
Abstract
Cardiorespiratory fitness (CRF) is a strong indicator of overall physical health, but its relevance for mental and neurocognitive health across the life course remains unclear. Here we synthesize evidence from cohort studies examining the associations between CRF and the risk of mental and neurocognitive disorders across all age groups in the general population. Twenty-seven studies comprising 4,007,638 individuals were included. Compared with low CRF, high CRF was associated with a reduced risk of depression (hazard ratio (HR) = 0.64; 95% confidence interval (CI), 0.56–0.74), all-cause dementia (HR = 0.61; 95% CI: 0.55–0.68) and psychotic disorders (HR = 0.71; 95% CI: 0.65–0.77) in adults. A one metabolic equivalent of task (1 MET; 3.5 ml kg−1 min−1) higher level of CRF was associated with lower risks of depression (HR = 0.95; 95% CI: 0.92–0.98) and all-cause dementia (HR = 0.81; 95% CI: 0.67–0.98). Overall certainty of evidence ranged from very low to moderate. These findings suggest that CRF may be a useful marker for identifying adults at increased risk of depression, dementia and psychotic disorders, highlighting the need for further large-scale longitudinal studies.
Similar content being viewed by others
Main
Mental and neurocognitive disorders are among the leading causes of disability burden worldwide1, affecting over 1.15 billion individuals in 20212. In addition, subthreshold symptoms can substantially impair quality of life and are associated with an increased risk of progression to a clinical diagnosis3. The etiology of mental and neurocognitive disorders involves a complex interaction of genetic, neurological, psychosocial, environmental and lifestyle factors, thus posing a challenge for the development of primary prevention strategies4,5.
Cardiorespiratory fitness (CRF) is a pivotal indicator of overall physical health, representing the ability of multiple physiological systems to efficiently deliver and use oxygen during sustained physical activity6. Genetics account for nearly half of the variation in CRF7, with the remaining influence being predominantly shaped by regular physical activity patterns8. Since early meta-analyses examining CRF utility as a predictor of health outcomes9, a substantial corpus of evidence from cohort studies has consistently highlighted the value of CRF in identifying individuals at heightened risk of mortality10 and cardiovascular diseases11. Consequently, CRF has been recognized as an important, readily measurable risk factor12,13, and its integration as a clinical vital sign has been specifically proposed for cardiovascular disease risk assessment14, providing precise insights that facilitate the development of physical activity recommendations and exercise prescriptions15.
A 2024 overview of meta-analyses of cohort studies indicates that CRF is a strong and consistent predictor of mortality and future chronic conditions such as stroke and type 2 diabetes mellitus among adults in the general population16. However, this study revealed the need for further evidence across additional health outcomes. CRF has been hypothesized to influence mental and neurocognitive health through various physiological and psychological mechanisms, including enhanced neuroplasticity, increased cerebral blood flow, reduced systemic inflammation and improved stress regulation17. So far, few meta-analyses have examined the associations between CRF and mental or neurocognitive disorders18,19. Each synthesized fewer than five primary studies, limiting the certainty of the available evidence and underscoring the need for additional high-quality research16. Furthermore, both meta-analyses were limited to adult populations and focused on anxiety, depression and all-cause dementia18,19. The recent surge in research on the determinants of mental and neurocognitive disorders underscores the urgent need to update this body of research4,5. From both clinical and public health perspectives, it is also important to clarify the role of CRF in the prevention of mental and neurocognitive health conditions across the lifespan, including less prevalent mental disorders such as neurodevelopmental and psychotic disorders. Accordingly, this Analysis synthesizes the available evidence from cohort studies on the associations between CRF levels and the risk of mental and neurocognitive disorders across all ages in the general population.
Results
Study selection
A total of 2,553 studies were considered for this title–abstract review; of these, 76 were fully assessed for eligibility and 49 were finally excluded (Supplementary Table 1), leaving a total of 27 cohort studies20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46 in the systematic review (Fig. 1).

Inclusion criteria were as follows: (1) general populations without mental or neurocognitive disorders at baseline, across all age groups, (2) CRF levels, (3) mental and neurocognitive health outcomes assessed either as clinical diagnoses or symptom severity measures, and (4) prospective or retrospective cohort studies published in peer-reviewed journals.
Study characteristics
Supplementary Tables 2 and 3 summarize the main characteristics of the studies included. The studies were published between 200928 and 202522. The follow-up period ranged from 4 (ref. 26) to 29 years46. The studies included a total of 4,007,638 individuals (30.5% female participants) in nine different countries, including Finland32,34,45, Germany41, Italy26, the Netherlands35, Norway27,29,31, Sweden24,25,30,34,39,42,43,46, Taiwan44, the United Kingdom20,22,33 and the United States21,23,28,36,37,38,40. The participants across studies were predominantly white (either of European ancestry or non-Hispanic in US cohorts). The mean age at baseline ranged from 10.6 (ref. 44) to 72.5 years26, comprising children under 12 years44 and adults aged 18–64 years20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,45,46 and 65 years or older26.
The CRF levels were estimated using direct32,41,45 or indirect20,21,22,23,24,25,26,27,28,29,30,31,33,34,35,36,37,38,39,40,42,43,44,46 measures through maximal or submaximal tests. The included studies provided data for CRF categories by standardizing the cutoff point for high and low levels according to participant’s age and sex22,23,26,27,28,29,30,31,32,33,35,36,38,40,42,43,45. Alternatively, data on age and sex were only adjusted in the estimate risk model25. Six studies were conducted exclusively among male participants30,32,39,42,43,45, and five studies disclosed data regarding study associations by sex20,26,28,37,40,44. The metrics used were distance26 or duration40,44 of field-based tests, metabolic equivalent of task (MET)20,21,22,23,28,33,34,36,37, peak workload30,35,39,42,43,46 and maximum oxygen consumption (VO2max)24,25,27,29,31,32,41,45. Cohort studies employed a single baseline assessment of CRF levels, with subsequent repeated measurements24,27,28,31,36,37. Analysis of CRF was performed as a continuous variable20,21,22,23,25,27,28,29,34,35,36,37,38,39,41,45 or as a comparison between categories22,23,25,26,27,28,29,30,31,32,33,35,36,38,40,42,43,44,45,46.
Mental and neurocognitive disorders, whether clinical diagnoses20,21,22,23,24,25,27,30,31,32,34,36,38,39,41,42,43,44,45,46 or manifestations of mild to severe symptoms26,28,29,33,35,37,40,41, primarily included anxiety disorders (hereafter anxiety)24,29,33,41,44, depressive disorders (hereafter depression)23,24,25,26,28,29,33,35,37,40,41,42,44, all-cause dementia20,21,22,27,30,31,32,34,36,38,46 and schizophrenia spectrum and other psychotic disorders (hereafter psychotic disorders)43,45. Table 1 summarizes the available cohort evidence on the associations between CRF and mental disorders in the general population.
Methodological quality and certainty of evidence
Among the included studies, 57.1% were rated as good quality and 42.9% were rated as fair quality (Supplementary Table 4). Cohort studies with fair quality were deficient in three key criteria: (1) a detailed definition of exposure measures; (2) multiple exposure measurements; and (3) an acceptable overall follow-up rate (>80%). A Grading of Recommendations, Assessment, Development and Evaluation (GRADE) assessment indicated moderate certainty of evidence for all-cause dementia and a very low certainty of evidence for anxiety, depression and psychotic disorders when comparing high versus low CRF. The GRADE assessment for a 1-MET increase in CRF indicated very low certainty of evidence for both depression and all-cause dementia. The very low certainty of evidence was primarily driven by risk of bias, inconsistency, imprecision and the inability to assess publication bias (Supplementary Tables 5 and 6).
Summary of outcomes not meta-analyzed
The prospective associations between CRF levels and some mental disorders were only analyzed in one study and were not included in the meta-analyses (Supplementary Table 3). In the general adult population, higher levels of CRF were significantly associated with a lower risk of bipolar and related disorders42, dissociative, obsessive–compulsive, somatic symptom and stressor-related disorders43, and sleep apnea39. Furthermore, higher levels of CRF were significantly associated with a reduced risk of anxiety and attention-deficit/hyperactivity disorder in children (boys and girls), whereas the association with depression was significant only in girls44.
Summary of outcomes meta-analyzed
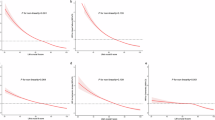
A total of 22 cohort studies20,21,22,23,25,26,27,28,29,30,31,32,33,35,36,37,38,40,42,43,44,45 were included in the meta-analyses. Given that the general adult population was mostly aged 18–64 years at baseline, the pooled hazard ratios (HRs) comparing the associations between the highest (versus lowest) category of CRF and the risk of mental and neurocognitive disorders (Fig. 2) were (1) 0.90 (95% CI: 0.75–1.09; I-squared (I2) = 56.9%; n = 2 (refs. 29,33)) for anxiety (n = 36,687; incident cases, 1,009; mild to severe symptoms; follow-up, 7–11 years); (2) 0.64 (95% CI: 0.56–0.74; I2 = 67.9%; predication interval (PI), 0.43–0.97; n = 9 (refs. 23,25,26,28,29,33,35,40,42)) for depression (n = 1,504,915; incident cases, 18,958; medical registry-based or mild to severe symptoms; follow-up, 4–17 years); (3) 0.61 (95% CI: 0.55–0.68; I2 = 0%; PI, 0.47–0.79; n = 7 (refs. 22,27,30,31,32,36,38)) for all-cause dementia (n = 1,287,561; incident cases, 4,170; medical registry-based; follow-up, 8–29 years); and (4) 0.71 (95% CI: 0.65–0.77; I2 = 0%; n = 2, male-only cohorts43,45) for psychotic disorders (n = 1,112,007; incident cases, 10,420; medical registry-based; follow-up, 23–25 years). One of the included studies did not report the number of incident cases for anxiety and depression33. In the meta-analysis of CRF as a continuous variable (Fig. 3), an increase of 1 MET (3.5 ml kg−1 min−1) was associated with a lower incidence of depression (HR = 0.95; 95% CI: 0.92–0.98; I2 = 17.0%; PI, 0.72–1.25; n = 5 (refs. 23,25,28,29,37); n = 362,256; incident cases, 6,158; medical registry-based or mild to severe symptoms; follow-up, 5–12 years) and all-cause dementia (HR = 0.81; 95% CI: 0.67–0.98; I2 = 97.3%; PI, 0.07–9.12; n = 5 (refs. 20,21,27,36,38); n = 123,229; incident cases, 2,971; medical registry-based; follow-up, 8–24 years).

Results from two-sided random-effects meta-analyses of prospective cohort studies are shown categorized by disorder: anxiety29,33, depression23,24,25,26,28,29,33,35,40,42, all-cause dementia22,27,30,31,32,36,38 and psychotic disorders43,45. Individual squares represent study-specific HRs, with horizontal lines indicating 95% CIs. Diamond symbols denote pooled HRs from random-effects models, and red horizontal bars indicate 95% prediction intervals where available (that is, when more than two studies are included). Point estimates represent HRs. HR values < 1 indicate a lower risk associated with higher CRF. Statistical inference is two-sided and based on 95% CIs, with no adjustments for multiple comparisons. ACLS, Aerobics Center Longitudinal Study; CCLS, Cooper Center Longitudinal Study; HPA, Health Profile Assessment; HUNT, Trøndelag Health Study; KIHD, Kuopio Ischemic Heart Disease study; MS, Maastricht Study; NR, not reported; ProVA, Progetto Veneto Anziani study; SMSCR, Swedish Military Service Conscription Register; UK, United Kingdom; UKB, UK Biobank; US, United States of America.

Results from two-sided random-effects meta-analyses of prospective cohort studies are shown categorized into depression23,24,25,28,29,37 and all-cause dementia20,21,27,36,38. Individual squares represent study-specific HRs, with horizontal lines indicating 95% CIs. Diamond symbols denote pooled HRs from random-effects models, and red horizontal bars indicate 95% prediction intervals. Point estimates represent HRs. HR values < 1 indicate a lower risk associated with higher CRF. Statistical inference is two-sided and based on 95% CIs, with no adjustments for multiple comparisons. Abbreviations as in Fig. 2.
Subgroup and sensitivity analysis
Subgroup analyses are presented in Supplementary Table 7. High (versus low) CRF was significantly associated with a lower risk of depression and all-cause dementia in participants younger than 50 years (HR = 0.64, 95% CI: 0.52–0.79 and HR = 0.62, 95% CI: 0.54–0.70, respectively) and those aged older than 50 years (HR = 0.65, 95% CI: 0.52–0.80 and HR = 0.60, 95% CI: 0.47–0.72, respectively). Similar associations were observed in both female (HR = 0.51; 95% CI: 0.39–0.66) and male (HR = 0.55; 95% CI: 0.51–0.60) participants for depression. In turn, the pooled HR remained statistically significant in studies of good and fair methodological quality, as well as in those assessing CRF using indirect maximal or submaximal tests and depression defined either by clinical diagnosis or by mild to severe self-reported symptoms. No significant differences were observed across subgroup comparisons (P > 0.05). Furthermore, the findings of sensitivity analyses were consistent with the primary results. The pooled effect sizes comparing the associations between the highest (versus lowest) category of CRF and the risk of depression and all-cause dementia were not modified when applying separate analyses by the type of risk estimate (Supplementary Table 8) and removing each study one by one (Supplementary Figs. 1 and 2). Finally, when a standardized effect size correction (Hedges’ g) was applied to mitigate potential biases, the results remained consistent (Supplementary Figs. 3 and 4).
Discussion
This systematic review and meta-analysis synthesizes the available evidence on the associations between CRF and the risk of mental and neurocognitive disorders in the general population across all age groups. Overall, high (versus low) CRF was associated with a reduced risk of depression (very low certainty), all-cause dementia (moderate certainty) and psychotic disorders (very low certainty, male-only evidence) in adults. No significant associations were found for anxiety (very low certainty). Furthermore, an increase of 1 MET (3.5 ml kg−1 min−1) in CRF was associated with a lower risk of depression and all-cause dementia (very low certainty). These findings suggest a potential role for CRF in mental and neurocognitive health, but given the very low certainty for most outcomes, the results should be interpreted with caution. Additional cohort studies are needed to confirm these findings, particularly for underrepresented populations (that is, individuals under 18 years and over 65 years), and to investigate mental disorders that are currently understudied or have not yet been examined.
The results align with previous systematic reviews and meta-analyses18,19 suggesting an inverse association of CRF with depression and all-cause dementia but extend the evidence base by incorporating a broader range of outcomes and a more comprehensive synthesis of available cohort studies. Specifically, this meta-analysis updates previous evidence in adults regarding anxiety, depression and all-cause dementia in adults18,19. Additionally, it integrates evidence on other mental disorders, including bipolar and related disorders, psychotic disorders, stressor-related disorders and sleep–wake disorders in adults, and anxiety, attention-deficit/hyperactivity disorder and depression in children. However, the limited number of studies restricts the ability to draw firm conclusions. Furthermore, no studies were found on certain mental disorders, such as autism spectrum disorders, disruption, impulse-control and conduct disorders, and feeding and eating disorders.
Several potential mechanisms may explain the observed protective associations of CRF on mental and neurocognitive disorders. From a physiological perspective, exercise and CRF improvements induce structural, cellular and molecular adaptations in the brain that enhance neuroplasticity and support cognitive and emotional regulation17,47,48. One key pathway involves the reduction of systemic inflammation and oxidative stress, both of which are implicated in the pathophysiology of mental and neurocognitive disorders17,49. Improvements in cardiovascular health may further mediate this relationship, as higher CRF is linked to better vascular function and cerebral perfusion, which help reduce inflammation and support brain integrity17. Chronic inflammation and oxidative damage have been associated with neurodegeneration, impaired synaptic function and disruptions in neurotransmitter systems, which may contribute to the onset and progression of conditions such as depression49 and dementia17. Additionally, exercise and higher CRF has been shown to promote hippocampal volumetric retention, a key neuroprotective adaptation given the hippocampus’ role in emotion regulation, memory and cognitive resilience17. Atrophy in this region has been consistently linked to mental50,51 and neurocognitive52 disorders. Moreover, higher CRF has been associated with increased global white-matter volume and local integrity53, which are essential for maintaining efficient neural connectivity and information processing. Deficits in white-matter microstructure have been observed in individuals with mental and neurocognitive disorders54,55,56,57, suggesting that CRF-related improvements may contribute to better cognitive and emotional stability. Furthermore, regular physical activity58, a major determinant of CRF59, has been shown to regulate the hypothalamic–pituitary–adrenal axis by reducing cortisol levels and blunting excessive stress responses60. Dysregulation of this axis is a well-established mechanism in the development of certain mental and neurocognitive disorders61,62, highlighting the potential role of CRF in modulating neuroendocrine function and improving stress resilience.
Despite biological plausibility, reverse causation remains a major challenge in disentangling the relationship between CRF and mental or neurocognitive health. Prodromal disorders and subthreshold symptoms may precede the observed associations and contribute to higher risk of mental and neurocognitive disorder63,64 and to lower CRF levels65,66,67, for instance through reduced motivation or engagement in physical activity49,68. Such temporal bias could lead to overestimation of the protective effects attributed to CRF. Although all studies included in this meta-analysis excluded participants with clinically diagnosed mental or neurocognitive disorders at baseline, there remains a possibility that early, undetected symptoms could have influenced CRF trajectories. However, bidirectional Mendelian randomization studies suggest a causal effect of physical activity on depression, with no evidence for the reverse direction69. So far, one genetically informed analysis examining CRF and Alzheimer’s disease has reported no statistically significant findings20, underscoring the need for further studies applying this approach. Addressing this challenge will require longitudinal cohorts with repeated CRF and mental and neurocognitive health assessments, the use of time-varying exposure models and, where feasible, multistate approaches to capture dynamic transitions between health states. Beyond observational evidence, randomized controlled trials are needed to establish whether specifically improving CRF can prevent the onset or progression of mental and neurocognitive disorders. Although numerous trials show robust antidepressant effects of exercise across baseline depression severity70, as well as promising cognitive benefits17, few have formally examined whether gains in CRF mediate these outcomes. Future trials should therefore incorporate neurobiological markers of neuroplasticity and behavioral indices of self-regulation to stratify participants, identify responders and optimize design48. Embedding such precision approaches into trial methodology will maximize CRF improvements, strengthen causal inference, and clarify the contribution of CRF to mental and neurocognitive health trajectories.
Genetic factors also warrant consideration when interpreting the link between CRF and mental or neurocognitive outcomes. In adults, responses to physical training vary considerably, with some individuals showing large improvements in CRF, and others only minimal gains71,72. Approximately half of this interindividual variability appears to be heritable7, suggesting that genetic factors may contribute to the observed findings. It is therefore plausible that part of the associations between CRF and mental or neurocognitive disorders reflects genetic pleiotropy, whereby individuals genetically predisposed to higher CRF also have a lower genetic liability for these disorders. However, evidence supporting this hypothesis remains limited. For instance, a large genome-wide association study found no single-nucleotide polymorphisms reaching statistical significance for exercise-induced changes in VO2max72, although recent evidence has identified candidate loci and polygenic predictors explaining a proportion of its variance73. The biological mechanisms through which these genetic variants influence CRF remain largely unclear71,74. Notably, CRF-associated genetic variants are involved in the regulation of gene expression in key cardiometabolic tissues75, and exercise may induce epigenetic modifications such as DNA methylation and microRNA activity76 that could mediate its long-term neuroprotective effects17. In addition, evidence on racial and ethnic differences in CRF remains inconsistent and often attenuates after adjustment for metabolic, lifestyle and socioeconomic factors77, suggesting that observed disparities are largely explained by modifiable environmental influences rather than fixed biological differences.
Importantly, CRF is a highly modifiable trait, and physical activity and exercise interventions can substantially improve it while simultaneously activating converging molecular and systemic pathways that support neuroplasticity, neurovascular health, immune regulation and metabolic resilience, including the upregulation of brain-derived neurotrophic factor and other neurotrophins, enhanced angiogenesis, modulation of gut microbiota, improved mitochondrial function, and reduced neuroinflammation and oxidative stress17,78. They also confer psychosocial benefits such as enhanced social support, self-esteem, self-efficacy and body image79,80. Overall, these considerations underscore the need for future research integrating genomic data and family-based designs to disentangle causality and to clarify the relative contributions of genetic, sociocultural and behavioral components of CRF to mental and neurocognitive health outcomes.
Despite the robust methodology employed in this meta-analysis, several limitations should be acknowledged. First, the limited number of available studies restricted the ability to explore or complete subgroup analyses (for example, by geographic region or CRF assessment method) and was insufficient (n < 10) to allow additional statistical assessments such as meta-regression or publication bias analyses81,82. As a result, the potential influence of sources of heterogeneity, residual confounding, and unpublished or selectively reported findings cannot be excluded. Second, some pooled estimates were accompanied by moderate to substantial between-study heterogeneity. Part of this heterogeneity may reflect methodological differences, such as variation in CRF assessments, outcome definitions and covariate adjustment strategies, which could introduce bias. Third, residual confounding due to mostly unmeasured factors—such as genetic predispositions, chronic pain, multimorbidity, social support and lifestyle behaviors (for example, physical activity, diet, smoking status)—cannot be ruled out. Fourth, subgroup analyses by age were based on aggregated study-level data rather than individual participant data, limiting the ability to draw definitive conclusions about age-specific associations. Fifth, because most cohorts consisted predominantly of white participants (either of European ancestry or non-Hispanic in US cohorts), generalizability to racially and ethnically diverse populations may be limited. Similarly, evidence for psychotic disorders was derived exclusively from two male conscript cohorts, limiting generalizability to female participants. Lastly, future studies should explore within-person variability in CRF over time and develop standardized CRF categories with defined cutoff values to enable dose–response analyses and inform thresholds for mental and neurocognitive risk reduction.
The findings have important implications for public health, clinical practice and future research. Given the inverse associations observed with depression, psychotic disorders (male-only evidence) and particularly all-cause dementia (moderate-certainty evidence for high versus low CRF), incorporating CRF into population-based evaluations could be considered. Measuring CRF may help identify individuals at increased risk of mental and neurocognitive disorders and inform interventions such as structured exercise programs and physical activity promotion aimed at improving CRF. This study underscores key limitations in the current body of evidence and offers specific recommendations to enhance the methodological quality and comparability of future research on the study associations (Supplementary Table 9). Briefly, it is recommended that future studies concentrate on identifying optimal CRF thresholds for mental and neurocognitive health benefits and explore potential sex- and age-specific associations. Accordingly, normalizing CRF to fat-free mass in future studies would improve the precision and comparability of measurements83. Additionally, subsequent studies should track co-existing long-term health conditions as part of the clinical complexity of general adult populations and examine how specific patterns (for example, accumulation, clusters, trajectories) may influence the associations under investigation. Genetically informed designs, such as Mendelian randomization studies using genetic variants associated with CRF, could help clarify the causal direction of these associations and disentangle genetic from behavioral or environmental pathways. Considering that physical activity and CRF are related but distinct phenotypes, future studies employing this approach should examine their independent and combined associations with mental and neurocognitive disorders. In addition, methods such as linkage disequilibrium score regression could be applied to quantify genetic correlations, providing complementary evidence on shared genetic architecture even in the absence of genome-wide significant variants. Finally, given the potential influence of population health profiles, healthcare systems, socioeconomic conditions, lifestyle factors and disease burden across different contexts, the results of this study underscore the need for future research to include underrepresented populations—both racially and ethnically diverse groups and those from regions such as Africa, Asia, Latin America and the Caribbean, and Oceania—to enhance the generalizability and applicability of evidence related to CRF and mental and neurocognitive disorders.
Conclusion
This systematic review and meta-analysis provides a comprehensive synthesis of the evidence on the associations between CRF and the incidence of mental and neurocognitive disorders in the general population across all age groups. The findings suggest that higher CRF is associated with lower risks of depression, dementia and psychotic disorders (male-only evidence) in adults. CRF may be considered a candidate marker for risk stratification. However, additional cohort studies are needed to clarify its preventive potential, particularly for anxiety, depression and psychotic disorders, where evidence remains of very low certainty. Other mental disorders have only been examined in single studies, limiting the ability to draw firm conclusions. Evidence across specific age groups, including children, adolescents and older adults, should be examined for all mental disorders to ensure comprehensive coverage across the lifespan.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 (ref. 84) and the Meta-analysis of Observational Studies in Epidemiology (MOOSE)85 statements. The study protocol was registered with PROSPERO (CRD42024547081). Two researchers (V.D.-G. and B.B.-P.) independently conducted the literature search, screening, study selection, data extraction, methodological quality, and certainty of evidence assessments. Any disagreements were resolved by consensus after consultation with a third investigator (V.M.-V.). The following sections provide a concise overview of the methods employed. Additional methodological details are available in Supplementary Methods.
Data sources and search strategy
The search process was conducted in accordance with the PRISMA-S guidelines86. Systematic searches were conducted in the following electronic databases from inception to 20 January 2025: PsycINFO, PubMed, Scopus, SPORTDiscus and Web of Science. Additional search methods were performed on online resources (Google Scholar) and citation searching (references of included studies and relevant systematic reviews). A comprehensive account of the search strategies employed is provided in Supplementary Table 10.
Eligibility criteria
To be included, studies retrieved from the scientific literature must report the following: (1) participants (general populations without mental or neurocognitive disorders at baseline assessments, encompassing all age groups); (2) exposure (CRF levels estimated via three methods16: (i) maximal cardiopulmonary exercise tests with gas analysis (that is, direct measures of VO2max), (ii) maximal or submaximal exercise tests (laboratory or field-based) without gas analysis (that is, indirect measures using exercise prediction equations or exercise performance data) or (iii) non-exercise prediction equations); (3) comparison (low levels of CRF); (4) outcome (mental and neurocognitive disorders, categorized according to the DSM-5-TR (Diagnostic and Statistical Manual of Mental Disorders, 5th edition–text revision) classification of the American Psychiatric Association87, were considered either as clinical diagnoses or as measures of symptom severity); and (5) study design (prospective or retrospective cohort studies published in peer-reviewed journals). No language or publication date restrictions were applied. The eligibility criteria are detailed in Supplementary Methods.
Study selection
All identified studies were uploaded to the Rayyan review system online88 and underwent deduplication. Subsequently, a two-step process was used. First, studies that did not address the study associations in the general population, as indicated by their title and abstract, were excluded. Second, the remaining studies were analyzed in full to ascertain whether they met the eligibility criteria.
Data extraction
The following data were extracted from the included studies: (1) authors and year of publication; (2) country where the data were collected; (3) main cohort or register; (4) data collection period and years of follow-up; (5) characteristics of the study population, including sample size, age, percentage of female participants, and body mass index; (6) characteristics related to CRF, including type of measure, assessment test, metric applied, mean value and data analysis (comparison across CRF categories and/or higher CRF as a continuous variable); (7) mental and neurocognitive health outcomes and assessment tools; and (8) prospective study associations, including effect size estimates and covariate adjustments. Data extraction was performed using Microsoft Excel (version 2510; Microsoft Corporation) between March and May 2025.
Methodological quality and certainty of evidence
The methodological quality of the cohort studies was evaluated using the National Institutes of Health (NIH) Quality Assessment Tool for Observational Cohort Studies89. The GRADE methodology was employed to determine the certainty of the evidence90. A summary of the details pertaining to the quality assessment tools for grading cohort studies is provided in Supplementary Methods.
Effect sizes
The studies mostly used HRs and odds ratios (ORs) as effect size estimators. Given the analysis of general populations (that is, excluding individuals with mental and neurocognitive disorders at baseline) and the low incidence of events across most included studies during follow-up periods (<12%), ORs and HRs were assumed to be equivalent and were thus combined as HRs82,91,92. Accordingly, the HRs and 95% CIs were considered the effect size for the meta-analyses and subjected to log transformations before being analyzed82. An HR value of less than 1 indicates a lower risk of mental and neurocognitive disorders in favor of higher levels of CRF. A complete list of effect sizes and the primary results from the studies included are provided in Supplementary Table 3.
Data synthesis
Meta-analyses were performed when at least two studies addressed the same outcome93. To facilitate the interpretation and comparison between studies, separate analyses were performed depending on whether CRF was reported as categorical (highest versus lowest levels as the reference category) or continuous (1-MET increase, that is, 3.5 ml kg−1 min−1) variables. Meta-analyses were conducted using a random effect model with the Sidik–Jonkman method94. Heterogeneity was estimated using the I2 statistic and classified as not important (0–40%), moderate (30–60%), substantial (50–90%) or considerable (75–100%)82. For I2 values falling within overlapping ranges, the corresponding P values were incorporated to enhance interpretation83. PIs were also reported to quantify the expected between-study dispersion of true effects82. Forest plots were used to display the pooled HRs for the associations between CRF (that is, highest versus lowest levels or 1-MET increase) and the risk of mental and neurocognitive disorders. Subgroup analyses were performed according to participant characteristics (age and sex), CRF assessment method, outcome measure and methodological quality of the included studies. Given the limited availability of stratified results by age groups within individual studies, subgroup analyses were performed based on the mean age of the study participants at baseline. Sensitivity analyses were performed to assess the robustness of the summary estimates using the leave-one-out method82 and performing separate analyses by the type of risk estimate applied in the included studies (HR and OR). Additionally, a sensitivity analysis was performed to calculate the standardized effect size, expressed as Hedges’ g, to account for potential biases arising from unequal sample sizes and variability in the outcome assessment tools82. Other methodological considerations pertaining to data collection and analysis are provided in Supplementary Methods.
Statistics and reproducibility
This study was a systematic review and meta-analysis of previously published data (observational cohort evidence). No statistical method was used to predetermine sample size, as sample sizes were defined by the included studies. No data were excluded from the analyses other than those not meeting the predefined eligibility criteria. Randomization and blinding were not applicable. All analyses were conducted following established Cochrane methodological guidelines to ensure transparency and reproducibility82. Statistical significance was set at a two-sided P < 0.05. All analyses were conducted using R software version 4.4.0 (R Foundation for Statistical Computing) with the meta95 and metafor96 packages.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
This systematic review and meta-analysis does not include original data. All data were extracted from published studies and are publicly available. The unprocessed data correspond to the original effect size estimates and related values reported in the included studies. The meta-analytic database generated and analyzed in this study, including study identifiers, effect sizes, confidence intervals and data used for visualization, is available via the Open Science Framework repository97.
Code availability
Analyses were performed using standard functions in R software with the meta and metafor packages. The R code used to conduct the meta-analysis is available via the Open Science Framework repository97.
References
GDB Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 9, 137–150 (2022).
2021 Global Burden of Disease study (Institute of Health Metrics and Evaluation and Global Health Data Exchange (GHDx), 2025); https://vizhub.healthdata.org/gbd-results/
Volz, H. P., Stirnweiβ, J., Kasper, S., Möller, H. J. & Seifritz, E. Subthreshold depression – concept, operationalisation and epidemiological data. A scoping review. Int. J. Psychiatry Clin. Pract. 27, 92–106 (2023).
Herrman, H. et al. Time for united action on depression: a Lancet–World Psychiatric Association Commission. Lancet 399, 957–1022 (2022).
Livingston, G. et al. Dementia prevention, intervention and care: 2024 report of the Lancet standing Commission. Lancet 404, 572–628 (2024).
Caspersen, C. J., Powell, K. E. & Christenson, G. M. Physical activity, exercise and physical fitness: definitions and distinctions for health-related research. Public Health Rep 100, 126–131 (1985).
Bouchard, C. et al. Familial resemblance for VO2max in the sedentary state: the HERITAGE family study. Med. Sci. Sports Exerc. 30, 252–258 (1998).
Myers, J., Kokkinos, P., Arena, R. & LaMonte, M. J. The impact of moving more, physical activity, and cardiorespiratory fitness: why we should strive to measure and improve fitness. Prog. Cardiovasc. Dis. 64, 77–82 (2021).
Kodama, S. et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 301, 2024–2035 (2009).
Myers, J. et al. Exercise capacity and mortality among men referred for exercise testing. N. Engl. J. Med. 346, 793–801 (2002).
Pettee Gabriel, K. et al. Analysis of cardiorespiratory fitness in early adulthood and midlife with all-cause mortality and fatal or nonfatal cardiovascular disease. JAMA Netw. Open 6, e230842 (2023).
Nauman, J. et al. Prediction of cardiovascular mortality by estimated cardiorespiratory fitness independent of traditional risk factors: the HUNT Study. Mayo Clin. Proc. 92, 218–227 (2017).
Kaminsky, L. A. et al. Cardiorespiratory fitness and cardiovascular disease—the past, present and future. Prog. Cardiovasc. Dis. 62, 86–93 (2019).
Ross, R. et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American Heart Association. Circulation 134, e653–e699 (2016).
Fletcher, G. F. et al. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation 128, 873–934 (2013).
Lang, J. J. et al. Cardiorespiratory fitness is a strong and consistent predictor of morbidity and mortality among adults: an overview of meta-analyses representing over 20.9 million observations from 199 unique cohort studies. Br. J. Sports Med. 58, 556–566 (2024).
Tari, A. R., Walker, T. L., Huuha, A. M., Sando, S. B. & Wisloff, U. Neuroprotective mechanisms of exercise and the importance of fitness for healthy brain ageing. Lancet 405, 1093–1118 (2025).
Lee, J. Influence of cardiorespiratory fitness on risk of dementia and dementia mortality: a systematic review and meta-analysis of prospective cohort studies. J. Aging Phys. Act. 29, 878–885 (2021).
Kandola, A., Ashdown-Franks, G., Stubbs, B., Osborn, D. P. J. & Hayes, J. F. The association between cardiorespiratory fitness and the incidence of common mental health disorders: a systematic review and meta-analysis. J. Affect. Disord. 257, 748–757 (2019).
Lu, H. et al. Observational and genetic associations between cardiorespiratory fitness and age-related diseases: longitudinal analyses in the UK Biobank study. EPMA J. 15, 629–641 (2024).
Meernik, C. et al. Dietary patterns and cardiorespiratory fitness in midlife and subsequent all-cause dementia: findings from the cooper center longitudinal study. Int. J. Behav. Nutr. Phys. Act. 21, 109 (2024).
Wang, S. et al. Association of cardiorespiratory fitness with dementia risk across different levels of genetic predisposition: a large community-based longitudinal study. Br. J. Sports Med. 59, 150–158 (2025).
Willis, B. L. et al. Association of midlife cardiorespiratory fitness with incident depression and cardiovascular death after depression in later life. JAMA Psychiatry 75, 911–917 (2018).
Wiklund, C. A. et al. Change in cardiorespiratory fitness and risk of depression, anxiety, and cerebrovascular disease. Am. J. Prev. Med. 67, 849–858 (2024).
Wiklund, C. A., Ekblom, Ö., Paulsson, S., Lindwall, M. & Ekblom-Bak, E. Cardiorespiratory fitness in midlife and subsequent incident depression, long-term sickness absence, and disability pension due to depression in 330,247 men and women. Prev. Med. 181, 107916 (2024).
Veronese, N. et al. Poor physical performance predicts future onset of depression in elderly people: Progetto Veneto Anziani longitudinal study. Phys. Ther. 97, 659–668 (2017).
Tari, A. R. et al. Temporal changes in cardiorespiratory fitness and risk of dementia incidence and mortality: a population-based prospective cohort study. Lancet Public Health 4, e565–e574 (2019).
Sui, X. et al. Prospective study of cardiorespiratory fitness and depressive symptoms in women and men. J. Psychiatr. Res. 43, 546–552 (2009).
Shigdel, R., Stubbs, B., Sui, X. & Ernstsen, L. Cross-sectional and longitudinal association of non-exercise estimated cardiorespiratory fitness with depression and anxiety in the general population: the HUNT study. J. Affect. Disord. 252, 122–129 (2019).
Nyberg, J. et al. Cardiovascular and cognitive fitness at age 18 and risk of early-onset dementia. Brain 137, 1514–1523 (2014).
Lerfald, M. et al. Longitudinal patterns of systolic blood pressure, diastolic blood pressure, cardiorespiratory fitness, and their association with dementia risk: the HUNT study. J. Gerontol. A 79, glae161 (2024).
Kurl, S., Laukkanen, J. A., Lonnroos, E., Remes, A. M. & Soininen, H. Cardiorespiratory fitness and risk of dementia: a prospective population-based cohort study. Age Ageing 47, 611–614 (2018).
Kandola, A. A., Osborn, D. P. J., Stubbs, B., Choi, K. W. & Hayes, J. F. Individual and combined associations between cardiorespiratory fitness and grip strength with common mental disorders: a prospective cohort study in the UK Biobank. BMC Med. 18, 303 (2020).
Hietanen, H., Pietilä, A., Kähönen, M. & Salomaa, V. Ankle blood pressure and dementia: a prospective follow-up study. Blood Press Monit 18, 16–20 (2013).
Gianfredi, V. et al. The association between cardio-respiratory fitness and incident depression: the Maastricht Study. J. Affect. Disord. 279, 484–490 (2021).
Gafni, T. et al. Independent and joint associations of cardiorespiratory fitness and BMI with dementia risk: the Cooper Center Longitudinal Study. BMJ Open. 13, e075571 (2023).
Dishman, R. K. et al. Decline in cardiorespiratory fitness and odds of incident depression. Am. J. Prev. Med. 43, 361–368 (2012).
DeFina, L. F. et al. The association between midlife cardiorespiratory fitness levels and later-life dementia: a cohort study. Ann. Intern. Med. 158, 162–168 (2013).
Crump, C., Sundquist, J., Winkleby, M. A. & Sundquist, K. Cardiorespiratory fitness and long-term risk of sleep apnea: a national cohort study. J. Sleep Res. 28, e12851 (2019).
Becofsky, K. M. et al. A prospective study of fitness, fatness and depressive symptoms. Am. J. Epidemiol. 181, 311–320 (2015).
Baumeister, S. E. et al. Associations of leisure-time and occupational physical activity and cardiorespiratory fitness with incident and recurrent major depressive disorder, depressive symptoms, and incident anxiety in a general population. J. Clin. Psychiatry 78, e41–e47 (2017).
Åberg, M. A. I. et al. Cardiovascular fitness in males at age 18 and risk of serious depression in adulthood: Swedish prospective population-based study. Br. J. Psychiatry 201, 352–359 (2012).
Nyberg, J. et al. Cardiovascular fitness in late adolescent males and later risk of serious non-affective mental disorders: a prospective, population-based study. Psychol. Med. 48, 416–425 (2017).
Chiang, H. L. et al. Physical fitness and risk of mental disorders in children and adolescents. JAMA Pediatr 178, 595–607 (2024).
Kunutsor, S. K., Kauhanen, J. & Laukkanen, J. A. Frequent sauna bathing and psychosis: interrelationship with cardiorespiratory fitness. J. Psychiatr. Res. 175, 75–80 (2024).
Hörder, H. et al. Midlife cardiovascular fitness and dementia: a 44-year longitudinal population study in women. Neurology 90, e1298–e1305 (2018).
Kandola, A., Hendrikse, J., Lucassen, P. J. & Yücel, M. Aerobic exercise as a tool to improve hippocampal plasticity and function in humans: practical implications for mental health treatment. Front. Hum. Neurosci. 10, 373 (2016).
Smith, P. J. & Merwin, R. M. The role of exercise in management of mental health disorders: an integrative review. Annu. Rev. Med. 72, 45–62 (2021).
Hird, E. J., Slanina-Davies, A., Lewis, G., Hamer, M. & Roiser, J. P. From movement to motivation: a proposed framework to understand the antidepressant effect of exercise. Transl. Psychiatry 14, 273 (2024).
Bray, M. J. C. et al. Hippocampal atrophy is associated with psychotic symptom severity following traumatic brain injury. Brain Commun. 3, fcab026 (2021).
Cole, J., Costafreda, S. G., McGuffin, P. & Fu, C. H. Y. Hippocampal atrophy in first episode depression: a meta-analysis of magnetic resonance imaging studies. J. Affect. Disord. 134, 483–487 (2011).
Song, T. et al. Mitochondrial dysfunction, oxidative stress, neuroinflammation, and metabolic alterations in the progression of Alzheimer’s disease: a meta-analysis of in vivo magnetic resonance spectroscopy studies. Ageing Res. Rev. 72, 101503 (2021).
Maleki, S. et al. Associations of cardiorespiratory fitness and exercise with brain white matter in healthy adults: a systematic review and meta-analysis. Brain Imaging Behav 16, 2402–2425 (2022).
Fields, R. D. White matter in learning, cognition and psychiatric disorders. Trends Neurosci 31, 361–370 (2008).
Flinkenflügel, K. et al. Associations between white matter microstructure and cognitive decline in major depressive disorder versus controls in Germany: a prospective case-control cohort study. Lancet Psychiatry 11, 899–909 (2024).
Koshiyama, D. et al. White matter microstructural alterations across four major psychiatric disorders: mega-analysis study in 2,937 individuals. Mol. Psychiatry 25, 883–895 (2019).
Shafer, A. T. et al. Accelerated decline in white matter microstructure in subsequently impaired older adults and its relationship with cognitive decline. Brain Commun. 4, fcac051 (2022).
Bizzozero-Peroni, B. et al. Daily step count and depression in adults: a systematic review and meta-analysis. JAMA Netw. Open 7, e2451208 (2024).
Knaeps, S., Bourgois, J. G., Charlier, R., Mertens, E. & Lefevre, J. Associations between physical activity and health-related fitness - volume versus pattern. J. Sports Sci. 35, 539–546 (2017).
Anderson, T., Berry, N. T. & Wideman, L. Exercise and the hypothalamic-pituitary-adrenal axis: a special focus on acute cortisol and growth hormone responses. Curr. Opin. Endocr. Metab. Res. 9, 74–77 (2019).
Misiak, B. et al. The HPA axis dysregulation in severe mental illness: can we shift the blame to gut microbiota? Prog. Neuropsychopharmacol. Biol. Psychiatry 102, 109951 (2020).
Sharan, P. & Vellapandian, C. Hypothalamic-pituitary-adrenal (HPA) axis: unveiling the potential mechanisms involved in stress-induced Alzheimer’s disease and depression. Cureus 16, e67595 (2024).
Zhang, R. et al. The prevalence and risk of developing major depression among individuals with subthreshold depression in the general population. Psychol. Med. 53, 3611–3620 (2023).
Michaud, T. L., Su, D., Siahpush, M. & Murman, D. L. The risk of incident mild cognitive impairment and progression to dementia considering mild cognitive impairment subtypes. Dement. Geriatr. Cogn. Dis. Extra 7, 15–29 (2017).
Koivukangas, J. et al. Physical activity and fitness in adolescents at risk for psychosis within the Northern Finland 1986 Birth Cohort. Schizophr. Res. 116, 152–158 (2010).
Pinto Pereira, S. M., Geoffroy, M. C. & Power, C. Depressive symptoms and physical activity during 3 decades in adult life: bidirectional associations in a prospective cohort study. JAMA Psychiatry 71, 1373–1380 (2014).
Stavrakakis, N., De Jonge, P., Ormel, J. & Oldehinkel, A. J. Bidirectional prospective associations between physical activity and depressive symptoms. The TRAILS study. J. Adolesc. Health 50, 503–508 (2012).
Farholm, A. & Sørensen, M. Motivation for physical activity and exercise in severe mental illness: a systematic review of intervention studies. Int. J. Ment. Health Nurs. 25, 194–205 (2016).
Choi, K. W. et al. Assessment of bidirectional relationships between physical activity and depression among adults: a 2-sample Mendelian randomization study. JAMA Psychiatry 76, 399–408 (2019).
Noetel, M. et al. Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. BMJ 384, e075847 (2024).
Williams, C. J. et al. Genes to predict VO2max trainability: a systematic review. BMC Genomics https://doi.org/10.1186/S12864-017-4192-6 (2017).
Bouchard, C. et al. Genomic predictors of the maximal O2 uptake response to standardized exercise training programs. J. Appl. Physiol. 110, 1160–1170 (2011).
Yang, X. et al. Genotype-phenotype models predicting V̇O2max response to high-intensity interval training in physically inactive Chinese. Med. Sci. Sports Exerc. 55, 1905–1912 (2023).
Klevjer, M., Nordeidet, A. N. & Bye, A. The genetic basis of exercise and cardiorespiratory fitness – relation to cardiovascular disease. Curr. Opin. Physiol. 33, 100649 (2023).
Hanscombe, K. B. et al. The genetic case for cardiorespiratory fitness as a clinical vital sign and the routine prescription of physical activity in healthcare. Genome Med 13, 180 (2021).
Brown, W. M. & Exercise-associated, D. N. A. methylation change in skeletal muscle and the importance of imprinted genes: a bioinformatics meta-analysis. Br. J. Sports Med. 49, 1568–1578 (2015).
Raghuveer, G. et al. Cardiorespiratory fitness in youth: an important marker of health: a scientific statement from the American Heart Association. Circulation. 142, E101–E118 (2020).
Ashdown-Franks, G. et al. Exercise as medicine for mental and substance use disorders: a meta-review of the benefits for neuropsychiatric and cognitive outcomes. Sports Med 50, 151–170 (2020).
White, R. L. et al. Physical activity and mental health: a systematic review and best-evidence synthesis of mediation and moderation studies. Int. J. Behav. Nutr. Phys. Act. 21, 134 (2024).
Nguyen Ho, P. T. et al. Mechanisms linking physical activity with psychiatric symptoms across the lifespan: a systematic review. Sports Med 53, 2171–2190 (2023).
Sterne, J. A. et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 343, d4002 (2011).
Higgins, J. P. T. et al. Cochrane Handbook for Systematic Reviews of Interventions (John Wiley & Sons, 2019).
Tripp, T. R., Kontro, H., Gillen, J. B. & MacInnis, M. J. Fit for comparison: controlling for cardiorespiratory fitness in exercise physiology studies of sex as a biological variable. J. Physiol. 603, 2219–2230 (2025).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
Stroup, D. F. et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA 283, 2008–2012 (2000).
Rethlefsen, M. L. et al. PRISMA-S: an extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst. Rev. 10, 39 (2021).
Diagnostic and Statistical Manual of Mental Disorders 5th edn, Revision DSM-5-TR (American Psychiatric Publishing, 2022).
Ouzzani, M., Hammady, H., Fedorowicz, Z. & Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst. Rev. 5, 210 (2016).
Quality Assessment Tool for Observational Cohort and Cross-sectional Studies (National Heart Lung and Blood Institute, 2021); https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
Guyatt, G. H., Oxman, A. D., Schünemann, H. J., Tugwell, P. & Knottnerus, A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 64, 380–382 (2011).
Davies, H. T. O., Crombie, I. K. & Tavakoli, M. When can odds ratios mislead? BMJ 316, 989–991 (1998).
Greenland, S. Interpretation and choice of effect measures in epidemiologic analyses. Am. J. Epidemiol. 125, 761–768 (1987).
Valentine, J. C., Pigott, T. D. & Rothstein, H. R. How many studies do you need?: a primer on statistical power for meta-analysis. J. Educ. Behav. Stat. 35, 215–247 (2010).
Sidik, K. & Jonkman, J. N. Simple heterogeneity variance estimation for meta-analysis. J. R. Stat. Soc. Ser. C 54, 367–384 (2005).
Balduzzi, S., Rücker, G. & Schwarzer, G. How to perform a meta-analysis with R: a practical tutorial. BMJ Ment. Health 22, 153–160 (2019).
Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 36, 1–48 (2010).
Díaz-Goñi, V. & Bizzozero-Peroni, B. Dataset for: Cardiorespiratory fitness and risk of mental disorders and dementia—a systematic review and meta-analysis. Open Science Framework https://doi.org/10.17605/OSF.IO/BJSGN (2025).
Acknowledgements
V.D.-G. received funding from the National Agency for Research and Innovation of Uruguay (POS_EXT_2023_1_175630). E.R.-G. received funding from the University of Castilla-La Mancha (2022-UNIVERS-11373). F.B.O. research activity is supported by the grant PID2023-148404OB-I00 funded by MICIU/AEI/10.13039/501100011033 and ERDF funds, EU, and additionally by a mobility grant for senior researchers to undertake research stays abroad, funded by the Spanish Ministry of Science, Innovation and Universities. B.B.-P. received funding from the Swedish Research Council for Health, Working Life and Welfare (project no. 2023-01125) and from the University of Castilla-La Mancha, co-financed by the European Social Fund (2024-UNIVERS-12849). The conclusions and interpretations provided, based on the scientific data reviewed, are those of the authors and not of the public funding agencies of the study. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Funding
Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
V.D.-G. and B.B.-P. conceived and designed the study. V.D.-G., V.M.-V. and B.B.-P. performed the screening and study selection. V.D.-G., V.M.-V. and B.B.-P. conducted the quality and certainty of evidence assessments. E.R.-G., M.E.V.-A., E.J.-L. and I.S.-D. contributed to data collection. V.D.-G., V.M.-V. and B.B.-P. performed the statistical analysis. J.F.L.-G., E.R.-G., M.E.V.-A., E.J.-L., I.S.-D., F.B.O., J.C.-P., A.E.M. and M.S.-L. contributed to data interpretation. V.D.-G., J.F.L.-G. and B.B.-P. drafted the paper, with input from E.R.-G., M.E.V.-A., E.J.-L., I.S.-D., F.B.O., J.C.-P., A.E.M., M.S.-L., V.M.-V. and B.B.-P. supervised the work. All authors have read and approved the final version of the paper.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Mental Health thanks Riccardo De Giorgi, David Stacey and Jesse Stewart for their contribution to the peer review of this work. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary Information (download PDF )
Supplementary methods, Tables 1–10 and Figs. 1–4.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Díaz-Goñi, V., López-Gil, J.F., Rodríguez-Gutiérrez, E. et al. Cardiorespiratory fitness and risk of mental disorders and dementia: a systematic review and meta-analysis. Nat. Mental Health (2026). https://doi.org/10.1038/s44220-026-00599-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44220-026-00599-4
