
Abstract
This study investigates the factors influencing users’ behavioral intention to adopt facial recognition payment (FRP) in smart hospitals, considering convenience and potential risks. The unified theory of acceptance and use of technology (UTAUT), the diffusion of innovations theory, and trust theory are employed to identify critical factors for promoting FRP adoption. A quantitative cross-sectional survey is conducted among smart hospital users in China, collecting 811 valid questionnaires, and the partial least squares structural equation method (PLS-SEM) is utilized for analysis. The results show that performance expectancy, effort expectancy, social influence, and facilitating conditions positively affect behavioral intention. Privacy concerns and perceived risks negatively impact trust in FRP, while familiarity enhances trust. Trust in FRP and personal innovativeness positively influence behavioral intention, with personal innovativeness moderating the trust-behavioral intention relationship. The findings emphasize the mediating role of trust in FRP and the importance of familiarity and personal innovativeness in driving FRP adoption. Gender (male or female) does not significantly impact the relationships and path coefficients in the model. However, slight discrepancies are observed between the permutation test and Henseler’s MGA in terms of the effect of privacy concerns on trust in FRP. This research contributes to the literature on users’ behavioral intentions, aiding smart hospitals in promoting FRP adoption while considering user concerns.
Similar content being viewed by others


Introduction
Recent advancements in internet and information technology (IT) have driven the development of non-cash digital payment solutions (Tee and Ong, 2016). Artificial intelligence (AI) technologies, particularly facial recognition (FR), have enhanced the purchasing experience for consumers (Lo Piano, 2020). Negri et al. (2019) found that 82.94% of passengers at three Brazilian airports are willing to use biometric check-in technology, highlighting its potential for faster, safer, and more efficient processes. Hwang et al. (2024) explored behavioral and switching intentions towards AI-based facial recognition payment (FRP) in restaurants, emphasizing cultural differences between South Korean and US consumers. Del Rio et al. (2016) reviewed FR technology’s effectiveness in European/Schengen airports, comparing ABC e-gates and recommending improvements.
China has led the commercialization of FR technology, including FRP, but similar advancements are occurring globally. For example, the US and Korea are exploring FRP in restaurants, emphasizing its convenience, efficiency, and security over QR code scanning (Hwang et al. 2024; Joo et al. 2024). The COVID-19 pandemic has accelerated the adoption of FRP, especially in healthcare settings where contactless transactions are critical (Priem, 2021). This trend aligns with the global push for “smart hospitals,” which reduce the workload on medical personnel while enhancing patient services (Liang et al. 2022). Integrating FRP with mHealth, telemedicine, and health kiosks offers more accessible and efficient medical services (Lee and Pan, 2023b), while intelligent management systems streamline administrative tasks.
Though QR codes have transformed electronic transactions, FRP has gained global popularity, especially in China (Gao et al. 2023; Li and Li, 2023; Moriuchi, 2021). In healthcare, the integration of digital platforms, online patient portals, and telehealth services has improved convenience, expanded self-service options, and enhanced access to remote healthcare (Liang et al. 2022). Studies in Europe and North America report similar benefits, further illustrating FRP’s global potential (Liu, 2020; Moriuchi, 2021). A report by Nielsen Norman Group (Liu, 2020) showed that new users complete the FRP payment process in 10–15 s, and regular users in less than 10 s—significantly faster than QR code-based mobile payments (Li and Li, 2023).
FR systems face challenges, such as occlusion, face pose variations, lighting, head motion, and demographic differences between the training and testing phases (Zhang et al. 2018). In healthcare, additional challenges include pricing transparency, complex billing, and manual billing processes. Fintech solutions like FRP can address these issues by streamlining payments and personalizing patient programs. However, adoption is limited by factors such as a lack of awareness among patients and healthcare providers, concerns over the security and privacy of sensitive information, and staff resistance to technological integration (Moriuchi, 2021; Palash et al. 2022; Shiau et al. 2023; Al-Okaily et al. 2020). Privacy is a critical concern, as FRP relies on collecting and processing facial data, which can be sensitive and prone to misuse (Li and Li, 2023). Strong privacy protections and security measures are essential to build trust and ensure user confidence in adopting FRP. This necessitates further exploration of the factors influencing FRP adoption in healthcare settings.
The Unified Theory of Acceptance and Use of Technology (UTAUT), trust theory, and diffusion of innovations (DOI) theory offer frameworks for understanding user behavior and decision-making (Yu et al. 2024b). UTAUT identifies performance expectancy (PE), effort expectancy (EE), social influence (SI), and facilitating conditions (FC) as key drivers of technology acceptance (Venkatesh et al. 2003). Trust theory highlights the importance of users’ confidence in FRP’s security and reliability, particularly given the sensitivity of facial data (Li and Li, 2023). Privacy concerns, perceived risks, and familiarity with FRP also affect user adoption (Shiau et al. 2023). Understanding the factors influencing FRP acceptance in smart hospitals is crucial for overcoming the challenges associated with traditional financial services, reducing transaction costs, and streamlining payments.
Despite FRP’s growing popularity, especially during the pandemic, there is limited research on patient-consumer perspectives and the factors influencing FRP acceptability in smart hospitals. Trust has been identified as a crucial factor in the intention to use FRP services (Moriuchi, 2021; Palash et al. 2022), but more research is needed to explore how trust is built in FRP systems. Privacy, security concerns, perceived risks, and familiarity with the technology are all factors that significantly impact users’ decisions in smart hospitals (Al-Okaily et al. 2020; Akhtar and Rattani, 2017; Breward et al. 2017; Gong et al. 2019; Hsieh and Li, 2021; Johnson et al. 2018; Lancelot Miltgen et al. 2013; Morosan, 2012b, 2016; Sharma et al. 2018). DOI theory provides insights into how innovations like FRP spread within social systems, from initial awareness to eventual adoption (Rogers et al. 2014).
This study aims to fill the gap in research by investigating the factors influencing behavioral intentions (BI) to adopt FRP in smart hospitals, focusing on the Chinese context. It extends the UTAUT framework by including personal innovativeness, trust, privacy concerns, perceived risks, and familiarity as factors influencing FRP adoption. Although previous studies have examined fintech solutions and FRP in retail, hospitality, and restaurants (Dang et al. 2022; Hwang et al. 2024; Morosan, 2020), research on FRP in smart hospitals remains limited.
This study addresses the following research questions:
-
1.
What factors, derived from UTAUT, trust theory, and DOI, influence users’ BI to use FRP in smart hospitals?
-
2.
Does personal innovativeness moderate the relationship between trust in FRP and BI to use FRP in smart hospitals?
-
3.
Are there gender differences in how these factors affect users’ BI to use FRP in smart hospitals?
This research contributes to the literature by applying UTAUT, DOI, and trust theory to the context of FRP adoption in smart hospitals, and by examining personal innovativeness as a moderator. It also investigates gender differences in the determinants of FRP adoption, providing valuable insights for practitioners, system designers, and hospital managers. By addressing the perspectives of these stakeholders, the study helps ensure the successful integration of FRP systems in hospital operations, improving both efficiency and patient satisfaction.
Literature review and research hypotheses
FRP in smart hospitals in China
Smart hospitals integrate advanced technologies like IoT, AI, big data analytics, and FRP systems to improve patient care, streamline operations, and offer a seamless experience for both patients and medical staff (Abdulkareem et al. 2021). These innovations enable features such as remote monitoring, automated administration, personalized treatments, and enhanced data security. In China, debates on healthcare reform have polarized opinions between advocates of centralized planning and proponents of controlled marketization. This divide affects FRP integration in smart hospitals. Marketization supporters push for reforms in provider payment mechanisms, favoring third-party purchasing and public contracts, while the government-backed faction prefers top-down control and regulation. Within this context, the adoption of FRP aims to facilitate “cardless” consultations, streamline hospital operations, and improve patient experiences. FRP-enabled medical insurance terminals connect with hospital information systems (HIS), integrating mobile payments and electronic insurance vouchers (Turban et al. 2018). Installed at hospital windows and service desks, these terminals expedite transactions. When users opt for FRP, a camera captures their facial image, which the system matches to stored biometrics. Upon successful verification, the payment is authorized and processed. Appendix 1 presents a storyboard illustrating the FRP journey in smart hospitals (Virtual Smart Technologies, 2024). Initially, patients register for FRP by scanning their faces and creating a digital profile stored securely. Upon hospital arrival, the system captures the patient’s face for identity verification. Verified patients can then access medical services, authorize payments through FR, and receive invoices and follow-up information digitally.
Despite these advancements, FRP faces challenges, particularly concerning privacy and security. The collection and processing of facial data raise concerns about misuse and unauthorized access (Li and Li, 2023). Effective privacy protections and security measures are crucial to building user confidence. Additionally, limited awareness among patients and healthcare providers about FRP’s benefits can hinder adoption (Surf, 2022). Resistance from staff due to the perceived complexity of integrating new technologies into established workflows further complicates implementation (Al-Okaily et al. 2020). Technical issues, such as the need for interoperability between FRP and existing systems, also pose challenges. However, FRP implementation aligns with Chinese medical insurance policies, improving real-name hospital visits and enabling remote payment for medical services. “Online hospitals” use digital technologies to provide remote healthcare services, including medical insurance payments for electronic prescriptions and drug deliveries. FRP technology has reduced outpatient waiting times, with over 60% of medical insurance patients experiencing a decrease from 10 to 3 min (Nigam et al. 2022).
Understanding the factors that influence BI to adopt FRP in Chinese smart hospitals is essential. This study explores how PE, EE, SI, FC, trust, privacy concerns, perceived risks, familiarity, and personal innovativeness affect FRP adoption. Additionally, it examines whether personal innovativeness moderates the relationship between trust and BI and whether gender differences impact these determinants. The findings will offer valuable insights for FRP system developers, policymakers, and hospital managers, helping to address privacy concerns, enhance trust, and promote the widespread use of FRP in smart hospitals.
Unified theory of acceptance and use of technology
The UTAUT model asserts that technology adoption depends on BI, influenced by PE, EE, SI, and FC. These predictors’ impact is moderated by age, gender, experience, and voluntariness of use (Venkatesh et al. 2003). UTAUT integrates eight prominent theories and models, providing superior performance in predicting BI. It accounts for 70% of variability in usage intention, surpassing models by Davis et al. (1992) and Sheppard et al. (1988).
UTAUT has been applied across various domains, including e-government (Rodrigues et al. 2016), biometric authentication systems (Akinnuwesi et al. 2016), biometric payments (Liu and Tu, 2021), collaborative technology use (Akinnuwesi et al. 2022; Brown et al. 2010), web-based learning (Chiu and Wang, 2008; Thongsri et al. 2018), and internet banking services (Rahi et al. 2019). While UTAUT has been used to explore FRP adoption (Ciftci et al. 2021; Liu and Tu, 2021; Moriuchi, 2021), its application in smart hospitals remains underexplored. UTAUT’s framework is ideal for studying FRP in smart hospitals, as it systematically examines how key factors and moderators impact technology acceptance.
In smart hospitals, PE reflects the perceived benefits of FRP in improving healthcare delivery, security, and operational efficiency. EE addresses the ease of use for healthcare staff and patients, while SI considers how peer, supervisor, and patient attitudes influence FRP adoption. FC examines the availability of technical infrastructure and support for FRP implementation. Moderating factors like age, gender, experience, and voluntariness of use are also critical. Younger professionals may be more open to FRP due to greater tech familiarity (Shiau et al. 2023), and the voluntariness of FRP usage can shape acceptance levels among staff and patients. Examining these factors through UTAUT can offer valuable insights for policymakers and healthcare administrators, helping them design effective FRP systems that enhance care quality and efficiency.
Trust theory
Trust is a key factor in technology adoption, particularly for FRP systems in smart hospitals. Studies (Luo et al. 2010; Tams et al. 2018; Yu et al. 2023b) emphasize trust’s role in influencing individuals’ behavioral intentions (BI) to adopt new technologies. Trust is the belief in the reliability, integrity, and benevolence of a party (Chen and Dhillon, 2003) and is crucial in relationships, transactions, and technology adoption (Alzahrani et al. 2017). In the context of FRP, trust significantly impacts users’ acceptance (Liu and Tao, 2022; Hernandez-Ortega, 2011).
Trust theory suggests that trust is shaped by trustworthiness and perceived risks (Kim et al. 2008). Trustworthiness encompasses competence, reliability, integrity, and benevolence (Sekhon et al. 2014). For FRP systems, users are more likely to trust the technology if they see it as reliable, secure, and accurate (Corbitt et al. 2003; Ray et al. 2011). For example, the system’s ability to correctly identify individuals and process payments builds trust (Kesharwani and Singh, 2012). Trust in the organizations implementing FRP also strengthens when they are viewed as reliable and trustworthy (Kim et al. 2008). Both social and institutional trust play roles in FRP adoption. Social trust refers to general trust in others or society (Kwon, 2019), while institutional trust relates to the credibility and ethics of the hospital (Smith, 2010; Giustiniano and Bolici, 2012). Trust in FRP systems is further influenced by the organization’s reputation and commitment to privacy and security (Lai and Rau, 2021). Ensuring transparency about data handling and implementing strong security measures, such as two-factor authentication and biometric verification, can boost user trust (Surf, 2022).
Perceived risks, like data breaches or identity theft, also affect trust. Concerns about privacy and unauthorized data access can undermine confidence in FRP (Zhang et al. 2019; Cavoukian, 2008). To build trust, organizations must implement robust security measures, transparent data practices, and clear communication about risk mitigation (Sicari et al. 2015). Privacy concerns are especially important in the case of biometric data, where fears of misuse or unauthorized access are common (Heimo et al. 2012). Addressing these concerns with strong data protection practices can foster trust and increase adoption (Palash et al. 2022; Moriuchi, 2021). Familiarity with FR technology also affects trust. Users who are more familiar with or have had positive experiences with FRP systems are more likely to trust and use them (Seng et al. 2021). Building familiarity through education, demonstrations, and user-friendly interfaces can increase trust and adoption (Ming-Yen Teoh et al. 2013).
In conclusion, while trust theory directly addresses trustworthiness and perceived risks, factors like privacy concerns, familiarity, and perceived risks also play a crucial role in influencing BI toward FRP in smart hospitals. Addressing these elements is essential for fostering trust and encouraging widespread adoption of FRP systems.
Diffusion of innovations theory
The DOI theory, introduced by Everett Rogers in 1962, offers a framework for understanding how new technologies, products, or ideas spread within a social system (Rogers et al. 2014). The theory outlines five stages in the adoption process: knowledge, persuasion, decision, implementation, and confirmation (Wisdom et al. 2014), each influenced by factors that either facilitate or hinder adoption (Kaufmann et al. 2009). DOI also categorizes individuals into groups based on their willingness to adopt: innovators, early adopters, early majority, late majority, and laggards (Dale et al. 2021). Innovators and early adopters are more open to new ideas and tend to adopt them earlier, making them key targets for promoting technologies like FRP in smart hospitals.
Several factors affect the diffusion of innovations: perceived relative advantage, compatibility, complexity, social influence, and resource availability. Perceived relative advantage refers to the belief that an innovation offers significant benefits over existing alternatives, such as improved efficiency or convenience, increasing its likelihood of adoption (Agarwal and Prasad, 1997; Lin and Chen, 2012). Compatibility measures how well an innovation aligns with potential adopters’ values and needs—innovations that fit with existing practices are more likely to be accepted (Meijer et al. 2015). Complexity, or how easy the innovation is to understand and use, also influences adoption—simpler technologies spread more quickly (Wisdom et al. 2014; Katona et al. 2011). Social influence plays a critical role in adoption. When individuals see others in their network benefiting from an innovation, they are more likely to adopt it (Cho et al. 2012). Adequate resources, training, and infrastructure also facilitate adoption, helping overcome barriers and building confidence (Wandersman et al. 2012). Personal innovativeness—the tendency to embrace new technologies early—can further accelerate diffusion, as early adopters often influence others in their networks (Marcati et al. 2008; Greenhalgh et al. 2004).
In the context of FRP systems in smart hospitals, DOI theory helps identify strategies to promote adoption and address potential barriers (Pan et al. 2019). Understanding how relative advantages, compatibility, complexity, social influence, and resource availability impact FRP adoption can inform tailored strategies (Lee and Coughlin, 2015). Emphasizing FRP’s benefits, ensuring compatibility with healthcare practices, simplifying the interface, leveraging social influence, and providing necessary support can drive adoption (Cresswell and Sheikh, 2013). Applying DOI theory in this way helps develop effective policies and strategies to foster the diffusion of FRP in healthcare settings.
Research hypotheses
The effect of performance expectancy
PE is derived from the UTAUT model, where it is a critical determinant of user acceptance of technology. The PE refers to the individual’s belief that the application of IT or a system can improve the level of an individual’s work performance (Venkatesh et al. 2003). Scholars have found that PE has a significant influence on BI in all types of models, whether in spontaneous or compulsive situations, through research and analysis (Agarwal and Prasad, 1998; Compeau and Higgins, 1995; Taylor and Todd, 1995; Thompson et al. 1991; Yu et al. 2023b). PE is a major factor driving IT acceptability, as it strongly correlates with the intention to use IT services. For example, PE has been found to significantly affect BI when evaluating location-based services and privacy risks (Zhou, 2012). Studies on biometric authentication, such as fingerprint-based systems, show that PE, particularly regarding security and expected performance, is a critical factor in user acceptance (Ogbanufe and Kim, 2018). Rasiah and Yen (2020) similarly found that PE is the most important factor influencing the acceptance of biometric identification, suggesting that users value the benefits of biometric solutions. In this study, PE refers to users’ perceptions of the utility and efficiency improvements offered by FRP systems in smart hospitals. Based on this, the following hypothesis is proposed:
H1: The PE positively influences the BI to use FRP.
The effect of effort expectancy
EE, from the UTAUT model, refers to how easy an individual perceives the use of a system to be, including the simplicity of its operation and the level of effort required to learn it (Venkatesh et al. 2003). Research has consistently shown that EE significantly impacts BI in various models (Agarwal and Prasad, 1997; Thompson et al. 1994). According to Venkatesh et al. (2003), EE plays a crucial role in shaping consumer behavior. For example, Tandon et al. (2016) found that EE strongly influenced Indian consumers’ online shopping intentions using the UTAUT2 model. Similarly, Muhayiddin et al. (2011) showed that consumer expectations regarding electronic payment systems significantly affect BI. Ease of use and reduced cognitive effort are known motivators for adopting biometric payment systems (Ogbanufe and Kim, 2018). In this study, EE refers to the effort individuals believe is required to adopt and use FRP in smart hospitals. This includes the ease of system use, how intuitive it feels, and the time and energy needed to operate it (Okumus et al. 2018). If users perceive FRP to have a clear interface and simple operation, they are more likely to adopt it (Morosan, 2020; Ciftci et al. 2021). Thus, if users believe FRP is easy to master and requires minimal effort, they are more likely to use it. Based on this, the following hypothesis is proposed:
H2. The EE positively influences the BI to use FRP.
The effect of social influence
SI refers to the extent to which individuals’ decisions to use IT systems are shaped by the opinions of important people or groups around them (Venkatesh et al. 2003). Yang (2010) found that SI was the most influential factor affecting American consumers’ willingness to use mobile shopping services. Ajzen (1985) argued that subjective perceptions and external contexts significantly influence decision-making. Taylor and Todd (1995) also highlighted the role of media and culture in shaping BI. Research on the adoption of e-government services, mobile wallets, and mobile banking consistently shows that SI plays a significant role in shaping BI (Hung et al. 2006; Ho et al. 2013; Powell et al. 2012; Shin, 2009). Nysveen et al. (2005) found that people often observe the behavior of those around them before adopting new technologies, including mobile information services. SI has also been identified as a key factor in adopting biometric technologies, such as FRP (Zimmermann and Geber, 2020). In the context of FRP, seeing others use the technology can normalize its use and increase its perceived value, even in environments with limited choices (Ciftci et al. 2021). The greater the societal influence, the more likely individuals are to adopt FRP in smart hospitals. Thus, the following hypothesis is proposed:
H3. The SI positively influences the BI to use FRP.
The effect of facilitating conditions
FC refers to the degree to which individuals believe that the existing organizational and technical infrastructure supports the use of IT or systems (Venkatesh et al. 2003). This includes the operational capabilities, technical support, and environmental conditions that enable technology adoption. Research shows that strong facilitating conditions positively impact user behavior by making it easier for individuals to adopt and integrate new technologies into their routines. For example, in mobile banking, marketing campaigns that increase user knowledge and skills improve perceptions of FC, leading to higher adoption rates (Zhou et al. 2010). Shibl et al. (2013) noted that FC significantly influences the behavior of medical professionals in adopting new technologies. Similarly, FC has been shown to impact the use of biometric technology in ATMs (Ngugi et al. 2011). During the COVID-19 pandemic, fear of physical contact increased the importance of FC, as they positively influenced BI toward digital payments (Musyaffi et al. 2021). Facilitating conditions include technical support, user-friendly interfaces, educational resources, and robust infrastructure like reliable internet and secure payment systems (Sarrab et al. 2016). In developing countries, government-provided legal and technological infrastructure enhances FC, which significantly affects users’ BI toward adopting technologies like Bitcoin and cryptocurrencies (Yeong et al. 2022; Miraz et al. 2022). In this study, FC refers to the technical resources and support available for users to adopt FRP in smart hospitals. Thus, the following hypothesis is proposed:
H4. FC positively influences consumers’ BI to use FRP.
The effect of privacy concerns
Privacy concerns have been widely recognized as a major barrier to the adoption of biometric technologies (Al-Okaily et al. 2020; Akhtar and Rattani, 2017; Breward et al. 2017; Gong et al. 2019; Hsieh and Li, 2021; Johnson et al. 2018; Lancelot Miltgen et al. 2013; Morosan, 2012b, 2016; Sharma et al. 2018). This research specifically addresses privacy issues related to FRP systems and their ability to safeguard customer data (Paine et al. 2007). Privacy concerns around FRP can be understood in two main areas. First, there is the fear that biometric data, such as facial patterns, could be misused for identifying and tracking individuals without consent (Akhtar and Rattani, 2017; Ngugi et al. 2011). Second, individuals worry that FRP systems may collect unnecessary or unauthorized data or that their facial images could be used inappropriately (Akhtar and Rattani, 2017; Ngugi et al. 2011). Research shows that privacy concerns are critical to building trust in new technologies. Yousafzai et al. (2009) highlighted the strong connection between perceived security and trust in Internet banking, while Pai et al. (2018) found that privacy concerns with FRP systems in hotels negatively impacted trust in the technology. Thus, the following hypothesis is proposed:
H5. Privacy concerns negatively influence the trust in FRP.
The effect of perceived risks
Perceived risks refer to individuals’ anticipation of negative outcomes when using IT or IS (Lim et al. 2003). These risks can include financial, performance, time, social, psychological, and privacy concerns (Hassan et al. 2006; Crespo et al. 2009). In the context of FRP systems in smart hospitals, perceived risks reflect users’ concerns about privacy, security, economic factors, and system performance. Research shows that perceived risks negatively impact the acceptance of mobile payments (Al-Saedi et al. 2020; Shao et al. 2019; Sharma et al. 2018). For example, Hong et al. (2020) found that performance, financial, and privacy risks are key reasons for resistance to mobile wallets. Similarly, users may avoid FRP systems due to these perceived risks in smart hospitals. Hence, the following hypothesis is posited:
H6. Perceived risks negatively influence trust in FRP.
The effect of familiarity
Familiarity refers to the level of knowledge, understanding, and experience an individual has with a technology (Byungura et al. 2018). In the context of FRP in smart hospitals, it includes users’ awareness of the technology’s functionality, benefits, and limitations (Shiau et al. 2023). Studies show that familiarity positively impacts users’ trust in new technologies (Benlian and Hess, 2011; Hajli et al. 2017). Familiarity fosters comfort and confidence, increasing trust in the technology’s reliability, security, and usability (Li et al. 2008; Casaló et al. 2008; Flavián et al. 2006). In the case of FRP, familiarity helps users better understand how the system works, its security measures, and its reliability (Moradi and Groth, 2019). This knowledge alleviates concerns about privacy and risks, boosting trust (Pavlou, 2003). Additionally, familiarity creates psychological comfort, making users more open to adopting the technology (Shiau et al. 2023). As users perceive FRP to be convenient and user-friendly (Mei et al. 2018), trust in the system grows, as they believe it will meet their needs effectively within smart hospitals (Lee, 2019).
H7. Familiarity positively influences trust in FRP.
The Effect of Trust in FRP
Trust refers to individuals’ confidence in FRP systems to effectively prevent, detect, and mitigate fraud (Morosan, 2020). It is built on perceived reliability, integrity, competence, and benevolence (Escobar-Rodriguez and Carvajal-Trujillo, 2014; McKnight and Chervany, 2001; Liao et al. 2024). Trust plays a crucial role in the decision to adopt and use FRP systems (Ngugi et al. 2011; O’Brien and Marakas, 2007). Studies consistently show a positive relationship between trust in technology and BI to use it (Kim et al. 2011; Zimmer et al. 2010; Yu et al. 2024a). When individuals trust a system, they develop a positive attitude and a stronger intention to use it (Connolly and Bannister, 2007). Trust acts as a mediator, linking system reliability perceptions to BI (Tamilmani et al. 2020). Key factors influencing trust in FRP include system reliability in preventing fraud, integrity in operations (e.g., transparency, ethical practices), and competence (e.g., advanced algorithms) (Lancelot Miltgen et al. 2013; Ngugi et al. 2011; Akhtar and Rattani, 2017). Additionally, the belief that the system protects users’ interests fosters trust and increases the intention to use it. Based on this, the following hypothesis is proposed:
H8. Trust in FRP positively affects the BI to use FRP.
The effect of personal innovativeness
Personal innovativeness refers to consumers’ preference for and interest in new products. Innovators are more willing to take risks and explore new technologies (Agarwal and Prasad, 1998). In IS research, personal innovativeness is used to assess individuals’ readiness to adopt new IT systems, with studies showing that more innovative consumers are quicker to embrace new technologies, including online shopping (Eastlick and Lotz, 1999). Personal innovativeness has been found to positively influence the intention to use services such as WAP in mobile commerce (Hung et al. 2003), and to affect new product adoption behavior (Im et al. 2003; Lian and Lin, 2008). In the context of biometric technology, research across various settings (hotels, airports, ATMs) has demonstrated the direct and indirect effects of personal innovativeness on BI to use technology (Morosan, 2012a, 2012b; Byun and Byun, 2013). Specifically, Morosan (2011) found that personal innovativeness positively influenced perceived ease of use, which in turn affected attitudes and intentions towards biometric technology. Recent meta-analyses confirm that personal innovativeness boosts technology adoption in hospitality and tourism (Ciftci et al. 2021). In smart hospitals, personal innovativeness has been shown to influence BI in areas like green consumption and the adoption of innovative solutions (Lu et al. 2005). Additionally, it has been found to moderate the relationship between trust and BI in various technological contexts (Fang et al. 2009). Thus, it is expected that personal innovativeness will play a similar role in FRP adoption in smart hospitals (Jackson et al. 2013). Therefore, the following hypothesis is proposed: Studies by Morosan (2012a) in hotels, Soh et al. (2010) in mobile applications, Morosan (2012b) in airport security checkpoints, Byun and Byun (2013) in fingerprint recognition for ATM access, and Lancelot Miltgen et al. (2013) in iris recognition for library account access have demonstrated both direct and indirect effects of personal innovativeness on BI. Specifically, Morosan (2011) found that personal innovativeness positively influenced perceived ease of use, which in turn affected attitudes and intentions towards biometric technology. Recent meta-analyses confirm that personal innovativeness boosts technology adoption in hospitality and tourism (Ciftci et al. 2021). In smart hospitals, personal innovativeness has been shown to influence BI in areas like green consumption and the adoption of innovative solutions (Lu et al. 2005). Additionally, it has been found to moderate the relationship between trust and BI in various technological contexts (Fang et al. 2009). Thus, it is expected that personal innovativeness will play a similar role in FRP adoption in smart hospitals (Jackson et al. 2013). Therefore, the following hypothesis is proposed:
H9. Personal innovativeness positively influences the BI to use FRP.
H10. Personal innovativeness positively moderates the relationship between trust in FRP and the BI to use FRP.
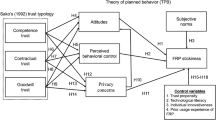
Hence, as presented in Fig. 1, the theoretical framework is introduced.

Determinants of behavioral Intention to use FRP in smart hospitals: drawing from the unified theory of acceptance and use of technology, the diffusion of innovations theory, and trust theory.
Research methodology
Measurement
The measurement items in this study comprised four items each and were adapted from existing research to suit the context of smart hospitals. For PE, modifications were made based on studies by Venkatesh et al. (2003) and Lee and Pan (2023a). Items for EE were drawn from Venkatesh et al. (2003) and Moriuchi (2021). SI and FC were assessed based on adaptations from Venkatesh et al. (2003) and Ciftci et al. (2021). The measurement items for privacy concerns were modified by Ciftci et al. (2021). Perceived risks originated from the study conducted by Liu and Tu (2021). Items for familiarity were drawn from Ouyang et al. (2020) and Shiau et al. (2023). Trust in FRP was assessed based on adaptations from Morosan (2020). Measurement items for personal innovativeness were modified from Zhong et al. (2021). BI to use FRP was drawn from Liu and Tu (2021). All items were rated on a 7-point Likert scale, ranging from “strongly disagree (1)” to “strongly agree (7)”.
To ensure content validity, feedback was obtained from two professors conducting studies on FRP, resulting in adjustments to the questionnaire. Additionally, the back-to-back translation method (Jin and Weber, 2013; Brislin, 1980) was used to validate the measurement items for the smart hospital context. A pilot test involving 50 FRP users was conducted to refine the measurement items and address any potential semantic confusion. Furthermore, a focus group discussion was held with the authors, three FRP service staff in smart hospitals, and several student respondents to further enhance the questionnaire. This optimization process involved clarifying scenarios, redesigning images, adjusting wording, removing irrelevant items, and improving clarity and precision (Zhang et al. 2023). The finalized questionnaire for the formal survey is presented in Table 1.
Data collection and sampling
We conducted a study on the FRP in smart hospitals in China using an online questionnaire distributed through the popular Chinese survey platform Wenjuanxing (https://www.wjx.cn/). To ensure a diverse range of participants, we employed a stratified random distribution approach to reach respondents with varied backgrounds and experiences in using FRP in smart hospitals. To mitigate selection bias, we stratified the population based on key demographic variables such as age, gender, education level, and geographical location. This stratification ensured that our sample would represent a wide array of demographic characteristics. Within each stratum, we randomly selected participants to receive the survey link. This approach enhanced the representativeness of our sample and improved the generalizability of our findings (Fan et al. 2019; Zhou et al. 2022). By stratifying based on age, gender, education level, and geographical location, we aimed to capture a diverse range of participants reflective of the broader population.
The questionnaire consisted of four parts. The introduction provided the research purpose, assured confidentiality, and explained FRP in smart hospitals. The second part included screening questions to determine suitable participants—individuals aged 18 or older residing in China, who are Chinese residents. Eligible participants proceeded to the survey, while others were disqualified. Participants who completed the survey received compensation of RMB5 to RMB10, which would incentivize participation and ensure a higher response rate (Wang et al. 2023). The final part of the survey aimed to collect demographic information from the participants, including gender, age, education level, and monthly income.
To determine an appropriate sample size for hypothesis testing, G*Power 3.1 was used before the survey, taking into account factors such as research complexity, desired statistical significance, effect size, and statistical power (Soper, 2018). Following conventional guidelines with an effect size (f2) of 0.15, α err prob of 0.05, and power (1−β err prob) of 0.95 (Cohen, 1992; Soper, 2018), a minimum of 172 participants was considered necessary. During the period from October 2023 to January 2024, a total of 1479 potential participants accessed the survey. However, only 1056 respondents successfully passed the screening questions and were deemed eligible to proceed to the formal questionnaire. After the screening process, a target sample was selected to complete the formal questionnaire. However, the survey platform identified 245 questionnaires as invalid and removed them from the analysis. Eventually, 811 valid responses remained, which constituted the final sample for the study. For a more detailed explanation and a visual representation of the screening process, please refer to Fig. 2 in the study report. This exceeded the required sample size, ensuring an ample participant pool for analyzing the structural paths in this model (Hair et al. 2016).

A visual representation of the screening process: 811 valid responses.
As shown in Table 2, demographic information from the 811 valid responses revealed a gender distribution of 47.8% male and 52.2% female. The majority of participants (24.9%) fell within the 46–55 age range, indicating active involvement from an older demographic in smart hospitals. A significant portion (27.5%) had a bachelor’s degree, and the income categories of (3001–6000) and (6001–9000) collectively represented 54.2% of the respondents. The demographic profile mirrored previous research on FRP in China (Gao et al. 2023; Hu et al. 2023).
Common method variance
The primary objective of implementing this strategy was to mitigate any potential common method bias (CMB), a concern acknowledged by Zheng et al. (2013). Various measures were taken to address this issue. Prior to data collection, the questionnaire structure was optimized by strategically placing demographic questions in the later sections. This was done to maintain brevity, prioritize the main research inquiries, and alleviate evaluation apprehension by ensuring respondents of their anonymity. Emphasis was placed on communicating that there were no right or wrong answers, thereby encouraging participants to provide genuine responses. To minimize potential bias from question order, the item sequence was counterbalanced, and the questionnaire was designed to be concise to sustain respondent engagement and prevent fatigue or boredom (Lindell and Whitney, 2001). Furthermore, demographic items were intentionally positioned at the end of the questionnaire to mitigate their potential impact on responses to the main construct items.
To address concerns regarding CMB, two approaches were employed. Firstly, Harman’s (1976) single-factor test was conducted, which revealed that no distinct factor beyond the primary factor accounted for more than 28.528% of the variance, falling below the 50% threshold recommended by Hair (2009) and Podsakoff et al. (2003). This indicates that CMB is not a significant concern. Secondly, to further address potential CMB, confirmatory factor analysis (CFA) using the marker technique was employed. Four items measuring perceptions of consequences for arriving late at work were used as marker variables, which are conceptually distinct from the primary study variables. The analysis found no significant associations between the marker variable and the other variables under investigation, supporting the conclusion that CMB in this study is acceptable and does not pose a significant threat to the validity of the results.
Data analysis and results
The data analysis for our study was performed using SmartPLS 4.0, which utilizes partial least-squares structural equation modeling (PLS-SEM). The decision to use PLS-SEM was based on several factors. Firstly, PLS-SEM is commonly employed in exploratory research, which is consistent with the nature of our study (Hair et al. 2021). Furthermore, considering that our data did not follow a normal distribution, PLS-SEM was deemed more appropriate (Hair et al. 2021), as it provides enhanced statistical power regardless of the data distribution.
Measurement model
The measurement model was evaluated by examining the reliability and validity of the constructs, as presented in Table 3. The reliability of the indicators was carefully assessed through factor loadings, and all factor loadings exceeded the commonly accepted threshold of 0.7. Additionally, all constructs demonstrated satisfactory Cronbach’s α scores, surpassing the desirable threshold of 0.7, as proposed by Fornell and Larcker (1981). The Cronbach’s α values for each factor ranged from 0.731 to 0.895, consistently surpassing the recommended threshold. Composite Reliability (CR) scores for each construct also exceeded the threshold of 0.7, further confirming the high reliability of the data. The CR values ranged from 0.832 to 0.927, providing additional evidence of reliability. Convergent validity was assessed using average variance extracted (AVE), and all AVE values ranged from 0.554 to 0.760, surpassing the recommended criterion of 0.5 (Fornell and Larcker, 1981). This confirms the convergent validity of the measures.
Discriminant validity was evaluated by examining the correlations between constructs in relation to the square root of the AVE for each factor, as presented in Table 4. The results indicated that the square root of the AVE values for all constructs exceeded the corresponding correlation coefficients, demonstrating robust discriminant validity in line with the criteria established by Fornell and Larcker (1981). Additionally, we assessed discriminant validity using the heterotrait–monotrait (HTMT) ratio. In our study, the highest HTMT ratio was 0.797, which is below the stringent criterion of 0.85 recommended by Henseler et al. (2015) and Kline (2023). This confirms the satisfactory discriminant validity among the constructs.
Structural model
After conducting the analysis of the measurement model, the structural model was examined using SmartPLS 4.0. The purpose of this evaluation was to validate the significance and relevance of relationships among variables and measure the extent of explained variance. The assessment of the structural model followed established practices and guidelines specific to this study (Maroufkhani et al. 2022). This process involved several critical steps, including evaluating collinearity concerns within the structural model, assessing the significance and relevance of correlations, and determining the coefficient of determination (R2). In accordance with Hair Jr et al. (2017), R2 values of 0.75, 0.50, and 0.25 are considered indicative of significant, moderate, and poor relationships, respectively. Additionally, effect sizes were measured using f2 values, as suggested by Jacob (1988). Small, moderate, and large effects are represented by f2 values of 0.02, 0.15, and 0.35, respectively. The effect sizes are presented in Table 5 accordingly.
To address potential collinearity issues that could lead to an overestimation of path coefficients, the study examined the variance inflation factor (VIF) values between constructs. The VIF values for formative constructs were all below the recommended threshold of 3.3, ranging from 1.085 to 1.982, indicating the absence of significant collinearity issues in the data (Hair et al. 2020).
Following the analysis of the structural model, the hypothesized relationships in the theoretical model were examined using bootstrapping with 5000 samples. The results indicated that factors related to UTAUT, DOT, and trust theory were significant in the context of FRP in smart hospitals in China. PE (β = 0.134, t = 5.095, p < 0.001), EE (β = 0.156, t = 4.017, p < 0.001), SI (β = 0.198, t = 5.407, p < 0.001) and FC (β = 0.198, t = 5.241, p < 0.001) positively influenced BI to use FRP. These results support H1–H4, indicating the significance of antecedents of UTAUT in shaping BI to use FRP in smart hospitals in China. Besides, in terms of trust in FRP, privacy concerns (β = −0.279, t = 7.827, p < 0.001) and perceived risks (β = −0.121, t = 3.461, p < 0.01) negatively influenced it. Familiarity (β = 0.273, t = 7.603, p < 0.001) positively influenced trust in FRP. These findings support H5–H7, indicating the factors influencing trust in FRP are significant. Furthermore, trust in FRP (β = 0.168, t = 4.913, p < 0.001), and personal innovativeness (β = 0.100, t = 2.814, p < 0.01) positively influenced BI to use FRP. H8 and H9 are both supported. This suggests that trust in FRP and personal innovativeness play a crucial role in influencing BI to use FRP in smart hospitals. Finally, personal innovativeness positively moderated the relationship between trust in FRP and BI to use FRP (H10; β = 0.076, t = 2.654, p < 0.01), indicating that individuals who have a higher level of personal innovativeness are more likely to translate their trust in FRP into a stronger intention to use FRP. Personal innovativeness acts as a moderator that amplifies the positive influence of trust in FRP on the BI to use FRP. The results are visually presented in Fig. 3. As for the mediation effect, to examine the mediation effect of trust in FRP, we employed the bootstrap method with 5000 resamples. We calculated 95% bias-corrected confidence intervals (BC-CI) to assess the significance of the mediation effects, following the approach outlined by Gao et al. (2023). The results of the mediation effect, as presented in Table 6 are all supported. The mediation effect of information vulnerability on FRP continuance usage intention through fear of financial losses was found to be negative and significant. Specifically, the indirect effect of privacy concerns on BI to use FRP mediated by trust in FRP had a mediation value of −0.047 (95% BC-CI: [−0.070, −0.026]). Similarly, the mediation effect of perceived risks on BI to use FRP through trust in FRP was also significant and negative with a mediation value of −0.020 (95% BC-CI: [−0.035, −0.008]). Conversely, the mediation effect of familiarity on BI to use FRP through trust in FRP was significant and positive with a mediation value of 0.046 (95% BC-CI: [0.025, 0.070]).

Structural model results: path coefficients and R2 for and trust in FRP and behavioural intention to use FRP. *P < 0.05, **P < 0.01 and ***P < 0.001.
The model explained 26.8% of the variance in trust in FRP and 53.0% of the variance in BI to use FRP. To assess the model’s predictive ability, a blindfold analysis was conducted, yielding predictive relevance (Q2) values for dependent variables. The Q2 values for trust in FRP and BI to use FRP were 0.174 and 0.288, respectively, surpassing the specific thresholds of 0.15 and 0.35, respectively, demonstrating the model’s effective predictive capability (Hair et al. 2012). The model’s goodness of fit was evaluated using the standardized root mean square residual (SRMR), which had a value of 0.048, meeting the commonly accepted criteria (SRMR < 0.100), indicating a well-fitted model (Hu and Bentler, 1999).
Multi-group analysis
To examine whether significant differences exist between groups with varying demographic characteristics, we conducted a multi-group analysis (MGA) using PLS-SEM. Previous research on gender has similarly considered demographic factors, revealing notable differences in gender among different groups (Si et al. 2022). In our survey, the subsamples for gender, age, educational level, and monthly income do not satisfy the sample size difference requirement, as each group’s sample size is less than half that of the other group (Hair et al. 2016). However, the subsamples for gender have adequate sizes to fulfill the MGA sample size difference criteria. The detailed analysis is as follows.
Before conducting the analysis, it was essential to establish measurement invariance using the measurement invariance of composite models (MICOM) approach recommended by Henseler et al. (2016). The MICOM approach involves several steps. In the first step, known as configural invariance, variables were equally modeled and evaluated in both groups to establish their equivalence (Rodríguez Torrico et al. 2020). This step ensures that the same measurement model can be applied to the gender group. The second step focused on compositional invariance, which examines whether the correlation c-value meets the requirement for compositional invariance. The results in Table 7 indicated that the correlation c-value satisfied the criteria for compositional invariance. This suggests that the relationships between variables in the measurement model are comparable across the different genders. The third step involved assessing composite equality. This step aims to determine if the mean original difference and variance original difference fall within specific confidence intervals (Matthews, 2017). Depending on whether both, one, or neither value falls within the interval, constructs demonstrate full, partial, or no invariance, respectively. For the gender group, partial invariance was confirmed for PE, FC, and BI to use FRP. This indicates that there are both similarities and differences between males and females in terms of these constructs. It suggests that PE, FC, and BI to use FRP may vary to some extent depending on the different gender.
After establishing measurement invariance, the study employed PLS-MGA to explore the differential influence of gender. Nonparametric methods, including Henseler’s MGA (Henseler et al. 2009) and the permutation test (Chin and Dibbern, 2010), were utilized in the analysis. The consistency between the two MGA analysis methods further enhances the credibility of the outcomes through a multi-method approach (Pérez-Macías et al. 2021; Yang et al. 2022). This comprehensive approach contributes to the robust validation of the study’s findings. Henseler’s MGA compared group-specific bootstrap estimates and considered p-values below 0.05 or above 0.95 as indicating significant differences between path coefficients across different genders (Henseler et al. 2009). The permutation test also yielded p-values, with differences considered significant at the 5% level if the p-value was below 0.05. The results presented in Table 8, indicated non-significant differences between males and females for all hypotheses, including the moderator interaction. This suggests that gender (male or female) does not significantly influence the relationships and path coefficients in the model. However, slight variations between the results of the permutation test and Henseler’s MGA were observed, specifically for the influence of privacy concerns on trust in FRP (H5).
Discussion
FRP has been examined in different contexts, including retail stores (Dang et al. 2022), hotels (Morosan, 2020), and the restaurant industry (Hwang et al. 2024). However, it has not been examined in the smart hospital context. To fill in the gap, this study aims to investigate the impact of original antecedents on BI to use FRP in smart hospitals, drawing from the UTAUT, DOI, and trust theory. The findings of the study shed light on critical aspects of FRP in the context of smart hospitals.
Firstly, the antecedents of UTAUT were found to be significant in influencing BI to use FRP. Specifically, PE, EE, SI, and FC all positively influenced users’ intention to use FRP. These results support H1–H4 and suggest that factors related to UTAUT play a crucial role in shaping users’ BI to engage with FRP in smart hospitals, which aligns with the previous research (Alkhowaiter, 2022; D. Liu and Tu, 2021). Secondly, trust in FRP was found to be influenced by privacy concerns, perceived risks, and familiarity. Privacy concerns and perceived risks negatively affected trust in FRP, while familiarity positively influenced it. These findings support H5-H7, indicating that the factors influencing trust in FRP are significant and should be considered when designing and implementing FRP in healthcare settings. These findings are in line with the prior research which has indicated that privacy concerns and perceived risks can significantly impact users’ trust in technology (Gurung and Raja, 2016). Privacy concerns arise from the potential misuse of personal data and unauthorized access, leading individuals to question the security and confidentiality of their information in the context of FRP (Liu et al. 2021). Similarly, perceived risks associated with FRP, such as the possibility of identity theft or financial fraud, can erode users’ trust in the system. On the other hand, familiarity with FRP positively influences users’ trust. When individuals have prior experience or exposure to FRP systems, they may have a better understanding of how the technology works and feel more comfortable using it (Palash et al. 2022). Familiarity builds confidence and trust in the system’s reliability and security, increasing users’ willingness to embrace FRP in healthcare settings (Liu et al. 2022). Furthermore, both trust in FRP and personal innovativeness positively influenced users’ BI to use FRP. This suggests that trust in FRP and personal innovativeness play crucial roles in shaping users’ intention to engage with FRP in smart hospitals. These findings support H8 and H9, emphasizing the importance of trust and personal innovativeness in driving users’ adoption and continued usage of FRP. This supports the view that establishing trust in FRP systems and catering to users’ personal innovativeness are essential strategies for promoting the BI to use FRP in smart hospitals (Palash et al. 2022). Additionally, personal innovativeness was found to act as a positive moderator in the relationship between trust in FRP and BI to use FRP. Individuals with a higher level of personal innovativeness are more likely to translate their trust in FRP into a stronger intention to use FRP. This finding supports H10 and suggests that personal innovativeness amplifies the positive influence of trust in FRP on users’ BI, as shown in Fig. 4. The results confirmed the moderating role of personal innovativeness. These findings are in line with prior research (Palash et al. 2022), which has indicated that personal innovativeness can act as a positive moderator in various technology adoption contexts. Personal innovativeness enhances individuals’ willingness to adopt and use new technologies, making them more open to embracing innovative solutions (Lu et al. 2005).

The moderating effect of personal innovativeness on the relationship between trust in FRP and behavioral intention.
The mediation analysis focused on the role of trust in FRP in mediating the relationship between information vulnerability and FRP continuance usage intention. The results revealed significant mediation effects. Privacy concerns and perceived risks negatively influenced BI to use FRP, mediated by trust in FRP. Conversely, familiarity positively influenced BI to use FRP, also mediated by trust in FRP. These findings provide further support for the significance of trust in FRP and its role as a mediator in the relationship between information vulnerability and users’ intention to engage with FRP. These findings are in line with the prior research which has indicated that familiarity with a technology positively influences users’ BI to adopt and use it (Lu et al. 2011). Familiarity, in the context of FRP in smart hospitals, refers to users’ prior exposure, experience, or knowledge of FRP systems (Shiau et al. 2023). When individuals are familiar with FRP and have a certain level of understanding and comfort with the technology, they are more likely to develop a positive attitude and intention to engage with it.
The results of the analysis comparing the influence of gender (male or female) on the relationships and path coefficients in the model revealed non-significant differences. This implies that gender does not significantly impact the relationships between the variables and the path coefficients in the model. The lack of significant differences between males and females suggests that the factors influencing users’ BI to use FRP in smart hospitals are similar for both genders. These findings indicate that the theoretical model holds true for both males and females, and the relationships between the variables are consistent across genders. This implies that the factors related to UTAUT, trust theory, and personal innovativeness, as well as their influence on BI to use FRP, are equally valid for both males and females in the context of smart hospitals in China. Furthermore, it is worth noting that slight variations were observed between the results of the permutation test and Henseler’s MGA for the influence of privacy concerns on trust in FRP (H5). Although the overall conclusion of non-significant differences between males and females remains the same, these variations suggest some differences in the specific effects of privacy concerns on trust in FRP between genders, as shown in Figs. 5 and 6.

Structural model results: path coefficients and R2 for and trust in FRP and behavioural intention to use FRP for 388 men.

Structural model results: path coefficients and R2 for and trust in FRP and behavioural intention to use FRP for 423 women.
Implications
Theoretical implications
The theoretical implications of the findings on FRP adoption in smart hospitals can be understood from several perspectives, particularly through the extension of UTAUT, trust theory, and DOI theory. Firstly, the significant influence of UTAUT antecedents (PE, EE, SI, and FC) on users’ BI to use FRP supports the applicability of the UTAUT framework in understanding FRP adoption in healthcare. This suggests that these factors should be considered when designing and implementing FRP systems in smart hospitals, thus broadening the application of UTAUT beyond its previous domains (Lee and Pan, 2023a; Palash et al. 2022; Li et al. 2018). Addressing these factors can enhance users’ acceptance and intention to use FRP in healthcare settings. Secondly, the study highlights the importance of trust in the acceptance and adoption of FRP in smart hospitals. Trust-related factors significantly influence users’ intention to use FRP, with privacy concerns and perceived risks negatively affecting trust, while familiarity with FRP positively influences it. These findings underscore the need for healthcare organizations to address privacy concerns and perceived risks to build trust in FRP (Nan et al. 2022). Efforts to increase familiarity with FRP can further enhance trust and users’ intention to adopt these technologies. Additionally, the study reveals that trust in FRP and personal innovativeness significantly impact users’ BI to use FRP. Trust in FRP enhances users’ intention to engage with the technology, and personal innovativeness amplifies this positive effect. This suggests that healthcare organizations should focus on building trust and targeting individuals with higher levels of personal innovativeness to promote FRP adoption in smart hospitals. Moreover, the study identifies trust as a crucial mediator in the relationship between information vulnerability and users’ intention to engage with FRP. Privacy concerns and perceived risks negatively influence users’ intention, mediated by trust, while familiarity positively influences intention, also mediated by trust (Liao et al. 2022). This highlights the importance of trust in mitigating concerns and facilitating the acceptance of FRP in healthcare settings. Finally, the study finds no significant gender differences in the factors influencing users’ BI to use FRP. This indicates that a gender-neutral approach can be adopted when designing and implementing FRP systems in smart hospitals, as the underlying factors and their influences are consistent for both males and females.
Practical implications
The practical implications in the context of FRP in smart hospitals can be derived from several perspectives. Firstly, the significant influence of UTAUT antecedents on users’ BI to use FRP suggests that healthcare organizations should focus on addressing factors such as PE, EE, SI, and FC. By enhancing these factors, healthcare organizations can increase users’ acceptance and intention to engage with FRP. This can be achieved through providing clear information about the performance benefits of FRP, ensuring that the technology is easy to use and understand, leveraging SI through training and support programs, and creating a supportive environment for FRP implementation. Secondly, the findings regarding the influence of trust-related factors on users’ intention to use FRP highlight the importance of building trust in FRP systems. Healthcare organizations should address privacy concerns and perceived risks associated with FRP by implementing robust privacy and security measures, transparently communicating data handling practices, and providing clear information about the benefits and risks of FRP (Cheng et al. 2022). Leveraging fintech trust signals within the UX design can reinforce credibility and trustworthiness. Displaying certifications, user testimonials, third-party reviews, and case studies can provide tangible proof of the system’s reliability and effectiveness. Transparent communication about pricing and the benefits of using the FRP system can further enhance trust. By clearly explaining the total cost, including functionalities, and any associated fees, users can make informed decisions without the fear of hidden costs. Highlighting the system’s unique advantages, such as time savings and improved outcomes, can demonstrate its value and encourage user adoption. Incorporating these trust-building elements into the UX design ensures that the FRP system addresses user concerns comprehensively, fostering a trustworthy and user-friendly experience. Besides, efforts should be made to familiarize users with FRP by providing training, education, and opportunities for hands-on experience. By building trust and familiarity, healthcare organizations can increase users’ intention to engage with FRP in smart hospitals. Moreover, the positive influence of trust in FRP and personal innovativeness on users’ BI to use FRP underscores the need to cultivate trust and target individuals with higher levels of personal innovativeness. Healthcare organizations should focus on establishing trust in FRP by fostering open communication, providing reliable and accurate information, and demonstrating transparency in the use of FRP. Furthermore, identifying and targeting individuals with a higher propensity for innovation can help drive FRP adoption. Healthcare organizations can engage these individuals as early adopters, opinion leaders, and advocates, thereby promoting FRP adoption among a broader user base. Additionally, the identified mediation effects of trust in FRP in the relationship between information vulnerability and users’ intention to engage with FRP highlight the role of trust as a mediator in mitigating concerns and facilitating FRP adoption. Healthcare organizations should prioritize efforts to build trust in FRP by addressing privacy concerns, minimizing perceived risks, and promoting familiarity. By doing so, they can enhance users’ intention to engage with FRP and encourage continued usage. Finally, the non-significant differences in the influence of gender on the relationships and path coefficients suggest that healthcare organizations can adopt a gender-neutral approach when designing and implementing FRP systems in smart hospitals. The underlying factors influencing users’ BI to use FRP are similar for both males and females. Therefore, healthcare organizations should focus on understanding and addressing the common factors affecting FRP adoption, rather than tailoring strategies specifically for each gender. This approach ensures that the theoretical model and its practical implications remain applicable and consistent across genders.
Limitations and directions for future work
While this study offers valuable insights into FRP adoption in smart hospitals in China, several limitations must be acknowledged. First, the focus on Chinese smart hospitals may limit the generalizability of findings to other healthcare settings or cultural contexts. Future research should replicate this study in diverse countries and healthcare systems to validate the results. Second, the cross-sectional design restricts the ability to establish causal relationships. A longitudinal approach could track changes in BI and actual FRP usage over time. Third, the reliance on self-reported data may introduce biases like common methods and social desirability. Future studies could address this by incorporating objective measures or observing actual usage behavior. The sample, drawn from specific hospitals, may not fully represent the broader population. Expanding sample size and diversity would enhance generalizability. Additionally, combining quantitative findings with qualitative methods, such as interviews or focus groups, could provide deeper insights into users’ perceptions and experiences with FRP. Qualitative research could explore the motivations, barriers, and facilitators of FRP adoption in greater detail. Future work should also integrate user-centered design principles to align FRP systems with users’ needs and usability requirements. Comparative studies between FRP and traditional systems would offer insights into FRP’s relative advantages. Given the sensitive nature of personal health data, future research must also explore the ethical and legal implications of FRP adoption, including privacy, security, and regulatory compliance. Investigating the factors influencing adoption across different user groups, such as healthcare professionals, patients, and caregivers, would help tailor strategies to promote acceptance. Addressing these limitations will contribute to more effective implementation and use of FRP technologies in healthcare.
Conclusion
This study examined the factors influencing the BI to use FRP in smart hospitals, drawing from theories such as UTAUT, DOI, and trust theory. The findings revealed that factors such as PE, EE, SI, and FC significantly influenced users’ intention to use FRP. Additionally, trust-related factors, including privacy concerns, perceived risks, and familiarity, were found to influence users’ trust in FRP. Trust in FRP and personal innovativeness were identified as significant predictors of users’ intention to use FRP, with personal innovativeness moderating the relationship between trust and intention. Furthermore, the study found that trust in FRP mediated the relationship between information vulnerability and users’ intention to engage with FRP. The study also highlighted the gender-neutral nature of the factors influencing FRP adoption, suggesting that healthcare organizations should adopt a gender-neutral approach when designing and implementing FRP systems. The practical implications of the study suggest that healthcare organizations should focus on addressing UTAUT antecedents, building trust in FRP, targeting individuals with higher personal innovativeness, and maintaining a gender-neutral approach to encourage FRP adoption. By implementing these strategies, healthcare organizations can enhance the acceptance and trust in FRP systems, leading to more efficient payment processes, reduced administrative burdens on healthcare staff, and increased patient satisfaction. Consequently, these improvements contribute to better health outcomes in smart hospital environments, as patients experience quicker access to necessary treatments and overall higher quality of care.
Data availability
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
References
Abdulkareem KH, Mohammed MA, Salim A, Arif M, Geman O, Gupta D, Khanna A (2021) Realizing an effective COVID-19 diagnosis system based on machine learning and IOT in smart hospital environment. IEEE Internet Things J 8(21):15919–15928. https://doi.org/10.1109/JIOT.2021.3050775
Agarwal R, Prasad J (1998) A conceptual and operational definition of personal innovativeness in the domain of information technology. Inf Syst Res 9(2):204–215. https://doi.org/10.1287/isre.9.2.204
Agarwal R, Prasad J (1997) The role of innovation characteristics and perceived voluntariness in the acceptance of information technologies. Decis Sci 28(3):557–582. https://doi.org/10.1111/j.1540-5915.1997.tb01322.x
Ajzen I (1985) From Intentions to Actions: A Theory of Planned Behavior. In: Kuhl J, Beckmann J (eds) Action Control. SSSP Springer Series in Social Psychology. Springer, Berlin, Heidelberg. pp. 11–39, https://doi.org/10.1007/978-3-642-69746-3_2
Akhtar Z, Rattani A (2017) A face in any form: new challenges and opportunities for FR technology. Computer 50(4):80–90. https://doi.org/10.1109/MC.2017.119
Akinnuwesi BA, Uzoka FME, Fashoto SG, Mbunge E, Odumabo A, Amusa OO, Owolabi O (2022) A modified UTAUT model for the acceptance and use of digital technology for tackling COVID-19. Sustain Oper Comput 3:118–135. https://doi.org/10.1016/j.susoc.2021.12.001
Akinnuwesi BA, Uzoka FME, Okwundu OS, Fashoto G (2016) Exploring biometric technology adoption in a developing country context using the modified UTAUT. Int J Bus Inf Syst 23(4):482–521. https://doi.org/10.1504/IJBIS.2016.080219
Alkhowaiter WA (2022) Use and behavioural intention of m-payment in GCC countries: extending meta-UTAUT with trust and Islamic religiosity. J Innov Knowl 7(4):100240. https://doi.org/10.1016/j.jik.2022.100240
Al-Okaily M, Lutfi A, Alsaad A, Taamneh A, Alsyouf A (2020) The determinants of digital payment systems’ acceptance under cultural orientation differences: the case of uncertainty avoidance. Technol Soc 63:101367. https://doi.org/10.1016/j.techsoc.2020.101367
Al-Saedi K, Al-Emran M, Ramayah T, Abusham E (2020) Developing a general extended UTAUT model for M-payment adoption. Technol Soc 62:101293. https://doi.org/10.1016/j.techsoc.2020.101293
Alzahrani L, Al-Karaghouli W, Weerakkody V (2017) Analysing the critical factors influencing trust in e-government adoption from citizens’ perspective: a systematic review and a conceptual framework. Int Bus Rev 26(1):164–175. https://doi.org/10.1016/j.ibusrev.2016.06.004
Benlian A, Hess T (2011) The signaling role of IT features in influencing trust and participation in online communities. Int J Electron Commer 15(4):7–56. https://doi.org/10.2753/JEC1086-4415150401
Breward M, Hassanein K, Head M (2017) Understanding consumers’ attitudes toward controversial information technologies: a contextualization approach. Inf Syst Res 28(4):760–774. https://doi.org/10.1287/isre.2017.0706.230
Brislin RW (1980) Translation and content analysis of oral and written materials. In: Triandis InHC, Berry JW (Eds.) Handbook of cross-cultural psychology, vol. 2. Methodology. Allyn & Bacon, Boston, pp. 389–444
Brown SA, Dennis AR, Venkatesh V (2010) Predicting collaboration technology use: integrating technology adoption and collaboration research. J Manag Inf Syst 27:9–54. https://doi.org/10.2753/MIS0742-1222270201
Byun S, Byun S-E (2013) Exploring perceptions toward biometric technology in service encounters: a comparison of current users and potential adopters. Behav Inf Technol 32(3):217–230. https://doi.org/10.1080/0144929X.2011.553741
Byungura JC, Hansson H, Muparasi M, Ruhinda B (2018) Familiarity with technology among first‑year students in Rwandan tertiary education. Electron J e-Learn 16(1):30–45
Casaló L, Flavián C, Guinalíu M (2008) The role of perceived usability, reputation, satisfaction and consumer familiarity on the website loyalty formation process. Comput Hum Behav 24(2):325–345. https://doi.org/10.1016/j.chb.2007.01.017
Cavoukian A (2008) Privacy in the clouds. Identity Inf Soc 1(1):89–108. https://doi.org/10.1007/s12394-008-0005-z
Chen SC, Dhillon GS (2003) Interpreting dimensions of consumer trust in e-commerce. Inf Technol Manag 4:303–318. https://doi.org/10.1023/A:1022962631249
Cheng X, Qiao L, Yang B, Zhang X (2022) Investigation on users’ resistance intention to facial recognition payment: a perspective of privacy. Electron Commer Res. https://doi.org/10.1007/s10660-022-09588-y
Chin WW, Dibbern J (2010) An introduction to a permutation based procedure for multi-group PLS analysis: results of tests of differences on simulated data and a cross cultural analysis of the sourcing of information system services between Germany and the USA. V. Esposito Vinzi, W. W
Chiu C-M, Wang ET (2008) Understanding Web-based learning continuance intention: the role of subjective task value. Inf Manag 45:194–201. https://doi.org/10.1016/j.im.2008.02.003
Cho Y, Hwang J, Lee D (2012) Identification of effective opinion leaders in the diffusion of technological innovation: a social network approach. Technol Forecast Soc Change 79(1):97–106. https://doi.org/10.1016/j.techfore.2011.06.003
Ciftci O, Choi EKC, Berezina K (2021) Let’s face it: are customers ready for facial recognition technology at quick-service restaurants? Int J Hosp Manag 95:102941. https://doi.org/10.1016/j.ijhm.2021.102941
Cohen J (1992) Quantitative methods in psychology: a power primer. Psychol Bull 112:1155–1159
Compeau DR, Higgins CA (1995) Computer self-efficacy: development of a measure and initial test. MIS Q 189–211. https://doi.org/10.2307/249688
Connolly R, Bannister F (2007) Consumer trust in internet shopping in Ireland: towards the development of a more effective trust measurement instrument. J Inf Technol 22(2):102–118. https://doi.org/10.1057/palgrave.jit.2000071
Corbitt BJ, Thanasankit T, Yi H (2003) Trust and e-commerce: a study of consumer perceptions. Electron Commer Res Appl 2(3):203–215. https://doi.org/10.1016/S1567-4223(03)00024-3
Crespo ÁH, Del Bosque IR, de los Salmones Sánchez MG (2009) The influence of perceived risk on Internet shopping behavior: a multidimensional perspective. J Risk Res. 12(2):259–277. https://doi.org/10.1080/13669870802497744
Cresswell K, Sheikh A (2013) Organizational issues in the implementation and adoption of health information technology innovations: an interpretative review. Int J Med Inform 82(5):e73–e86. https://doi.org/10.1016/j.ijmedinf.2012.10.007
Dale V, McEwan M, Bohan J (2021) Early adopters versus the majority: characteristics and implications for academic development and institutional change. J Perspect Appl Acad Pract 9(2):54–67. https://doi.org/10.14297/jpaap.v9i2.483
Dang VT, Nguyen N, Nguyen HV, Nguyen H, Van Huy L, Tran VT, Nguyen TH (2022) Consumer attitudes toward facial recognition payment: an examination of antecedents and outcomes. Int J Bank Mark 40(3):511–535. https://doi.org/10.1108/IJBM-04-2021-0135
Davis FD, Bagozzi RP, Warshaw PR (1992) Extrinsic and intrinsic motivation to use computers in the workplace 1. J Appl Soc Psychol 22(14):1111–1132. https://doi.org/10.1111/j.1559-1816.1992.tb00945.x
Del Rio JS, Moctezuma D, Conde C, de Diego IM, Cabello E (2016) Automated border control e-gates and facial recognition systems. Comput Secur 62:49–72. https://doi.org/10.1016/j.cose.2016.07.001
Eastlick MA, Lotz S (1999) Profiling potential adopters and non‐adopters of an interactive electronic shopping medium. Int J Retail Distrib Manag https://doi.org/10.1108/09590559910278560
Escobar-Rodriguez T, Carvajal-Trujillo E (2014) Online purchasing tickets for low cost carriers: an application of the unified theory of acceptance and use of technology (UTAUT) model. Tour Manag 43:70–88. https://doi.org/10.1016/j.tourman.2014.01.017
Fan J, Zhou W, Yang X, Li B, Xiang Y (2019) Impact of social support and presence on swift guanxi and trust in social commerce. Ind Manag Data Syst 119(9):2033–2054. https://doi.org/10.1108/imds-05-2019-0293
Fang J, Shao P, Lan G (2009) Effects of innovativeness and trust on web survey participation. Comput Hum Behav 25(1):144–152. https://doi.org/10.1016/j.chb.2008.08.002
Flavián C, Guinalíu M, Gurrea R (2006) The influence of familiarity and usability on loyalty to online journalistic services: the role of user experience. J Retail Consum Serv 13(5):363–375. https://doi.org/10.1016/j.jretconser.2005.11.003
Fornell C, Larcker DF (1981) Evaluating structural equation models with unobservable variables and measurement error. J Mark Res 18(1):39–50. https://doi.org/10.1177/002224378101800104
Gao W, Guo Q, Jiang N (2023) Information vulnerability in facial recognition payment: an explanation of technology threat avoidance and information boundary theory. Electron Commer Res Appl 61:101298. https://doi.org/10.1016/j.elerap.2023.101298
Giustiniano L, Bolici F (2012) Organizational trust in a networked world: analysis of the interplay between social factors and Information and Communication Technology. J Inf Commun Ethics Soc 10(3):187–202. https://doi.org/10.1108/14779961211261076
Gong X, Zhang KZK, Chen C, Cheung CMK, Lee MKO (2019) What drives self-disclosure in mobile payment applications? The effect of privacy assurance approaches, network externality, and technology complementarity. Inf Technol People 33(4):1174–1213. https://doi.org/10.1108/ITP-03-2018-0132
Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O (2004) Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q 82(4):581–629. https://doi.org/10.1111/j.0887-378X.2004.00325.x
Gurung A, Raja MK (2016) Online privacy and security concerns of consumers. Inf Comput Secur 24(4):348–371. https://doi.org/10.1108/ICS-05-2015-0020
Hair Jr JF, Howard MC, Nitzl C (2020) Assessing measurement model quality in PLS-SEM using confirmatory composite analysis. J Bus Res. 109:101–110. https://doi.org/10.1016/j.jbusres.2019.11.069
Hair Jr J, Hult F, GTM R, Sarstedt M (2017) A primer on partial least squares structural equation modeling (PLS-SEM), 2nd edn. Sage Publications, Thousand Oaks
Hair JF (2009) Multivariate data analysis. Exploratory factor analysis
Hair JF, Hult GTM, Ringle C, Sarstedt M (2016) A primer on partial least squares structural equation modeling (PLS-SEM). SAGE Publications
Hair JF, Sarstedt M, Ringle CM, Mena JA (2012) An assessment of the use of partial least squares structural equation modeling in marketing research. J Acad Mark Sci 40(3):414–433. https://doi.org/10.1007/s11747-011-0261-6
Hair JF, Hult GTM, Ringle CM, Sarstedt M (2021) A primer on partial least squares structural equation modeling (PLS-SEM), 3rd edn. Sage Publications, Thousand Oaks, CA
Hajli N, Sims J, Zadeh AH, Richard MO (2017) A social commerce investigation of the role of trust in a social networking site on purchase intentions. J Bus Res 71:133–141. https://doi.org/10.1016/j.jbusres.2016.10.004
Harman HH (1976) Modern factor analysis. University of Chicago press
Hassan AM, Kunz MB, Pearson AW, Mohamed FA (2006) Conceptualization and measurement of perceived risk in online shopping. Mark Manag J 16(1):138–147
Heimo OI, Hakkala A, Kimppa KK (2012) How to abuse biometric passport systems. J Inf, Commun Ethics Soc 10(2):68–81. https://doi.org/10.1108/14779961211226985
Henseler J, Ringle CM, Sarstedt M (2016) Testing measurement invariance of composites using partial least squares. Int Mark Rev 33(3):405–431. https://doi.org/10.1108/IMR-09-2014-0304
Henseler J, Ringle CM, Sinkovics RR (2009) The use of partial least squares path modeling in international marketing. In: Sinkovics RR, Ghauri PN (eds) New challenges to international marketing, vol 20. Emerald Group Publishing Limited, pp. 277–319
Henseler J, Ringle CM, Sarstedt M (2015) A new criterion for assessing discriminant validity in variance-based structural equation modeling. J Acad Mark Sci 43(1):115–135. https://doi.org/10.1007/s11747-014-0403-8
Hernandez-Ortega B (2011) The role of post-use trust in the acceptance of a technology: drivers and consequences. Technovation 31(10-11):523–538. https://doi.org/10.1016/j.technovation.2011.07.001
Ho LH, Hung CL, Chen HC (2013) Using theoretical models to examine the acceptance behavior of mobile phone messaging to enhance parent–teacher interactions. Comput Educ 61:105–114. https://doi.org/10.1016/j.compedu.2012.09.009
Hong A, Nam C, Kim S (2020) What will be the possible barriers to consumers’ adoption of smart home services? Telecommun Policy 44(2):101867. https://doi.org/10.1016/j.telpol.2019.101867
Hsieh JK, Li HT (2021) Exploring the fit between mobile application service and application privacy. J Serv Mark https://doi.org/10.1108/JSM-01-2021-0023
Hu B, Liu Y, Yan W (2023) Should I scan my face? The influence of perceived value and trust on Chinese users’ intention to use facial recognition payment. Telemat Inform 78:101951. https://doi.org/10.1016/j.tele.2023.101951
Hu LT, Bentler PM (1999) Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model 6(1):1–55. https://doi.org/10.1080/10705519909540118
Hung SY, Chang CM, Yu TJ (2006) Determinants of user acceptance of the e-Government services: the case of online tax filing and payment system. Gov Inf Q 23(1):97–122. https://doi.org/10.1016/j.giq.2005.11.005
Hung SY, Ku CY, Chang CM (2003) Critical factors of WAP services adoption: an empirical study. Electron Commer Res Appl 2(1):42–60. https://doi.org/10.1016/S1567-4223(03)00008-5
Hwang J, Kim JS, Kim HM, Kim JJ (2024) Effects of motivated consumer innovativeness on facial recognition payment adoption in the restaurant industry: a cross-cultural study. Int J Hosp Manag 117:103646. https://doi.org/10.1016/j.ijhm.2023.103646
Im S, Bayus BL, Mason CH (2003) An empirical study of innate consumer innovativeness, personal characteristics, and new-product adoption behavior. J Acad Mark Sci 31(1):61–73. https://doi.org/10.1177/0092070302238602
Jackson JD, Mun YY, Park JS (2013) An empirical test of three mediation models for the relationship between personal innovativeness and user acceptance of technology. Inf Manag 50(4):154–161. https://doi.org/10.1016/j.im.2013.02.006
Jacob C (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Taylor & Francis Inc
Jin X, Weber K (2013) Developing and testing a model of exhibition brand preference: the exhibitors’ perspective. Tour Manag 38:94–104. https://doi.org/10.1016/j.tourman.2013.02.018
Johnson VL, Kiser A, Washington R, Torres R (2018) Limitations to the rapid adoption of M-payment services: understanding the impact of privacy risk on M-Payment services. Comput Hum Behav 79:111–122. https://doi.org/10.1016/j.chb.2017.10.035
Joo K, Kim J, Hwang J (2024) Effects of foodservice consumers’ perceptions of face recognition payment on attitude, desire, and behavioral intentions: a cross-cultural study. J Travel Tour Mark 41(3):359–376. https://doi.org/10.1080/10548408.2024.2318429
Katona Z, Zubcsek PP, Sarvary M (2011) Network effects and personal influences: the diffusion of an online social network. J Mark Res 48(3):425–443. https://doi.org/10.1509/jmkr.48.3.425
Kaufmann P, Stagl S, Franks DW (2009) Simulating the diffusion of organic farming practices in two New EU Member States. Ecol Econ 68(10):2580–2593. https://doi.org/10.1016/j.ecolecon.2009.04.001
Kesharwani A, Singh Bisht S (2012) The impact of trust and perceived risk on internet banking adoption in India: an extension of technology acceptance model. Int J Bank Mark 30(4):303–322. https://doi.org/10.1108/02652321211236923
Kim DJ, Ferrin DL, Rao HR (2008) A trust-based consumer decision-making model in electronic commerce: the role of trust, perceived risk, and their antecedents. Decis Support Syst 44(2):544–564. https://doi.org/10.1016/j.dss.2007.07.001
Kim MJ, Chung N, Lee CK (2011) The effect of perceived trust on electronic commerce: shopping online for tourism products and services in South Korea. Tour Manag 32(2):256–265. https://doi.org/10.1016/j.tourman.2010.01.011
Kline RB (2023) Principles and practice of structural equation modeling. Guilford Publications
Kwon OY (2019) Social trust: its concepts, determinants, roles, and raising ways. In: Social trust and economic development. Edward Elgar Publishing, pp. 19–49, https://doi.org/10.4337/9781784719609.00008
Lai X, Rau PLP (2021) Has facial recognition technology been misused? A public perception model of facial recognition scenarios. Comput Hum Behav 124:106894. https://doi.org/10.1016/j.chb.2021.106894
Lancelot Miltgen C, Popovic A, Oliveira T (2013) Determinants of end-user acceptance of biometrics: integrating the “big 3” of technology acceptance with privacy context. Decis Support Syst 56:103–114. https://doi.org/10.1016/j.dss.2013.05.010
Lee CT, Pan L-Y (2023a) Resistance of facial recognition payment service: a mixed method approach. J Serv Mark. https://doi.org/10.1108/JSM-01-2022-0035
Lee CT, Pan L-Y (2023b) Smile to pay: predicting continuous usage intention toward contactless payment services in the post-COVID-19 era. Int J Bank Mark. https://doi.org/10.1108/IJBM-03-2022-0130
Lee C, Coughlin JF (2015) PERSPECTIVE: older adults’ adoption of technology: an integrated approach to identifying determinants and barriers. J Prod Innov Manag 32(5):747–759. https://doi.org/10.1111/jpim.12176
Lee D (2019) Effects of key value co-creation elements in the healthcare system: focusing on technology applications. Serv Bus 13(2):389–417. https://doi.org/10.1007/s11628-018-00388-9
Li C, Li H (2023) Disentangling facial recognition payment service usage behavior: a trust perspective. Telemat Inform 77:101939. https://doi.org/10.1016/j.tele.2023.101939
Li H, Li L, Gan C, Liu Y, Tan C-W, Deng Z (2018) Disentangling the factors driving users’ continuance intention towards social media: a configurational perspective. Comput Hum Behav 85:175–182. https://doi.org/10.1016/j.chb.2018.03.048
Li X, Hess TJ, Valacich JS (2008) Why do we trust new technology? A study of initial trust formation with organizational information systems. J Strateg Inf Syst 17(1):39–71. https://doi.org/10.1016/j.jsis.2008.01.001
Lian JW, Lin TM (2008) Effects of consumer characteristics on their acceptance of online shopping: comparisons among different product types. Comput Hum Behav 24(1):48–65. https://doi.org/10.1016/j.chb.2007.01.002
Liang J, He Y, Fan L, Nuo M, Shen D, Xu J, Lei J (2022) A preliminary study on the abnormal deaths and work burden of Chinese physicians: a mixed method analysis and implications for smart hospital management. Front Public Health 9:803089. https://doi.org/10.3389/fpubh.2021.803089
Liao J, He S, Feng W, Filieri R (2024) “I love it” versus “I recommend it”: the impact of implicit and explicit endorsement styles on electronic word-of-mouth persuasiveness. J Travel Res 63(4):779–795. https://doi.org/10.1177/00472875231175083
Liao M, Agnihotri D, Zhong X (2022) “Paying with my face”—understanding users’ adoption and privacy concerns of facial recognition payment. In: Proceedings of the human factors and Ergonomics Society annual meeting, vol 66(1). SAGE Publications, Sage, CA; Los Angeles, CA, pp. 731–735
Lin A, Chen NC (2012) Cloud computing as an innovation: perception, attitude, and adoption. Int J Inf Manag 32(6):533–540. https://doi.org/10.1016/j.ijinfomgt.2012.04.001
Lindell MK, Whitney DJ (2001) Accounting for common method variance in cross-sectional research designs. J Appl Psychol 86(1):114–121. https://doi.org/10.1037/0021-9010.86.1.114
Liu A, Urquía-Grande E, López-Sánchez P, Rodríguez-López A (2022) How technology paradoxes and self-efficacy affect the resistance of facial recognition technology in online microfinance platforms: evidence from China. Technol Soc 70:102041. https://doi.org/10.1016/j.techsoc.2022.102041
Liu D, Tu W (2021) Factors influencing consumers’ adoptions of biometric recognition payment devices: combination of initial trust and UTAUT model. Int J Mob Commun 19(3):345. https://doi.org/10.1504/IJMC.2021.114324
Liu F (2020) Making cutting-edge technology approachable: a case study of facial-recognition payment in China. Nielsen Norman Gr. https://www.nngroup.com/articles/face-recognition-pay/. Accessed 29 Jun 2022
Liu K, Tao D (2022) The roles of trust, personalization, loss of privacy, and anthropomorphism in public acceptance of smart healthcare services. Comput Hum Behav 127:107026. https://doi.org/10.1016/j.chb.2021.107026
Liu Y, Yan W, Hu B (2021) Resistance to facial recognition payment in China: the influence of privacy-related factors. Telecommun Policy 45(5):102155. https://doi.org/10.1016/j.telpol.2021.102155
Lo Piano S (2020) Ethical principles in machine learning and artificial intelligence: cases from the field and possible ways forward. Humanit Soc Sci Commun 7(1). https://doi.org/10.1057/s41599-020-0501-9
Lu J, Yao JE, Yu CS (2005) Personal innovativeness, social influences and adoption of wireless Internet services via mobile technology. J Strateg Inf Syst 14(3):245–268. https://doi.org/10.1016/j.jsis.2005.07.003
Lu Y, Cao Y, Wang B, Yang S (2011) A study on factors that affect users’ behavioral intention to transfer usage from the offline to the online channel. Comput Hum Behav 27(1):355–364. https://doi.org/10.1016/j.chb.2010.08.013
Luo X, Li H, Zhang J, Shim JP (2010) Examining multi-dimensional trust and multi-faceted risk in initial acceptance of emerging technologies: an empirical study of mobile banking services. Decis Support Syst 49(2):222–234. https://doi.org/10.1016/j.dss.2010.02.008
Marcati A, Guido G, Peluso AM (2008) The role of SME entrepreneurs’ innovativeness and personality in the adoption of innovations. Res Policy 37(9):1579–1590. https://doi.org/10.1016/j.respol.2008.06.004
Maroufkhani P, Asadi S, Ghobakhloo M, Jannesari MT, Ismail WKW (2022) How do interactive voice assistants build brands’ loyalty? Technol Forecast Soc Change 183. https://doi.org/10.1016/j.techfore.2022.121870
Matthews L (2017) Applying multigroup analysis in PLS-SEM: a step-by-step process. In: Latan H, Noonan R (eds) Partial least squares path modeling: basic concepts, methodological issues and applications. Springer International Publishing, pp. 219–243
McKnight DH, Chervany NL (2001) What trust means in e-commerce customer relationships: an interdisciplinary conceptual typology. Int J Electron Commer 6(2):35–59. https://doi.org/10.1080/10864415.2001.11044235
Mei H, Ma Y, Wei Y, Chen W (2018) The design space of construction tools for information visualization: a survey. J Vis Lang Comput 44:120–132. https://doi.org/10.1016/j.jvlc.2017.10.001
Meijer SS, Catacutan D, Ajayi OC, Sileshi GW, Nieuwenhuis M (2015) The role of knowledge, attitudes and perceptions in the uptake of agricultural and agroforestry innovations among smallholder farmers in sub-Saharan Africa. Int J Agric Sustain 13(1):40–54. https://doi.org/10.1080/14735903.2014.912493
Ming‐Yen Teoh W, Choy Chong S, Lin B, Wei Chua J (2013) Factors affecting consumers’ perception of electronic payment: an empirical analysis. Internet Res 23(4):465–485. https://doi.org/10.1108/IntR-09-2012-0199
Miraz MH, Hasan MT, Rekabder MS, Akhter R (2022) Trust, transaction transparency, volatility, facilitating condition, performance expectancy towards cryptocurrency adoption through intention to use. J Manag Inf Decis Sci 25:1–20
Moradi R, Groth KM (2019) Hydrogen storage and delivery: review of the state of the art technologies and risk and reliability analysis. Int J Hydrog Energy 44(23):12254–12269. https://doi.org/10.1016/j.ijhydene.2019.03.041
Moriuchi E (2021) An empirical study of consumers’ intention to use biometric facial recognition as a payment method. Psychol Mark 38(10):1741–1765. https://doi.org/10.1002/mar.21495
Morosan C (2011) Customers’ adoption of biometric systems in restaurants: an extension of the technology acceptance model. J Hosp Mark Manag 20(6):661–690. https://doi.org/10.1080/19368623.2011.570645
Morosan C (2012a) Theoretical and empirical considerations of guests’ perceptions of biometric systems in hotels: extending the technology acceptance model. J Hosp Tour Res 36(1):52–84. 10.1177%2F1096348010380601
Morosan C (2012b) Voluntary steps toward air travel security: an examination of travelers’ attitudes and intentions to use biometric systems. J Travel Res 51(4):436–450. 10.1177%2F0047287511418368
Morosan C (2016) An empirical examination of U.S. travelers’ intentions to use biometric e-gates in airports. J Air Transp Manag 55:120–128. https://doi.org/10.1016/j.jairtraman.2016.05.005
Morosan C (2020) Hotel facial recognition systems: insight into guests’ system perceptions, congruity with self-image, and anticipated emotions. J Electron Commer Res 21(1):21–38
Muhayiddin MN, Ahmed EM, Ismail H (2011) Technology acceptance of a gold dinar based electronic payment system. https://doi.org/10.4236/ib.2011.33039
Musyaffi AM, Sari DAP, Respati DK (2021) Understanding of digital payment usage during COVID-19 pandemic: a study of UTAUT extension model in Indonesia. J Asian Financ Econ Bus 8(6):475–482. https://doi.org/10.13106/jafeb.2021.vol8.no6.0475
Nan D, Kim Y, Huang J, Jung HS, Kim JH (2022) Factors affecting intention of consumers in using face recognition payment in offline markets: an acceptance model for future payment service. Front Psychol 13:830152. https://doi.org/10.3389/fpsyg.2022.830152
Negri NAR, Borille GMR, Falcão VA (2019) Acceptance of biometric technology in airport check-in. J Air Transp Manag 81:101720. https://doi.org/10.1016/j.jairtraman.2019.101720
Ngugi B, Kamis A, Tremaine M (2011) Intention to use biometrics systems. e-Serv J 7(3):20–46. https://doi.org/10.2979/eservicej.7.3.20
Nigam D, Patel SN, Raj Vincent PM, Srinivasan K, Arunmozhi S (2022) Biometric authentication for intelligent and privacy-preserving healthcare systems. J Healthcare Eng. https://doi.org/10.1155/2022/1789996
Nysveen H, Pedersen PE, Thorbjørnsen H, Berthon P (2005) Mobilizing the brand: the effects of mobile services on brand relationships and main channel use. J Serv Res 7(3):257–276. https://doi.org/10.1177/1094670504271151
O’Brien J, Marakas G (2007) Introduction to information systems, 13th edn. McGraw-Hill, New York, NY
Ogbanufe O, Kim DJ (2018) Comparing fingerprint‐based biometrics authentication versus traditional authentication methods for e-payment. Decis Support Syst 106:1–14. https://doi.org/10.1016/j.dss.2017.11.003
Okumus B, Ali F, Bilgihan A, Ozturk AB (2018) Psychological factors influencing customers’ acceptance of smartphone diet apps when ordering food at restaurants. Int J Hosp Manag 72:67–77. https://doi.org/10.1016/j.ijhm.2018.01.001
Ouyang Z, Yao CN, Hu X (2020) “Crisis spillover of corporate environmental misconducts: the roles of perceived similarity, familiarity, and corporate environmental responsibility in determining the impact on oppositional behavioral intention”. Bus Strategy Environ 29(4):1797–1808. https://doi.org/10.1002/bse.2474
Pai CK, Wang TW, Chen SH, Cai KY (2018) Empirical study on Chinese tourists’ perceived trust and intention to use biometric technology. Asia Pac J Tour Res 23(9):880–895. https://doi.org/10.1080/10941665.2018.1499544
Paine C, Reips UD, Stieger S, Joinson A, Buchanan T (2007) Internet users’ perceptions of ‘privacy concerns’ and ‘privacy actions’. Int J Hum Comput Stud 65(6):526–536. https://doi.org/10.1016/j.ijhcs.2006.12.001
Palash MAS, Talukder MS, Islam AN, Bao Y (2022) Positive and negative valences, personal innovativeness and intention to use facial recognition for payments. Ind Manag Data Syst 122(4):1081–1108. https://doi.org/10.1108/IMDS-04-2021-0230
Pan J, Ding S, Wu D, Yang S, Yang J (2019) Exploring behavioural intentions toward smart healthcare services among medical practitioners: a technology transfer perspective. Int J Prod Res 57(18):5801–5820. https://doi.org/10.1080/00207543.2018.1550272
Park J, Gunn F, Han SL (2012) Multidimensional trust building in e-retailing: cross-cultural differences in trust formation and implications for perceived risk. J Retail Consum Serv 19(3):304–312. https://doi.org/10.1016/j.jretconser.2012.03.003
Pavlou PA (2003) Consumer acceptance of electronic commerce: integrating trust and risk with the technology acceptance model. Int J Electron Commer 7(3):101–134. https://doi.org/10.1080/10864415.2003.11044275
Pérez-Macías N, Fernández-Fernández J-L, Rúa-Vieites A (2021) Entrepreneurial intention among online and face-to-face university students: the influence of structural and cognitive social capital dimensions. J Int Entrep 19(3):434–467. https://doi.org/10.1007/s10843-020-00280-6
Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP (2003) Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol 88(5):879–903. https://doi.org/10.1037/0021-9010.88.5.879
Powell A, Williams CK, Bock DB, Doellman T, Allen J (2012) e-Voting intent: a comparison of young and elderly voters. Gov Inf Q 29(3):361–372. https://doi.org/10.1016/j.giq.2012.01.003
Priem R (2021) An exploratory study on the impact of the COVID-19 confinement on the financial behavior of individual investors. Econ Manag Financ Mark 16:9–40. https://doi.org/10.22381/emfm16320211
Rahi S, Abd. Ghani M (2019) Investigating the role of UTAUT and e-service quality in Internet banking adoption setting. TQM J 31(3):491–506. https://doi.org/10.1108/TQM-02-2018-0018
Rasiah D, Yen YY (2020) User acceptance of ATM biometric authentication. Glob J Comput Sci: Theory Res 10(1):011–017. https://doi.org/10.18844/gjcs.v10i1.4748
Ray S, Ow T, Kim SS (2011) Security assurance: how online service providers can influence security control perceptions and gain trust. Decis Sci 42(2):391–412. https://doi.org/10.1111/j.1540-5915.2011.00316.x
Rodrigues G, Sarabdeen J, Balasubramanian S (2016) Factors that influence consumer adoption of e-government services in the UAE: a UTAUT model perspective. J Internet Commer 15(1):18–39. https://doi.org/10.1080/15332861.2015.1121460
Rodríguez-Torrico P, San-Martín S, San José Cabezudo R (2020) The role of omnichannel tendency in digital information processing. Online Inf Rev 44(7):1347–1367. https://doi.org/10.1108/OIR-08-2019-0272
Rogers EM, Singhal A, Quinlan MM (2014) Diffusion of innovations. In: An integrated approach to communication theory and research. Routledge, pp. 432–448
Sarrab M, Elbasir M, Alnaeli S (2016) Towards a quality model of technical aspects for mobile learning services: an empirical investigation. Comput Hum Behav 55:100–112. https://doi.org/10.1016/j.chb.2015.09.003
Sekhon H, Ennew C, Kharouf H, Devlin J (2014) Trustworthiness and trust: influences and implications. J Mark Manag 30(3-4):409–430. https://doi.org/10.1080/0267257X.2013.842609
Seng S, Al-Ameen MN, Wright M (2021) A first look into users’ perceptions of facial recognition in the physical world. Comput Secur 105:102227. https://doi.org/10.1016/j.cose.2021.102227
Shao Z, Zhang L, Li X, Guo Y (2019) Antecedents of trust and continuance intention in mobile payment platforms: the moderating effect of gender. Electron Commer Res Appl 33:100823. https://doi.org/10.1016/j.elerap.2018.100823
Sharma SK, Mangla SK, Luthra S, Al-Salti Z (2018) Mobile wallet inhibitors: developing a comprehensive theory using an integrated model. J Retail Consum Serv 45:52–63. https://doi.org/10.1016/j.jretconser.2018.08.008
Sheppard BH, Hartwick J, Warshaw PR (1988) The theory of reasoned action: a meta-analysis of past research with recommendations for modifications and future research. J Consum Res 15(3):325–343. https://doi.org/10.1086/209170
Shiau WL, Liu C, Zhou M, Yuan Y (2023) Insights into customers’ psychological mechanism in facial recognition payment in offline contactless services: integrating belief–attitude–intention and TOE–I frameworks. Internet Res 33(1):344–387. https://doi.org/10.1108/INTR-08-2021-0629
Shibl R, Lawley M, Debuse J (2013) Factors influencing decision support system acceptance. Decis Support Syst 54(2):953–961. https://doi.org/10.1016/j.dss.2012.09.018
Shin DH (2009) Towards an understanding of the consumer acceptance of mobile wallet. Comput Hum Behav 25(6):1343–1354. https://doi.org/10.1016/j.chb.2009.06.001
Si H, Duan X, Cheng L, Zhang Z (2022) Determinants of consumers’ continuance intention to use dynamic ride-sharing services. Transp Res Part D: Transp Environ 104:103201. https://doi.org/10.1016/j.trd.2022.103201
Sicari S, Rizzardi A, Grieco LA, Coen-Porisini A (2015) Security, privacy and trust in Internet of Things: the road ahead. Comput Netw 76:146–164. https://doi.org/10.1016/j.comnet.2014.11.008
Smith ML (2010) Building institutional trust through e‐government trustworthiness cues. Inf Technol People 23(3):222–246. https://doi.org/10.1108/09593841011069149
Soh KL, Wong WP, Chan KL (2010) Adoption of biometric technology in online applications. Int J Bus Manag Sci 3(2):121–146. https://doi.org/10.3316/informit.341612190471725
Soper D (2018) A-priori sample size calculator for multiple regression. https://www.danielsoper.com/statcalc
Surf (2022) How to build Fintech Trust with app users: top 5 UX design practices. https://surf.dev/how-to-build-fintech-trust-with-app-users-top-5-ux-design-practices/
Tamilmani K, Rana NP, Dwivedi YK (2020) Consumer acceptance and use of information technology: a meta-analytic evaluation of UTAUT2. Inf Syst Front 1–19 https://doi.org/10.1007/s10796-020-10007-6
Tams S, Thatcher JB, Craig K (2018) How and why trust matters in post-adoptive usage: the mediating roles of internal and external self-efficacy. J Strateg Inf Syst 27(2):170–190. https://doi.org/10.1016/j.jsis.2017.07.004
Tandon U, Kiran R, Sah AN (2016) Understanding online shopping adoption in India: unified theory of acceptance and use of technology 2 (UTAUT2) with perceived risk application. Serv Sci 8(4):420–437. https://doi.org/10.1287/serv.2016.0154
Taylor S, Todd PA (1995) Understanding information technology usage: a test of competing models. Inf Syst Res 6(2):144–176. https://doi.org/10.1287/isre.6.2.144
Tee H-H, Ong H-B (2016) Cashless payment and economic growth. Financ Innov 2(1):4. https://doi.org/10.1186/s40854-016-0023-z
Thompson RL, Higgins CA, Howell JM (1991) Personal computing: toward a conceptual model of utilization. MIS Q 125–143. https://doi.org/10.2307/249443
Thompson RL, Higgins CA, Howell JM (1994) Influence of experience on personal computer utilization: testing a conceptual model. J Manag Inf Syst 11(1):167–187. https://doi.org/10.1080/07421222.1994.11518035
Thongsri N, Shen L, Bao Y, Alharbi IM (2018) Integrating UTAUT and UGT to explain behavioural intention to use M-learning: a developing country’s perspective. J Syst Inf Technol 20(3):278–297. https://doi.org/10.1108/JSIT-11-2017-0107
Turban E, Outland J, King D, Lee JK, Liang TP, Turban DC, ... & Turban DC (2018) Electronic commerce payment systems. In: Electronic Commerce 2018: A Managerial and Social Networks Perspective. Springer, Cham, pp. 457–499
Venkatesh V, Morris MG, Davis GB, Davis FD (2003) User acceptance of information technology: toward a unified view. MIS Q 27(3):425–478. https://doi.org/10.2307/30036540
Virtual Smart Technologies (2024) When it comes to security, Facial Recognition not only enhances control over who is entering and exiting a special area or building, but when combined with an Access Control System, also ensures that entry/exit is limited only to authorised personnel. Facial Recognition. https://virtualsmarttech.com/virtual-products-services/security-systems/cctv-systems/facial-recognition/
Wandersman A, Chien VH, Katz J (2012) Toward an evidence‐based system for innovation support for implementing innovations with quality: tools, training, technical assistance, and quality assurance/quality improvement. Am J Community Psychol 50(3–4):445–459. https://doi.org/10.1007/s10464-012-9509-7
Wang C, Dai J, Zhu K, Yu T, Gu X (2023) Understanding the continuance intention of college students toward new E-learning spaces based on an integrated model of the TAM and TTF. Int J Hum–Comput Interact 1–14. https://doi.org/10.1080/10447318.2023.2291609
Wisdom JP, Chor KHB, Hoagwood KE, Horwitz SM (2014) Innovation adoption: a review of theories and constructs. Adm Policy Ment Health Ment Health Serv Res 41:480–502. https://doi.org/10.1007/s10488-013-0486-4
Yang K (2010) Determinants of US consumer mobile shopping services adoption: implications for designing mobile shopping services. J Consum Mark 27(3):262–270. https://doi.org/10.1108/07363761011038338
Yang S, Isa SM, Ramayah T (2022) Does uncertainty avoidance moderate the effect of self-congruity on revisit intention? A two-city (Auckland and Glasgow) investigation. J Destin Mark Manag 24:100703. https://doi.org/10.1016/j.jdmm.2022.100703
Yeong YC, Kalid KS, Savita KS, Ahmad MN, Zaffar M (2022) Sustainable cryptocurrency adoption assessment among IT enthusiasts and cryptocurrency social communities. Sustain Energy Technol Assess 52:102085. https://doi.org/10.1016/j.seta.2022.102085
Yousafzai S, Pallister J, Foxall G (2009) Multi-dimensional role of trust in internet banking adoption. Serv Ind J 29(5):591–605. 10.1080/02642060902719958
Yu T, Teoh AP, Bian Q, Liao JY, Wang CL (2024a) Can virtual influencers affect purchase intentions in tourism and hospitality e-commerce live streaming? An empirical study in China. Int J Contemp Hosp Manag. https://doi.org/10.1108/IJCHM-03-2024-0358
Yu T, Wang C, Bian Q, Teoh AP (2024b) Acceptance of or resistance to facial recognition payment: a systematic review. J Consum Behav 1–19. https://doi.org/10.1002/cb.2385
Yu T, Zhang Y, Teoh AP, Wang A, Wang C (2023b) Factors influencing university Students’ behavioral intention to use electric car-sharing Services in Guangzhou, China. SAGE Open 13(4):21582440231210551. https://doi.org/10.1177/21582440231210551
Zhang L, Verma B, Tjondronegoro D, Chandran V (2018) Facial expression analysis under partial occlusion: a survey. ACM Comput Surv (CSUR) 51(2):1–49. https://doi.org/10.1145/3158369
Zhang T, Tao D, Qu X, Zhang X, Lin R, Zhang W (2019) The roles of initial trust and perceived risk in public’s acceptance of automated vehicles. Transp Res Part C: Emerg Technol 98:207–220. https://doi.org/10.1016/j.trc.2018.11.018
Zhang X, Shi Y, Li T, Guan Y, Cui X (2023) How do virtual AI streamers influence viewers’ livestream shopping behavior? The effects of persuasive factors and the mediating role of arousal. Inf Syst Front. https://doi.org/10.1007/s10796-023-10425-2
Zheng Y, Zhao K, Stylianou A (2013) The impacts of information quality and system quality on users’ continuance intention in information-exchange virtual communities: an empirical investigation. Decis Support Syst 56:513–524. https://doi.org/10.1016/j.dss.2012.11.008
Zhong Y, Oh S, Moon HC (2021) Service transformation under industry 4.0: investigating acceptance of facial recognition payment through an extended technology acceptance model. Technol Soc 64:101515. https://doi.org/10.1016/j.techsoc.2020.101515
Zhou T (2012) Examining location-based services usage from the perspectives of unified theory of acceptance and use of technology and privacy risk. J Electron Commer Res 13(2):135
Zhou T, Lu Y, Wang B (2010) Integrating TTF and UTAUT to explain mobile banking user adoption. Comput Hum Behav 26(4):760–767. https://doi.org/10.1016/j.chb.2010.01.013
Zhou W, Dong J, Zhang W (2022) The impact of interpersonal interaction factors on consumers’ purchase intention in social commerce: a relationship quality perspective. Ind Manag Data Syst 123(3):697–721. https://doi.org/10.1108/imds-06-2022-0392
Zimmer JC, Arsal RE, Al-Marzouq M, Grover V (2010) Investigating online information disclosure: effects of information relevance, trust and risk. Inf Manag 47(2):115–123. https://doi.org/10.1016/j.im.2009.12.003
Zimmermann V, Gerber N (2020) The password is dead, long live the password—a laboratory study on user perceptions of authentication schemes. Int J Hum–Comput Stud 133:26–44. https://doi.org/10.1016/j.ijhcs.2019.08.006
Acknowledgements
This work was supported by 2024 Guangdong Education Science Planning Project (Special Project of Higher Education, Grant number: 2024GXJK449), 2024 Regular Project of the “14th Five-Year Plan” for the Development of Philosophy and Social Sciences in Guangzhou (Grant number: 2024GZQN85), and 2024 Higher Education Research Project under the “14th Five-Year Plan” by the Guangdong Society of Higher Education (Grant number: 24GQN27).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study obtained approval from the Research Ethical Board at Guangzhou College of Commerce (No. REBGCC/10/2023). The research was conducted in accordance with the ethical guidelines set forth by the university. Simultaneously, in studies involving human participants, all procedures adhered to the ethical standards of the institutional and/or national research committee, as well as the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
The researcher sought and gained the written informed consent of the participants to take part in the study. Out of the 1479 sampled participants, all 1479 accepted and voluntarily participated in the study after the researcher assured them of anonymity and that their responses were solely for academic purposes. All participants read and signed a consent form before the study conducted in October 2023.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix 1
Appendix 1

Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yu, T., Teoh, A.P., Wang, C. et al. Convenient or risky? Investigating the behavioral intention to use facial recognition payment in smart hospitals. Humanit Soc Sci Commun 11, 1592 (2024). https://doi.org/10.1057/s41599-024-03910-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-024-03910-9
This article is cited by
-
ROFI: a deep learning-based ophthalmic sign-preserving and reversible patient face anonymizer
npj Digital Medicine (2025)
