
Abstract
Many biological tissues contain colloids within a fibrillar structure. Here, we develop and characterize colloidal-fibrillar scaffolds through examination of the effects of relative colloid and fiber ratios within a fibrin-based model system composed of fibrin-based nanoparticles (FBNs) within a natural fibrin scaffold. At lower concentrations, FBNs primarily integrate into the fibrillar fibrin matrix, strengthening it. At high concentrations, colloid-colloid interactions dominate and FBNs primarily form a highly aligned secondary structure that does not strengthen the fibrillar matrix. At intermediate concentrations, both reinforcement of the fibrin matrix and colloid-colloid interactions are observed. Our characterization of this colloidal-fibrillar system provides insight into new avenues for wound healing biomaterial development. Using structural and mechanical results, we developed a biomimetic surgical sealant. When applied to a vascular healing model, FBN gel resulted in improved vessel healing. This colloidal-fibrillar composite can greatly improve healing outcomes and should be applied to other tissues.
Similar content being viewed by others


Introduction
Scaffold porosity is critical to cellular infiltration and tissue regeneration. However, porosity is hard to control in naturally-derived scaffolds and void space often comes as a trade-off with strength1. The advent of microporous annealed particle (MAP) hydrogels has maximized control over scaffold porosity2. MAP gels are constructed from colloidal building blocks that form a bulk scaffold upon annealing. Particle size and concentration are finely tuned to achieve optimal porosity for different applications3. Because they are formed from pre-polymerized particles and delivered in suspension, MAP gels are convenient for both topical and injectable uses4,5,6.
While colloidal MAP gels exhibit impressive capacity for cellular infiltration across many tissues, they do not capture the fibrillar characteristics of natural extracellular matrix, nor do they benefit from the strength of fibrillar networks. Microlevel fibrillar structure of native extracellular matrix also provides crucial cues to guide tissue regeneration7,8. We were inspired by the interplay between soft colloids and microfibrillar structure in the body to investigate the impact of colloids and fiber relative composition in governing structure, mechanics, and biological outcomes in colloidal-fibrillar composite gels. Our ultimate goal is to develop a biomimetic scaffold that brings together the porosity, tunability, and convenience of MAP gels and the strength of fibrillar matrixes for use in a range of biomedical applications. By imitating in vivo structure, we aim to minimize fibrosis and scarring, while promoting appropriate cellular infiltration and remodeling. In this work, we develop scaffolds comprised of fibrin-based nanoparticles (FBNs) within a fibrillar fibrin matrix.
Fibrin forms a fibrillar structure that is crucial to wound healing through its structural support of both clot formation and cellular re-infiltration during tissue remodeling. Bulk fibrin gels have many clinical applications, including as surgical sealants9,10,11. Indeed, high-density fibrin glues (HDFGs) are the only surgical sealants used internally. HDFGs work by mixing concentrated solutions of fibrinogen and thrombin (40-100X physiologic concentrations) to mimic the end of the coagulation cascade. However, these high concentrations result in short working-times and a hyperdense fibrin structure. Furthermore, HDFG components are expensive and have impractical cold chain requirements.
Our group has developed pre-polymerized fibrin-based nanoparticles (FBNs), which may be used as particles or in a MAP-like scaffold12,13. Here, we investigate the integration of colloidal FBNs within a fibrillar network with the ultimate goal of developing a vascular surgical sealant with physiologically-relevant porosity (Fig. 1A-C). FBNs are produced through a simple scalable process (Fig. 1D), resulting in diameters of ~250-280 nm (Fig. 1E, Supplementary Fig. 1). Particles are room temperature stable (Fig. 1F) and resuspend rapidly ( < 10 sec; Fig. 1G), making their clinical use and storage straightforward. We have used our FBN colloidal-fibrillar surgical sealant (FBN gel) as an adjunct to stitches for repair of gross vascular injury.

A Schematic comparing. material properties of high-density fibrin glues with those of FBN gels. Fibrin fibers are represented by purple ribbons, and FBNs are represented by small purple dots. The top panel depicts the high-density structure of fibrin glue which inhibits cell infiltration. The bottom panel depicts the high porosity of FBN gels, which allows for high cellular infiltration, as demonstrated by different cell types infiltrating the material. B Representative cryoSEM images of high-density fibrin glue, FBN gel, and a fibrin clot of physiologic density. Scale bar = 10 μm. C Representative confocal images of HUVEC cells seeded in high-density fibrin glue, FBN gel, and a fibrin clot of physiologic density after one week of growth, demonstrating relative cellular-level porosity. Scale bar = 200 μm. D Schematic of fibrin-based nanoparticle production. E Representative atomic force microscopy image of fibrin-based nanoparticle. Scale bar = 1 μm. F Representative image of lyophilized FBNs. Scale bar = 1 cm. G Representative images before and after rapid resuspension of lyophilized FBNs in deionized water via 10 seconds of mixing via vortex.
As drug-loaded FBNs allow for finely tuned load/release kinetics, we loaded FBNs with the small molecule tazarotene. Like other retinoids, tazarotene is known to increase cellular turnover and limit scar formation14. This class of drugs has been enormously effective in clinical practice for superficial applications (e.g. psoriasis, acne, Kaposi’s sarcoma)15 and in experiments for deeper dermal healing of complex woundbeds (e.g. pressure ulcers, chronic diabetic wounds)16,17. Many other experimental wound healing materials rely on the use of growth factors (e.g. vascular endothelial growth factor, epidermal growth factor), however these growth factors are extremely expensive. One of our main goals in prioritizing a lack of refrigeration in our development process was to produce a wound-healing material that could be used across a wide array of treatment environments, including low-resource settings. Implementing tazarotene (a medication with a generic formulation in the United States) allowed us to access the vascular endothelial growth factor-Notch signaling pathway and promote angiogenesis16,18,19. without the use of growth factors that would make the ultimate material prohibitively expensive for many applications that we envision. Here, we describe the development, characterization and in vivo use of the first fibrin-based colloidal surgical sealant that brings together the best aspects of MAP gels and fibrillar scaffolds to produce an effective vascular surgical sealant that promotes tissue regeneration and accelerates long-term healing.
Results
Fibrin-Based Nanoparticle Characterization
FBNs were produced via bulk fibrin shearing and sonication (Fig. 1D). Dry and hydrodynamic particle diameters were 235.2±39.97 nm (Fig. 1E) and 254±75 nm (Supplementary Fig. 1A), respectively. Due to tazarotene’s low aqueous solubility, established diffusion-based drug-loading20 was not successful, and other solvents caused FBN damage. Successful loading was achieved through tazarotene inclusion (1 mM) in the bulk fibrin gel sheared to produce FBNs (average particle load 2±0.4 picomole (Supplementary Fig. 2)).
FBN Gel Polymerization and Biomechanics as a Function of Colloidal Inclusion
FBN gels were formed through the addition of FBNs to whole blood (WB) fibrin gels. Gel polymerization was evaluated through rheology (Fig. 2A), with gelation time defined as the point at which storage modulus is three times larger than loss modulus, as the classic definition where the two are equal did not yield clinically meaningful gelation. The use of this nonclassical gelation time is used to bring clinical and lay meaning to this term. FBN addition to WB resulted in faster gelation, with a statistically significant increase observed with the addition of 66 M FBN/mL (WB: 310±171 sec, 66 M FBN/mL: 66±16 sec; p = 0.012; Fig. 2B). The fastest gelation was reached with the addition of 130 M FBN/mL (22±10 sec), after which additional FBNs led to slower gelation. HDFGs polymerized fastest (0±0 sec; i.e. polymerization occurred during the 2 second measuring system recording delay), but were not statistically different from WB + 33 M, 66 M, 130 M, or 260 M FBN/mL conditions. Storage modulus followed a similar trend; greater FBN concentrations increased storage modulus through 260 M FBN/mL (101±50 Pa) after which storage modulus dropped (400 M FBN/mL: 26±11 Pa, 530 M FBN/mL: 1±1 Pa, Fig. 2C), though differences were not significant. HDFG storage modulus was significantly greater and more variable than any other group (956±601 Pa). Loss modulus was also similarly explored and showed similar results (Supplementary Fig. 3A,B).

Comparisons across all tests are between whole blood gels, high-density fibrin glue (HDFG) and whole blood-FBN gels of varying FBN concentration. A Average polymerization curves determined via rheometry for whole blood clots, high-density fibrin glue, and whole blood-FBN gels using differing concentrations of FBNs. Thrombin (0.5 U/mL) and CaCl2 (0.05 mM) and FBNs (varying final concentrations) were added to whole blood. N = 3. B Comparison of gelation time between whole blood clots, high-density fibrin glue, and whole blood-FBN gels with differing concentrations of FBNs. (C) Comparison of storage modulus after 15 minutes of polymerization between whole blood clots, high-density fibrin glue, and whole blood-FBN gels with differing concentrations of FBNs. (D) Schematic demonstrating Instron UTS methods utilized to measure tension, shear adhesion, and wound closure. E Comparison of tensile strength between gels. HDFG: N = 3, Other groups: N = 11-15 (F) Comparison of shear adhesion between gels. N = 7-11 G Comparison of wound closure rupture extension between gels. N = 8-10 (H) Schematic of material leak testing process. N = 7-15 (I) Comparison of leak pressure between biomaterials. J Comparison of degradation over four hours between gels. HDFG: N = 3. Other groups: N = 5. K Comparison of tensile strength of whole blood-FBN gel (330 M FBN/mL) made using newly polymerized FBNs or 1-year-old FBNs (lyophilized; room temperature (RT) storage). N = 11. L Comparison of adhesive strength of whole blood-FBN gel (330 M FBN/mL) made using newly polymerized FBNs or 1-year-old FBNs (lyophilized; RT storage). N = 9–13. M Comparison of leak pressure of whole blood-FBN gel (330 M FBN/mL) made using newly polymerized FBNs or 1-year-old FBNs (lyophilized; RT storage). N = 7. All comparisons were performed using one-way ANOVA with Tukey’s post hoc analysis or unpaired Student’s t-test. ns= p > 0.05, *=p < 0.05, **=p < 0.01, ***=p < 0.001.
Tensile strength, shear adhesive strength, and wound closure were measured using an Instron Universal Testing System (UTS) (Fig. 2D). Local maxima in tensile strength were achieved at 33 M FBN/mL and 330 M FBN/mL (33 M FBN/mL: 26±9 N, 330 M FBN/mL: 17±6 N). HDFG was significantly stronger than all other groups (HDFG: 474±54 N) (Fig. 2E). All particle concentrations at or above 130 M FBN/mL significantly decreased shear adhesion compared to WB only (Fig. 2E), but values were not statistically different from HDFG. 66 M FBN/mL was also found to be significantly different from 260 M FBN/mL. Wound closure was largely stable across groups. HDFG demonstrated a slightly greater average rupture extension, which was significantly greater than the 66 M FBN/mL gels (66 M FBN/mL: 4.6±3.1 N, HDFG: 11.3±3.1 N, p = 0.011; Fig. 2F, Supplementary Fig. 4A).
Sealant Functionality and Degradation
Sealant functionality was determined by the air pressure required to dislodge in situ polymerized gels from a puncture in latex tubing (Fig. 2G). Based on prior mechanical testing, WB + 330 M FBN/mL was chosen as the ideal composition for a surgical sealant, therefore only this formulation was compared to HDFG. FBN gels outperformed HDFGs, with significantly higher leak pressures. (FBN: 51±14 mbar, HDFG: 28±30 mbar, p = 0.031; Fig. 2H, I). Material degradation was also evaluated. Increased FBN concentration led to slower degradation, with 530 M and 400 M FBN/mL groups performing comparably to HDFG (Fig. 2J).
Long-term Particle Stability
Tensile strength, shear adhesion, and leak pressure testing were performed on 330 M FBN/mL gels prepared using lyophilized FBNs stored for 1 year at room temperature. Across all tests, no statistical difference was noted between new and old FBN groups, thus demonstrating their long-term room temperature stability (Fig. 2K-M).
Structural Analysis
Cryogenic scanning electron microscopy of platelet-poor plasma (PPP) FBN gels demonstrated an interesting, triphasic structural phenomenon as FBN composition increased. At lower concentrations ( < 200 M FBN/mL), FBNs are primarily found within the fibrillar matrix resulting in a structurally similar, but more robust fibrin network (Fig. 3A-C). Confocal microscopy confirmed increased fibrillar density at these concentrations (Supplementary Fig. 4B-C). At higher concentrations ( > 400 M FBN/mL), FBNs primarily form a highly aligned secondary structure outside the fibrillar matrix, in which colloid-colloid interactions dominate without enhancing fibrillar structure. At intermediate concentrations ( ~ 200-400 M FBN/mL), both reinforcement of the fibrin matrix and colloid-colloid interactions are observed. FBNs increase fiber thickness, peaking at 260 M FBN/mL (1.7±0.6μm), and then decreasing to baseline levels at 530 M FBN/mL (PPP: 0.71±0.28μm, 530 M FBN/mL: 0.73±0.23μm; Fig. 3D). Porosity decreased significantly with added FBNs, (PPP: 81±2%, 66 M FBN/mL: 51±9%, 260 M FBN/mL: 45±3%, 400 M FBN/mL: 37±5%, 530 M FBN/mL: 35±9%, p < 0.0001 for all comparisons with PPP; Fig. 3E). Increasing particle concentration did not change the alignment of the primary structure, but analysis isolating the secondary structure at 530 M FBN/mL – (530 M(2) in Fig. 3F) – demonstrated this secondary structure has significantly greater alignment index than any gel’s primary alignment.

A Schematic describing how increasing FBN concentration affects fibrin-colloid composite structure. B Representative cryoSEM images of a platelet poor plasma (PPP) gel, as well as PPP-FBN gels with 66 M, 330 M, and 530 M FBN/mL. Scale bar = 10 μm. C Representative detailed cryoSEM images of FBNs integrated into the fibrin matrix (top image) and FBNs polymerized among themselves to form highly aligned secondary fibrin network (bottom image). FBNs false colored in blue. Scale bar = 1 μm. D Comparison of fiber thickness between PPP gels and PPP-FBN gels with different concentrations of FBNs. N = 32-38 E Comparison of porosity between PPP gels and PPP-FBN gels with different concentrations of FBNs. N = 3-5. F Comparison of fiber alignment between PPP gels and PPP-FBN gels with different concentrations of FBNs. Measurements were taken based on cryoSEM images taken. N = 3-5. G Schematic of Instron UTS method used to generate stress-relaxation curves for mathematical modeling. H Stress-relaxation curves from high-density fibrin glue (HDFG), differentially colored in red and blue to draw attention to two sub-populations of curve patterns. Average curves for each sub-population included in black. N = 10 total; 5 per subpopulation. (I) Average stress-relaxation curves for whole blood clots, WB-FBN gels with 66 M, 130 M, 260 M, or 400 M FBN/mL, and HDFG sub-populations plotted together (left) with detail inset (right). For 400 M FBN/mL group, representative curve was plotted, rather than average, to preserve depiction of inertial regime in this group. J Schematic depicting stress-relaxation curve changes as FBNs are added to whole blood (WB), and FBN concentration is increased, in accordance with (K) Representative stress-relaxation curves for whole blood clots and WB-FBN gels (particle concentrations: 66 M, 130 M, 260 M & 400 M FBN/mL; these same concentrations are compared throughout remaining panels.) plotted alongside their best-fit Kelvin viscoelastic model, where appropriate. Kelvin schematic included for each representative image to depict system differences from baseline whole blood gel without FBNs. (L) Comparison of stress-relaxation time between whole blood clots, whole blood-FBN gels, and HDFG. N = 4-11. M Comparison of strain-relaxation time between whole blood clots, whole blood-FBN gels, and HDFG. N = 4-11 N Comparison of equilibrium stress between whole blood clots, whole blood-FBN gels, and HDFG. N = 4–11. All comparisons were performed using one-way ANOVA with Tukey’s post hoc analysis. *=p < 0.05, **=p < 0.01, ***=p < 0.001, ****=p < 0.0001.
Stress-Relaxation and Viscoelastic Modeling
Tensile stress-relaxation was evaluated (Fig. 3G). HDFGs exhibited two different stress-relaxation behaviors (Fig. 3H), which aligns with the heterogeneity noted in leak pressure and structural analyses, likely due to rapid polymerization (Fig. 2I, Supplementary Fig. 4C). HDFGs were the only group to demonstrate distinct intragroup patterns (Fig. 3I). WB and FBN gels with lower particle concentrations predominantly acted as viscoelastic solids. With greater FBN incorporation, gels demonstrated greater inertial noise, until inertial forces dominated at 400 M FBN/mL creating an oscillatory regime (Fig. 3J, K, Supplementary Fig. 5A-B). Differences between characteristic material parameters were quantified through Kelvin model fitting (Fig. 3K, Supplementary Fig. 5C). Residuals confirmed that this model was appropriate (Supplementary Fig. 5B). An extended Kelvin model fit better for HDFG, but it was important to use the same model across all materials (Supplementary Fig. 6). 260 M FBN/mL gels demonstrated higher stress-relaxation times than any other FBN gels (69±9 sec; p < 0.01 for all comparisons; Fig. 3L). Differences in strain relaxation time were insignificant, aside from the second HDFG subpopulation, which was greater than all other groups (p < 0.001 for all comparisons; Fig. 3M). As displacement was the controlled input, it follows that strain relaxation time provided less meaning. The elastic model component increased through 130 M FBN/mL, and then decreased again, but this was not significant. Both HDFG subpopulations had a higher elastic model component than all other groups, with HDFG-A significantly higher than all other groups (p < 0.0001 for all comparisons; Fig. 3N).
Tazarotene Dosing
For surgical sealant design, 330 M FBN/mL was chosen to optimize mechanics while ensuring the presence of secondary aligned structure. We also wanted to leverage the localized drug delivery capacity of FBNs. Prior work demonstrating tazarotene’s angiogenic effects led us to investigate its vascular network effects to determine optimal dosage16,18,19. Therefore, we employed a microfluidic vasculogenesis assay wherein human umbilical vein endothelial cells (HUVECs) and human lung fibroblasts (HLFs) were embedded in fibrin gels and co-cultured with free tazarotene (Supplementary Fig. 7A)21. 20-200 pM tazarotene concentrations resulted in significantly greater endothelial network area and segment width compared to controls (Supplementary Fig. 7B-E).
To evaluate cellular morphology, HUVECs were cultured on bulk-loaded fibrin gels containing different tazarotene concentrations; no effects on attachment were noted (Supplementary Fig. 8A-C). Increased tazarotene increased spreading through 200 nM, after which cells spread less (Supplementary Fig. 8D). With more tazarotene, cells exhibited less circularity and greater perimeter (Supplementary Fig. 8E-F). This data indicates a wide dosage band for the promotion of HUVEC polarization. To validate tazarotene delivery via FBNs, HUVECs were cultured on FBN gels containing differing tazarotene-loaded to unloaded FBN ratios. Similar trends to those using free tazarotene were observed, validating that loaded FBNs release tazarotene when incorporated into FBN gels (Supplementary Fig. 9). We selected an optimized ratio of tazarotene-loaded to unloaded FBNs (1:1000) for loaded FBN (tFBN) gels, as this concentration produced the best cellular characteristics.
In Vivo Clinical Outcomes and Vascular Healing
To investigate the in vivo healing properties of FBN and tFBN gels, we focused on the common clinical problem of leak prevention in surgical vascular repair. In these studies, FBN gel, tFBN gel, or HDFG was used over suture closure of an injured rabbit carotid vessel (Fig. 4A-B, Supplementary Fig. 10A). Suture without sealant was used as a control. Ultrasound was used to evaluate vessel patency post-surgery and one- and two-weeks post-op (Fig. 4C, Supplementary Fig. 10B). Treatment course for all surgically-treated rabbits was uncomplicated, with no adverse events. Two rabbits experienced cardiac arrest after pre-surgical sedation, however, this is not uncommon for prey animals22,23. Three rabbits out of 28 experienced complete vessel blockages. In all three, post-op ultrasound demonstrated patency and blockage was noted in the one-week ultrasound. Two occurred in the HDFG group, where material properties may have increased thrombotic risk, as ex vivo analysis demonstrated HDFG to be more thrombogenic than FBN gel (p < 0.0001, Fig. 4D). No difference in vessel cross-sectional area was found (Fig. 4E, Supplementary Fig. 10C). Both FBN and tFBN gels resulted in smaller wounds as a percentage of vessel cross-sectional area than either stitches alone or HDFG (stitches alone: 43±19%, HDFG: 54±7%, FBN: 13±3%, tFBN: 11±3%, stitches alone vs FBN: p = 0.0004, HDFG vs FBN: p < 0.0001, stitches alone vs tFBN: p = 0.0001, HDFG vs tFBN: p < 0.0001; Fig. 4F, G, Supplementary Fig. 10C). This analysis did not include blocked vessels. Additionally, FBN-treated vessels demonstrated greater endothelial continuity than HDFG-treated vessels, indicating more effective tissue remodeling (HDFG: 1.8±0.45, FBN: 2.8±0.45, p = 0.03; Fig. 4H). The tunica muscularis demonstrated similar, but non-significant trends (Supplementary Fig. 11A). Additional pathologic analysis was performed following established protocols24 and demonstrated trends towards greater inflammation with HDFGs and less with FBNs (Supplementary Fig. 11B-F).

A Schematic of leporine vascular healing assay employed. B Representative images of FBN gel following polymerization in situ on rabbit vessel injury site (top) and injury site with stitches alone (bottom). C Representative ultrasound images used to evaluate patency of vessel surgical site before assay endpoint. Red arrows indicate location of vessel cross-section. Narrowing can be seen at the surgical site. D Thrombogenicity determined via activated partial thromboplastin clotting time of whole blood in the presence of the clot, FBN gel, or high density fibrin glue (HDFG). N = 3-5 E Comparison of vessel cross-sectional area between surgical groups: stitches alone, stitches with high-density fibrin glue, stitches with FBN gel, and stitches with tazarotene-loaded FBN (tFBN) gel. Vessels that experienced complete thrombosis are highlighted in red. N = 7 F Representative H&E histology from each surgical group, with wound area circumscribed in yellow and detailed higher magnification inset for each wound site. Scale bar = 400 μm. G Comparison of wound percentage of vessel area between surgical groups: stitches alone, stitches with high-density fibrin glue, stitches with FBN gel, and stitches with tazarotene-loaded FBN (tFBN) gel. Vessels that experienced complete thrombosis were excluded from this comparison. N = 5-7 H Comparison of endothelial continuity between surgical groups: stitches alone, stitches with high-density fibrin glue, stitches with FBN gel, and stitches with tazarotene-loaded FBN (tFBN) gel. N = 5-7 I Comparison of vessel thickness between surgical groups: stitches alone, stitches with high-density fibrin glue, stitches with FBN gel, and stitches with tazarotene-loaded FBN (tFBN) gel. Vessels that experienced complete thrombosis were excluded from this comparison. N = 5–7. J Comparison of endothelial hypertrophy between surgical groups: stitches alone, stitches with high-density fibrin glue, stitches with FBN gel, and stitches with tazarotene-loaded FBN (tFBN) gel. N = 5–7 K Representative fibrin immunohistochemistry (IHC) images of vessels treated with FBN gel (left) and with high-density fibrin gel (right). Fibrin is in red, allowing for visualization of FBNs and HDFG remnants. Cell nuclei are in blue. Stitches, where present, are false colored in green. Scale bar = 400 μm. L Comparison of fibrin integrated density at vessel injury site between surgical groups via analysis of fibrin IHC images. N = 5-7 M Comparison of adhesion grading of vessel surgical site, determined during tissue collection. Grade 0 = no attachment of vessel to surrounding tissue. Grade 5 = full circumferential attachment to surrounding tissue. N = 5–7. All comparisons were performed using one-way ANOVA with Tukey’s post hoc analysis. *=p < 0.05, **=p < 0.01, ***=p < 0.001, ****=p < 0.0001.
A three-week endpoint was chosen to evaluate neointimal hyperplasia at the wound site – a common negative outcome in vascular surgery that increases risk for vessel (re)stenosis25,26. Quantification of vessel thickness demonstrated no differences between surgical and non-surgical vessels among FBN- and tFBN-treated animals (Supplementary Fig. 12). HDFG-treated vessels showed significantly greater difference from baseline than FBN and tFBN gels (HDFG: 112±81μm, FBN: -12±26μm, tFBN: -12±21μm, p = 0.001 for both; Fig. 4I, Supplementary Fig. 11). Endothelial hypertrophy was significantly less in FBN groups than the HDFG group (HDFG:1±0.71, FBN: 0±0, p = 0.036, Fig. 4J). These results support that neointimal hyperplasia is not a significant risk with these biomaterials. HDFG-treated vessel tissue and surrounding fascia were anecdotally noted to be stiffer during tissue collection, however no quantitative testing was able to be performed due to tissue sacrifice for specimen pathology and tissue transcriptomics.
Differences in fibrin remnants and diffuse fibrin deposition were evaluated via fibrin immunohistochemistry (IHC) (Fig. 4K, Supplementary Fig. 13). Significantly more fibrin was found at HDFG wound sites, which is a risk factor for surgical adhesions (Fig. 4L). Large remnants of HDFG were found during tissue collection, which were confirmed to be fibrin via IHC and lack of degradation was corroborated in vitro (Supplementary Fig. 14A-C). Additionally, HDFG-treated animals had significantly greater surgical adhesions than all other treatments (HDFG vs stitches alone: p = 0.0006, p < 0.0001 for all other comparisons, Fig. 4M, Supplementary Fig. 15-16). Tazarotene-loaded FBN gels exhibited significantly fewer surgical adhesions than all other groups (stitches alone vs tFBN: p < 0.0001, FBN vs tFBN: p = 0.0006, Fig. 4L).
Cellular and Vascular Network Responses
We used transcriptomic analysis to evaluate mechanistic causes for in vivo differences. Trends suggested less collagen and greater inflammation in HDFG-treated tissue (Supplementary Fig. 17A-B). HDFG-treated tissue trended towards expression of more CD68, potentially indicating greater M1-macrophage polarization27,28. FBN-treated tissue expressed significantly more TGF-β1 than HDFG-treated (HDFG: 10±27% difference from healthy vessel (DFHV), FBN: 72±15% DFHV, p = 0.047, Fig. 5A, Supplementary Fig. 17C). The only difference between FBN- and tFBN-treated tissue was that tFBN-treated tissues expressed less VCAM1 (Supplementary Fig. 17D). tFBN-treated tissues were the only ones not to express significantly more VCAM1 than healthy control, and they expressed significantly less VCAM1 than stitches alone (Stitches Alone: 136±32% DFHV, tFBN: 26±31% DFHV, p = 0.028, Fig. 5A, Supplementary Fig. 17D), potentially partially explaining this group’s reduction in post-surgical adhesions.

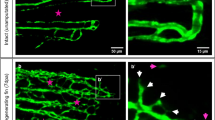
A Heatmap comparison of transcriptomic analysis of vessel wound site tissue between surgical groups: stitches alone, stitches with high-density fibrin glue (HDFG), stitches with FBN gel, and stitches with tazarotene-loaded FBN (tFBN) gel. B Schematic representation of vasculogenesis assay. HUVEC and human lung fibroblast (HLF) cells were seeded in the biomaterial (HDFG, FBN gel, or tFBN gel) during in situ polymerization of the material within the central channel. C Representative images of vascular networks formed during vasculogenesis assay. HLFs are stained in green, HUVECs are stained in red, and cell nuclei are cyan. Scale bar = 100 μm. D Detailed representative images of HUVEC networks formed during vasculogenesis assay and comparison of total HUVEC cellular area in vascular network between FBN gel, tFBN gel, and HDFG. Scale bar = 100 μm. N = 6–9 E Detailed representative images of HLF networks formed during vasculogenesis assay and comparison of total HLF cellular area in vascular network formed between FBN gel, tFBN gel, and HDFG. N = 5-7 Scale bar = 200 μm. N = 6–9 F Schematic of HUVEC thin film cellular effects assay. Thin films of biomaterial (FBN gel, tFBN gel, or HDFG) were allowed to polymerize for 2 hr. HUVECs were seeded onto thin films and given normal HUVEC media. Cells were counted and imaged after 16 hours. G Representative images of HUVECs after culture on FBN gel, tFBN gel, or HDFG for 16 hours. Scale bar = 100 μm. H Comparison of HUVEC cellular attachment after 16 hours of culture on FBN gel, tFBN gel, or HDFG. N = 7-15 I Comparison of HUVEC individual cell area after 16 hours of culture on FBN gel, tFBN gel, or HDFG. N = 15-28 J Comparison of HUVEC individual cell perimeter after 16 hours of culture on FBN gel, tFBN gel, or HDFG. N = 15 K Comparison of HUVEC individual cell circularity after 16 hours of culture on FBN gel, tFBN gel, or HDFG. N = 15. All comparisons were performed using one-way ANOVA with Tukey’s post hoc analysis. *=p < 0.05, **=p < 0.01, ***=p < 0.001, ****=p < 0.0001.
Effects on vascular network formation were evaluated via a vasculogenesis assay (Fig. 5B). While no difference was seen between FBN and tFBN gel networks, there was no endothelial growth or network formation in HDFGs (HDFG: 1500±1600μm2, FBN gel: 266,000±98,600 μm2, tFBN gel: 293,000±69,000μm2, both comparisons: p < 0.0001, Fig. 5C, D). Indeed, >99% of endothelial cells embedded in HDFG were dead, likely due to extreme thrombin exposure29,30. Though alive, fibroblast network formation was significantly less than those embedded in other gels (HDFG: 352,000±206,000μm2, FBN gel: 753,000±113,000μm2, tFBN gel: 848,000±164,000μm2, HDFG vs FBN: p = 0.0008, HDFG vs tFBN: p < 0.0001, Fig. 5C-E). Cells cultured on FBN and tFBN gels displayed greater spreading and attachment, while cells on HDFG remained circular and small (Fig. 5F-K). These results demonstrate the relative intolerance of HUVECs to growth into/onto HDFG, providing insight into the capsular formation witnessed in vivo.
Discussion
Porous scaffolds with colloidal properties, such as MAP gels, have enormous potential to promote tissue regeneration, and new clinical applications are constantly emerging. MAP gels, also referred to as granular hydrogels, have advantages compared to traditional bulk gels—notably, their high porosity structures. These MAP gels, created from microgel building blocks, produce modular systems that are easily applied in flowable solutions and then crosslinked to enhance their structural stability. In recent years, the utility of MAP gels has been demonstrated in several applications, particularly regarding wound healing applications. Griffin et al. showed that MAP gels could be used to enhance cell migration and wound healing in vivo31. In another example, Pruett et al. described a MAP scaffold containing heparin microislands that allow for the organization of native growth factors, facilitating enhanced healing4. Beyond wound healing applications, MAP-based hydrogels have also shown promise in other applications, including ischemic stroke32,33, calvarial defects34, cancer postoperative therapy35, spinal cord injury36,37, stem cell delivery38,39,40, mRNA delivery41, surgical micropuncture42, and vaccine delivery43. The modular and flowable nature of these MAP-based systems makes them useful for a range of applications. However, in vivo, many cells crucial to tissue healing benefit from a stronger fibrillar scaffold for growth – an aspect that is not encompassed in current MAP gels. Furthermore, while some naturally derived MAP gels have been described, a majority are synthesized from synthetic polymers. While synthetic polymers allow for a high degree of material tunability, the use of naturally derived materials to create pro-regenerative wound healing constructs capitalizes on the inherent pro-regenerative capability and biodegradability of these materials44,45,46. To that end, here, we combined the colloidal properties of MAP gels with a physiologic fibrin scaffold to develop a new class of pro-healing materials and identified an optimal formulation for use as a surgical sealant, which was successfully used over suture-based vascular closure to prevent surgical complications and promote healing.
While our studies have shown that HDFGs are significantly stronger than FBN gels, this strength is not clinically meaningful, as it does not appear to consistently translate into superior sealant capacity. HDFGs polymerize almost instantaneously, leading to short clinical work time and structural heterogeneity as gelation occurs before true mixing can be achieved, leaving areas of unpolymerized fibrinogen gel and areas of hyperdense elastic fibrin. This leads to the large variability in their physical properties, most notably in stress-relaxation and in leak pressure. When the high-density structure dominates the viscoelastic properties of the HDFG, we see a higher material elasticity, whereas the thinner sections of stress-accepting material when there is greater contribution from unpolymerized fibrinogen gel, result in greater creep and stress relaxation times as those smaller fibers undergo greater irreversible deformation. With greater colloidal component, FBN gels are softer and less elastic with a longer stress-relaxation time. This type of construct with lower internal peak stresses, is advantageous over one that generates high internal peak stresses, as it is able to gradually deform to accommodate surrounding tissues. In contrast, HDFG is less responsive to its environment and more likely to deform or impede surrounding tissues.
In the design of the FBN gel, our goal was to maximize the colloidal properties of the material, while maintaining sufficient strength to act as a surgical sealant. To this end, it was imperative for us to fully evaluate the physical, structural, and viscoelastic properties with respect to changing nanogel particle concentrations, and compare them with currently used HDFGs. At a concentration of 330 M FBN/mL, we were able to optimize tensile strength, polymerization dynamics, wound closure, and adhesive properties within the range of concentrations that demonstrated the highly aligned secondary structure. While the development of the secondary aligned structure noted via cryoSEM at this concentration results in slightly lower porosity, the alignment of the network is reminiscent of the highly aligned fibrin scaffolds seen in neonatal fibrinogen clots, where they are known to meaningfully improve healing47. This type of naturally aligned scaffold also appears in other nonfibrin extracellular matrix to promote the regeneration of other tissues, such as nerves and tendons. So, it was important to us to choose an FBN concentration for the gel that would remain within this regime where the natural fibrin matrix remains strong, yet this secondary aligned construct is well-developed. Higher concentration FBN gels which demonstrate even greater alignment but lack strength may be excellent candidates for topical wound healing materials as in burns or chronic wounds.
In vivo leporine vascular healing studies showed that FBN and tFBN gels performed better in healing metrics than either stitches alone or HDFG. Importantly, no evidence of neointimal hyperplasia was noted. Future work should investigate assess long-term scar formation and safety of internal tazarotene release. tFBN gels displayed fewer adhesions; this is important, as adhesions cause pain and increase risk during repeat surgeries. Through transcriptomic investigation, tFBN gels were found to express less VCAM1 than other treatments. As VCAM1 facilitates immune cells adhesion to vascular endothelium, it is possible these anti-inflammatory effects prevent adhesions. Future work should further investigate the mechanism of tazarotene’s lessened adhesion burden and whether it is replicable in other tissues and surgical procedures.
The lack of HDFG degradation that we saw both in vitro and in vivo could be a cause for concern. Even though HDFGs are naturally derived and non-toxic, the use of extreme supraphysiologic concentrations (40-100X concentrations seen in naturally occurring fibrin clots) appears to create a material that cannot be easily degraded by the body and is not conducive to any cellular infiltration, even over the course of a month. This resulted in capsule formation around large HDFG remnants. In this way, HDFGs actively impeded long-term tissue regeneration and healing by effectively creating a foreign body insult that provoked additional damage to the tissues surrounding the vessel injury site. Importantly, appropriate degradation profiles both in vivo and in vitro were noted with FBN gels. Furthermore, a key finding of these studies is that FBN colloidal composite gels can be created with porosity that is much improved compared to HDFGs. As can be seen in Fig. 1B, the porosity of HDFG is substantially less than any of the colloidal-fibrillar composite formulations, including the 330 M FBN/mL group that was used for in vivo and in vitro analysis. Indeed, results shown in Fig. 5 clearly depict that HUVEC and fibroblast network formation are very minimal in the HDFG groups, presumably due to the minimal porosity of these networks. However, the FBN-containing groups greatly improve HUVEC and fibroblast network formation in these studies, likely due at least in part to the improved porosity of these networks.
In addition to the structural and pro-healing properties of FBN gels, the importance of their clinical translatability should not be understated. We demonstrated the long-term shelf stability of FBNs and their rapid resuspension. For the gels, we chose to use a patient cofactor with no processing requirements as the fibrillar component so that it can be collected at the time of use without refrigeration. These aspects contrast with HDFGs whose use are limited by thaw times and cold-chain requirements. Thus, FBN gels can make improved healing through cutting-edge biomaterials accessible to more people.
Beyond the specific design and development of our FBN and tFBN surgical sealants, this work defines how ratios of colloids to fibrillar networks can highly tune porosity, mechanics, and structure, both in fibrin-based materials and beyond. Colloids embedded in fibrillar networks are a common natural motif – from tendons and cartilage to blood clots and skin. Thus, a deeper understanding of colloidal-fibrillar interactions, mechanics, and cellular effects is crucial to understanding the body’s many tissues. This work can also act as a model system and define design criteria for materials suited to a wide range of applications. In seeking to recreate two layers of structural complexity (fibril and colloid) in these composite materials, by tuning the relative colloidal presence, we developed a material with three layers of structural complexity (a larger structural scaffold, a secondary aligned scaffold, and a colloid). Other colloidal-fibrillar composites may display similarly surprising properties following investigation.
Materials And Methods
Fibrin-Based Nanoparticle (FBN) Production and Drug Loading
Fibrin-based nanoparticles were produced via a well-established technique in our lab (Fig. 1D)12. A 5 mL bulk fibrin gel is produced to a final concentration of 0.5 U/mL thrombin, 2 mg/mL fibrinogen, and 25 mM N-2-hydroxyethylpiperazine-N′-2-ethanesulfonic acid (HEPES) buffer (0.15 M NaCl, 5 mM CaCl2, pH 7.4). After allowing two hours for polymerization, the bulk gel is diced and pushed through a 70 µm filter. The resultant liquid is pulse-sonicated on ice for six minutes, then filtered through a 40 µm filter. The particle solution is then frozen at -80°C and lyophilized into dry powder form.
While a number of different methods for drug-loading particles were attempted, the best outcomes were achieved through the addition of tazarotene to the initial bulk fibrin gel to a final concentration of 1 mM, prior to thrombin-mediated polymerization (Supplementary Fig. 9A). Due to tazarotene’s high solubility in ethanol, unincorporated tazarotene was able to be scavenged through ethanol dissolution of the residual fibrin and tazarotene mixture left after the first filtration step. All remaining steps in FBN production remain the same.
FBN Characterization
FBN size characterization was done via NanoSight particle tracking analysis (Malvern Panalytical) and atomic force microscopy (AFM, MFP 3D Bio AFM, Asylum). Using 2 mg/mL concentrations of FBNs in deionized water (diH2O), NanoSight was used to determine the concentration of particles per milligram of lyophilized particles from batch to batch. This was used to allow for conversion to particles/mL concentrations of FBNs. NanoSight was also used to determine average hydrodynamic particle diameters. For AFM characterization, FBNs were placed into 0.01 mg/mL solution in sterile PBS. A cleaned glass coverslip was covered in the solution and allowed to dry overnight. Particle characterization was done in air topography mode, with diameter data being collected for 10 particles.
FBN Gel Formation
FBN gels were formed through the addition of CaCl2 (5 mM final concentration) and FBNs to a patient co-factor. Porcine whole blood was collected through North Carolina State University Tissue Sharing Program. Platelet-poor plasma (New York Blood Center) was used for assays where red blood cells impeded visualization. Human α-thrombin (0.5 U/mL, Enzyme Research Labs) was used to polymerize gels. High-density fibrin glues (HDFG, Tisseel, Baxter; VistaSeal, Ethicon), were used as control surgical sealants throughout these studies. They were stored and formed following manufacturer’s instructions, without deviation.
FBN Gel Polymerization and Degradation
To investigate the tunability of FBN glue polymerization dynamics, a rheometer (Anton Paar MCR 92) with a cone-plate fixture was used. For 30 minutes following thrombin-initiated polymerization, oscillating time sweep analysis was performed using 0.5% strain, 1 Hz constant rates at 37°C, measuring every 0.1 seconds. Storage and loss moduli were captured at each measurement. Gelation time was defined as the time at which the storage modulus is three times larger than loss modulus. For each group, three replicates were used.
To evaluate degradation under the electrolyte balance of the body, 1 mL gel samples were formed and allowed to polymerize for one hour inside individual weigh boats, after which they were covered with 0.9% (isotonic) saline. At each hour time point, saline was drained, the gel was blotted, and then weighed. Timing resumed once the gel was re-submerged in saline solution. This proceeded for a total of 4 hours (4 time points). Five replicates were used for each group, except HDFG, for which 3 replicates were used. For 24-hour degradation, gels were left submerged at room temperature for 24 consecutive hours, followed by draining, blotting and weighing only at the end of 24 hours. Here, 3 replicates were used for all groups.
FBN Gel Mechanics
All mechanical assays were performed using an Instron 3400 Series Single-column Universal Testing Machine (Instron, Norwood, MA) and Bluehill software. For tensile studies, 1.5 mL of FBN gel were polymerized overnight, then clamped into the Instron (Fig. 2D). In order to minimize sample pre-load, gels were clamped into the top first and allowed to hang before being clamped below. Tension was administered at a rate of 0.01 mm/s until the point of rupture. Rupture force was recorded for 11-15 replicates per sample group, except for HDFG, for which 3 replicates were tested.
As shear strength is most applicable to clinical use for vascular anastomosis, we focused on this aspect of adhesion (Fig. 2D). 50 µL of FBN gel was polymerized for 1 hour between two glass coverslips, each affixed to a glass slide. Slides were clamped in the Instron and extension proceeded at 0.01 mm/sec. Shear strength was recorded for 7-11 replicates per sample group.
To approximate wound closure ability, 0.5 mL of FBN gel was applied to a 0.5 cm linear defect in a 1.5 ×2.5 cm piece of porcine carotid artery and allowed to polymerize overnight. Adult porcine carotid artery samples were collected from pigs available through the NCSU Tissue Sharing Program. Samples were loaded into the Instron, where extension proceeded at a rate of 0.01 mm/s (Fig. 2D, Supplementary Fig. 3). Extension at the point of sealant rupture was recorded for 8-10 replicates per sample type.
FBN Gel Sealant Test
For our use of this material as a surgical sealant, it was imperative that we test FBN gels’ sealant capacity and burst pressure. To test sealant capacity, 0.5 mL of FBN gel was applied to a 3 mm diameter puncture defect in latex tubing. After allowing 15 minutes for polymerization, the puncture surface was rested on a petri dish of water and 2% aniline blue dye was allowed to flow through. The latex tube was lifted from the surface and any aniline blue dye visible in the petri dish was taken as indication of ineffective seal formation, i.e. a leak pressure of 0 mbar. Tubing samples that passed this leak test were attached to an air pump and submerged in water. With the non-pump side of the tube sealed, increasing air pressure was applied to the tube in 10 mbar increments until biomaterial seal was broken, which was visualized through the appearance of bubbles. Air pressure at time of rupture was recorded as the leak pressure. Between 7 and 15 replicates were used for each sample group.
Long-Term Particle Stability Testing
To determine long-term stability of particle properties, we performed head-to-head comparison of 330 million (M) particles/mL FBN gels made with new FBNs ( < 1 month old, refrigerated) and with FBNs stored at room temperature for 1 year. These comparisons followed the same tensile, adhesive, and leak pressure protocols listed earlier. For tensile testing, 11 replicates were tested per group. For adhesive testing, 9-13 replicates were tested per group. For leak pressure testing, 7 replicates were tested per group.
FBN Gel Structural Analysis
FBN gel structure was imaged and characterized using both confocal microscopy and cryogenic scanning electron microscopy (cryoSEM), allowing for both gross and detailed visualization48,49,50,51,52,53. For confocal microscopy, 50 μL FBN gels with 2.5% (w/w) Alexa-Fluor 488 labeled fibrinogen (Thermo Fisher Scientific) were polymerized between a glass slide and coverslip for 1 hour, then imaged using a Zeiss Laser Scanning Microscope (LSM 710, Zeiss Inc.) at 40× magnification.
Five clots were formed per gel type, and a minimum of 3 random 5.67 μm z-stacks were acquired for each gel. ImageJ (National Institutes of Health) was used to produce 8-bit z-stack projections. Gel fiber density was determined by thresholding the images to produce a black-and-white binary image and then calculating the ration of fiber to background pixels in each image. For cryoSEM imaging, FBN gels of 150 μL were formed in 0.6 mL Eppendorf tubes and allowed to polymerize for 12 hours. Clots were rapidly plunge-frozen in super-cooled liquid nitrogen, fractured with a cold knife, etched for 10 minutes, and sputter-coated with gold. Imaging was performed at 1000×, 1500×, 2000×, and 2500× on two samples per gel type, in at least three random locations within the clot. ImageJ (National Institutes of Health) was used to perform image segmentation and determine pore size and percent porosity. FiberFit (Boise State University) was used to analyze fiber alignment54.
FBN Gel Stress-Relaxation and Standard Linear Viscoelastic (Kelvin) Model
As it is well-established that blood clots display viscoelastic material properties, we pursued a standard linear viscoelastic (Kelvin) model to describe the stress-relaxation properties of our whole blood FBN (WB-FBN) gels55,56,57. In this model, which can be thought of as a mechanical circuit, the time-dependent viscosity component of the material is modeled by a dashpot and a spring in series (spring constant \({k}_{2}\) > 0, damping coefficient c > 0, respectively). A second spring in parallel with the first component models the elastic properties of the material (spring constant k1 > 0, Supplementary Fig. 5C)58. This model may be expressed in a simple mathematical form:
where: \({\tau }_{1}=\frac{c}{{k}_{2}},{\tau }_{2}=c\left[\frac{1}{{k}_{1}}+\frac{1}{{k}_{2}}\right],{and}\,{\tau }_{2} \, > \,{\tau }_{1}\).
Here F(t) represents force as a function of time acting on the viscoelastic solid and u(t) represents displacement (stretch) over time. In this expression, \({\tau }_{1}\) may be thought of as the stress-relaxation time and \({\tau }_{2}\) may be thought of as the creep-relaxation time. We chose to use the Kelvin model, as it is the simplest model that accounts for both stress relaxation and creep. There are many extensions of the Kelvin model, through the addition of further parallel components, but our goal here was to determine and apply the simplest model that was able to reflect the viscoelastic properties of the WB-FBN gels.
We solved the Kelvin model as it relates to a (linear) ramp and hold displacement with a ramp time \({t}_{p}\), final displacement \({u}_{p}\), and initial force on the sample that is represented by \({F}_{o}\):
For the acquisition of stress-relaxation curves for validation of the Kelvin model, 0.5 mL WB gels, WB-FBN gels, and HDFG gels were produced using earlier described methods. Gels were polymerized into roughly 2 cm by 1 cm rectangles in weigh boats and allowed to polymerize overnight. Upon being clamped into the Instron UTS, gels were stretched (1 mm/sec) for 30 seconds, followed by 10 minutes held without additional displacement. Force measurements were taken every 0.1 seconds throughout stress and relaxation. Resultant curves were cleaned of noise by using a 20 point (2 second) moving average. The presence of outlier curves was determined through co-localized plotting and grossly variant curves were removed. No more than two curves were considered outliers per group.
Initial estimates for τ2, and k1 were made based on an initial guess for τ1 and calculated values derived from observed experimental values – time at peak (\({t}_{p}\)), final displacement (\({u}_{p}\)), initial force (\({F}_{o}\)), peak force (\({F}_{p}\)), and equilibrium force (\({F}_{\infty }\)):
This first estimation was used to initialize a least squares optimization via MatLab using a Nelder-Mead simplex (direct search) method (“fminsearch”). This resulted in estimated values for.\({\tau }_{1}\), \({\tau }_{2}\), and k1, which were found to be robust to perturbation of the initial guess. Cost and residuals were evaluated for goodness of fit (Supplementary Fig. 5), resulting in validation of the use of a Kelvin model for WB gels and WB-FBN gel groups with the addition of <400 M FBN/mL. Curves from WB-FBN gels with 400 M FBN/mL clearly demonstrated wave-like properties indicative of a regime in which inertial forces dominate. A Kelvin model adequately approximated curves from HDFG samples, but was not ideal (Supplementary Fig. 6). An extended Kelvin model, with the addition of another parallel kelvin body component (dashpot and spring in series), was applied to all samples, but only made a meaningful improvement in cost for HDFG samples. Hence, a Kelvin model was used to compare parameters across gel types.
Vasculogenesis Assay
The effects of tazarotene dosage on vascular network formation were investigated through the use of an established microfluidic vasculogenesis model (Supplementary Fig. 7A)21,59. HUVECs and HLFs were embedded in 2 mg/mL human fibrin gels made 25 mM HEPES buffer and 0.5 U/mL thrombin. Media channels in the microdevice (Supplementary Fig. 7A) were filled with HUVEC media supplemented with free tazarotene. Daily media changes and brightfield imaging were completed until cells were fixed with 4% paraformaldehyde at 1 week after seeding. Cells were permeabilized with 0.3% Triton X-100 (Sigma), immunostained with PECAM-1 antibody (ThermoFisher), and stained with phalloidin (Invitrogen) and DAPI (Invitrogen) in order to visualize networks of both HUVECs and HLFs. Imaging was performed using a confocal microscope (Olympus FV3000 laser scanning confocal microscope) with a 10× objective. At least 3 devices were imaged for each experimental group and 3 images were taken per device. ImageJ was used to quantify vascular network characteristics (average segment length, average segment width, average number of branch points, and total endothelial area).
For analysis of vascular network response to the biomaterials used in our in vivo surgical studies, we used a permutation of this vasculogenesis assay. Instead of embedding cells in fibrin gels in the central channel, cells were embedded in FBN gel (330 M FBNs/mL), tFBN gel, or HDFG, and cells were cultured with regular HUVEC media. Cell culture and imaging proceeded as described earlier. At least 3 devices per biomaterial were cultured with HUVECs and HLFs and at least another 3 devices were only cultured with HUVECs.
Thin Film Cell Culture
The effects of tazarotene released from bulk fibrin gels on individual cellular morphology was determined through the low-density culture of HUVECs on thin films of loaded fibrin gels. Fibrin gels with varying concentrations of bulk tazarotene incorporated were allowed to polymerize between two clean glass coverslips for 1 hour, in order to form thin films. Thin films of 80 µL were made using 2 mg/ml human fibrinogen (Enzyme Research Laboratories), HEPES buffer (25 mM), and 0.5 U/ml human thrombin. Upon removal of one glass coverslip, the remaining glass and attached gel were placed within the well of a 12-well plate and rinsed with PBS. HUVECs (15,000 cells/well) were cultured for 16 hours, at which point they were fixed and stained. Images of cells were captured at 10× using an EVOS FL Auto Imaging System, with at least 5 images taken per thin film. In order to validate the nanoparticle release of tazarotene from FBNs, 80 µL FBN gel (330 M particles/mL) thin films were formed with different relative ratios of tazarotene-loaded to unloaded FBNs. All other elements of the procedure were the same.
For analysis of HUVEC cellular morphology response to the biomaterials used in our in vivo surgical studies, we used a variation of the thin film protocols already described. Cells were cultured in the same manner on thin films of FBN gel, tFBN gel, and HDFG. Staining, imaging, and quantification proceeded following the earlier description. At least 3 thin films were analyzed per sample group, with at least 5 images taken per thin film.
In Vivo Vascular Wound Healing Model and Vascular Tissue Preservation
All in vivo experiments were approved by North Carolina State University Institutional Animal Care and Use Committee and conducted in Association for Assessment and Accreditation of Laboratory Animal Care international-accredited facilities. Our studies used 90 to 150-day old New Zealand White rabbits (1:1 male-to-female sex ratio; Charles River Laboratories) in order to investigate vascular healing following the use of FBN and tFBN gels as an adjunct sealant material following suture repair of a carotid artery injury (Fig. 4A, Supplementary Fig. 10A-B). While distinct from previous studies, our in vivo model follows established models for assessing vascular healing60,61,62,63,64,65,66. Rabbits were pre-treated for pain management with hydromorphone (0.1-0.3 mg/kg) or buprenorphine (0.05 mg/kg). Prior to anesthesia, rabbits were sedated with a one-time intramuscular injection of ketamine (10-20 mg/kg) and dexmedetomidine (0.025 mg/kg). Upon achievement of appropriate sedation, rabbits were intubated and anesthesia and analgesia persisted throughout surgery with maintenance via isoflurane ( < 5%), as well as ketamine constant rate infusion (CRI, 0.2-1.2 mg/kg/hr), lidocaine CRI (50-100 mcg/kg/hr), buprenorphine (0.05 mg/kg IV) and dexmedetomidine boluses during surgery (0.025-0.25 mg/Kg IM). A bupivacaine incisional block (2 mg/kg) was administered locally prior to incision into the neck and following final closure. Vital signs were monitored throughout surgery by dedicated staff.
Rabbits were fasted for 1-2 hours prior to surgery to minimize the likelihood of complications during intubation. Following sedation and intubation, the rabbit was placed in a dorsal recumbent position and the neck was shaved and cleaned with alternating antiseptic and alcohol scrubs. The right carotid artery was isolated from the surrounding connective tissue and muscle by using metal ring clips. The right carotid artery (CA) of each rabbit was clamped, longitudinally cut between the clamps, then repaired with 6-0 PDS using interrupted sutures with <1 mm between each to reduce the likelihood of stenosis or hypertrophy. The suture-line was sealed with 0.2 mL FBN gel, tFBN gel, HDFG, or nothing, with 7 rabbits per treatment group. 3 mL of blood was drawn from each animal after sutures were placed, which was used as a patient cofactor to make the FBN gel or tFBN gel in those treatment groups. The closure was performed in a layered fashion: muscle layer, fascia, subdermal, and dermal layers, each being closed sequentially. The closure used dissolvable sutures. Atipamezole was administered as needed as a reversal agent due to prolonged anesthesia. Prior to recovery from anesthesia, ultrasound was used to validate the patency of the surgical vessel and compare it to the non-surgical side.
Ultrasound imaging (Butterfly iQ) was performed at 1 week and 2 weeks after surgery to evaluate vessel patency. Prior to imaging, rabbits were sedated with a one-time intramuscular injection of ketamine (10–20 mg/kg) and dexmedetomidine (0.025 mg/kg). At 3 weeks after surgery, carotid arteries and surrounding tissues were collected in a 10% sucrose PBS solution. Tissues were exposed to a serial dilution (10%, 20%, 30% sucrose, each for 24 hours), prior to embedding in optimal cutting temperature medium. A 28-gauge syringe was used to fill the vessel lumen with optimal cutting temperature medium to minimize vessel tissue damage during freezing. Embedded tissues were frozen gradually via exposure to dry ice. After hardening of the optimal cutting temperature medium, embedded tissues were stored at -80°C.
Histologic Analysis of Vascular Tissue
Sectioning of tissues proceeded using a cryotome set to 5 µm thickness. Sections were fixed in 4% paraformaldehyde for 15 minutes. Hematoxylin and eosin (H&E) staining was performed using established protocols. These H&E sections were imaged using the 10× objective of an EVOS FL Auto Imaging System, with at least 3 sections imaged per animal. These images were analyzed for vessel cross-sectional area, wound percentage of vessel, and vessel thickness using ImageJ (Supplementary Fig. 10C). H&E sections were also analyzed by a veterinary pathologist under blinded conditions following best practices for toxicologic histopathology (Supplementary Fig. 11)24.
Fibrin immunohistochemistry was used to identify both any remnant FBNs or HDFG, as well as any evidence of widespread fibrin deposition. Anti-fibrin antibody (UC45) (Genetex 19079, 1:67 dilution), was used for this imaging, alongside a goat-anti-mouse secondary antibody. All samples were counter-stained using VectaShield mounting medium with DAPI. Samples were imaged using the 10× objective of an EVOS FL Auto Imaging System, with at least 3 sections imaged per animal. These images were analyzed for fibrin-integrated density using ImageJ.
RNA Extraction and Transcriptomic Analysis
Prior to transcriptomic analysis, RNA extraction was performed on the remaining cryo-preserved vessel tissue. Frozen tissue was homogenized in 0.5 mL of lysis buffer (Invitrogen) with the use of a beadmill. RNA extraction proceeded through the use of a TRIzol Plus RNA Purification Kit (Invitrogen), following the manufacturer’s instructions without deviation. Total purified RNA concentrations were determined using a NanoDrop 1000 spectrophotometer (Thermo Scientific). NanoDrop was also used to verify that all RNA samples were of appropriate purity (260/230 ratio > 1.8) for transcriptomic analysis. For quantification of RNA expression by tissues, we used the purified RNA samples in a NanoString nCounter study using a custom codeset (selected group of genes). NanoString protocols for sample preparation and testing were followed without deviation.
Biomaterial Thrombogenicity Analysis
Biomaterial thrombogenicity was compared using a modification of established techniques for determining activated partial thromboplastin time testing. A whole blood-activated partial thromboplastin time test was performed following manufacturer’s instructions, with the addition of 20 µL of lyophilized biomaterial at the bottom of the testing well. Time for gelation to occur was recorded for 3–5 replicates per sample group.
Statistical Methods
Statistical analysis was performed using GraphPad Prism 9 software. Data was evaluated using a one-way ANOVA with Tukey’s post hoc using a 95% confidence interval or an unpaired Student’s t-test. Significance was defined as p < 0.05. Where appropriate, outliers were excluded following ROUT evaluation (Q = 1%).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The raw numerical data used generate the figures in the article and Supplementary Figs. are available in Supplementary Data Files 1 and 2, respectively. The MATLAB code for the viscoelastic model can be found at (https://github.com/sanikapandit/NatureCommEng_ViscoelasticModel_MATLAB.git).
Code availability
All stress relaxation data used for viscoelastic modeling was measured using an Instron Universal Testing System. The MATLAB code used to develop the model can be found at (https://github.com/sanikapandit/NatureCommEng_ViscoelasticModel_MATLAB.git). All data plotting for the viscoelastic model was done on MATLAB and GraphPad Prism. All statistical analyses were computed on GraphPad Prism.
References
Hollister, S. J. Porous scaffold design for tissue engineering. Nat. Mater. 4, 518–524 (2005).
Truong, N. F. et al. Microporous annealed particle hydrogel stiffness, void space size, and adhesion properties impact cell proliferation, cell spreading, and gene transfer. Acta Biomater. 94, 160–172 (2019).
Anderson, A. R., Nicklow, E. & Segura, T. Particle fraction is a bioactive cue in granular scaffolds. Acta Biomater. 150, 111–127 (2022).
Pruett, L., Jenkins, C., Singh, N., Catallo, K. & Griffin, D. Heparin Microislands in Microporous Annealed Particle Scaffolds for Accelerated Diabetic Wound Healing. Adv. Funct. Mater. 31, 2104337 (2021).
Roosa, C. et al. Microfluidic Synthesis of Microgel Building Blocks for Microporous Annealed Particle Scaffold. J Vis Exp, https://doi.org/10.3791/64119 (2022).
Pruett, L. J. et al. De novo tissue formation using custom microporous annealed particle hydrogel provides long-term vocal fold augmentation. NPJ Regen. Med 8, 10 (2023).
Hench, L. L. & Polak, J. M. Third-generation biomedical materials. Science 295, 1014–1017 (2002).
Diller, R. B. & Tabor, A. J. The Role of the Extracellular Matrix (ECM) in Wound Healing: A Review. Biomimetics (Basel) 7, https://doi.org/10.3390/biomimetics7030087 (2022).
Bayer, I. S. Advances in Fibrin-Based Materials in Wound Repair: A Review. Molecules 27, https://doi.org/10.3390/molecules27144504 (2022).
Jackson, M. R. Fibrin sealants in surgical practice: An overview. Am. J. Surg. 182, 1s–7s (2001).
de Boer, M. T., Boonstra, E. A., Lisman, T. & Porte, R. J. Role of fibrin sealants in liver surgery. Dig. Surg. 29, 54–61 (2012).
Roosa, C. A. et al. Synthesis of sonicated fibrin nanoparticles that modulate fibrin clot polymerization and enhance angiogenic responses. Colloids Surf. B Biointerfaces 204, 111805 (2021).
Muhamed, I., Sproul, E. P., Ligler, F. S. & Brown, A. C. Fibrin Nanoparticles Coupled with Keratinocyte Growth Factor Enhance the Dermal Wound-Healing Rate. ACS Appl. Mater. Interfaces 11, 3771–3780 (2019).
Zasada, M. & Budzisz, E. Retinoids: active molecules influencing skin structure formation in cosmetic and dermatological treatments. Postepy Dermatol Alergol. 36, 392–397 (2019).
Motamedi, M., Chehade, A., Sanghera, R. & Grewal, P. A Clinician’s Guide to Topical Retinoids. J. Cutan. Med Surg. 26, 71–78 (2022).
Liu, P. et al. Tazarotene-loaded PLGA nanoparticles potentiate deep tissue pressure injury healing via VEGF-Notch signaling. Mater. Sci. Eng. C. Mater. Biol. Appl 114, 111027 (2020).
Yuan, M. et al. GelMA/PEGDA microneedles patch loaded with HUVECs-derived exosomes and Tazarotene promote diabetic wound healing. J. Nanobiotechnol. 20, 147 (2022).
Al Haj Zen, A. et al. The Retinoid Agonist Tazarotene Promotes Angiogenesis and Wound Healing. Mol. Ther. 24, 1745–1759 (2016).
Zhu, Z. et al. Tazarotene Released from Aligned Electrospun Membrane Facilitates Cutaneous Wound Healing by Promoting Angiogenesis. ACS Appl Mater. Interfaces 11, 36141–36153 (2019).
Mihalko, E. P. et al. Fibrin-specific poly(N-isopropylacrylamide) nanogels for targeted delivery of tissue-type plasminogen activator to treat thrombotic complications are well tolerated in vivo. Bioeng. Transl. Med 7, e10277 (2022).
Aw, W. Y. et al. Microphysiological vascular malformation model reveals a role of dysregulated Rac1 and mTORC1/2 in lesion formation. bioRxiv, 2022.2009.2003.506415, https://doi.org/10.1101/2022.09.03.506415 (2022).
Buckley, G. J., DeCubellis, J., Sharp, C. R. & Rozanski, E. A. Cardiopulmonary Resuscitation in Hospitalized Rabbits: 15 cases. J. Exot. Pet. Med. 20, 46–50 (2011).
Gardhouse, S. & Sanchez, A. Rabbit Sedation and Anesthesia. Vet. Clin. North Am. Exot. Anim. Pract. 25, 181–210 (2022).
Crissman, J. W. et al. Best practices guideline: toxicologic histopathology. Toxicol. Pathol. 32, 126–131 (2004).
Ullrich, H., Olschewski, M., Münzel, T. & Gori, T. Coronary In-Stent Restenosis: Predictors and Treatment. Dtsch Arztebl Int 118, 637–644 (2021).
Stilo, F. et al. The management of carotid restenosis: a comprehensive review. Ann. Transl. Med 8, 1272 (2020).
Chistiakov, D. A., Killingsworth, M. C., Myasoedova, V. A., Orekhov, A. N. & Bobryshev, Y. V. CD68/macrosialin: not just a histochemical marker. Lab. Investig. 97, 4–13 (2017).
Barros, M. H. M., Hauck, F., Dreyer, J. H., Kempkes, B. & Niedobitek, G. Macrophage polarisation: an immunohistochemical approach for identifying M1 and M2 macrophages. PloS one 8, e80908 (2013).
Bogatcheva, N. V., Garcia, J. G. & Verin, A. D. Molecular mechanisms of thrombin-induced endothelial cell permeability. Biochem. (Mosc.) 67, 75–84 (2002).
Bae, J. S., Kim, Y. U., Park, M. K. & Rezaie, A. R. Concentration dependent dual effect of thrombin in endothelial cells via Par-1 and Pi3 Kinase. J. Cell Physiol. 219, 744–751 (2009).
Griffin, D. R., Weaver, W. M., Scumpia, P. O., Di Carlo, D. & Segura, T. Accelerated wound healing by injectable microporous gel scaffolds assembled from annealed building blocks. Nat. Mater. 14, 737–744 (2015).
Darling, N. J. et al. Click by Click Microporous Annealed Particle (MAP) Scaffolds. Adv. Healthc. Mater. 9, 1901391 (2020).
Nih, L. R., Sideris, E., Carmichael, S. T. & Segura, T. Injection of Microporous Annealing Particle (MAP) Hydrogels in the Stroke Cavity Reduces Gliosis and Inflammation and Promotes NPC Migration to the Lesion. Adv. Mater. 29, 1606471 (2017).
Isaac, A. H. et al. Impact of PEG sensitization on the efficacy of PEG hydrogel-mediated tissue engineering. Nat. Commun. 15, 3283 (2024).
Kuang, G., Zhang, Q., Li, W. & Zhao, Y. Biomimetic Tertiary Lymphoid Structures with Microporous Annealed Particle Scaffolds for Cancer Postoperative Therapy. ACS Nano 18, 9176–9186 (2024).
Tigner, T. J. et al. Clickable Granular Hydrogel Scaffolds for Delivery of Neural Progenitor Cells to Sites of Spinal Cord Injury. Adv. Healthcare Materials 13, 2303912 (2024).
Ross, B. C. et al. Building-Block Size Mediates Microporous Annealed Particle Hydrogel Tube Microenvironment Following Spinal Cord Injury. Adv. Healthcare Materials 13, 2302498 (2024).
Caprio, N. D., Davidson, M. D., Daly, A. C. & Burdick, J. A. Injectable MSC Spheroid and Microgel Granular Composites for Engineering Tissue. Adv. Mater. 36, 2312226 (2024).
Pfaff, B. N., Flanagan, C. C. & Griffin, D. R. Microporous Annealed Particle (MAP) Scaffold Pore Size Influences Mesenchymal Stem Cell Metabolism and Proliferation Without Changing CD73, CD90, and CD105 Expression Over Two Weeks. Adv. Biol. 8, 2300482 (2024).
Mora-Boza, A., Ghebrezadik, S. G., Leisen, J. E. & García, A. J. Rapid and Facile Light-Based Approach to Fabricate Protease-Degradable Poly(ethylene glycol)−norbornene Microgels for Cell Encapsulation. Adv. Healthc. Mater. 12, 2300942 (2023).
Carvalho, B. G. et al. Gelatin methacryloyl granular scaffolds for localized mRNA delivery. Aggregate 5, e464 (2024).
Ataie, Z. et al. Accelerating Patterned Vascularization Using Granular Hydrogel Scaffolds and Surgical Micropuncture. Small 20, 2307928 (2024).
Miwa, H. et al. Improved Humoral Immunity and Protection against Influenza Virus Infection with a 3d Porous Biomaterial Vaccine. Adv. Sci. 10, 2302248 (2023).
Pepelanova, I. in Tunable Hydrogels: Smart Materials for Biomedical Applications (eds Antonina Lavrentieva, Iliyana Pepelanova, & Dror Seliktar) 1-35 (Springer International Publishing, 2021).
Jiang, C. et al. Self-healing polyurethane-elastomer with mechanical tunability for multiple biomedical applications in vivo. Nat. Commun. 12, 4395 (2021).
Worch, J. C. et al. Elastomeric polyamide biomaterials with stereochemically tuneable mechanical properties and shape memory. Nat. Commun. 11, 3250 (2020).
Brown, A. C. et al. Fibrin Network Changes in Neonates after Cardiopulmonary Bypass. Anesthesiology 124, 1021–1031 (2016).
Nellenbach, K., Guzzetta, N. A. & Brown, A. C. Analysis of the structural and mechanical effects of procoagulant agents on neonatal fibrin networks following cardiopulmonary bypass. J. Thromb. Haemost. 16, 2159–2167 (2018).
Sproul, E. P., Hannan, R. T. & Brown, A. C. Controlling Fibrin Network Morphology, Polymerization, and Degradation Dynamics in Fibrin Gels for Promoting Tissue Repair. Methods Mol. Biol. 1758, 85–99 (2018).
Valladolid, C. et al. Modulating the rate of fibrin formation and clot structure attenuates microvascular thrombosis in systemic inflammation. Blood Adv. 4, 1340–1349 (2020).
Nellenbach, K., Kyu, A., Guzzetta, N. & Brown, A. C. Differential sialic acid content in adult and neonatal fibrinogen mediates differences in clot polymerization dynamics. Blood Adv. 5, 5202–5214 (2021).
Sproul, E. P. et al. Development of biomimetic antimicrobial platelet-like particles comprised of microgel nanogold composites. Regen. Eng. Transl. Med 6, 299–309 (2020).
Sproul, E. P., Nandi, S., Roosa, C., Schreck, L. & Brown, A. C. Biomimetic microgels with controllable deformability improve healing outcomes. Adv Biosyst 2, https://doi.org/10.1002/adbi.201800042 (2018).
Morrill, E. E. et al. A validated software application to measure fiber organization in soft tissue. Biomech. Model Mechanobiol. 15, 1467–1478 (2016).
Kim, W.-J., Kang, J. G. & Kim, D.-W. Blood clot-inspired viscoelastic fibrin gel: New aqueous binder for silicon anodes in lithium ion batteries. Energy Storage Mater. 45, 730–740 (2022).
Lakshmanan, R. S., Efremov, V., O’Donnell, J. S. & Killard, A. J. Measurement of the viscoelastic properties of blood plasma clot formation in response to tissue factor concentration-dependent activation. Anal. Bioanal. Chem. 408, 6581–6588 (2016).
Rausch, M. K., Sugerman, G. P., Kakaletsis, S. & Dortdivanlioglu, B. Hyper-viscoelastic damage modeling of whole blood clot under large deformation. Biomech. Model. Mechanobiol. 20, 1645–1657 (2021).
Valdez-Jasso, D. et al. Viscoelastic mapping of the arterial ovine system using a Kelvin model. (2007).
Zhang, S., Wan, Z. & Kamm, R. D. Vascularized organoids on a chip: strategies for engineering organoids with functional vasculature. Lab Chip 21, 473–488 (2021).
Lu, Q. et al. End-to-end vascular anastomosis using a novel magnetic compression device in rabbits: a preliminary study. Sci. Rep. 10, 5981 (2020).
Guzeloglu, M., Reel, B., Atmaca, S., Bagrıyanık, A. & Hazan, E. The effects of PPARγ agonist rosiglitazone on neointimal hyperplasia in rabbit carotid anastomosis model. J. Cardiothorac. Surg. 7, 57 (2012).
Guzeloglu, M. et al. Effect of tadalafil on neointimal hyperplasia in a rabbit carotid artery anastomosis model. Ann. Thorac. Cardiovasc Surg. 19, 468–474 (2013).
Schiller, W. et al. Sutureless anastomoses of rabbit carotid arteries with BioGlue. J. Thorac. Cardiovasc Surg. 134, 1513–1518 (2007).
Sürer, S. et al. Effect of the P2Y12 antagonist ticagrelor on neointimal hyperplasia in a rabbit carotid anastomosis model. Interact. Cardiovasc Thorac. Surg. 19, 198–204 (2014).
Kavala, A. A., Kuserli, Y. & Turkyilmaz, S. Effect of N-acetylcysteine on intimal hyperplasia and endothelial proliferation in rabbit carotid artery anastomosis. Arch. Med Sci. 15, 1576–1581 (2019).
Yao, Y., Jeong, Y., Zaw, A. M., Kukumberg, M. & Yim, E. K. F. in Vascular Tissue Engineering: Methods and Protocols (eds Feng Zhao & Kam W. Leong) 177-189 (Springer US, 2022).
Acknowledgements
Thank you to the staff of the North Carolina State University Center for Veterinary Medicine, Large Animal Research center, and Central Procedures Laboratory, who were indispensable to the success of these studies. This work was performed in part at the Analytical Instrumentation Facility (AIF) at North Carolina State University, which is supported by the State of North Carolina and the National Science Foundation (award number ECCS-2025064). The AIF is a member of the North Carolina Research Triangle Nanotechnology Network (RTNN), a site in the National Nanotechnology Coordinated Infrastructure (NNCI). Some figure components were made using BioRender. Financial support for this work was provided by the National Science Foundation: CMMI 2235857 (ACB); National Heart, Lung, and Blood Institute: R01HL146701 (ACB); National Heart, Lung, and Blood Institute: 5F30HL163869 (NM); NIH 5T34GM131947-05 (NZ); NSF DGE-2137100 (SP and AS); NIH 5T32GM133366 (AS), an NC State University FRPD award (ACB) and the NC State University Chancellor’s Innovation award (ACB).
Author information
Authors and Affiliations
Contributions
Conceptualization: N.M., A.C.B., M.H., W.P., S.O. Methodology: N.M., S.P., N.Z., W.Y.A., K.N., A.S., J.L., M.H., B.T. Supervision: A.C.B., W.Y.A., W.P., M.H., S.O. Writing – original draft: N.M. Writing – review & editing: N.M., S.P., M.H., A.C.B., B.T., S.O., W.Y.A., W.P., J.L., E.C., N.Z., K.N., A.S.
Corresponding author
Ethics declarations
Competing interests
ACB is co-founder of Selsym Biotech Inc., a start-up company that focuses on clinical translation of hemostatic materials. ACB, NM, KN, and SP are inventors on a US Patent Application (18/921,390) titled “Colloidal Fibrin Nanoparticle Compositions and Uses” submitted by NC State University related to the materials described in this manuscript. All other authors declare no competing interests.
Peer review
Peer review information
Communications Engineering thanks Michael Monaghan, and the other, anonymous, reviewers for their contribution to the peer review of this work. Primary Handling Editors: [Inge Herrmann] and [Rosamund Daw].
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Moiseiwitsch, N.A., Pandit, S., Zwennes, N. et al. Colloidal-fibrillar composite gels demonstrate structural reinforcement, secondary fibrillar alignment, and improved vascular healing outcomes. Commun Eng 4, 67 (2025). https://doi.org/10.1038/s44172-025-00400-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44172-025-00400-x
This article is cited by
-
Editors’ Choice 2025
Communications Engineering (2026)
