
Abstract
The Dominantly Inherited Alzheimer Network Observational Study (DIAN Obs) is a longitudinal, global cohort study investigating brain aging and autosomal dominant Alzheimer’s disease (ADAD), a rare monogenic form of Alzheimer’s disease (AD). Established in 2008 with support from the National Institute on Aging (NIA), DIAN Obs is designed to collect comprehensive and uniform data with the aim to characterize brain biology and clinical trajectory of individuals at risk for ADAD. Mutations in the amyloid protein precursor (APP), presenilin 1 (PSEN1), or presenilin 2 (PSEN2) genes cause ADAD with virtually full penetrance and a predictable age at symptomatic onset. Participants, both mutation carriers and non-carriers from affected families, undergo longitudinal clinical and cognitive assessments, neurologic and physical examinations, structural and functional neuro-imaging, and amyloid and tau positron emission tomography (PET). Biospecimens include cerebrospinal fluid, plasma, serum, and whole blood for biochemical, genetic and multi-omic analyses, with brain donation upon death. This dataset enables one of the most detailed longitudinal examinations of the human brain across the continuum from presymptomatic to symptomatic AD. The extensive DIAN Obs data and biospecimen repository provides a globally accessible resource to advance understanding of AD pathophysiology, aging, and the development of preventive and therapeutic interventions.
Similar content being viewed by others

Introduction
The vast majority of AD dementia is sporadic and generally occurs in older ages, but a small proportion (less than 1%) of AD dementia is caused by mutations in the Aβ precursor protein (APP), presenilin 1 (PSEN1), or presenilin 2 (PSEN2) genes with almost 100% penetrance, generally at predictable younger ages. This form of AD is known as autosomal dominant AD (ADAD). ADAD is thought to have an underlying pathogenic process similar to that of the more common sporadic AD and thus may hold the key to understanding the pathogenesis of AD and identification of effective treatments for both ADAD and sporadic AD. To leverage this population's potential for AD research, the DIAN Obs was established in 2008. It aims to track individuals from families with known ADAD mutations, employing a wide array of cognitive assessments and biomarker tests. Since its inception time, the DIAN Obs has amassed a substantial repository of clinical and biomarker data and samples, facilitating a deeper understanding of ADAD's natural history.
The DIAN Obs cohort has been longitudinally followed for over 15 years and is amongst the most deeply phenotyped cohorts of brain aging, function, and AD measures in predominantly 18 to 55-year-old people. The inaugural year of DIAN Obs included ten performance sites in three countries (US, UK, and Australia) with English as the language for all initial sites. The continued success of DIAN Obs has since grown to twenty-three performance sites in eleven countries and supporting seven languages: English, Spanish, German, Japanese, Korean, French, and Portuguese (Fig. 1 and Supplementary Table 1). A total of 664 participants have enrolled in DIAN Obs; currently the study has 314 active participants. Through these participant provided resources, DIAN Obs has fulfilled more than 300 data and tissue requests globally to investigators with hypotheses and aims outside of DIAN Obs (Fig. 1).

DIAN Obs, or DIAN Observational Study and DIAN-TU, or the DIAN Trials Unit, global site locations are represented by the red icons. DIAN EXR, or DIAN Expanded Registry, exploratory areas for potential new sites for DIAN Obs and DIAN-TU are represented by the yellow icons. For the Value bar, data and tissue requests fulfilled is represented by the shading of each country; United States = 216 (darkest shade) and countries in gray reflect zero requests.
DIAN Obs is the key scientific and discovery study for ADAD and also provides natural history information for the DIAN-Trials Unit (DIAN-TU), which is the therapeutic and target validation platform for treatment and prevention trials. The DIAN-TU [dian.wustl.edu/our-research/clinical-trial/]1 is a global research effort established in 2012 to design and conduct clinical trials for the prevention or treatment of ADAD1. Data from DIAN Obs and DIAN-TU studies were designed to be conducted together, with nearly identical protocols, including cognitive and clinical assessments, biomarker measures, and quality control.
Participant outreach, recruitment, and retention for both DIAN Obs and DIAN-TU are facilitated via the international DIAN Expanded Registry (DIAN EXR) [dian.wustl.edu/our-research/registry], established in 2012 for individuals who are or may be affected by ADAD. DIAN EXR serves as a collaborative research effort not only to facilitate study referral to DIAN Obs and DIAN-TU, but also to support educational and outreach activities with ADAD family members.
DIAN Obs and DIAN-TU have distinct purposes with differing eligibility requirements and site locations allowing the DIAN EXR to act as a central mechanism for navigation and referral of interested registrants to potential research opportunities (Fig. 2).

DIAN Obs, or DIAN Observational Study, provides natural history data collection for scientific studies with currently 673 total enrolled participants. DIAN-TU, or DIAN Trials Unit, serves as the therapeutic sector for prevention and treatment clinical trials with 385 total enrolled participants. DIAN EXR, or DIAN Expanded Registry, provides support for education and outreach for participants and family members with 643 registered individuals. These three distinct groups within the network collaborate and support one another with the goal to advance Alzheimer’s disease research and treatment options to the medical community. PET positron emission tomography, MRI magnetic resonance imaging, CSF cerebrospinal fluid.
The main scientific hypotheses of DIAN Obs aim to address fundamental questions regarding the pathophysiology of AD. First, longitudinal changes in AD biomarkers will distinguish mutation carriers (MC) many years before the onset of clinical symptoms, supporting the concept of a measurable preclinical phase of AD. Second, the initial biomarker changes in the preclinical stage of ADAD will involve Aβ42, followed sequentially by biomarkers of neurodegeneration and, ultimately, by detectable cognitive decline. Third, the clinical, biomarker, and neuropathological phenotypes of ADAD will parallel those observed in “sporadic” late onset AD (LOAD). DIAN Obs emphasizes longitudinal data as it provides more accurate and precise information on the magnitude and rate of change for biofluid and imaging biomarkers throughout the preclinical stage of ADAD.
In ADAD, the age of symptomatic onset is tightly linked to the specific mutation and family history, allowing researchers to derive an estimated years of onset (EYO) for individual carriers. This permits the use of EYO as a temporal anchor: negative values reflect years remaining before expected symptom onset, zero corresponds to predicted conversion, and positive values indicate years since onset2. By aligning participants along this EYO axis, it becomes possible to map biomarker and cognitive trajectories relative to the expected onset point even before clinical symptoms appear.
Additionally, in the DIAN Obs cohort, individuals who do not carry the familial Alzheimer’s mutation provide a rare and valuable control group access early to middle adulthood. Because these non-carriers (NC) are enrolled alongside mutation carriers using identical protocols and longitudinal follow-ups, they offer exceptionally well-matched healthy baselines. This design allows the data and tissue resources generated from the DIAN Obs protocol to contribute not only to understanding ADAD, but also the potential to broader studies of normative aging trajectories and biomarker baselines in younger adults.
DIAN Obs has provided seminal advances in the understanding of brain health, the onset and progression of ADAD, and how this compares to the more common sporadic AD (Fig. 3). In 2012, DIAN Obs described a comprehensive order of clinical, cognitive, imaging, and biomarker changes that occur across a time span two decades before and a decade after symptom onset. Amyloid plaques continuously accumulate for 15–20 years before symptom onset, defining an amyloid growth phase2,3,4,5, while tau tangles appear and accumulate in the transition to and during the symptomatic phase6. A series of biochemical changes in CSF and blood begin with amyloid-beta 42/40 decreasing, followed closely by p-tau217/181/231 associated with amyloid plaques, then p-tau205, neurofilament light chain (NfL), and total tau increasing before the appearance of tangles. Cortical hypometabolism begins up to 18 years prior to symptom onset, and cortical atrophy up to 13 years prior to symptom onset3,4,7,8. Finally, changes in cognitive performance are detected several years before onset.

The evolution of amyloid and tau pathophysiology is observed through distinct phases in CSF and plasma providing comparison from the DIAN cohort to onset and progression of sporadic Alzheimer’s disease (AD). Measures of different amyloid (Aβ 42/40) and tau (p-T217, p-T181, p-T205) species and aggregate tau demonstrate over 35 years sequential change by stage of disease related to plaque formation, cortical atrophy and metabolism. A Amyloid plaques intiated (brown line). B p-T217 (purple line), p-T181 (dark blue line) and NfL (orange line) levels begin to increase. C With the decrease of cortical metabolism, p-T205 (green line) and soluble t-tau (light blue line) begin to increase and tau PET tangles (red line) begin to develop while p-T217 and p-T181 decrease. CSF cerebrospinal fluid, Aβ amyloid beta, p- phosphorylated, NfL neurofilament light chain, t- total.
DIAN-TU implements therapeutic trials in a trial platform with the goal to slow, delay, or prevent dementia in the ADAD population1,9. DIAN Obs and DIAN-TU implement harmonization efforts to ensure the combination and comparability of DIAN-TU and DIAN Obs protocols, including International Council for Harmonization Good Clinical Practice (ICH GCP) guideline compliance. These harmonization efforts increase longitudinal data and sample resources that can be combined across DIAN Obs and DIAN-TU. The Biostatistics Core enables the ability to link coded participant data across the DIAN Obs and DIAN-TU, enabling combining and comparing across the studies. Key measures harmonized include electronic capture of clinical and cognitive assessments, sample collection protocols, and imaging (MRI and PET).
Results
Study description
With over 15 years of follow-up, the DIAN has enrolled more than 600 participants from families carrying mutations in APP, PSEN1, or PSEN2, including both mutation carriers and non-carriers. Longitudinal assessments across clinical, cognitive, imaging, and fluid biomarker domains revealed a consistent temporal sequence of Alzheimer’s disease (AD) pathophysiological changes. Amyloid accumulation on PET and reductions in CSF Aβ42 were observed up to two decades before estimated symptom onset, followed by increases in CSF total-tau and phosphorylated-tau, cortical thinning, and metabolic decline on PET approximately 10–15 years prior to expected onset. Cognitive decline, as measured by global and domain-specific composites, emerged roughly 5–10 years before symptomatic conversion, paralleling clinical diagnostic progression from asymptomatic to prodromal and dementia stages. Collectively, these findings provide a comprehensive 15-year longitudinal framework describing the natural history of dominantly inherited AD and establish the foundation for prevention and interventional trials targeting the earliest stages of disease.
Discussion
Washington University in St. Louis is the recipient of a U19 grant from the NIA and serves as the DIAN Obs Coordinating Center, which oversees both the scientific and administrative center and serves as a performance site. The DIAN Obs Coordinating Center consists of eight Cores: Administration, Clinical, Genetics, Cognition, Imaging, Biomarker, Neuropathology, and Biostatistics and three scientific Projects: Amyloid-β, Tau, and Novel Mechanisms. All performance sites have access to adequate numbers of potential DIAN Obs participants and the resources and capabilities to conduct all elements of the DIAN Obs protocol.
The human data outlined in this manuscript are stored in the DIAN Repository managed by the Division of Biomedical Statistics and Informatics at Washington University in St. Louis. Data freezes are completed annually, synchronizing the study’s efforts to collect, process, and review data for distribution. The amount of data in this natural history study does not currently have a cap as it is collected upon study start and longitudinally every other year for asymptomatic participants and annually for symptomatic participants, with no data collection gap and no study end planned. Each data freeze produces a blinded cumulative snapshot of all available vetted data across all study modalities and consists of the following stages: (1) data cut-off, (2) processing cut-off, (3) quality control of raw and derived data, (4) outlier quality control, and (5) dataset preparation and blinding (see Fig. 4). With the NIH Data Management and Sharing Policy implemented in January 2023, the study’s next grant cycle will transition the human data to the Becker Medical Library’s Digital Commons Data Repository and Research Infrastructure.

eCOA electronic Clinical Outcome Assessment, EDC electronic data capture, DCA DIAN Central Archive, MRI magnetic resonance imaging, PET positron emission tomography, BM Biomarker, Gen Genetics, QC quality control.
The study’s primary human data is highly sensitive and will be protected. Access will require a data request, followed by review and approval before access is granted. Investigators who wish to submit a data request may review the types of data that are available and complete a data request form on the DIAN website (https://dian.wustl.edu/). Each request is received by the study data sharing committee, which will review and upon approval, a Data Use Agreement (DUA) is required to be in place prior to data release. Data file types and formats include: .tiff, .lif, .fastq, .tsv, .mzML, .mtx, .csv, .rsd., and .dcm. Raw data files will be analyzed to generate .csv or .tsv files for statistical analysis.
Methods
This observational, natural history study is managed through the DIAN Obs Coordinating Center based at Washington University in St. Louis and is conducted at sites globally with all sites requiring a current Institutional Review Board (IRB)/Independent Ethics Committee (IEC) approval to conduct study visits in accordance with the DIAN Obs protocol. Participants review and discuss the consent form with the performance site study team prior to being asked to sign the informed consent for study participation. A copy of the consent is provided to participants, and the original is maintained in the participant’s research record. For this multi-center study, the local IRB/IEC committees are: Advarra (single IRB for U.S based sites and Coordinating Center)/IRB reference #: Pro00065069, Comité de Bioética de la Facultad de Medicina, Comite de Etica en Ivestigacion en Investigacion en Salud de UCASAL, Comite de Etica en Ivestigacion INNN MSC, Eberhard Karls Universitat/ Univerity Hosptials Tubingen, Ethikkomission bei der Ludwig-Maximillians Unversitat Munchen, FLENI Comite de etica en Investigaciones biomedicas, McGill Institutional Review Board, NHS Health Research Authority; Berkshire REC Centre, Niigata University, Ramsay Health Care WA SA HREC, Seoul Asan Medical Center IRB, South Eastern Sydney Local Health District HREC, and The University of Tokyo Research Ethics Committee.
Administration core
The DIAN Obs Administration Core provides oversight and management of the DIAN Obs project, including: coordinating activities of the other Cores, scientific research Projects, and subcontractors; managing and supporting the DIAN Obs Steering Committee; seeking and facilitating feedback from the External Advisory Committee; interacting with the NIA liaisons; and managing activation, maintenance, and data collection of all performance sites.
The Administration Core has established a web-based system to support data and tissue resource dissemination to investigators. The DIAN Obs data and biospecimen application form is available on the DIAN website (dian.wustl.edu). All requests are reviewed by relevant Core Leaders, the Study Director, and DIAN Obs Steering Committee. Upon receiving request approval, with appropriate institutional review board (IRB)/institutional ethics committee (IEC) approvals and data and tissue sharing agreements, data and/or biospecimens are shared with support from the related Cores and Biostatistics Core. The DIAN Obs Data and Tissue Sharing, Notifications, Publications, and Authorship Policies govern the sharing of DIAN Obs resources and guidelines for publications10. As of December 2022, DIAN Obs has received 288 data requests and 114 tissue requests, with 231 and 85 requests fulfilled, respectively. An overview of resources that may be requested is provided in Fig. 5.

A summary of DIAN Obs, or DIAN Observational Study, data types available to researchers. PET positron emission tomography, MRI magentic resonance imaging, CSF cerebrospinal fluid, AD Alzheimer’s disease, iPSC induced pluripotent stem cells, WGS whole genome sequencing, GWAS genome-wide association study.
Clinical core
The Clinical Core oversees clinical protocol execution and associated activities, encompassing participant recruitment, retention, clinical evaluations, CSF and blood sample acquisition, safety protocols, and quality control initiatives. Enrollment eligibility criteria include being 18 years of age or older and having a known pathogenic ADAD mutation in the family with a risk of inheriting the mutation. All DIAN Obs participants have access to genetic counseling and testing.
Upon participant consent, a visit anniversary date is established, initiating the DIAN Obs visit schedule with a frequency of one to three years. In-person site visits commence with the initial assessment and subsequently alternate with remote assessments for asymptomatic participants. Symptomatic participants undergo annual in-person evaluations under the current protocol. Table 1 details clinical and cognitive data collection procedures and data availability. A comprehensive list of current and former DIAN Obs performance sites is included as Supplementary Table 1.
Genetics core
The goals of the Genetics Core are to obtain and bank tissue for genetic and multi-omic studies, as well as to generate, process, and/or harmonize genetic and multi-omic data. At each DIAN Obs in-person initial visit, whole blood is collected and used for ADAD mutation status, APOE genotype, genome-wide association study (GWAS) genotyping array, and whole genome sequencing (WGS). At each DIAN Obs in-person initial and follow-up visit, buffy coat blood and PAXgene blood tubes are collected for longitudinal assessment of DNA methylomics and RNA transcriptomics, respectively. Additionally, the Core obtains and banks dermal fibroblasts and then generates induced pluripotent stem cells (iPSCs) (Table 2). These resources support DIAN Obs Projects and are available to the research community with an approved data and/or tissue request.
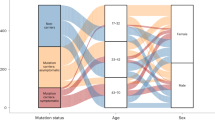
The Genetics Core provides central determination and confirmation of gene sequence, whether normal or disease-causing mutation carrier, and APOE genotype on each of the 673 total study participants derived from 251 families. Table 3 presents the distribution of genetic variants and carrier status, categorized by gene. The Core, in coordination with the Clinical Core and DIAN EXR, maintains and curates a list of pathogenic mutations as well as confirms that new DIAN families carry an ADAD mutation.
The Genetics Core generates GWAS genotyping arrays, WGS, and APOE genotype data for all individuals. This data has been leveraged to generate polygenic risk scores (PRSs) for LOAD risk, onset, and progression, as well as Parkinson’s disease risk. Recent studies indicate that in DIAN Obs ADAD, LOAD risk PRS is not significantly associated with mutations status, but is associated with levels of CSF Aβ, total-tau, and p-tau, suggesting that known AD risk variants may modify age at onset (AAO) in the ADAD population. Polygenic risk score of sporadic late-onset Alzheimer's disease reveals a shared architecture with the familial and early-onset forms11.
Finally, the Genetics Core serves as a central repository for increasingly rich multi-omic data12,13. Currently, this catalog includes: DNA methylomics (Illumina MethylationEPIC 850k array) for brain (44 participants) and buffy coat blood (790 longitudinal samples from 266 participants); RNA-seq for brain (44 participants) and blood (575 longitudinal samples from 319 participants); and proteomics (SomaLogic 7k) and metabolomics/lipidomics (Metabolon HD4) for brain (44 participants), CSF (495 participants), and plasma (495 participants). These data have been used to identify circular RNAs in brain associated with AD and AD pathology14,15, as well as to identify proteins associated with carrying an ADAD mutation and change between 20 to -30 years before the onset, some of them even before some of the validated biomarkers.
Cognition core
A primary goal of the Core is to maintain the cognitive assessment battery to align with scientific aims and to incorporate novel measures and novel assessment methodologies that are more sensitive to early cognitive changes in ADAD. The Cognition Core serves the overall grant by overseeing rater training and maintaining rigorous quality control (QC) and documentation standards that ensure the fidelity of longitudinal cognitive assessments. In addition, the Cognition Core plays a pivotal role in maintaining the consistency of cognitive assessments across various languages, ensuring culturally relevant translations and adaptations across different sites and countries. These methodologies will improve the reliability in the measurement of the key features of ADAD. The assessment of cognition is central for achieving the scientific aims of all DIAN Obs Projects and Cores. The Cognition Core works with the Project and Core leaders to ensure that fully validated cognitive data is available for DIAN Obs data freezes and provides guidance on appropriate cognitive measures and data analyses to support Project and Core aims. Refer to Table 4 for Core data availability. Novel methods implemented in the Cognition Core include the use of remote cognitive testing via Ambulatory Research in Cognition (ARC), and the development of novel remote cognitive tasks, including tests of long-term forgetting and statistical learning paradigms.
Imaging core
The Imaging Core is responsible for the acquisition, QC, processing, and analysis of the MRI and PET neuroimaging data for DIAN Obs. The imaging data set collected in DIAN Obs participants to date represents a highly valuable resource for AD research. It has supported cross-sectional analysis of PET and MRI data to develop a timeline for imaging biomarkers in ADAD. Carriers of AD-causing mutations and their non-carrier (NC) siblings are enrolled and followed in the Clinical Core through the international DIAN Obs performance sites. Participants undergo structural and functional MRI, amyloid PET, tau PET, and metabolic PET imaging in conjunction with their clinical visits. The Core obtains and analyzes longitudinal imaging data that is fully integrated with clinical, psychometric, and CSF biomarkers, and allows for mutation-specific genotype-phenotype analysis. MRI data are processed using the Freesurfer Imaging suite to derive regions of interest. These regions are then used to process the PET data. Imaging Core data formats available are outlined in Table 5. A neuroimaging-specific resource paper detailing in-depth imaging protocols has recently been published5,16.
For tau PET, sites obtain scans with two tracers [18F]-MK-6240 or [18F]-AV-1451 (aka Flortaucipir [FTP], T807). Because there is no single tracer with the international distribution to reach all DIAN sites, each site has the ability to include one or both of the two tau PET tracers. While the use of multiple tracers maximizes the number of sites that can perform tau PET imaging, it is recognized that the limitations of using multiple tracers in the same study. The Imaging Core has performed preliminary analyses directly comparing head-to-head FTP and MK-6240 data collected from ADAD participants. Prior work has demonstrated that the tau PET signal only goes up with the onset of impairment3,17. The regional correlations seen between tracers are low in non-carriers and asymptomatic mutation carriers, and in individuals who are symptomatic, the correlations between tracers are very high, particularly in areas known to have high deposition. Images released through data requests will be defaced using the Mayo Imaging Pipeline (see Fig. 4).
Biomarker core
The DIAN Obs Biomarker Core is a high-capacity biorepository enabling high-throughput processing while maintaining high-quality, gold-standard biomarker measurements of cerebrospinal fluid (CSF) and plasma samples available to investigators upon completion and approval through the DIAN tissue request process. The Biomarker Core obtains measures of the following biomarker analytes using the Lumipulse automated assay platform: CSF (Aβ1-40, Aβ1-42, total tau [t-tau], p-tau 181). Data and sample availability is outlined in Table 6. Core samples may be leveraged in a longitudinal manner, in conjunction with extensive clinical and biological data, to study both traditional and exploratory biomarkers. With the main priority of the Biomarker Core to evaluate fluid biomarker profiles in ADAD participants comparing MCs to NC, DIAN Obs, along with others, have helped give insight to expected biomarker trajectories given the availability of expected AAO in MC individuals3,11. The Biomarker Core has demonstrated that fluid biomarkers changes begin during the preclinical period (20-30 years before expected symptom onset). However, collection and analysis of additional longitudinal samples are required to define the patterns of change of known and novel fluid biomarkers that happen right when an individual progresses from asymptomatic (or preclinical) to symptomatic. Given the minimally invasive nature of phlebotomy, the field is invested in the identification of plasma biomarkers. In response to the needs in the field, DIAN Obs’ scientific Projects will measure and analyze established markers of amyloid (Aβ and %p-tau217 ratio) and tau (MTBR243) deposition, inflammation (GFAP, sTREM2), and neurodegeneration (NfL) in CSF and plasma.
Neuropathology core
The Neuropathology Core houses the network’s post-mortem tissue. DIAN sites are supported in providing intact fixed hemi-brain specimens for uniform neuropathologic examination. Neuropathology Core efforts include maintaining unfixed frozen and formalin-fixed tissue; a resource supporting DIAN’s Projects and available to the research community with an approved tissue request.
Fixed hemibrains are prepared in standard fashion (hemispheres coronally; cerebelli parasagittally; brainstems axially), digitally photographed, and sampled for histology, generating a set of 17 formalin-fixed, paraffin-embedded (FFPE) tissue blocks, representing the following areas: Middle frontal gyrus; anterior cingulate gyrus at the level of the genu of the corpus callosum; precentral gyrus; superior and middle temporal gyri; inferior parietal lobe (angular gyrus); occipital lobe (including the calcarine sulcus and peristriate cortex); posterior cingulate gyrus and precuneus at the level of the splenium; amygdala and entorhinal cortex; hippocampus and parahippocampal gyrus at the level of the lateral geniculate nucleus; striatum (caudate nucleus and putamen with nucleus accumbens) and olfactory cortex; lentiform nuclei (globus pallidus and putamen) at the level of the anterior commissure with the nucleus basalis of Meynert; thalamus with subthalamic nucleus; midbrain; pons; medulla oblongata; cerebellum with dentate nucleus; and cervical spinal cord. Remaining wet formalin-fixed tissue is kept in formalin in perpetuity as a research resource.
The Core prepares histology slides from a uniform set of seventeen FFPE blocks from each case. These are stained with hematoxylin and eosin for histomorphologic assessment, and with immunohistochemistry (IHC) for the more common neurodegenerative lesions, using antibodies for Aβ (10D5, Eli Lilly), phosphorylated tau (PHF1, Feinstein Institute for Medical Research, Manhasset, NY), α-synuclein (LB509, MilliporeSigma), and phosphorylated TAR DNA-binding protein of 43 kDa (pTDP-43, Cosmo Bio USA). This protocol enables the Neuropathology Core to identify and rigorously stage the pathological underpinnings of the major classes of neurodegenerative diseases. Histological slides are then reviewed and scored, using published semi-quantitative scoring criteria for histopathological lesions. These data inform the formulation of diagnoses for each case (using consensus staging and neuropathological criteria for AD [Khachaturian, CERAD, NIA-Reagan Institute, and NIA-AA]18,19,20,21,22,23,24 and for non-AD disorders25,26,27,28,29,30,31,32,33). To date, a total of 41 DIAN participant specimens have been secured. Core data and sample availability are outlined in Table 7.
Biostatistics core
The activities of the Biostatistics Core enhance the research objectives of DIAN by imparting a smooth transition from the database to statistical analyses, providing appropriate statistical analysis resources to all Cores and Projects, and developing longitudinal statistical models to test the preclinical hypotheses of DIAN on all major biomarkers of AD. The Core provides application of methodological significance as it is a necessity of state-of-the-art longitudinal statistical models to adequately estimate and compare the longitudinal rates of change on multi-modal biomarkers during the preclinical and symptomatic stages, and to assess their predictive power to cognitive decline.
The high dimensional data from Imaging Core from many modalities (MRI, PiB PET, Tau PET over a large number of brain regions) and the omics data from the Genetics and Multi-Omics Core present another unique analytic challenge to DIAN Obs. The Biostatistics Core seeks biologically meaningful dimension reduction, and conduct analyses to combine imaging markers and omics markers into composites for the test of critical hypotheses. Principal component analyses and partial least square analyses34,35 will be implemented, as well as methodologies developed by the Core36,37. The Biostatistics Core also analyzes longitudinal rates of change for these biomarkers jointly through general linear mixed models and correlate the rates of changes across modalities.
The Biostatistics Core have recently published multiple novel statistical methods driven by DIAN Obs database: analysis of biomarkers subject to detection limits38, correlations with family-clustered design39, diagnostic accuracy with ROC surface40, detection of unknown changepoints (in age) from multiple longitudinal biomarkers41, and a novel Bayesian ADAD progression model42. The Core continues to expand these models, and tackle other emerging analytic challenges from DIAN Obs: measurement errors in the EYO, small sample inferences on MCs who ‘escaped’ from their expected AAO, and high dimensional longitudinal data from imaging and omics. To control the false discovery rate (FDR), the Benjamini and Hochberg procedure is utilized43.
Scientific projects
In 2019, DIAN Obs added three scientific Projects to the study: Project 1: Amyloid-beta, Project 2: Tau, and Project 3: Novel Mechanisms. The goal of these scientific projects is to uniquely address central scientific questions that require significant DIAN Obs Core involvement.
Project 1 aimed to define the impact of ADAD mutations and amyloidosis on amyloid β proteoforms in CSF and plasma. This was accomplished using an IP-mass spectrometry approach to capture major Aβ proteoforms in plasma, CSF, and brain. Specifically, this Project monitored Aβ37, 38, 39, 40, 42, and 43 in CSF, plasma, and brain homogenates and observed that Aβ isoform patterns of change differ. Additionally, Project 1 aimed to describe the impact of ADAD mutations in human iPSC-derived neurons and the relationship of brain proteoforms with histologic amyloid structure.
The next phase of this project will combine cell-based characterizations of individual ADAD variants with mass-spectrometry, IHC, and ELISA-based measures of Aβ burden in brain parenchyma, cerebrovasculature, CSF, and blood from ADAD pathogenic variant carriers participating in DIAN Obs and DIAN-TU. This will provide a path toward the understanding of molecular composition and variant-level diversity of deposited and soluble Aβ species, and compare these to the biochemical properties of each variant. These studies will offer a unique bench-to-bedside investigation of which types of Aβ are likely to be pathogenic, which are likely to deposit in brain and vessel walls, and how anti-amyloid therapies alter the balance of soluble Aβ species in the CNS and peripheral circulation.
The goal of Project 2 is to quantify the amount and regional distribution of tau pathology utilizing PET to illustrate differences between mutation carriers and non-carriers, investigate connections between tau pathology and other biomarkers, as well as cognitive decline. The Project also aims to validate the specificity and sensitivity of tau PET tracers (MK6240, AV1451, & PI2620) in postmortem tissue. Project 2 works to measure using mass spectrometry tau proteoforms in CSF, brain tissue, and iPSC-derived neurons, relating them to mutation status, EYO, AD biomarkers, and cognitive measures.
Initial work done within the Project used samples collected through 2017. During the study’s current grant cycle, analyses have expanded to CSF on samples collected since 2017. This expanded analysis included 411 total samples, which captured 67 individuals with longitudinal visits. From these samples, the Project derived measures of p-tau phosphorylated at different sites. Also, these samples were used to generate MTBR-tau243 data.
Project 3 aims to map molecular interactions, providing a greater explanation of how ADAD mutations, inflammation, synaptic function, and associated therapeutic targets may influence one another. The molecular profiling is completed by transcriptomics and mass spectrometry-based proteomics. Project 3 also explores defining profiles of targeted and novel fluid markers of neuroinflammation and injury to evaluate biomarker levels pre-clinically to progression to predict cognitive decline. Targeted inflammation markers in CSF include YKL-40, sTREM2, and progranulin (via immunoassay), and neuronal injury markers include CSF VILIP-1, neurogranin, SNAP-25, and NfL and plasma NfL.
Future initiatives
DIAN Obs has led major scientific advances in the understanding of AD stages, CSF and plasma biomarkers, mechanistic links to therapeutic targets, and enabled ground-breaking prevention and interventional trials2,9,44. DIAN Obs has helped define the sequence, timing, and magnitude of longitudinal AD biomarker changes decades before symptoms begin2,4,5,16. This work directly led to the development and implementation of primary and secondary prevention trials for ADAD and the validation of the amyloid-tau-neurodegeneration (ATN) criteria45. DIAN Obs intends to build on these advances to further understand major contributors to disease progression, resilience, and heterogeneity, and target validation for future therapeutics.
As DIAN prepares for its next phase, study hypotheses will expand and move to be supported by home-based remote assessments, smartphone-based applications, and wearable technologies. Home health nurse visits are being incorporated into the DIAN protocol, allowing for clinical and cognitive assessments and biospecimen samples to be collected at visits occurring in years between a participant’s in-person visit. Additionally, the Cognition Core will extend the use the ARC smartphone application to include novel measures of long-term forgetting rates, which have been shown to be highly sensitive in preclinical ADAD14,46. Another novel task is a measure of statistical learning that assesses and evaluates learning rates over several consecutive days. Pilot data show that this is extremely sensitive to AD biomarkers in a sporadic AD population and is well tolerated by participants. Finally, DIAN will increase the generation and leverage of omic technologies to not only answer the main questions of the study but also generate new hypotheses and discover new biomarkers.
DIAN will continue its outreach to new families and regions of the world. The success demonstrated with DIAN’s South American performance sites has laid the groundwork to explore additional sites in Chile and Puerto Rico. There is a need to expand diversity in populations minimally represented in the DIAN cohort, with discussions initiated with potential collaborators in South Africa, Morocco, and Nigeria. There is also interest in re-establishing performance sites in the Western United States serving families previously identified in the region by former DIAN sites.
DIAN will maintain its lead role in defining the profiles of targeted and novel fluid markers of neuroinflammation and neuronal and synaptic injury over the course of the disease and evaluate the ability of biomarker levels at baseline and longitudinal change over time to predict cognitive decline. The landscape of biomarkers is expected to change rapidly due to amyloid removal treatment approaches. During the next years, DIAN plans to explore different omic layers to better characterize ADAD, but also to identify novel biomarkers.
The DIAN has provided seminal discoveries in AD pathophysiology and helped define the current understanding of the sequence of events that begin two decades before the first symptom onset, and progress through a decade of dementia. These advances are made on one of the world’s largest, deeply phenotyped cohorts of both normal brain aging and AD progression. The data and sample sets are available through a comprehensive study approach (Fig. 6) to address questions and hypotheses on human brain function, aging, and AD, and with further utilization, promises to have even larger impacts.

A DIAN Obs, or DIAN Observational Study, progressive approach from establishing global regions through providing data to prevention and treatment trials. B Study aims and data types collected to understand Alzheimer’s disease’s mechanistic links to therapeutic targets. C DIAN Obs is multi-interdisciplinary with eight Cores and varying scientific projects. ADAD autosomal dominant Alzheimer’s disease, AD Alzheimer’s disease, WGS whole genome sequencing, CSF cerebrospinal fluid, Admin Administration, Aβ amyloid beta.
Data availability
The datasets generated during the current study are not publicly available due to the sensitive nature of this human subjects data set, but are available from the corresponding author on reasonable request. All requests for data must be submitted in writing via the electronic data request form available on the DIAN website (https://dian.wustl.edu/our-research/for-investigators/dian-observational-study-investigator-resources/](https:/dian.wustl.edu/our-research/for-investigators/dian-observational-study-investigator-resources). Currently human data generated in this research is quality controlled and preserved with the DIAN Obs Biostatistics Core and in process to transition to the Washington University Becker Medical Library’s Digital Commons Data Repository and the Research Infrastructure Service (RIS). This repository meets the desirable characteristics of an acceptable NIH repository under the NIH Data Management and Sharing Policy implemented on January 25, 2023. The Core and Project primary data is highly sensitive and will be protected. Access will require a data request, followed by review and approval before access is granted. Those who wish to submit a data request will be able to see the types of data that are available, but a formal online request will be required to protect our subjects and for tracking purposes. The request form will include investigator affiliation, contact information, funding support, institutional review board (IRB) approval (if applicable), an NIH-style biosketch, and a brief description of the project, including specific aims, study design, characteristics of the data requested, and analysis plans. Investigators requesting data will also be required to sign a data user agreement and an acknowledgement agreement. The request will be received by the study data sharing committee, which will review for appropriateness. Upon their approval to release the data, a DUA will be required to be in place before the requested data is released. Each request is tracked by the DIAN Administration Core, and a data sharing report will be generated for progress and final reports to the National Institute on Aging (NIA). Each data request will specify the data elements required for the planned analyses. The Biostatistics Core personnel will prepare a file containing only these data elements, together with a participant identification number (not the DIAN ID# but an identifier recoded to protect confidentiality), so that questions about particular individuals can be resolved without the investigator’s knowledge of the participant’s identity. Image data will be available to approved investigators in post-processed formats via the DIAN Central Neuroimaging Data Archive (CNDA) after a formal DUA has been signed by both institutions. For data generated in this study, the following software may be useful for manipulating and utilizing the shared data: SAS, R, STATA, Python and MATLAB.
Code availability
No custom code was used to generate the data described in this manuscript. Precautions to ensure confidentiality are taken by DIAN and recipients of DIAN Obs data. The final dataset is stripped of DIAN Obs identifiers and re-coded with dummy IDs prior to release and transferred only with encryption and password protection by the Biostatistics Core. For all analyses, data is provided in a blinded way with the outcome variables and then unblinded after the results of the analysis are returned to the DIAN Biostatistics Core. This ensures blinding, avoids bias and multiple comparisons (p-hacking). The Biostatistics Core enables the ability to link coded participant data across the DIAN Obs and DIAN-TU, enabling combining and comparing across the studies.
References
Mills S. M., et al. Preclinical trials in autosomal dominant AD: Implementation of the DIAN-TU trial. Rev. Neurol.169. https://doi.org/10.1016/j.neurol.2013.07.017.
Bateman, R. J. et al. Clinical and biomarker changes in dominantly inherited Alzheimer’s disease. N. Engl. J. Med. 367, 795–804 (2012).
Benzinger, T. L. S. et al. Regional variability of imaging biomarkers in autosomal dominant Alzheimer’s disease. Proc. Natl. Acad. Sci. 110, E4502–E4509 (2013).
Gordon, B. A. et al. Spatial patterns of neuroimaging biomarker change in individuals from families with autosomal dominant Alzheimer disease: a longitudinal study. Lancet Neurol. 17, 241–250 (2018).
McDade, E. et al. Longitudinal cognitive and biomarker changes in dominantly inherited Alzheimer disease. Neurology 91, e1295–e1306 (2018).
Gordon, B. A. et al. Tau PET in autosomal dominant Alzheimer’s disease: relationship with cognition, dementia and other biomarkers. Brain J. Neurol. 142, 1063–1076 (2019).
Quiroz, Y. T. et al. Cortical atrophy in presymptomatic Alzheimer's disease presenilin 1 mutation carriers. J. Neurol. Neurosurg. Psychiatry 84, 556–561 (2013).
Ridha, B. H. et al. Tracking atrophy progression in familial Alzheimer's disease: a serial MRI study. Lancet Neurol. 5, 828–834 (2006).
Bateman, R. J. et al. The DIAN-TU Next Generation Alzheimer’s prevention trial: Adaptive design and disease progression model. Alzheimer's Dement J. Alzheimer's Assoc. 13, 8–19 (2017).
Washington University in St. Louis. Publication Policy. Dominantly Inherited Alzheimer Network (DIAN). https://dian.wustl.edu/for-investigators/dian-observational-study-investigator-resources/publication-policy/ (2025).
Cruchaga, C. et al. Polygenic risk score of sporadic late-onset Alzheimer’s disease reveals a shared architecture with the familial and early-onset forms. Alzheimers Dement 14, 205–214 (2018).
Timsina, J. et al. Comparative Analysis of Alzheimer’s Disease Cerebrospinal Fluid Biomarkers Measurement by Multiplex SOMAscan Platform and Immunoassay-Based Approach. J. Alzheimers Dis. JAD 89, 193–207 (2022).
Sung, Y. J. et al. Proteomics of brain, CSF, and plasma identifies molecular signatures for distinguishing sporadic and genetic Alzheimer’s disease. Sci. Transl. Med. 15, eabq5923 (2023).
Kurylo, D. D., Corkin, S. & Iii, J. F. R. Greater relative impairment of object recognition than of visuospatial abilities in Alzheimer’s disease. Neuropsychology 10, 74–81 (1996).
Llibre-Guerra J. J. et al. Association of longitudinal changes in cerebrospinal fluid total Tau and Phosphorylated Tau 181 and Brain Atrophy With Disease Progression in Patients With Alzheimer's disease. JAMA Netw. Open. 2, e1917126 (2019).
McKay, N. S. et al. Positron emission tomography and magnetic resonance imaging methods and datasets within the Dominantly Inherited Alzheimer Network. DIAN. Nat. Neurosci 26, 1449–1460 (2023).
O’Connor, A. et al. Tau acculuation in autosomal dominant Alzheimer’s disease: a longitudinal [18F]flortaucipir study. Alzheimer's Res Ther. 15, 1–11 (2023).
Braak, H. & Braak, E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol. 82, 239–259 (1991).
Braak, H., Alafuzoff, I., Arzberger, T., Kretzschmar, H. & Tredici, K. D. Staging of Alzheimer disease-associated neurofibrillary pathology using paraffin sections and immunocytochemistry. Acta Neuropathol. 112, 389–404 (2006).
Thal, D. R., Rub, U., Orantes, M. & Braak, H. Phases of amyloid-beta deposition in the human brain and its relevance for the development of AD. Neurology 58, 1791 (2002).
Khachaturian, Z. S. Diagnosis of Alzheimer's disease. Arch. Neurol. 42, 1097–1105 (1985).
Mirra, S. S. et al. The Consortium to Establish a Registry for Alzheimer's Disease (CERAD). Part II. Standardization of the neuropathologic assessment of Alzheimer's disease. Neurology 41, 479–486 (1991).
National Institute on Aging and Reagan Institute Working Group Consensus recommendations for the postmortem diagnosis of Alzheimer's disease. Neurobiol. Aging 18, S1–S2.5.4 (1997).
Montine, T. J. et al. National Institute on Aging-Alzheimer's Association guidelines for the neuropathologic assessment of Alzheimer's disease: a practical approach. Acta Neuropathol. 123, 1–11 (2012).
McKeith, I. G. et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 47, 1113–1124 (1996).
McKeith, I. et al. Consortium on DLB Diagnosis and management of dementia with Lewy bodies: Third report of the DLB consortium. Neurology 65, 1863–1872 (2005).
McKeith, I. G. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB International Workshop. J. Alzheimers Dis. 9, 417–423 (2006).
Braak, H., Tredici, K. D., Rub, U. & de Vos, R. A. I. Steur ENHJ, Braak E. Staging of brain pathology related to sporadic Parkinson's disease. Neurobiol. Aging 24, 197–211 (2003).
Attems, J. et al. Neuropathological consensus criteria for the evaluation of Lewy pathology in post-mortem brains: a multi-centre study. Acta Neuropathol. 141, 159–172, https://doi.org/10.1007/s00401-020-02255-2 (2021).
Cairns, N. J. et al. Neuropathologic diagnostic and nosologic criteria for frontotemporal lobar degeneration: consensus of the Consortium for Frontotemporal Lobar Degeneration. Acta Neuropathol. 114, 5–22 (2007).
Mackenzie, I. R. et al. Nomenclature and nosology for neuropathologic subtypes of frontotemporal lobar degeneration: an update. Acta Neuropathol. 119, 1–4 (2010).
Josephs, K. A. et al. Updated TDP-43 in Alzheimer's disease staging scheme. Acta Neuropathol. 131, 571–585, https://doi.org/10.1007/s00401-016-1537-1 (2016).
Nelson, P. T. et al. LATE-NC staging in routine neuropathologic diagnosis: an update. Acta Neuropathol. 145, 159–173, https://doi.org/10.1007/s00401-022-02524-2 (2023).
Gregoria Mateos-Aparicio Partial Least Squares (PLS) Methods: Origins, Evolution, and Application to Social Sciences. Commun. Stat. - Theory Methods 40, 2305–2317 (2011).
Krishnan, A., Williams, L. J., McIntosh, A. R. & Abdi, H. Partial Least Squares (PLS) methods for neuroimaging: a tutorial and review. Neuroimage 56, 455–7537 (2011).
Xiong, C., McKeel, D. W., Miller, J. P. & Morris, J. C. Combining correlated diagnostic tests-application to neuropathologic diagnosis of Alzheimer's disease. Med. Decis. Mak. 24, 659–669 (2004).
Xiong, C. et al. Combining Multiple Markers to Optimize the Longitudinal Rate of Progression-Application to Clinical Trials on the Early Stage of Alzheimer’s Disease. Statistics in Biopharmaceutical. Research 5, 54–66 (2013).
Xiong, C., Luo, J., Agboola, F., Grant, E. & Morris, J. C. A family of estimators to diagnostic accuracy when candidate tests are subject to detection limits-Application to diagnosing early stage Alzheimer disease. Stat. Methods Med Res. 31, 882–898, https://doi.org/10.1177/09622802211072511 (2022).
Luo, J. et al. Statistical estimation and comparison of group-specific bivariate correlation coefficients in family-type cluster studies. J. Appl. Stat. 49, 2246–2270 (2021).
Xiong, C. et al. Estimating diagnostic accuracy for clustered ordinal diagnostic groups in the three-class case-application to the early diagnosis of Alzheimer's disease. Stat. Methods Med. Res. 27, 701–714 (2018).
Luo, J. et al. Dominantly Inherited Alzheimer Network (DIAN OBS). Accelerated longitudinal changes and ordering of Alzheimer disease biomarkers across the adult lifespan. Brain 145, 4459–4473 (2022).
Wang G. et al. Dominantly Inherited Alzheimer Network Trials Unit. A novel cognitive disease progression model for clinical trials in autosomal-dominant Alzheimer's disease. Stat. Med. https://doi.org/10.1002/sim.7811.
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. Royal Stat. Soc. Ser. 57, 289–300 (1995).
Johnson, E. C. B. et al. Cerebrospinal fluid proteomics define the natural history of autosomal dominant Alzheimer’s disease. Nat. Med. 29, 1979–1988 (2023).
Jack, C. R. et al. Revised criteria for diagnosis and staging of Alzheimer's disease: Alzheimer's Association Workgroup. Alzheimer's. Dement. 20, 5143–5169 (2024).
Suzuki A. et al. Establishing a new screening system for mild cognitive impairment and Alzheimer’s disease with mental rotation tasks that evaluate visuospatial function. J. Alzheimer’s Dis. 61, 1653–1665. (2018).
Acknowledgements
Data collection and sharing for this project was supported by The Dominantly Inherited Alzheimer Network (DIAN, U19AG032438) funded by the National Institute on Aging (NIA), the Alzheimer’s Association (SG-20-690363-DIAN), the German Center for Neurodegenerative Diseases (DZNE), Raul Carrea Institute for Neurological Research (FLENI), Partial support by the Research and Development Grants for Dementia from Japan Agency for Medical Research and Development (AMED) (JP23dk0207066), the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), Korea Dementia Research Center (KDRC), funded by the Ministry of Health & Welfare and Ministry of Science and ICT, Republic of Korea (HI21C0066), and Spanish Institute of Health Carlos III (ISCIII). This manuscript has been reviewed by DIAN Study investigators for scientific content and consistency of data interpretation with previous DIAN Study publications. We acknowledge the altruism of the participants and their families, and the contributions of the DIAN research and support staff at each of the participating sites for their contributions to this study.
Author information
Authors and Affiliations
Consortia
Contributions
AJD): writing, reviewing and editing, data curation, figure generation; (EM): methodology, clinical data processing, reviewing and editing, funding acquisition, data harmonization; (JJLG): funding acquisition, methodology reviewing and writing, figure generation; (CX): data QC and processer, manuscript reviewing and editing, data sharing pipeline management; (RJP): Brain sample curation and accessing, funding acquisition, manuscript reviewing and editing; (LI): fluid biomarker sample and data curation and accessing, methodology, writing, reviewing and editing; (CSB): manuscript reviewing and writing, methodology, funding acquisition; (CC): methodology, reviewing and editing, genomic data and resource curation; (AG): methodology, reviewing and editing; (AER): genomic data curation, processing and QC, reviewing and editing; (TLSB): imaging data curation, processing and QC, funding acquisition, manuscript reviewing and editing; (BAG): imaging data curation, processing and QC, manuscript reviewing and editing; (JH): cognition data curation, processing and QC, manuscript reviewing and editing; (CK): data curation, processing and QC, funding acquisition, manuscript reviewing and editing; (AL): data curation, processing and QC, manuscript reviewing and editing; (JCM): manuscript reviewing and editing, study conception; (VB): manuscript reviewing and editing, study conception; (RFA): funding acquisition, manuscript reviewing and editing, data acquisition; (PC): manuscript reviewing and editing, data acquisition; (SBB): manuscript reviewing and editing, data acquisition; (JPC): manuscript reviewing and editing, data acquisition; (MRF): manuscript reviewing and editing, data acquisition; (NCF): manuscript reviewing and editing, data acquisition; (GSD): manuscript reviewing and editing, data acquisition; (TI): funding acquisition, manuscript reviewing and editing, data acquisition; (MJ): funding acquisition, manuscript reviewing and editing, data acquisition; (JHL): funding acquisition, manuscript reviewing and editing, data acquisition; (JL): funding acquisition, manuscript reviewing and editing, data acquisition; (DA): data acquisition; (LT): manuscript reviewing and editing, data acquisition; (ALS): manuscript reviewing and editing, data acquisition; (RM): manuscript reviewing and editing, data acquisition; (HM): funding acquisition, manuscript reviewing and editing, data acquisition; (JMN): manuscript reviewing and editing, data acquisition; (SS): manuscript reviewing and editing, data acquisition; (EH): manuscript reviewing and editing, data acquisition; (RSV): funding acquisition, manuscript reviewing and editing; (PRS): manuscript reviewing and editing, data acquisition; (JHR): funding acquisition, manuscript reviewing and editing, data acquisition; (RJB): funding acquisition, study design; manuscript writing, reviewing and editing, data acquisition; and the Dominantly Inherited Alzheimer Network (DIAN): funding acquisition, data acquisition and curation, analysis, interpretation, methodology.
Corresponding authors
Ethics declarations
Competing interests
RJB, Professor of Neurology at Washington University’s School of Medicine (WUSM) receives lab research funding from the National Institutes of Health, Alzheimer’s Association, BrightFocus Foundation, Rainwater Foundation, Association for Frontotemporal Degeneration FTD Biomarkers Initiative, Tau Consortium, Novartis, Centene Corporation, Association for Frontotemporal Degeneration, the Cure Alzheimer’s Fund, Coins for Alzheimer’s Research Trust Fund, The Foundation for Barnes-Jewish Hospital, Good Ventures Foundation, DIAN-TU Pharma Consortium, Centene Corporation, Tau SILK Consortium (AbbVie, Biogen, Eli Lilly and Company and an anonymous organization), the NfL Consortium (AbbVie, Biogen, Bristol Meyers Squibb, Hoffman La Roche, and an anonymous organization). RJB has received honoraria as a speaker/consultant/advisory board member from Eisai, F. Hoffman-LaRoche, Janssen, Biogen; and reimbursement of travel expenses from Korean Dementia Association, American Neurological Association, Fondazione Prada, Weill Cornell Medical College, Harvard University, CTAD, FBRI, Beeson Foundation, Adler, Alzheimer’s Association Roundtable, Duke Margolis Roundtable, Bright Focus Foundation, Tau Consortium Investigator’s, NAPA Advisory Council on Alzheimer’s Research. RJB serves as principal investigator of the DIAN-TU, which is supported by the Alzheimer’s Association, GHR Foundation, an anonymous organization and the DIAN-TU Pharma Consortium (Active: Biogen, Eisai, Eli Lilly and Company/Avid Radiopharmaceuticals, F. Hoffman-La Roche/Genentech, and Janssen. Previous: Abbvie, Amgen, AstraZeneca, Forum, Mithridion, Novartis, Pfizer, Sanofi, and United Neuroscience). The DIAN-TU-001 Clinical Trial is supported by Pharmaceutical Partners Eli Lilly and Company, F. Hoffman-La Roche and Janssen, the Alzheimer’s Association, NIH U01AG042791, NIH U01AG42791-S1 (FNIH and Accelerating Medicines Partnership), NIH R01AG046179, NIH R56AG053267, NIH R01AG053267, NIH U01AG059798, NIH R01AG068319, Avid Radiopharmaceuticals, GHR Foundation, and an anonymous organization. In-kind support has been received from CogState, Cerveau, Signant Health and Eisai Corporation. RJB is a co-founder of C2N Diagnostics and receives income from C2N Diagnostics for serving on the scientific advisory board. Washington University (WU) has equity ownership interest in C2N Diagnostics. C2N Diagnostics will be analyzing samples from the Knight Family DIAN-TU-001 trial of E2814 for primary, secondary, and exploratory endpoints. Should the DIAN-TU trials impact the value of C2N Diagnostics, WU and RJB could directly benefit. TLSB has received funding from the National Institutes of Health and Siemens; has a licensing agreement from Sora Neuroscience but receives no financial compensation; has received honoraria for lectures, presentations, speakers bureaus, or educational events from Biogen and Eisai Genetech; has served on a scientific advisory board for Biogen; holds a leadership role in other board, society, committee, or advocacy groups for the American Society for Neuroradiology (unpaid) and Quantitative Imaging Biomarkers Alliance (unpaid); and has participated in radiopharmaceuticals and technology transfers with Avid Radiopharmaceuticals, Cerveau, and LMI. JPC serves as the chair of the American Neurological Association Dementia and Aging Special Interest Group and is on the medical advisory board of Humana Healthcare. CC receives research support from: Biogen, EISAI, Alector and Parabon. The funders of the study had no role in the collection, analysis, or interpretation of data; in the writing of the report; or in the decision to submit the paper for publication. Dr. Cruchaga is a member of the advisory board of Vivid genetics, Halia Therapeutics Adx Healthcare and ADMit. JH is a paid consultant for F. Hoffmann-La Roche, Ltd., Takeda, and Lundbeck, and is on the Data Safety and Monitoring Board for Eisai. JJLG is supported by NIH-NIA (K01AG073526), the Alzheimer’s Association (AARFD-21-851415, SG-20-690363), the Michael J. Fox Foundation (MJFF-020770), the Foundation for Barnes-Jewish Hospital and the McDonnell Academy. EMD received support from the National Institute on Aging, an anonymous organization, the GHR Foundation, the DIAN-TU Pharma Consortium, Eli Lilly, and F Hoffmann La-Roche; has received speaking fees from Eisai and Eli Lilly; and is on the data safety and monitoring board and advisory boards of Eli Lilly, Alector, and Alzamend. JCM is the Friedman Distinguished Professor of Neurology, Director, Knight ADRC; Associate Director of DIAN and Founding Principal Investigator of DIAN. He is funded by NIH grants # P30 AG066444; P01AG003991; P01AG026276; U19 AG032438; and U19 AG024904. RJP receives research funding from the National Institutes of Health and the National Institute on Aging. AER has received funding from National Institute on Aging, National Institute of Neurological Disorders and Stroke, Alzheimer’s Association, JPB Foundation, and Donors Cure. AG serves on the scientific review board for Genentech and the scientific advisory board Muna Therapeutics. PRS receives funding from the National Health and Medical Research Council (Australia) grants 1176716 and 2022057 and the Medical Research Future Fund (Australia) grants 1200428 and 1200428. He is a director (unpaid) of the Australian Dementia Network Ltd. NCF reports consulting fees from Biogen, Eisai, Ionis, Lilly, Roche/Genentech, and Siemens – paid to UCL; he has served on a Data Safety Monitoring Board for Biogen; he acknowledges grant support from the Alzheimer’s Society, Alzheimer’s Research UK, Rosetrees Trust, the Sigrid Rausing Trust, the UK Dementia Research Institute and the UK NIHR UCLH Biomedical Research Centre. All other authors have no competing interests to disclose. CK is an associate editor of npj Dementia.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Daniels, A.J., McDade, E., Llibre-Guerra, J.J. et al. 15 years of longitudinal genetic, clinical, cognitive, imaging, and biochemical measures in DIAN. npj Dement. 2, 13 (2026). https://doi.org/10.1038/s44400-025-00047-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44400-025-00047-7
