. Improved diagnosis and research representation across diverse global settings will clarify the scope of the problem and support calls for expanding funding and investment needed to address the growing challenge posed by concomitant MASLD and CHB.
Conclusions
Many tools are available for clinical assessment of liver disease, but there is a pressing need to advance the field by unifying classification systems, expanding access, and collecting consistent data. These are urgent public health imperatives, given the increasing morbidity and mortality associated with both CHB and metabolic disease. There are substantial knowledge gaps regarding the mechanisms and impact of the interaction between these conditions in individuals and at a population level. As new tests, risk-stratification tools and algorithms emerge, their efficacy should be measured not only by their predictive accuracy in liver disease but also by their global accessibility and potential value in evaluating the impact of viral hepatitis infection on metabolic and cardiovascular healthcare.
References
GBD 2021 Causes of Death Collaborators Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 403, 2100–2132 (2024).
World Health Organization. Guidelines for the Prevention, Diagnosis, Care and Treatment for People with Chronic Hepatitis B Infection Available at: https://www.who.int/publications/i/item/9789240090903 (World Health Organization, 2024).
Chen, C.-J. & Yang, H.-I. Natural history of chronic hepatitis B REVEALed. J. Gastroenterol. Hepatol. 26, 628–638 (2011).
Su, C.-W., Liang, Y.-J. & Wu, J.-C. Unravelling the heterogeneous HCC risk in indeterminate chronic hepatitis B. Gut 74, 1873–1882 (2025).
Miao, L., Targher, G., Byrne, C. D., Cao, Y.-Y. & Zheng, M.-H. Current status and future trends of the global burden of MASLD. Trends Endocrinol. Metab. 35, 697–707 (2024).
World Health Organization. Diabetes (Fact sheet, 14 November 2024). WHO. Available at: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed 16 January 2026).
Hagström, H., Shang, Y., Hegmar, H. & Nasr, P. Natural history and progression of metabolic dysfunction-associated steatotic liver disease. Lancet Gastroenterol. Hepatol. 9, 944–956 (2024).
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in underweight and obesity from 1990 to 2022: a pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet 403, 1027–1050 (2024).
Rinella, M. E. et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J. Hepatol. 79, 1542–1556 (2023).
Grundy, S. M. et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 112, 2735–2752 (2005).
Lim, A. et al. Heterogeneity in the prevalence of cardiovascular risk factors by ethnicity and birthplace among Asian subgroups: evidence from the 2010 to 2018 National Health Interview Survey. J. Am. Heart Assoc. 13, e031886 (2024).
Martyn, E. et al. The forgotten people: Hepatitis B virus (HBV) infection as a priority for the inclusion health agenda. Elife 12, e81070 (2023).
Delphin, M. et al. Under-representation of the WHO African region in clinical trials of interventions against hepatitis B virus infection. Lancet Gastroenterol. Hepatol. 9, 383–392 (2024).
Machado, M. V., Oliveira, A. G. & Cortez-Pinto, H. Hepatic steatosis in hepatitis B virus infected patients: meta-analysis of risk factors and comparison with hepatitis C infected patients. J. Gastroenterol. Hepatol. 26, 1361–1367 (2011).
Jiang, D. et al. Concurrence and impact of hepatic steatosis on chronic hepatitis B patients: a systematic review and meta-analysis. Ann. Transl. Med. 9, 1718 (2021).
Zheng, Q. et al. Systematic review with meta-analysis: prevalence of hepatic steatosis, fibrosis and associated factors in chronic hepatitis B. Aliment. Pharmacol. Ther. 54, 1100–1109 (2021).
Mao, X. et al. Steatosis, HBV-related HCC, cirrhosis, and HBsAg seroclearance: a systematic review and meta-analysis. Hepatology 77, 1735–1745 (2023).
Zhou, R. et al. Clinical impact of hepatic steatosis on chronic hepatitis B patients in Asia: a systematic review and meta-analysis. J. Viral Hepat. 30, 793–802 (2023).
Wong, Y. J. et al. Impact of fatty liver on long-term outcomes in chronic hepatitis B: a systematic review and matched analysis of individual patient data meta-analysis. Clin. Mol. Hepatol. 29, 705–720 (2023).
Rui, F. et al. Antiviral therapy response in patients with chronic hepatitis B and fatty liver: a systematic review and meta-analysis. J. Viral Hepat. 31, 372–382 (2024).
Shen, S. & Pan, L. Effect of metabolic dysfunction‑associated fatty liver disease on the risk of hepatocellular carcinoma in patients with chronic hepatitis B: a systematic review and meta‑analysis. Exp. Ther. Med. 27, 99 (2024).
Han, C.-L. et al. The association of fatty liver and risk of hepatocellular carcinoma in HBV or HCV infected individuals: a systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 17, 189–198 (2023).
Liu, S.-Y., Wang, D., Liu, J., Yang, L.-P. & Chen, G.-Y. Influence of nonalcoholic fatty liver disease on response to antiviral treatment in patients with chronic hepatitis B: a meta-analysis. World J. Hepatol. 16, 465–476 (2024).
Zhu, Q. et al. Impact of metabolic dysfunction-associated fatty liver disease of varying severity on antiviral treatment outcomes and clinical prognosis in patients with chronic hepatitis B: a systematic review and meta-analysis. Infect. Dis. Ther. 14, 1599–1617 (2025).
Huang, S.-C. et al. All-cause and cause-specific mortality in patients with chronic hepatitis B and concurrent steatotic liver disease. J. Hepatol. 83, 43–51 (2025).
Huang, R. et al. Impacts of metabolic syndrome diseases on long-term outcomes of chronic hepatitis B patients treated with nucleos(t)ide analogues. Clin. Mol. Hepatol. 31, 1003–1017 (2025).
Huang, S.-C. et al. Pre-existing and new-onset metabolic dysfunctions increase cirrhosis and its complication risks in chronic hepatitis B. Am. J. Gastroenterol. 120, 401–409 (2025).
Zhang, J. et al. Chronic hepatitis B and non-alcoholic fatty liver disease: conspirators or competitors? Liver Int. 40, 496–508 (2020).
Tourkochristou, E., Assimakopoulos, S. F., Thomopoulos, K., Marangos, M. & Triantos, C. NAFLD and HBV interplay-related mechanisms underlying liver disease progression. Front. Immunol. 13, 965548 (2022).
Huang, S.-C. et al. Metabolic dysfunction-associated steatotic liver disease facilitates hepatitis B surface antigen seroclearance and seroconversion. Clin. Gastroenterol. Hepatol. 22, 581–590.e6 (2024).
Huang, S.-C. & Liu, C.-J. Chronic hepatitis B with concurrent metabolic dysfunction-associated fatty liver disease: challenges and perspectives. Clin. Mol. Hepatol. 29, 320–331 (2023).
European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 83, 502–583 (2017).
Terrault, N. A. et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 67, 1560–1599 (2018).
Sanyal, A. J. et al. Prospective study of outcomes in adults with nonalcoholic fatty liver disease. N. Engl. J. Med. 385, 1559–1569 (2021).
Dulai, P. S. et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: systematic review and meta-analysis. Hepatology 65, 1557–1565 (2017).
Hagström, H. et al. Fibrosis stage but not NASH predicts mortality and time to development of severe liver disease in biopsy-proven NAFLD. J. Hepatol. 67, 1265–1273 (2017).
Chowdhury, A. B. & Mehta, K. J. Liver biopsy for assessment of chronic liver diseases: a synopsis. Clin. Exp. Med. 23, 273–285 (2023).
Zelber-Sagi, S. et al. Food inequity and insecurity and MASLD: burden, challenges, and interventions. Nat. Rev. Gastroenterol. Hepatol. 21, 668–686 (2024).
Ferraioli, G. et al. Quantification of liver fat content with ultrasound: a WFUMB position paper. Ultrasound Med. Biol. 47, 2803–2820 (2021).
Afdhal, N. H. Fibroscan (transient elastography) for the measurement of liver fibrosis. Gastroenterol. Hepatol. (New York) 8, 605–607 (2012).
Tapper, E. B. & Loomba, R. Noninvasive imaging biomarker assessment of liver fibrosis by elastography in NAFLD. Nat. Rev. Gastroenterol. Hepatol. 15, 274–282 (2018).
de Lédinghen, V. et al. Diagnosis of liver fibrosis and cirrhosis using liver stiffness measurement: comparison between M and XL probe of FibroScan®. J. Hepatol. 56, 833–839 (2012).
Yoshizawa, E. & Yamada, A. MRI-derived proton density fat fraction. J. Med. Ultrason. (2001) 48, 497–506 (2021).
Reeder, S. B. Emerging quantitative magnetic resonance imaging biomarkers of hepatic steatosis. Hepatology 58, 1877–1880 (2013).
Zoncapè, M., Liguori, A. & Tsochatzis, E. A. Non-invasive testing and risk-stratification in patients with MASLD. Eur. J. Intern. Med. 122, 11–19 (2024).
Rinella, M. E. et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 77, 1797–1835 (2023).
European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD) & European Association for the Study of Obesity (EASO) EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). J. Hepatol. 81, 492–542 (2024).
Caussy, C. et al. Optimal threshold of controlled attenuation parameter with MRI-PDFF as the gold standard for the detection of hepatic steatosis. Hepatology 67, 1348–1359 (2018).
Karlas, T. et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. J. Hepatol. 66, 1022–1030 (2017).
European Association for the Study of the Liver. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis - 2021 update. J. Hepatol. 75, 659–689 (2021).
Eddowes, P. J. et al. Accuracy of fibroscan controlled attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver disease. Gastroenterology 156, 1717–1730 (2019).
Petroff, D. et al. Assessment of hepatic steatosis by controlled attenuation parameter using the M and XL probes: an individual patient data meta-analysis. Lancet Gastroenterol. Hepatol. 6, 185–198 (2021).
Li, Q., Huang, C., Xu, W., Hu, Q. & Chen, L. Accuracy of FibroScan in analysis of liver fibrosis in patients with concomitant chronic Hepatitis B and nonalcoholic fatty liver disease. Medicine (Baltimore) 99, e20616 (2020).
Rui, F. et al. The reduced accuracy of non-invasive tests for significant fibrosis in chronic hepatitis B patients with metabolic dysfunction-associated steatotic liver disease. J. Clin. Transl. Hepatol. 12, 827–829 (2024).
Liu, J. et al. Hepatic steatosis leads to overestimation of liver stiffness measurement in both chronic hepatitis B and metabolic-associated fatty liver disease patients. Clin. Res. Hepatol. Gastroenterol. 46, 101957 (2022).
Shen, F. et al. Moderate to severe hepatic steatosis leads to overestimation of liver stiffness measurement in chronic hepatitis B patients without significant fibrosis. Aliment. Pharm. Ther. 50, 93–102 (2019).
Papatheodoridi, M. et al. Refining the Baveno VI elastography criteria for the definition of compensated advanced chronic liver disease. J. Hepatol. 74, 1109–1116 (2021).
Wang, X.-D. et al. Effect of liver steatosis on liver stiffness measurement in chronic hepatitis B patients with normal serum alanine aminotransferase levels: a multicentre cohort study. J. Viral Hepat. 29, 196–204 (2022).
Xu, L. et al. A comparison of hepatic steatosis index, controlled attenuation parameter and ultrasound as noninvasive diagnostic tools for steatosis in chronic hepatitis B. Dig. Liver Dis. 49, 910–917 (2017).
Zhang, Z., Wang, G., Kang, K., Wu, G. & Wang, P. Diagnostic accuracy and clinical utility of a new noninvasive index for hepatic steatosis in patients with hepatitis B virus infection. Sci. Rep. 6, 32875 (2016).
Parikh, P., Ryan, J. D. & Tsochatzis, E. A. Fibrosis assessment in patients with chronic hepatitis B virus (HBV) infection. Ann. Transl. Med. 5, 40 (2017).
Lin, K. W. et al. The utility of non-invasive tests to assess advanced fibrosis in Asian subjects with chronic hepatitis B and concomitant hepatic steatosis. Liver Int. 43, 1008–1014 (2023).
Rui, F., Ni, W., Shi, J., Xie, Q. & Li, J. Superior diagnostic efficacy of Agile 3+ score for diagnosing advanced fibrosis in patients with chronic hepatitis B and concurrent metabolic dysfunction-associated steatotic liver disease. J. Hepatol. 81, e295–e297 (2024).
Chen, L. et al. Noninvasive tests maintain high accuracy for advanced fibrosis in chronic hepatitis B patients with different nomenclatures of steatotic liver disease. J. Med. Virol. 96, e29613 (2024).
Zeng, S. et al. The non-invasive serum biomarkers contributes to indicate liver fibrosis staging and evaluate the progress of chronic hepatitis B. BMC Infect. Dis. 24, 638 (2024).
Li, Q., Lu, C., Li, W., Huang, Y. & Chen, L. The gamma-glutamyl transpeptidase to platelet ratio for non-invasive assessment of liver fibrosis in patients with chronic hepatitis B and non-alcoholic fatty liver disease. Oncotarget 8, 28641–28649 (2017).
O’Hara, G. et al. Liver function tests and fibrosis scores in a rural population in Africa: a cross-sectional study to estimate the burden of disease and associated risk factors. BMJ Open 10, e032890 (2020).
Lemoine, M. et al. The gamma-glutamyl transpeptidase to platelet ratio (GPR) predicts significant liver fibrosis and cirrhosis in patients with chronic HBV infection in West Africa. Gut 65, 1369–1376 (2016).
Stockdale, A. J., Phillips, R. O., Geretti, A. M. & HEPIK Study Group The gamma-glutamyl transpeptidase to platelet ratio (GPR) shows poor correlation with transient elastography measurements of liver fibrosis in HIV-positive patients with chronic hepatitis B in West Africa. Response to: “The gamma-glutamyl transpeptidase to platelet ratio (GPR) predicts significant liver fibrosis and cirrhosis in patients with chronic HBV infection in West Africa” by Lemoine et al. Gut 65, 882–884 (2016).
Papatheodoridi, M. et al. Agile scores in MASLD and ALD: external validation and their utility in clinical algorithms. J. Hepatol. 81, 590–599 (2024).
Angulo, P. et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 45, 846–854 (2007).
Jun, D. W. et al. External validation of the non-alcoholic fatty liver disease fibrosis score for assessing advanced fibrosis in Korean patients. J. Gastroenterol. Hepatol. 32, 1094–1099 (2017).
Wang, J. et al. A novel non-invasive model for the prediction of advanced liver fibrosis in chronic hepatitis B patients with NAFLD. J. Viral Hepat. 30, 287–296 (2023).
Rui, F. et al. Development of a machine learning-based model to predict hepatic inflammation in chronic hepatitis B patients with concurrent hepatic steatosis: a cohort study. EClinicalMedicine 68, 102419 (2024).
Masoodi, M. et al. Metabolomics and lipidomics in NAFLD: biomarkers and non-invasive diagnostic tests. Nat. Rev. Gastroenterol Hepatol. 18, 835–856 (2021).
Noureddin, M. et al. Serum identification of at-risk MASH: the metabolomics-advanced steatohepatitis fibrosis score (MASEF). Hepatology 79, 135–148 (2024).
Caussy, C., Reeder, S. B., Sirlin, C. B. & Loomba, R. Noninvasive, quantitative assessment of liver fat by MRI-PDFF as an endpoint in NASH trials. Hepatology 68, 763–772 (2018).
Cusi, K. et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings: Co-Sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr. Pract. 28, 528–562 (2022).
Xiao, G., Yang, J. & Yan, L. Comparison of diagnostic accuracy of aspartate aminotransferase to platelet ratio index and fibrosis-4 index for detecting liver fibrosis in adult patients with chronic hepatitis B virus infection: a systemic review and meta-analysis. Hepatology 61, 292–302 (2015).
Xiao, G. et al. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: a meta-analysis. Hepatology 66, 1486–1501 (2017).
Luo, J. et al. Gamma-Glutamyl Transpeptidase-to-Platelet ratio predicts liver fibrosis in patients with concomitant chronic hepatitis B and nonalcoholic fatty liver disease. J. Clin. Lab. Anal. 36, e24596 (2022).
Yang, C., Teh, Y. E., Chua, N. G. S., Lee, K. L. S. & Ng, R. Q. M. An overview of multimorbidity and polypharmacy in older people living with HIV. Geriatr. Gerontol. Int. 24, 49–59 (2024).
Wong, G. L. H., Gane, E. & Lok, A. S. F. How to achieve functional cure of HBV: Stopping NUCs, adding interferon or new drug development? J. Hepatol. 76, 1249–1262 (2022).
National Institute for Health and Care Excellence. Overview. Semaglutide for Managing Overweight and Obesity (NICE Guidance, 2023).
Chen, V. L. et al. Resmetirom therapy for metabolic dysfunction-associated steatotic liver disease: October 2024 updates to AASLD Practice Guidance. Hepatology 81, 312–320 (2025).
Hu, Y., Sun, C., Chen, Y., Liu, Y.-D. & Fan, J.-G. Pipeline of new drug treatment for non-alcoholic fatty liver disease/metabolic dysfunction-associated steatotic liver disease. J. Clin. Transl. Hepatol. 12, 802–814 (2024).
GBD 2021 Diabetes Collaborators Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 402, 203–234 (2023).
GBD 2021 Adult BMI Collaborators. Global, regional, and national prevalence of adult overweight and obesity, 1990–2021, with forecasts to 2050: a forecasting study for the Global Burden of Disease Study 2021. Lancet 405, 813–838 (2025).
Rankin, J. EU will struggle to fill gap left by USAID as European countries cut their budgets. The Guardian https://www.theguardian.com/global-development/2025/apr/15/eu-struggle-fill-gap-usaid-european-countries-cut-budgets (2025).
Wang, S. et al. Pathogens don’t respect politicians: US federal disruption poses a new threat to global public health. Lancet Gastroenterol. Hepatol. 10, 291–292 (2025).
Zeng, G., Holmes, B. R., Alqahtani, S. A., Gill, U. S. & Kennedy, P. T. F. The co-existence of NAFLD and CHB is associated with suboptimal viral and biochemical response to CHB antiviral therapy: a systematic review and meta-analysis. Front. Gastroenterol. 3, 1333988 (2024).
Ferraioli, G. & Barr, R. G. Ultrasound evaluation of chronic liver disease. Abdom. Radiol (NY). 50, 1158–1170 (2024).
Kelly, E. M., Feldstein, V. A., Etheridge, D., Hudock, R. & Peters, M. G. Sonography predicts liver steatosis in patients with chronic hepatitis B. J. Ultrasound Med. 36, 925–932 (2017).
Hernaez, R. et al. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology 54, 1082–1090 (2011).
Chen, Z. et al. Impact of hepatic steatosis on liver stiffness measurement by vibration-controlled transient elastography and its diagnostic performance for identifying liver fibrosis in patients with chronic hepatitis B. Insights Imaging 15, 283 (2024).
Xie, X. et al. Liver stiffness as measured by two-dimensional shear wave elastography overestimates the stage of fibrosis in patients with chronic hepatitis B and hepatic steatosis. Clin. Res. Hepatol. Gastroenterol. 45, 101421 (2021).
Zhang, G.-L. et al. Transient elastography and ultrasonography: optimal evaluation of liver fibrosis and cirrhosis in patients with chronic hepatitis B concurrent with nonalcoholic fatty liver disease. Biomed. Res. Int. 2019, 3951574 (2019).
Moura Cunha, G. et al. Interpretation, reporting, and clinical applications of liver MR elastography. Radiology 310, e231220 (2024).
Sterling, R. K. et al. Performance of serum-based scores for identification of mild hepatic steatosis in HBV mono-infected and HBV-HIV co-infected adults. Dig. Dis. Sci. 67, 676–688 (2022).
Chang, J. W. et al. Hepatic steatosis index in the detection of fatty liver in patients with chronic hepatitis B receiving antiviral therapy. Gut Liver 15, 117–127 (2021).
Hinkson, A. et al. Meta-analysis: enhanced liver fibrosis test to identify hepatic fibrosis in chronic liver diseases. Aliment. Pharmacol. Ther. 57, 750–762 (2023).
Lan, Y. et al. The burden of liver cirrhosis and underlying etiologies: results from the Global Burden of Disease Study 2019. Hepatol. Commun. 7, e0026 (2023).
Younossi, Z. M., Wong, G., Anstee, Q. M. & Henry, L. The global burden of liver disease. Clin. Gastroenterol. Hepatol. 21, 1978–1991 (2023).
Terrault, N. A., Francoz, C., Berenguer, M., Charlton, M. & Heimbach, J. Liver Transplantation 2023: status report, current and future challenges. Clin. Gastroenterol. Hepatol. 21, 2150–2166 (2023).
Younossi, Z. M. et al. The changing epidemiology of adult liver transplantation in the United States in 2013–2022: the dominance of metabolic dysfunction-associated steatotic liver disease and alcohol-associated liver disease. Hepatol. Commun. 8, e0352 (2024).
Martyn, E. Figure 1: Hepatitis B virus (HBV) and metabolic dysfunction-associated steatotic liver disease (MASLD) as major global health challenges. BioRender https://BioRender.com/wvagdlp (2025).
Barritt, A. S. et al. High concordance between nonalcoholic fatty liver disease and metabolic dysfunction-associated steatotic liver disease in the TARGET-NASH Real-World Cohort. Am. J. Gastroenterol. 119, 1624–1627 (2024).
Eslam, M. et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J. Hepatol. 73, 202–209 (2020).
Lee, J.-H. et al. Hepatic steatosis index: a simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 42, 503–508 (2010).
JGraph. Draw.io https://app.diagrams.net/ (2025).
Acknowledgements
P.C.M. receives funding from the Francis Crick Institute which receives its core funding from Cancer Research UK, the UK Medical Research Council and the Wellcome Trust (ref. CC2223) and is also supported by University College London NIHR Biomedical Research Centre. E.M. is a doctoral clinical fellow funded by the Francis Crick Institute.
Author information
Authors and Affiliations
Contributions
The article was conceived by E.M. and P.C.M. The primary literature review and manuscript draft were undertaken by E.M., supervised by P.C.M. Figures were made by E.M. and P.C.M. A.A.P., R.G., N.C., S.F., D.M., E.A.T., W.D.F.V., and J.M.G. contributed to refining the text, citations, and presentation of the final article.
Corresponding author
Ethics declarations
Competing interests
P.C.M. has received funding support from GSK for a member of her team (2019-2023) outside the scope of this paper and has received payment from J&J for delivery of educational material during 2025. P.C.M. is clinical co-lead for the NIHR Health Informatics Collaborative for viral hepatitis and liver disease which has received GSK funding support, and is co-chair of the National Strategic Group for Viral Hepatitis. A.A.P. reports investigator-initiated study grants and/or personal fees from ViiV Healthcare, Gilead Sciences, and Jansen Pharmaceuticals (now Johnson & Johnson Innovative Medicine), outside the scope of this paper. W.D.F.V.’s unit receives funding from the Bill and Melinda Gates Foundation, SA Medical Research Council, National Institutes for Health, Unitaid, Foundation for Innovative New Diagnostics (FIND), Merck and the Children’s Investment Fund Foundation (CIFF), has previously received funding from USAID, and received drug donations from ViiV Healthcare, Merck, J&J and Gilead Sciences for investigator-led clinical studies. This unit does investigator-led studies with Merck, J&J, Gilead, and ViiV, providing financial support, and is doing commercial drug studies for Merck and Novo, and performs evaluations of diagnostic devices for multiple biotech companies. Individually, W.D.F.V. receives honoraria for educational talks and advisory board membership for Gilead, ViiV, Mylan/Viatris, Merck, Adcock-Ingram, Aspen, Abbott, Roche, J&J, Sanofi, Boehringer Ingelheim, Thermo-Fischer, and Virology Education. J.M.-G. is a site Principal Investigator for clinical trials with Viiv, GSK, Gilead, and Merck that fall outside the scope of this paper. N.C.’s unit receives research funding from Gilead and has received honoraria from Gilead Sciences and Novo Nordisk. R.G.’s unit receives research funding from Gilead, GSK, ViiV Healthcare, and Janssen. S.F. has received honoraria, conference support, and research grants from Viiv, Gilead, and MSD. Other authors have no competing interests to declare.
Peer review
Peer review information
Communications Medicine thanks Lung-Yi Mak and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Martyn, E., Arenas-Pinto, A., Gilson, R. et al. Diagnosing and defining MASLD in people living with chronic hepatitis B. Commun Med 6, 273 (2026). https://doi.org/10.1038/s43856-026-01383-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-026-01383-2
