
Abstract
Osteoporosis, primarily characterized by low bone mineral density (LBMD), is a major skeletal disorder among postmenopausal women (PMW), yet its global burden remains poorly quantified. Leveraging data from the Global Burden of Disease (GBD) Study 2021, we assessed the LBMD burden in PMW across 204 countries and territories between 1990 and 2021. Metrics included deaths, disability-adjusted life years (DALYs), years of life lost (YLLs), and years lived with disability (YLDs), with temporal trends evaluated via estimated annual percentage change (EAPC). We found that in 2021, LBMD was responsible for 219,552 deaths and 7.76 million DALYs in PMW globally, with age-standardized DALY rates reaching 979.2 per 100,000 population. Compared to premenopausal women, PMW experienced a 15.17-fold higher mortality, a 5.84-fold higher burden in DALYs, and a 6.29-fold higher burden in YLDs. While age-standardized rates (ASR) for deaths and DALYs showed slight declines from 1990 to 2021, the absolute number of LBMD-related deaths more than doubled, increasing from 91,941 in 1990 to 219,552 in 2021, largely driven by global population aging. South Asia experienced the greatest burden, with India reporting the highest DALYs rates. The burden was highest in women aged ≥80 years and increased most rapidly in those aged ≥95. Regions with a high Socio-demographic Index (SDI) exhibited lower mortality rates but disproportionately higher levels of disability, whereas low-SDI regions bore a greater burden of mortality. Projections to 2045 suggest a sustained rise in deaths and disability, despite modest rate reductions. These findings underscore the urgent need for age-tailored, equity-focused interventions to mitigate fracture risk and improve musculoskeletal health among aging female populations worldwide.
Similar content being viewed by others

Introduction
LBMD, encompassing both osteopenia and osteoporosis, is a common aging-related condition characterized by reduced bone mass and microarchitectural deterioration, leading to increased skeletal fragility and fracture risk1,2. Recognized as a major global public health issue, LBMD currently affects approximately 200 million women worldwide, including more than 10 million in the United States3. Meanwhile, due to its strong association with fragility fractures, LBMD not only affects a large population but also imposes a heavy and growing economic burden. In the United States alone, the annual cost of osteoporotic fractures exceeds $20 billion, while the European Union faces a comparable burden of approximately €30 billion4,5. As global population aging accelerates, individuals with LBMD are increasingly affected by high treatment costs, fracture-related disability, psychological distress, and long-term care needs6,7. Understanding the evolving burden of LBMD is therefore essential for guiding targeted public health interventions, informing resource allocation, and narrowing health disparities in aging populations worldwide.
PMW, characterized by estrogen deficiency as a defining biological feature, are widely recognized as a high-risk population for osteoporotic fractures8,9,10. Estrogen deficiency following menopause induces a cascade of physiological alterations—accelerated bone turnover, trabecular thinning, and increased cortical porosity—all of which have been extensively elucidated in mechanistic studies11,12,13,14. Furthermore, molecular and clinical investigations have firmly linked menopause-associated hormonal changes with dysregulation in bone remodeling pathways, including the RANK/RANKL/OPG axis, Wnt/β-catenin signaling, and increased oxidative stress, leading to compromised bone quality and microarchitectural deterioration15,16,17,18. Nevertheless, a major evidence gap persists: while mechanistic and interventional research has been robust, there remains a lack of comprehensive, population-level epidemiological data that accurately reflect the burden and distribution of LBMD in PMW across regions and time.
This study investigates the trends in LBMD disease burden across 204 countries and territories, considering variations in SDI levels and geographical factors. It utilizes a range of key indicators—such as death, DALYs, YLLs, and YLDs—to assess the overall impact of LBMD. The study also examines health inequalities in both absolute and relative terms, with a focus on how disease burden correlates with economic development. This is done through the application of the Inequality Slope Index and Concentration Index. Additionally, the Bayesian age-period-cohort (BAPC) model is used to forecast potential public health challenges related to LBMD by 2045 (Fig. 1). The insights from this research offer critical epidemiological data that can guide healthcare policymakers, clinicians, and epidemiologists in refining health strategies and optimizing resource allocation. These findings are essential for shaping effective, region-specific policies aimed at alleviating the global burden of LBMD.

A: Schematic representation of the study population, focusing on LBMD in PMW. B: Global distribution of LBMD burden in PMW across 204 countries/territories in 2021, showing variations in the burden by region. C: Comparison of LBMD disease burden proportions between premenopausal women and PMW in terms of deaths, DALYs, YLLs,and YLDs. D: The relationship between economic burden and LBMD in PMW across different global regions. E: Projected future trends in LBMD-related disease burden in PMW, highlighting changes from 1990 to 2045 across different age groups.
Results
Global disparities in the burden of LBMD among PMW
According to United Nations data, PMW accounted for 20% of the total female population in 2021, up from 13.75% in 1990. According to the GBD 2021, the burden of LBMD among PMW accounted for more than 20% of the total LBMD burden among the female population. Specifically, PMW were responsible for 93.81% of LBMD-related deaths, 85.39% of DALYs, 86.28% of YLDs, and 84.19% of YLLs among all age groups of women, as shown in Fig. 2A. These findings indicate that PMW bear a disproportionately high burden of LBMD and are significantly more susceptible to the disease compared to women of other age groups.

A In 2021, the number of deaths, DALYs, YLDs and YLLs for PMW as a percentage of the total female population. B-E: The global age-standardized deaths, DALYs, YLDs and YLLs rates for LBMD in PMW across 204 countries/territories in 2021. Panels (B), (C), (D–E) represent the age-standardized deaths, DALYs, YLDs and YLLs rates in 2021, respectively. F: The age-standardized death rates, DALYs, YLDs, and YLLs of LBMD among PMW in 2021 across 21 GBD regions.
From 1990 to 2021, the global burden of LBMD among PMW demonstrated a diverging trend between absolute numbers and ASR. The global age-standardized death rate decreased slightly from 29.34 per 100,000 population in 1990 to 27.51 in 2021, with an EAPC of -0.05, while the total number of deaths more than doubled from 91,941 to 219,552 cases. A similar pattern was observed in DALYs, where the ASR declined from 1,074.43 to 979.20 per 100,000 population (EAPC = –0.30), despite the absolute number of DALYs rising markedly from 4 million to 8 million cases over the same period. This downward shift in DALY rates was driven by reductions in both non-fatal and fatal components: the ASR of YLDs rate declined from 623.50 to 567.51 (EAPC = –0.36), while the ASR of YLLs rate decreased from 450.92 to 411.69 per 100,000 population (EAPC = –0.21). (Fig. 2B–E, Fig. 3A–D, Tables 1, 2).

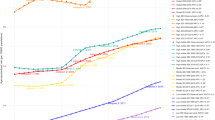
A–D The EAPC of age-standardized deaths (A), DALYs (B), YLDs (C) and YLLs (D) rates of LBMD among PMW from 1990 to 2021, globally. E The EAPC of age-standardized deaths, DALYs, YLDs and YLLs rates of LBMD among PMW from 1990 to 2021, in 21 GBD regions.
Regional variations in LBMD burden in PMW
In 2021, marked geographical heterogeneity was observed in the ASR of LBMD-related burden among PWM across the 21 GBD regions. South Asia exhibited the highest age-standardized death rate at 70.18 per 100,000 population, followed by Eastern Sub-Saharan Africa (54.10) and Central Sub-Saharan Africa (49.29). For DALYs, South Asia also ranked first with an ASR of 1833.32 per 100,000 population, significantly higher than that of Australasia (1268.62) and High-income North America (1194.14). While South Asia had the highest YLLs ASR (1079.51), followed by Eastern (792.56) and Central Sub-Saharan Africa (769.52), the burden of YLDs was more pronounced in high-income regions. Specifically, Australasia (985.02), High-income North America (875.36), and Western Europe (833.65) reported the highest YLD rates, indicating a greater proportion of non-fatal disability in these settings (Fig. 2F).
Temporal trends from 1990 to 2021, as measured by the EAPC, further revealed stark contrasts. High-income North America and Australasia were the only two regions where all four indicators—deaths, DALYs, YLDs, and YLLs—exhibited an upward trend. In contrast, Central Europe, Central Latin America, and High-income Asia Pacific experienced the most pronounced declines across all four metrics. Notably, the increase in DALYs in Western Sub-Saharan Africa, Oceania, Andean Latin America, Caribbean, and Central Sub-Saharan Africa was primarily driven by rising YLDs, suggesting that disability associated with LBMD is becoming an increasingly dominant contributor to disease burden in these regions. These regional variations underscore the interplay between healthcare capacity, aging demographics, and diagnostic availability in shaping LBMD outcomes across the globe (Fig. 3E, Tables 1, 2).
Cross-national differences in LBMD-related mortality and YLDs among PMW
In 2021, Palau (86.06 per 100,000) recorded the highest age-standardized death rate, whereas Azerbaijan (3.24 per 100,000) reported the lowest. India (2100.67 per 100,000) exhibited the highest age-standardized DALY rate, reflecting its large population size and substantial disease burden. For DALYs, the highest ASR were noted in India (2100.67), Andorra (1938.73), and Greenland (1894.41). The top countries for YLDs were Andorra (1647.13), Belgium (1316.99), and Greenland (1288.32), whereas the YLL burden was highest in India (1242.10), the United Arab Emirates (1161.93), and Palau (1053.44) (Fig. 2B–E).
In terms of temporal trends, the most pronounced increases in death rates were observed in the United Arab Emirates (EAPC = 4.18), Georgia (EAPC = 2.53), and the United States of America (EAPC = 2.03). For DALYs, the highest upward trends occurred in the Netherlands (EAPC = 1.73), United Arab Emirates (EAPC = 1.71), and Georgia (EAPC = 1.34). The most significant increases in YLDs were seen in Bhutan (EAPC = 1.83), Netherlands (EAPC = 1.83), and Cambodia (EAPC = 1.27), while YLLs rose most steeply in the United Arab Emirates (EAPC = 2.88), Georgia (EAPC = 2.00), and Lesotho (EAPC = 1.81). In contrast, Hungary experienced the largest decreases in both age-standardized death rate (EAPC = –5.47) and DALYs (EAPC = –3.53) during the study period (Fig. 3A–D, Tables S1–2).
Age-specific disparities in LBMD burden among PMW
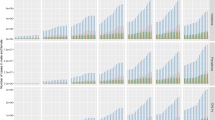
In 2021, the ASR of all LBMD-related burden indicators, including deaths, DALYs, YLDs, and YLLs, demonstrated a marked increase with advancing age. In terms of the absolute number of cases, LBMD-related deaths were predominantly concentrated among individuals aged 80–94 years, with a peak observed in the 80–84 age group. For DALYs, YLLs, and YLDs, the burden was mainly distributed among those aged 65–89 years, also reaching a maximum in the 80–84 age group. Although the absolute number of cases declined slightly in females aged 95 years and older, the ASRs for all indicators remained substantially elevated in this age group, particularly for deaths and DALYs.
Temporal trends from 1990 to 2021 further revealed that the percentage increase in ASR was most prominent in the 95+ age group across all four measures, suggesting worsening control of LBMD outcomes in the oldest-old population. By contrast, the 55–64 age groups showed the most significant reductions in ASR, especially for deaths and YLLs, implying improved early detection and management among younger PMW. Middle-old age groups (65–84) displayed relatively stable or mildly fluctuating burden rates (Fig. 4E–H).

A–D Number of cases (bars, left axis) and rate (lines, right axis) of LBMD-related deaths (A), DALYs (B), YLDs (C), and YLLs (D) across age groups of PMW in 2021. The x-axis represents age groups in 5-year intervals from 55–59 to 95+ years. E–H Percentage change in rates of deaths (E), DALYs (F), YLDs (G), and YLLs (H) from 1990 to 2021 across age groups, showing the differential trends in disease burden over time. The x-axis represents age groups in 5-year intervals from 55–59 to 95+ years.
SDI-associated patterns in the global burden of LBMD
Between 1990 and 2021, distinct disparities were observed in the burden of LBMD among PMW across SDI quintiles. Age-standardized trends in deaths, DALYs, YLLs, and YLDs demonstrated a consistent gradient pattern, with higher SDI regions generally showing declining trends, while lower SDI regions experienced increases. Specifically, the EAPC for death rate was highest in low-SDI (EAPC = 0.28) and low-middle-SDI (EAPC = 0.29) regions, in contrast to decreasing trends in high-, high-middle-, and middle-SDI settings. A similar pattern was observed for DALYs and YLLs, where high-SDI regions showed declining rates, while low- and low-middle-SDI regions exhibited mild to moderate increases (Fig. 5A–D).

A–D EAPC of deaths (A), DALYs (B), YLDs (C), and YLLs (D) due to LBMD among PMW across five SDI regions (high, high-middle, middle, low-middle, and low SDI) between 1990 and 2021. E–H Temporal trends in ASR for deaths (E), DALYs (F), YLDs (G), and YLLs (H) from 1990 to 2021, stratified by SDI region. Each line represents a specific SDI category, demonstrating how the LBMD burden has evolved over time in different socioeconomic contexts.
In terms of absolute disease burden, low-SDI regions maintained the highest ASR for deaths, DALYs, and YLLs throughout the three-decade observation period. Notably, a peak was recorded between 2013 and 2015, with the highest values reached in 2014: deaths (73.43 per 100,000), DALYs (1482.71 per 100,000), and YLLs (1054.70 per 100,000). This sustained elevation contrasts sharply with the substantially lower ASR observed in high- and high-middle-SDI regions (Fig. 5E–H).
For YLDs, however, a different pattern emerged. Although high- and high-middle-SDI regions experienced decreasing trends in YLDs—especially in high-middle-SDI regions (EAPC = –0.76)—they consistently exhibited higher YLD ASR compared to lower-SDI regions. Throughout the study period, YLDs in high-SDI regions remained above 750 per 100,000 population, more than 1.5 times greater than those in low-SDI settings. This suggests that in higher-SDI regions, while mortality and years of life lost have declined, the non-fatal disability burden associated with LBMD remains substantial.
SDI-Based Inequalities in LBMD Burden Among PMW
Between 1990 and 2021, substantial income-based inequalities in LBMD burden among PMW were identified, both in absolute and relative terms. Absolute inequality, as indicated by the Slope Index of Inequality (SII) derived from weighted regression against SDI rank, showed diverging patterns across burden types (Fig. S1A–D). LBMD-related deaths and YLLs were predominantly concentrated in low-SDI countries. From 1990 to 2021, the SII for deaths was –8 (1990) and –6 (2021), while the SII for YLLs remained consistently large, decreasing slightly from –267 to –230. Conversely, DALYs and YLDs showed an increasing concentration in higher-SDI regions. The SII for DALYs declined from 330 in 1990 to 276 in 2021, and for YLDs remained stable, with values above 500 across both years (537 in 2021), indicating persistent absolute disparities favoring higher-SDI countries.
Relative inequality, as measured by the concentration index, reinforced these findings (Fig. S1E–H). The concentration index for deaths shifted from –0.09 (95% CI: –0.14 to –0.06) in 1990 to –0.11 (95% CI: –0.16 to –0.06) in 2021, and for YLLs from –0.17 (95% CI: –0.22 to –0.12) to –0.19 (95% CI: –0.24 to –0.13), highlighting an increasing concentration of mortality and premature death in lower-SDI settings. In contrast, DALYs remained nearly evenly distributed across the SDI spectrum, with a slight rightward shift in concentration index from 0.03 (1990) to 0.01 (2021). YLDs consistently favored higher-SDI regions, with the concentration index declining only marginally from 0.17 (95% CI: 0.14 to 0.20) to 0.15 (95% CI: 0.12 to 0.19), indicating persistent relative disparities in disability burden (Fig. S1).
Future burden of LBMD
According to projections from the BAPC model, the global burden of LBMD among PMW is expected to continue rising in absolute terms from 2021 to 2045, despite a mild decline in ASR, reflecting a divergence between population aging and disease rate control. Specifically, the number of LBMD-related deaths is projected to surpass 386,000 by 2045, even as the death ASR declines from 28 to 19 per 100,000 population. Similarly, YLDs are expected to exceed 9 million cases globally, with the ASR decreasing to 548 per 100,000 population. DALYs and YLLs will follow the same pattern—continued increases in case numbers accompanied by slight reductions in ASR—suggesting a growing absolute burden due to demographic expansion and life expectancy gains (Fig. S2).
Age-stratified projections further underscore the intensifying burden among the oldest-old. PMW aged ≥85 years will remain the primary contributors to LBMD burden across all metrics, with particularly sharp increases expected in the 95+ age group. By 2045, the YLD ASR in women aged 95 and older is projected to reach 3,336.83 per 100,000 population—twice that of the 90-94 group. For deaths, the ASR among women aged 95+ is projected to be 1.6 times higher than that of those aged 90–94 (Fig. 6). These trends point to a substantial intensification of frailty, comorbidity, and functional loss in the oldest cohorts—indicating that current prevention and treatment strategies may be insufficient to mitigate disability and mortality in this expanding age segment.

A–D Historical and projected trends in rates of deaths (A), DALYs (B), YLDs (C), and YLLs (D) due to LBMD across nine postmenopausal age groups from 1990 to 2045. The dashed vertical line at 2021 separates observed data (1990–2021) from forecasted data (2022–2045). Solid lines represent mean estimates, with shaded areas indicating 95% uncertainty intervals.
Discussion
This study provides the first comprehensive, population-based assessment of the global epidemiological patterns and burden of LBMD among PMW, using data from the GBD 2021 Study. It highlights the substantial impact of regional disparities and socioeconomic development on LBMD outcomes across 204 countries and territories. The main findings are as follows: First, LBMD exhibits a pronounced population clustering effect among PMW. Compared to premenopausal women, PMW had a 15.17-fold higher burden of overall disease mortality, and a 6.29-fold higher burden of YLDs due to LBMD, emphasizing the critical role of the postmenopausal stage in the spectrum of bone metabolic disorders. Second, from 1990 to 2021, although ASR of death, DALYs, YLLs, and YLDs attributable to LBMD in the global PMW population have shown a general decline, the absolute number of affected individuals has continued to rise due to population aging—indicating an expanding demand for bone health services worldwide. Third, significant health improvements have been achieved among women aged 55–74. However, women aged 85 and above have become the core burden group for LBMD. Notably, the risks of death and disability caused by LBMD continue to increase among those aged 90 and older, suggesting that this age group should be prioritized in prevention and control strategies. Fourth, certain countries and regions have shown alarming trends of high and increasing LBMD burden. For example, India has experienced a rapid rise in LBMD-related burden among PMW, likely influenced by multiple factors such as population structure, screening rates, nutritional status, and healthcare resource allocation—requiring further research and targeted policy interventions. Fifth, an observable “high YLDs–low mortality” pattern exists across regions with different SDI levels. In high-SDI regions, elevated YLDs may reflect better recognition and documentation of disease-related functional loss, while early screening and secondary prevention help keep mortality rates low. Conversely, in low-SDI regions, delayed diagnosis and inadequate treatment are associated with significantly higher mortality burdens.
Osteoporosis is highly prevalent in aging women and is closely linked to the postmenopausal hormonal transition12,19. Although multiple risk factors—such as aging, genetics, lifestyle, and comorbidities—contribute to the pathogenesis of osteoporosis, estrogen deficiency remains the dominant driver in PMW19. The North American Menopause Society underscores this by identifying menopause-related hypoestrogenism as the most critical factor precipitating rapid bone loss in this population20. Supporting this, data from Cauley et al. show that women with serum estradiol (E2) levels below 5 pg/mL have a 2.5-fold increased risk of vertebral and hip fractures, confirming the direct link between estrogen depletion and skeletal fragility21. The clinical imperative for studying LBMD in PMW is rooted in the profound physiological consequences of estrogen deficiency on bone metabolism22. Estrogen plays a central role in regulating bone remodeling by maintaining the balance between osteoblastic bone formation and osteoclastic bone resorption. During menopause, the sharp decline in circulating estrogen—particularly E2—leads to an upregulation of basic multicellular unit (BMU) activity, increased osteoblast apoptosis, and prolonged osteoclast lifespan23. These changes result in a net loss of bone mass and microarchitectural deterioration, hallmark features of postmenopausal osteoporosis24,25. Furthermore, the prolonged BMU cycle exacerbates the imbalance, wherein bone resorption exceeds formation, leaving newly formed bone insufficient to compensate for structural voids. These findings underscore the need to complement molecular insights with large-scale epidemiological studies to assess the real-world burden of disease, better inform clinical risk models, and guide resource allocation and prevention strategies for aging female populations.
According to data from the United Nations Department of Economic and Social Affairs, the global PMW population increased from 360 million in 1990 to 790 million in 2019, representing a 117% rise26. The proportion of PMW in the total female population also grew from 13.7% to 20%, indicating a rapidly expanding group under global aging trends. Alarmingly, although PMW account for only one-fifth of the female population, the health burden from LBMD is disproportionately high. Our analysis shows that PMW bear more than 80% of the total LBMD-related disease burden among women, with over 90% of female deaths from LBMD occurring in this group. Even more concerning is that the mortality risk from LBMD among PMW is more than 15 times that of premenopausal women, reaffirming the central importance of this population in bone health management. This trend is also supported by epidemiological evidence. For instance, a study in the UK reported that approximately 50% of women aged over 50 will suffer from osteoporotic fractures in their lifetime—twice the incidence seen in men of the same age group27. This illustrates both the severity and specificity of postmenopausal osteoporosis at the population level.
The stark contrast between high- and low-SDI regions further highlights the role of social determinants in LBMD prevention and control. The highest concentration of deaths and DALYs from LBMD occurs in low-SDI regions, particularly sub-Saharan Africa and South Asia, consistent with widespread shortages of DXA screening, calcium/vitamin D supplementation programs, and access to osteoporosis medications28,29,30. For example, a Canadian study found that women in the lowest income quintile were twice as likely to qualify for osteoporosis treatment based on fracture risk assessment using the FRAX® tool with bone mineral density, compared to those in the highest income group31. This diagnostic gap contributes to a higher proportion of late-stage cases, with major disabling outcomes such as fractures often becoming irreversible. The rising mortality rate in low-SDI areas (EAPC = 0.28) likely reflects systemic failures in post-fracture care. Studies from Nigeria have reported 1-year mortality rates of 22.5% following hip fractures, attributed to limited surgical resources, inadequate rehabilitation services, and the absence of secondary prevention programs32. In contrast, high-SDI countries in Western Europe to USA have significantly reduced LBMD mortality by implementing fracture liaison services (FLS), which improve bisphosphonate adherence and reduce secondary fracture risk by approximately 37.2%33.
South Asia has become the “epicenter” of LBMD-related deaths, reporting 70,968 such deaths in 2021. The underlying causes are multifaceted, including accelerated population aging, widespread vitamin D deficiency (60–80% among Indian PMW), and cultural constraints on physical activity. South Asia accounts for 26% of the global female population but contributes to 32% of LBMD deaths—an imbalance that likely stems from overlapping structural factors: (1) Nutritional deficiencies, particularly in vitamin D and calcium, influenced by poor dietary diversity and sun exposure restrictions (e.g., the “purdah” system)34,35; (2) Fragmented medical infrastructure focusing more on fracture treatment than prevention36; (3) Rapid PMW population growth (India will have more than 401 million PMW by 2026), outpacing healthcare system preparedness37; (4) High out-of-pocket expenditures in several South Asian countries, limiting access to early diagnosis. In India, for example, the age-standardized death rate from LBMD reached 2100.67 per 100,000 in 2021, illustrating the amplified health burden under constrained resources. In contrast, the significant reduction in LBMD mortality in Central European countries reflects the effectiveness of national prevention strategies. Hungary’s nationwide LBMD program, which subsidized DXA screening for women aged 50 and above and mandated fracture registries, reduced hip fracture incidence by 28% between 2010 and 2020. Similarly, the Netherlands implemented mandatory vitamin D fortification in margarine and promoted fall-prevention programs in elderly care institutions, successfully slowing the growth of DALYs despite increasing population aging38,39.
Notably, while the overall burden of LBMD among PMW is declining globally, women aged 85 and older are experiencing a reversed trend. GBD data show that in 2021, both mortality rates and YLDs related to LBMD among women aged 90 and above reached historic highs, with a sharper increase than in any other age group. However, this group remains largely underserved in current bone health strategies. Studies report that the 1-year mortality rate following a first hip fracture among women aged 80+ can reach 30%, significantly higher than in the 65–79 age group. Despite this, diagnostic and treatment rates for osteoporosis in this cohort remain notably low. For example, a retrospective Japanese cohort study on denosumab treatment found that patients aged 80 years and above had significantly lower continuation rates than those aged below 80. The continuation rate declined from 85.3% at 12 months to 69.3% at 60 months40. Barriers include multimorbidity, which complicates prescribing decisions due to drug interactions and side effects; renal function decline limiting the use of common osteoporosis drugs; age limits in clinical trials (often capped at 80), leading to a lack of evidence-based guidance; and societal misconceptions that “aggressive prevention” is unnecessary in this age group. These attitudes often overlook the profound impacts of fractures on independence and quality of life. Current bone health interventions primarily target those aged 65–79, while the 85+ group faces marked deficits in drug accessibility, rehabilitation support, and family care. An age-sensitive management system is urgently needed. Integrating bone health assessments into multimorbidity management, improving community-based care networks, and promoting age-friendly home environments and muscle-strengthening programs can help build a sustainable, low-burden intervention system tailored to this group—essential for addressing the “third wave” of fracture burden driven by demographic shifts.
While forecasts suggest that by 2045, the global age-standardized death rate from LBMD may decline to 19 per 100,000, this statistic masks structural vulnerabilities. PMW aged 80 and above are expected to bear the greatest future burden, and health systems must prioritize geriatric fracture care accordingly. Japan’s “Orange Plan,” which combines community fitness41, home safety renovation, and pharmacist-led medication reviews, led to a 45% reduction in YLLs between 1990 and 2021. This low-cost, community-centered model shows high adaptability for high-burden regions such as South Asia. Nevertheless, widespread implementation faces challenges, including weak infrastructure, fragmented service delivery, and age-related cultural attitudes. Capacity-building through community health worker training, integration with family-based care, and low-cost environmental modifications can improve feasibility—provided resource constraints and data gaps are addressed through phased pilots and policy integration.
To address the growing burden of postmenopausal LBMD, a comprehensive and multifaceted prevention strategy is essential. The increasing global prevalence of LBMD, particularly among women aged 85 and older, necessitates both individual-level interventions and systemic public health strategies. At the individual level, early identification through periodic fracture risk assessments, using tools such as FRAX® with or without BMD input, is crucial, especially in resource-limited settings. Nutritional optimization—ensuring adequate calcium and vitamin D intake—alongside regular weight-bearing exercises and muscle-strengthening activities, has proven effective in reducing fracture risk, improving balance, and preventing falls. Smoking cessation, alcohol moderation, and home safety modifications should be part of routine counseling for PMW to further minimize risk. On the pharmacological front, bisphosphonates and denosumab remain first-line treatments for high-risk individuals, while emerging anabolic agents such as romosozumab have shown promise in enhancing bone formation and structural integrity. For women in the early stages of menopause with low fracture risk but significant symptoms, hormone therapy (HT) and estrogen therapy (ET) can provide effective prevention, offering benefits that outweigh potential risks when appropriately used. Public health strategies must also tackle the disparities in LBMD outcomes across different socioeconomic strata. In low- and middle-income countries, increasing access to affordable DXA screenings, subsidizing calcium/vitamin D supplementation, and deploying trained community health workers will be key to improving early detection and treatment adherence. Programs like Japan’s “Orange Plan,” Hungary’s subsidized DXA program, and Korea’s integration of osteoporosis care into primary health services provide scalable and cost-effective models for intervention. National FLS, when incorporated into hospital discharge and outpatient systems, have been shown to reduce secondary fractures by over 35%, demonstrating the importance of a holistic approach to osteoporosis care. Digital health platforms and mobile-based educational tools present new opportunities to enhance awareness and improve compliance, particularly in regions with low health literacy. Ultimately, addressing LBMD in PMW requires a lifecycle approach, starting from peak bone mass optimization in early adulthood to promoting active aging strategies for the elderly. A multilevel approach, combining clinical interventions, community-based programs, and policy initiatives, is crucial to mitigating the future fracture epidemic, reducing long-term disability, and enhancing quality of life for aging women worldwide.
This study reveals LBMD as a biosocial disease shaped not only by menopausal biology but also by persistent inequalities in healthcare systems. Although ASRs have declined, the absolute burden among PMW continues to rise—particularly in low-SDI regions and among the oldest-old, where access to timely diagnosis and treatment remains limited. Addressing this challenge requires a shift in perspective: from seeing LBMD as an inevitable sign of aging to treating it as a preventable, manageable condition through integrated, life-course-based strategies. Crucially, LBMD is not merely a marker of biological aging—it is a lens through which we must confront the deeper inequities embedded in global aging and gendered health systems. Ensuring equitable access to bone health interventions is not only a clinical necessity but a moral imperative in the era of demographic transition.
Methods
Data source
This study utilizes data from the GBD 2021 results (available at https://vizhub.healthdata.org/gbd-results/), offering a comprehensive assessment of the burden of 371 diseases and injuries at global, regional, and national levels. GBD 2021 estimates cover 204 countries and territories across 21 regions. LBMD, as defined by the World Health Organization (WHO), is a skeletal disease marked by reduced bone density and microarchitectural deterioration, leading to increased fracture risk42.
We extracted data on the annual incidence, death, and DALY for LBMD from 1990 to 2021. Bayesian meta-regression disease modeling (DisMod-MR, version 2.1) was used for data analysis. This framework generates internally consistent estimates of disease prevalence, incidence, remission, and death, stratified by sex, region, year, and age group, and supports ASR analyses using linear regression models43. DALYs, the primary metric in our study, represent the sum of YLLs and YLDs, offering a comprehensive measure of health losses due to premature death and reduced quality of life. YLDs are calculated using disease prevalence and associated disability weights, while YLLs are based on death counts and life expectancy data, estimated via demographic data and survival models. DisMod-MR enables consistent estimation of these metrics, accounting for factors such as sex, age group, region, and year43. Additionally, the SDI, a composite measure of social development, was incorporated. The SDI, calculated as the geometric mean of fertility rates, education levels, and per capita income, is categorized into five levels: low, low-middle, middle, high-middle, and high. This classification helps analyze the impact of socioeconomic development on health outcomes across regions.
Statistics
All rate data are reported per 100,000 population with 95% confidence intervals (CI), derived by drawing 1000 samples from the posterior distribution and calculating the 25th and 95th ordered values. DALYs rates are presented as estimates per 100,000 population, while case counts represent the absolute burden of LBMD among PMW; both metrics include 95% CI. All data analyses and visualizations were performed using R software, with two-sided p-values less than 0.05 considered statistically significant.
EAPC
Temporal trends in age-standardized incidence and DALY rates for LBMD were assessed using the EAPC method. ASR is calculated to adjust for population age structure, enabling cross-temporal comparisons. EAPC, derived from a log-linear regression model, quantifies the annual rate of change in ASR. The model is expressed as (1):
where y is the natural logarithm of ASR, x denotes calendar year, α is the intercept, β represents the slope coefficient, and ε is the error term. The EAPC is calculated as (2):
Trends were categorized as follows based on 95% CI: increasing if the EAPC and its lower CI limit were both positive, decreasing if the EAPC and its upper CI limit were both negative, and stable if the 95% CIs included zero. All analyses were conducted in R (version 4.3.1) using the ggplot2 package for visualization, with graphical outputs refined in Adobe Illustrator 2024 (version 28) to ensure clarity and reproducibility44.
Cross-country inequality analysis
We quantified absolute and relative inequalities in LBMD burden among PMW using the WHO-recommended SII and Concentration Index. SII for incidence, death, and DALYs was derived via weighted regression models based on a relative socioeconomic position scale, defined by cumulative population percentiles ranked by per capita GDP. The Concentration Index was calculated by integrating the area between the Lorenz curve of the LBMD burden and the line of equality, linked to income distribution. To assess temporal trends (1990–2021), we analyzed data from 204 countries/territories using robust regression (rlm) to minimize bias from outliers and heterogeneity. Sensitivity analyses confirmed the superiority of rlm over linear regression (lm) in handling skewed data. For DALYs-based inequality, the Concentration Index was further calculated by aligning cumulative DALY proportions with population distributions ranked by SDI. Global burden metrics (deaths, DALYs, YLLs, YLDs) were systematically evaluated for LBMD among PMW. This dual approach (SII/ Concentration Index) provided robust estimates of both absolute and relative health inequalities, supporting comparative analyses across populations and time periods45.
BAPC model projection
In this study, we utilized the BAPC model to forecast the global trends in LBMD death and disease burden among PMW. The BAPC model, which has been widely applied in epidemiological forecasting, was chosen for its ability to estimate age-specific rates while accounting for temporal effects and cohort effects. This approach allows for more accurate predictions by considering age-related trends, period-specific variations, and cohort-specific influences. The model was implemented in a Bayesian framework, using a Markov Chain Monte Carlo (MCMC) algorithm to estimate the posterior distributions of parameters. This allowed us to incorporate uncertainty in the model’s predictions and generate 95% CI for all outcomes. Specifically, we used data from the GBD study, which provides comprehensive estimates of death and DALYs for LBMD on a global scale. The data were age-standardized to account for differences in population structures over time, and the model was fitted separately for each region and sex. The model incorporated data from 1990 to 2021 and projected future trends up to 2045. Sensitivity analyses were conducted to assess the robustness of the model, particularly in regions with limited data availability. In addition to estimating the overall global burden, we also assessed regional variations and incorporated potential socio-economic factors that may influence trends in LBMD death and disease burden. The results of the BAPC model were presented as point estimates along with the 95% credible intervals, providing a range of uncertainty for the predicted values46.
Data availability
The data analyzed is publicly provided by the Institute for Health Metrics and Evaluation (http://www.healthdata.org/; http://ghdx.healthdata.org/gbd-results-tool).
Code availability
Some or all data, models, or code generated or used during the study are available from the corresponding author by request.
References
Eastell, R. & Szulc, P. Use of bone turnover markers in postmenopausal osteoporosis. The Lancet Diabetes & Endocrinology 5, 908–923 (2017).
Wu, C., Chen, D., Stout, M. B., Wu, M. & Wang, S. Hallmarks of ovarian aging. Trends in Endocrinology & Metabolism (2025).
Foundation, N. O. America’s bone health: the state of osteoporosis and low bone mass in our nation. Washington, Dc: National Osteoporosis Foundation, 1-55 (2002).
Cummings, S. R. & Melton, L. J. Epidemiology and outcomes of osteoporotic fractures. The Lancet 359, 1761–1767 (2002).
Cooper, C. et al. Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos. Int. 22, 1277–1288 (2011).
Adami, G. et al. Osteoporosis in 10 years time: a glimpse into the future of osteoporosis. Ther. Adv. Musculoskelet. Dis. 14, 1759720X221083541 (2022).
Onizuka, N. & Onizuka, T. Disparities in osteoporosis prevention and care: understanding gender, racial, and ethnic dynamics. Curr. Rev. Musculoskelet. Med. 17, 365–372 (2024).
Händel, M. N. et al. Fracture risk reduction and safety by osteoporosis treatment compared with placebo or active comparator in postmenopausal women: systematic review, network meta-analysis, and meta-regression analysis of randomised clinical trials. Bmj. 381 (2023).
Curry, S. J. et al. Screening for osteoporosis to prevent fractures: us preventive services task force recommendation statement. Jama. 319, 2521–2531 (2018).
Ji, M. & Yu, Q. Primary osteoporosis in postmenopausal women. Chronic Diseases and Translational Medicine 1, 9–13 (2015).
Black, D. M. & Rosen, C. J. Postmenopausal osteoporosis. N. Engl. J. Med. 374, 254–262 (2016).
Raisz, L. G. Pathogenesis of osteoporosis: concepts, conflicts, and prospects. The Journal of Clinical Investigation 115, 3318–3325 (2005).
Laib, A., Kumer, J. L., Majumdar, S. & Lane, N. E. The temporal changes of trabecular architecture in ovariectomized rats assessed by microct. Osteoporos. Int. 12, 936–941 (2001).
Hense, J. D. et al. The role of cellular senescence in ovarian aging. Npj Aging 10, 35 (2024).
Bonnet, N., Bourgoin, L., Biver, E., Douni, E. & Ferrari, S. Rankl inhibition improves muscle strength and insulin sensitivity and restores bone mass. The Journal of Clinical Investigation 129, 3214–3223 (2023).
Khosla, S. Minireview: the opg/rankl/rank system. Endocrinology 142, 5050–5055 (2001).
Macdonald, B. T., Tamai, K. & He, X. Wnt/β-catenin signaling: components, mechanisms, and diseases. Dev. Cell 17, 9–26 (2009).
Isola, J. V. et al. Reproductive ageing: inflammation, immune cells, and cellular senescence in the aging ovary. Reproduction 168 (2024).
Kuo, T. & Chen, C. Bone biomarker for the clinical assessment of osteoporosis: recent developments and future perspectives. Biomark. Res. 5, 18 (2017).
Mcclung, M. R. et al. Management of osteoporosis in postmenopausal women: the 2021 position statement of the north american menopause society. Menopause-J. N. Am. Menopause Soc. 28, 973–997 (2021).
Cauley, J. A. Estrogen and bone health in men and women. Steroids 99, 11–15 (2015).
Lu, L. & Tian, L. Postmenopausal osteoporosis coexisting with sarcopenia: the role and mechanisms of estrogen. J. Endocrinol. 259 (2023).
Bolamperti, S., Villa, I. & Rubinacci, A. Bone remodeling: an operational process ensuring survival and bone mechanical competence. Bone Res 10, 48 (2022).
Velarde, M. C. Pleiotropic actions of estrogen: a mitochondrial matter. Physiol. Genomics 45, 106–109 (2013).
Raehtz, S., Bierhalter, H., Schoenherr, D., Parameswaran, N. & Mccabe, L. R. Estrogen deficiency exacerbates type 1 diabetes–induced bone tnf-α expression and osteoporosis in female mice. Endocrinology 158, 2086–2101 (2017).
United, N., Department, O. E. A. S. & Population, D. World population prospects 2024, online edition (United Nations, 2024).
Van Staa, T. P., Dennison, E. M., Leufkens, H. A. & Cooper, C. Epidemiology of fractures in england and wales. Bone 29, 517–522 (2001).
Mogire, R. M. et al. Prevalence of vitamin d deficiency in africa: a systematic review and meta-analysis. The Lancet Global Health 8, e134–e142 (2020).
Reid, I. R. & Bolland, M. J. Calcium and/or vitamin d supplementation for the prevention of fragility fractures: who needs it? Nutrients 12, 1011 (2020).
Chan, S. P., Scott, B. B. & Sen, S. S. An asian viewpoint on the use of vitamin d and calcium in osteoporosis treatment: physician and patient attitudes and beliefs. Bmc Musculoskelet. Disord. 11, 1–13 (2010).
Brennan, S. L., Leslie, W. D. & Lix, L. M. Is lower income associated with an increased likelihood of qualification for treatment for osteoporosis in canadian women? Osteoporos. Int. 25, 273–279 (2014).
Adesina, S. A. et al. Fragility hip fractures among nigerian older adults: a retrospective study of epidemiology, mobility and mortality outcomes at 3 and 12 months post-hospital discharge. Arch. Osteoporos. 20, 61 (2025).
Mclellan, A. R. et al. Fracture liaison services for the evaluation and management of patients with osteoporotic fracture: a cost-effectiveness evaluation based on data collected over 8 years of service provision. Osteoporos. Int. 22, 2083–2098 (2011).
Aparna, P., Muthathal, S., Nongkynrih, B. & Gupta, S. K. Vitamin d deficiency in india. J. Fam. Med. Prim. Care 7, 324–330 (2018).
Narula, R. et al. Vitamin d deficiency among postmenopausal women with osteoporosis. Journal of Clinical and Diagnostic Research: Jcdr 7, 336 (2013).
Patni, R. Normal bmd values for indian females aged 20–80 years. J. Mid-Life Health 1, 70–73 (2010).
Pallikadavath, S. et al. Natural menopause among women below 50 years in india: a population-based study. Indian. J. Med. Res. 144, 366–377 (2016).
Vaes, A. et al. Food sources of vitamin d and their association with 25-hydroxyvitamin d status in dutch older adults. The Journal of Steroid Biochemistry and Molecular Biology 173, 228–234 (2017).
Lips, P., Graafmans, W. C., Ooms, M. E., Bezemer, P. D. & Bouter, L. M. Vitamin d supplementation and fracture incidence in elderly persons: a randomized, placebo-controlled clinical trial. Ann. Intern. Med. 124, 400–406 (1996).
Kobayashi, K. et al. Persistence of denosumab therapy among patients with osteoporosis. Asian Spine J 14, 453 (2020).
Chen, L., Inoue, M. & Buckley, N. Case studies on community care in japan: considerations for mitigating social isolation and loneliness in older adults with dementia. Front. Public Health 12, 1411217 (2024).
Brauer, M. et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. The Lancet 403, 2162–2203 (2024).
Ferrari, A. J. et al. Global incidence, prevalence, years lived with disability (ylds), disability-adjusted life-years (dalys), and healthy life expectancy (hale) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. The Lancet 403, 2133–2161 (2024).
Hankey, B. F. et al. Partitioning linear trends in age-adjusted rates. Cancer. Causes. Control. 11, 31–35 (2000).
Ordunez, P. et al. Rheumatic heart disease burden, trends, and inequalities in the americas, 1990–2017: a population-based study. The Lancet Global Health 7, e1388–e1397 (2019).
Knoll, M. et al. An r package for an integrated evaluation of statistical approaches to cancer incidence projection. Bmc Med. Res. Methodol. 20, 1–11 (2020).
Acknowledgements
The authors acknowledge the Institute for IHME at the University of Washington, the GBD collaborators, and all staff who contributed to data collection and processing. This study was supported by the National Natural Science Foundation of China (Grant No. 82460548) and the Natural Science Foundation of Jiangxi Province (Grant No. 20242BAB20368), both awarded to J.Y.T.
Author information
Authors and Affiliations
Contributions
J.Y.T., S.K.Z., and B.S.Y. conceived and designed the study. H.F.L., S.B.C., and M.L.S. contributed to drafting the manuscript and collecting GBD data. H.F.L., S.B.C., M.L.S., and J.L.X. conducted age standardization of the data, EAPC analysis, and health inequality analysis of the GBD data. J.Y.T., B.S.Y., H.F.L., S.B.C., C.X.Z., and J.L.X. participated in the discussion of the manuscript and the verification and confirmation of the study conclusions. Final approval of manuscript: all authors.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liang, H., Chen, S., Shi, M. et al. Global epidemiology and burden of osteoporosis among postmenopausal women: insights from the Global Burden of Disease Study 2021. npj Aging 11, 78 (2025). https://doi.org/10.1038/s41514-025-00269-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41514-025-00269-2
