
Abstract
Background
The systematic review aimed to assess the effects of GLP-1 receptor agonists (GLP-1 RA) and dual GLP-1/GIP agonists on weight loss and body composition in individuals with overweight or obesity, with or without type 2 diabetes mellitus.
Methods
The study protocol was registered in PROSPERO (CRD420251002447). A systematic search of PubMed, Scopus, and Web of Science was conducted up to December 2024 according to PRISMA guidelines. Following the predefined inclusion and exclusion criteria, 36 studies were included in this systematic review and underwent qualitative analysis. In addition, 24 studies met the criteria for quantitative synthesis (meta-analysis). Data were pooled using random-effects models with subgroup analyses by drug type and treatment duration (3, 6, and 12 months).
Results
GLP-1 RA treatment consistently reduced body weight, BMI, and waist circumference across all time points. At 3 months, mean body weight decreased by approximately 9%, accompanied by marked reductions in fat mass and visceral adipose tissue. At 6 months, weight reduction averaged 5%, with semaglutide, liraglutide, and exenatide showing comparable effects, while lean mass remained largely preserved. At 12 months, weight loss persisted at around 4%, with variability between agents, most notably liraglutide. Across studies, fat mass decline predominated, whereas reductions in lean body mass were modest.
Conclusion
GLP-1 RAs provide clinically meaningful weight loss primarily through selective fat mass reduction, with relative preservation of lean tissue, supporting their role in achieving “quality” weight loss. Differences between agents highlight the importance of individualized treatment strategies, complemented by nutritional and exercise interventions to optimize long-term outcomes.

Similar content being viewed by others

Introduction
Obesity is a complex, multifactorial chronic disease characterized by excess adiposity, with or without abnormal distribution or function of adipose tissue, leading to adverse effects on health. Over the past several decades, its prevalence has risen at an alarming rate worldwide, reaching pandemic proportions and showing no signs of stabilization [1, 2]. The pathogenesis of obesity involves a dynamic interplay of genetic, environmental, behavioral, and metabolic factors [2, 3]. Obesity is associated with numerous cardiometabolic complications and contributes to increased overall mortality [4, 5]. These comorbidities contribute to a marked reduction in both life expectancy and quality of life. Beyond physical health, obesity often carries substantial psychological and social burdens, such as depression, stigma, and reduced self-esteem [6]. Given its complexity, effective obesity management necessitates a multidisciplinary, individualized approach that combines nutritional and behavioral interventions, physical activity, pharmacological therapies, and metabolic-bariatric surgery when indicated. The primary goal of treatment should extend beyond weight loss to encompass the preservation of lean mass, improvement in metabolic health, and long-term prevention of obesity-related complications [7].
Glucagon-like peptide-1 (GLP-1) is an incretin hormone released from enteroendocrine L-cells in the gastrointestinal tract in response to nutrient intake. It plays a pivotal role in energy balance and postprandial metabolism by enhancing glucose-dependent insulin secretion, suppressing glucagon release, delaying gastric emptying, and promoting satiety through central mechanisms [8, 9]. Due to its rapid enzymatic degradation, the physiological half-life of GLP-1 is short; however, GLP-1 receptor agonists (GLP-1RAs) have been developed to prolong its activity and maximize its metabolic benefits. GLP-1RAs exert pleiotropic effects that extend well beyond their initial use in glycemic management [8]. In individuals with obesity, these agents contribute to significant and sustained weight reduction by enhancing satiety, reducing appetite, and lowering overall caloric intake [9]. Weight loss achieved through GLP-1 RAs therapy is accompanied by meaningful improvements in multiple obesity-related comorbidities. Additionally, GLP-1 RAs have demonstrated cardioprotective properties, including favorable effects on cardiac function, vascular integrity, and endothelial performance [10]. Their metabolic actions include enhanced peripheral glucose uptake, reduced hepatic glucose output, and improved lipid metabolism [11]. The development of next-generation GLP-1 RAs and dual agonists further expands the therapeutic potential of this drug class in addressing the complex, multisystem consequences of obesity [8].
The weight-lowering effects of GLP-1 RAs are mediated through multiple, interrelated mechanisms. Primarily, they act on the hypothalamus to enhance satiety, delay gastric emptying, and reduce caloric intake, leading to a preferential reduction in fat body mass (FBM). GLP-1 RAs also improve insulin sensitivity, reduce ectopic fat deposition, and modulate adipose tissue metabolism by stimulating lipolysis and inhibiting lipogenesis [12, 13]. Importantly, their influence extends to skeletal muscle, where GLP-1 RAs promote glucose uptake via the AMP-activated protein kinase pathway, increase vascular blood flow, and mitigate glucotoxicity, thereby supporting muscle protein synthesis and inhibiting catabolic pathways [14, 15]. Preclinical data further indicate that liraglutide activates the SIRT1 signaling cascade, suppresses atrophy-related genes, and upregulates myogenic differentiation factors, thereby protecting against obesity-induced muscle atrophy and contributing to structural muscle integrity [14, 16]. Collectively, these findings highlight the dual capacity of GLP-1 RAs to reduce FBM while supporting skeletal muscle health, a distinction of clinical importance in the long-term management of obesity.
Despite these favorable mechanisms, concerns remain regarding the impact of GLP-1 RAs on lean body mass (LBM) and the potential risk of sarcopenia. Clinical and meta-analytic data indicate that, although FBM reduction predominates, modest decreases in LBM can occur, particularly during substantial weight loss [17, 18]. This raises questions about whether GLP-1 RAs may contribute to muscle loss in vulnerable populations, such as older adults or those with pre-existing frailty. Sporadic reports of skeletal muscle decline highlight the need for careful monitoring, as sarcopenia, characterized by reduced muscle mass and impaired physical function, may worsen metabolic outcomes and increase morbidity [19, 20]. Importantly, the observed LBM reduction has not consistently translated into functional impairment, and emerging evidence suggests that GLP-1 RAs may counterbalance this effect by improving muscle quality and metabolism [21]. Nonetheless, in patients at high risk of sarcopenia, tailored management including nutritional optimization and concurrent resistance training should be considered to mitigate potential adverse consequences during pharmacologically induced weight loss [20].
Given the heterogeneity among GLP-1RAs in terms of pharmacokinetic profiles, therapeutic efficacy, adverse event rates, and dosing regimens, each agent should be assessed individually. Moreover, a thorough understanding of the specific benefits and limitations of each GLP-1 RA is essential for informed clinical decision-making. To address this need, we conducted a systematic review and meta-analysis to evaluate and compare the efficacy of GLP-1 RAs in promoting weight loss and modulating body composition in individuals with overweight or obesity with or without T2DM.
Methods
Data sources and search strategy
This systematic review was conducted up to 01 December 2024 in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines. A comprehensive literature search was performed across three databases: PubMed, Scopus, and Web of Science. The search strategy was developed to identify clinical studies investigating the effects of GLP-1RAs on body composition and anthropometric indices for individuals with overweight or obesity, with or without T2DM. The following search algorithm was applied: ((“GLP-1 receptor agonist” OR “glucagon-like peptide-1 receptor agonist” OR “GIP receptor agonist” OR “glucose-dependent insulinotropic polypeptide” OR liraglutide OR semaglutide OR dulaglutide OR tirzepatide) AND (“body composition” OR “fat mass” OR “muscle mass” OR “lean mass” OR “adiposity” OR “body fat” OR “sarcopenia”)) AND (“clinical trial” OR “study” OR “randomized controlled trial” OR “RCT” OR “intervention study”).
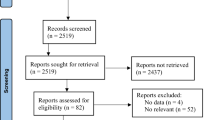
The literature search was independently performed by three investigators. After the removal of duplicates, titles and abstracts were screened for eligibility. Full-text articles were assessed against prespecified inclusion and exclusion criteria. Discrepancies during the screening process were resolved by consulting the clinical experts and methodologists. The specific criteria for inclusion and exclusion of relevant studies in terms of PI(E)COS (“Population”, “Intervention”/”Exposure”, “Comparison”, “Outcomes”, and “Study design”) are provided in Table 1. A detailed search flowchart is shown in Supplementary Fig. S1.
The study protocol was registered in the International Prospective Register of systematic reviews PROSPERO (CRD420251002447).
Quality assessment and critical appraisal for the systematic review of the included studies
The methodological quality of the included studies was evaluated independently by two reviewers using the Study Quality Assessment Tools developed by the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH), tailored to the design of each included study. Each study was assessed across key domains, including clarity of objectives, eligibility criteria, sample size justification, outcome measurement, blinding (if applicable), and adequacy of statistical analyses. Studies were then categorized as having low, moderate, or high risk of bias based on cumulative scoring. A summary of the risk of bias assessment is presented in Supplementary Fig. S2.
Data synthesis and analysis
All included studies were discussed as part of the quantitative analysis. The quantitative analysis comprised 24 studies involving a total of 1,032 patients who presented numerical data on changes in selected anthropometric and body composition parameters resulting from GLP-1 RA therapy. A subgroup meta-analysis was conducted based on the type of GLP-1 RA used, separately for three treatment durations: 3 months, 6 months, and 12 months. For each parameter, the mean difference or ratio of means was calculated. Selected relationships of particular clinical significance were additionally presented graphically using forest plots. The results of the meta-analysis for the associated biochemical parameters are presented in Supplementary Tables S1–S3. Due to study heterogeneity, random-effects models were applied. Egger’s test was used to assess publication bias. A significance level of alpha = 0.05 was adopted for all analyses. All analyses were conducted using Statistica 13.3 software (StatSoft, Kraków, Poland).
Results
Descriptive data are summarized in Table 2. The included studies showed notable geographical diversity, with the majority originating from Europe and Asia. Studies were categorized according to the duration of therapy, with the majority reporting outcomes after a 6-month follow-up period. Both patients with T2DM (24 studies) and those without T2DM were included. The most frequently investigated GLP-1 RAs were liraglutide and semaglutide, predominantly administered via the subcutaneous route. Body composition (BC) was assessed using various methods, most commonly bioelectrical impedance analysis (BIA), followed by dual-energy X-ray absorptiometry (DXA).
3-month GLP-1 RA therapy
Following 3 months of GLP-1 RA therapy, significant improvements were observed across anthropometric and body composition parameters (Table 3).
Meta-analysis revealed a substantial 9% reduction in body mass (RoM 0.91; 95% CI: 0.90 to 0.93; p < 0.001), BMI (MD −2.96 kg/m²; 95% CI: −3.03 to −2.88; p < 0.001), and waist circumference (MD −9.6 cm; 95% CI: −9.9 to −9.4; p < 0.001). These effects were consistently notable across individual studies, with the greatest reductions observed in those receiving beinaglutide.
Regarding body composition, GLP-1 RA therapy led to a significant 17% decline in fat mass (RoM 0.83; 95% CI: 0.82–0.85; p < 0.001) and visceral adipose tissue area (MD −29.25 cm²; 95% CI: −30.22 to −28.28; p < 0.001). A modest but statistically significant 2% reduction in lean body mass was also observed (RoM 0.98; 95% CI: 0.97–0.99; p = 0.004).
Intergroup comparisons revealed statistically significant differences between GLP-1 RAs across most parameters (p < 0.001), except from lean body mass. Egger’s test indicated potential publication bias for some outcomes.
6-month GLP-1 RA therapy
Following six months of GLP-1 RA therapy, a meta-analysis revealed statistically significant improvements in multiple anthropometric and body composition parameters (Table 4).
Body mass was significantly reduced by 5% (RoM 0.95; 95% CI: 0.93–.96; p < 0.001). Consistent reductions were observed across studies utilizing exenatide, liraglutide, and semaglutide, without significant intergroup differences (p = 0.310). Similarly, BMI decreased significantly (MD −2.40 kg/m²; 95% CI: −2.86 to −1.94; p < 0.001), again without significant differences between GLP-1 RA types (p = 0.513). Waist circumference also improved modestly but significantly (MD −2.3 cm; 95% CI: −2.8 to −1.7; p < 0.001), with significant intergroup heterogeneity (p = 0.012).
Regarding body composition, fat body mass decreased significantly by 6% (RoM 0.94; 95% CI: 0.91–0.96; p < 0.001), with differences between GLP-1 RAs (p < 0.001). Fat-free mass did not significantly change (RoM 1.01; 95% CI: 0.97–1.05; p = 0.657), nor did the relative skeletal muscle index (MD −0.04 kg/m²; 95% CI: −0.19 to 0.11; p = 0.563). Lean body mass was significantly reduced by 1% (RoM 0.99; 95% CI: 0.97–1.00; p = 0.021), and skeletal muscle mass significantly declined by 3% (RoM 0.97; 95% CI: 0.94–1.00; p = 0.034); both without intergroup heterogeneity (p = 0.516 and p = 0.716, respectively). Also, visceral adipose tissue area significantly decreased (MD −32.31 cm²; 95% CI: −42.64 to −21.98; p < 0.001).
For the majority of outcomes, no significant evidence of publication bias was detected.
12-month GLP-1 RA therapy
After 12 months of GLP-1 RA therapy, significant improvements were observed across several anthropometric and body composition parameters (Table 5).
Body mass was significantly reduced by 4% (RoM 0.96; 95% CI: 0.95–0.97; p < 0.001). The effect was most pronounced with liraglutide in Capristo et al. – 24% (RoM 0.76), while smaller reductions were noted with semaglutide—6% (RoM 0.94) and dulaglutide – 1% (RoM 0.99). Intergroup differences were statistically significant (p < 0.001). Similarly, BMI was significantly reduced by −1.74 kg/m² (95% CI: −1.89 to −1.60; p < 0.001), with larger reductions again seen in the liraglutide group (−9.72 kg/m²). However, no significant intergroup differences were detected (p = 0.323). Waist circumference decreased significantly by −3.2 cm (95% CI: −4.1 to −2.2; p < 0.001), with consistent reductions across semaglutide and liraglutide studies—no intergroup differences were observed (p = 0.575).
Regarding body composition, fat mass was significantly reduced by 4% (RoM 0.96; 95% CI: 0.92–0.99; p < 0.001), although with substantial intergroup differences (p < 0.001). A significant 4% reduction was also observed in lean body mass (RoM 0.96; 95% CI: 0.95–0.97; p < 0.001), again with notable intergroup heterogeneity.
Egger’s test indicated no evidence of significant publication bias across most outcomes, with the exception of waist circumference, where bias could not be excluded (p = 0.019).
Discussion
Anthropometric and body composition changes during GLP-1 RA treatment
The results of this meta-analysis consistently highlight the substantial effectiveness of GLP-1RAs therapy in reducing key anthropometric indicators associated with obesity. BW, BMI, and WC all decreased significantly after 3, 6, and 12 months of treatment, suggesting both short- and long-term benefits (Fig. 1). The most rapid and substantial changes occurred during the initial three months of therapy, with beinaglutide emerging as the most potent agent in this early phase, particularly in terms of weight and BMI reduction. Specifically, after 3 months of therapy, BW decreased by approximately 9%. By 6 months, the effects remained pronounced, with BW reduced by 5%, largely comparable across agents, though semaglutide and liraglutide demonstrated a more sustained impact. At 12 months, BW reduction ranged around 4%, with liraglutide appearing to produce the most significant individual reduction in BW in one outlying study, although interstudy variability must be considered when interpreting this finding. In addition, the attenuation of BW loss observed at longer treatment durations may plausibly reflect more challenging long-term adherence to therapy and lifestyle recommendations, as well as potential adaptive physiological responses over time. Reductions in WC, a key marker of visceral adiposity, paralleled weight loss at all time points and were especially notable in early treatment phases. While intergroup differences were present, particularly in the short term, they became less distinct over time, reflecting convergence in therapeutic efficacy among agents with prolonged use. Although longer-term interventions sustained the anthropometric benefits, the rate of improvement appeared to attenuate over time, possibly reflecting adaptive metabolic responses or changes in treatment adherence.

Beyond improvements in total BW, GLP-1 RAs induced favorable alterations in BC, underscoring their impact on both quantity and quality of weight loss (Fig. 2). Treatment led to significant reductions in total fat body mass (FBM) and visceral adipose tissue (VAT), with the most pronounced effects observed within the first 6 months, aligning with earlier reductions in WC. Notably, beinaglutide was particularly effective in early reduction of FBM, while semaglutide achieved the most substantial decreases in visceral fat area at 6 and 12 months. Liraglutide also consistently demonstrated efficacy in reducing fat depots over longer durations. While a concurrent decline in LBM was detected, especially at the 3- and 12-month time points, these changes were proportionally modest relative to the overall BW loss. Among the agents, no single drug consistently preserved lean tissue better than others. However, liraglutide was associated with a more pronounced reduction in LBM in one long-term study, which may warrant closer monitoring in specific populations. These findings highlight the importance of integrating resistance training and nutritional support into pharmacological weight loss strategies.

Consistent with these meta-analytic findings, additional insights are provided by real-world observational studies. In a retrospective observational study applying a hybrid care model, patients with obesity with or without pre-diabetes were treated with semaglutide titrated to 1 mg weekly, tirzepatide escalated to 10 mg weekly, or liraglutide administered at 3 mg daily, alongside structured lifestyle support. After 3 months, the overall mean BW reduction reached 8.5% from baseline. Patients receiving semaglutide and tirzepatide achieved similar outcomes, with reductions of 8.3% and 8.8% respectively, while liraglutide was associated with a somewhat smaller decrease of 7.0%. BW loss was driven predominantly by reductions in FBM: 15.5% in the tirzepatide group, 13.9% with liraglutide, and 12.5% with semaglutide. Clinically meaningful thresholds were achieved in the majority of participants, with most patients surpassing a 10% reduction in BW within the first three months, and over one-third of those treated with tirzepatide exceeding a 15% reduction [22].
Multiple clinical studies have demonstrated that GLP-1 RAs are effective in inducing clinically meaningful BW loss across diverse patient populations, depending on the specific agent, dose, and treatment regimen. Yu et al. [23] examined the impact of liraglutide compared with lifestyle interventions on BC and abdominal fat distribution in patients with obesity and T2DM. Over the 12-week intervention, liraglutide in a dose up to 1.8 mg produced consistent improvements across key anthropometric parameters, with reductions in BW, BMI, and WC that exceeded those achieved with lifestyle modification alone. However, the overall degree of BW loss was modest and did not reach the clinically meaningful threshold of 5%. Importantly, BC analyses revealed not only a decrease in total FBM but also a preferential reduction in visceral and subcutaneous abdominal fat, accompanied by a decline in liver fat content. This is especially important, as ectopic fat distribution may be a critical determinant of cardiometabolic risk, in addition to overall obesity. Furthermore, Muñoz et al. [24] evaluated the use of liraglutide as an adjuvant therapy for preoperative BW loss in a high-risk cohort of patients with severe obesity undergoing preparation for bariatric-metabolic surgery. After 12 weeks of treatment with liraglutide 3.0 mg combined with lifestyle management, 94.6% of patients experienced BW reduction, with a mean total weight loss of 5.5%. In turn, Capristo et al. [25] went further and evaluated liraglutide 3.0 mg in combination with a highly structured lifestyle intervention that included a very low-calorie diet (VLCD) followed by a high-protein, low-carbohydrate regimen and intensive physical activity. This integrated approach resulted in an impressive 24% reduction in baseline BW, nearly twice the loss achieved by lifestyle modification alone and approaching the outcomes seen with sleeve gastrectomy. Total FBM decreased substantially, while LBM was better preserved than in patients undergoing surgery, likely due to the combination of high-protein intake and resistance-based exercise. Although patients lost over 8 kg of LBM, the proportional loss was smaller than in the surgical group, highlighting the protective effect of combining pharmacotherapy with diet and resistance training.
In turn, Rodríguez Jiménez et al. [26] demonstrated that 24 weeks of treatment with semaglutide, administered either orally at a maintenance dose of 14 mg daily or subcutaneously at 1 mg weekly, resulted in an average BW loss close to 10% of baseline BW. Patients treated with the oral formulation lost on average 8.6 kg, corresponding to 9.4% of initial BW, while those receiving the subcutaneous formulation lost 10.0 kg, or 9.5% of baseline BW. Importantly, the BW reduction was primarily attributable to loss of FBM, which declined by 8.0 kg in the oral group and 8.5 kg in the subcutaneous group, whereas LBM decreased only modestly by 0.7 kg and 1.7 kg, respectively. Additionally, in a retrospective analysis of Chinese patients with obesity, weekly subcutaneous semaglutide at a maintenance dose of 1.0 mg combined with lifestyle intervention over 24 weeks resulted in an average BW reduction of approximately 11%, with more than half of participants achieving at least a 10% decrease from baseline. BC analysis revealed that the majority of BW loss was attributable to reductions in FBM, which declined more than threefold compared with LBM. Notably, SMM percentage increased despite small absolute losses, and muscle strength, as assessed by grip testing, remained stable [27].
Compared with injectable formulations, oral semaglutide is associated with a more modest reduction in BW. For example, in a study by Pantanetti et al. [28], patients with obesity and T2DM treated with oral semaglutide titrated to a maintenance dose of 14 mg daily over 6 months experienced modest but significant improvements in anthropometric parameters. Average BW decreased by just over 3 kg, corresponding to a reduction of roughly 3–4% from baseline, and this was accompanied by a parallel decline in BMI. It is worth noting that the observed decrease in FBM percentage was minimal, as were the changes observed for other parameters, such as muscle mass and water content. Additionally, in a real-world study by Volpe et al. [29], patients with obesity and T2DM who received oral semaglutide at a maintenance dose of 7 mg daily for six months experienced an average BW reduction of approximately 4 kg, corresponding to a roughly 5% decrease from baseline, accompanied by significant parallel reductions in BMI and WC. Importantly, BC analysis revealed a selective reduction in total FBM and fat mass index, while FFM and SMM were preserved. Indeed, indices of SMM showed a tendency to increase, leading to a more favorable SMM/VAT ratio, despite the absence of specific exercise recommendations. The favorable evolution of the SMM/VAT ratio suggests that semaglutide not only promotes adiposity loss but also helps to counteract the development of sarcopenic visceral obesity, a condition strongly linked to insulin resistance and cardiometabolic risk. The preservation of lean tissue may reflect the pleiotropic effects of GLP-1 RAs on skeletal muscle, including improved vascular perfusion, stimulation of glucose uptake via AMP-activated protein kinase, and enhanced microvascular recruitment, all of which can favor protein synthesis and limit muscle breakdown. These physiological actions contribute to maintaining muscle integrity while promoting preferential fat loss, ultimately leading to a more metabolically favorable BC profile in patients with T2DM.
In the pilot trial by Anyiam et al. [30], individuals with obesity and T2DM were randomized to receive once-weekly subcutaneous semaglutide titrated to a target dose of 1 mg, VLCD, or a combination of both for 12 weeks. Individuals treated with semaglutide alone achieved an average BW reduction of 6 kg, corresponding to nearly 6% of baseline BW. In contrast, participants following a VLCD or the combination regimen experienced greater BW loss of approximately 13 kg, representing reductions of 11–13%. BC analysis confirmed that FBM loss was the dominant driver of these changes, with semaglutide alone reducing FBM by about 4 kg, compared with 9 kg reductions observed in both the VLCD and combined groups. Importantly, LBM decreased modestly across all interventions, without significant between-group differences, suggesting that the preferential reduction in adipose tissue was preserved irrespective of treatment allocation.
In contrast, dulaglutide treatment appears to exert a more modest effect on BW reduction, and its use has largely been restricted to Asian populations. In the study by Chen et al. [31], treatment with dulaglutide 1.5 mg once weekly for 3 months in patients with overweight or obesity and T2DM resulted in a meaningful reduction in BW of approximately 4%, accompanied by significant decreases in visceral fat area and total FBM. Importantly, although LBM and SMM showed slight absolute declines, their relative proportions within total BC increased. A similar efficacy in BW reduction was observed in the study by Seko et al. [32], where patients with NAFLD and T2DM received 12 weeks of treatment with dulaglutide 0.75 mg once weekly. Notably, BC analysis demonstrated a significant reduction in total FBM, while SMM and muscle distribution were preserved throughout the intervention. In turn, in the study by Zhang et al. [33], women with overweight and obesity with PCOS experienced a mean BW reduction of about 7% from baseline after intervention with either a calorie-restricted diet alone or in combination with dulaglutide 1.5 mg once weekly. While the overall magnitude of BW loss and accompanying decreases in VAT, total FBM, and LBM were comparable across groups, the addition of dulaglutide allowed participants to reach the BW loss target in a shorter time.
Exenatide treatment was also consistently associated with significant reductions in BW, BMI, and total FBM, often accompanied by favorable changes in fat distribution. In the study by Agcakaya et al. [34], a six-month exenatide regimen in metformin-treated patients with T2DM resulted in a mean BW reduction of > 7 kg and a BMI decrease of 2.8 kg/m². These changes were paralleled by marked decreases in total, abdominal, leg, and arm fat percentage, along with increases in FFM and total body muscle percentage. Improvements in visceral adiposity exceeded those observed in the comparator group receiving a sodium-glucose cotransporter 2 (SGLT2) inhibitor. Evidence also supports a beneficial effect of exenatide on ectopic fat depots, with potential mechanisms that may not be entirely weight dependent. In patients with T2DM and hepatic steatosis, Cuthbertson et al. [35] reported that a 6-month exenatide-based therapy produced a 42% relative reduction in intrahepatic lipid content, accompanied by a mean BW loss of 5 kg and significant decreases in both abdominal subcutaneous and visceral fat volumes. In contrast, Mittag-Roussou et al. [36], in a real-world cohort treated with GLP-1 RAs including exenatide, observed a mean BW loss of 2.5 kg and a BMI reduction of 0.9 kg/m² without a significant change in intrahepatic lipid content, reflecting variability in hepatic responses across populations.
These findings collectively emphasize that while GLP-1RAs are effective in reducing FBM, strategies to preserve or enhance SMM, such as resistance training and adequate protein intake, should be integral to obesity management. Beyond quantitative preservation, maintaining skeletal muscle function, including strength and metabolic capacity, remains a critical therapeutic goal in ensuring long-term health outcomes. While LBM loss appears to be less pronounced than FBM loss in many studies, the clinical significance of even modest reductions in skeletal muscle remains uncertain, particularly in older adults or individuals at risk of sarcopenia. Importantly, lean tissue has a higher metabolic rate than adipose tissue, and its preservation is critical for sustaining metabolic health, physical function, and long-term weight maintenance. The distinction between adaptive and maladaptive muscle loss is central to understanding the quality, not just the quantity, of BW loss achieved with GLP-1 RA-based therapies [37, 38]. Given the emerging concern around potential muscle loss, strategies to mitigate reductions in FFM during pharmacologically induced BW loss should be prioritized. Nutritional interventions, especially increased protein intake, may offer protective effects against muscle loss, though GLP-1 RAs therapies may inadvertently suppress protein-rich food consumption. Likewise, resistance exercise remains one of the most effective tools for preserving muscle mass and strength during caloric restriction [37].
Cardiometabolic parameters during GLP-1 RA treatment
GLP-1 RAs have also demonstrated important cardioprotective benefits that extend beyond their impact on BW loss. Emerging evidence indicates their potential role in the management of diverse obesity-related comorbidities, including metabolic dysfunction-associated steatotic liver disease, obstructive sleep apnea, polycystic ovary syndrome, neurodegenerative disorders, and even substance use disorders. While BW reduction likely contributes to improvements in conditions, such as hepatic steatosis or sleep apnea, GLP-1 RAs may also exert direct disease-specific effects, particularly through central mechanisms implicated in neurodegeneration and addiction [39]. Consistent with these observations, patients included in the studies analyzed in this systematic review frequently reported significant cardiometabolic benefits in addition to BW loss. These were reflected in improvements in lipid profiles and glycemic control, with notable reductions in HbA1c and insulin requirements, although the magnitude of benefit varied by specific GLP-1 RA, dosage, and duration of follow-up.
Factors associated with response to GLP-1 RA treatment
Older adults and GLP-1 RA treatment response
In elderly patients with overweight or obesity with T2DM, Perna et al. [40] reported that liraglutide 3.0 mg over 24 weeks achieved modest BW loss of about 2.5% but substantial reduction in FBM, particularly in the android region. Importantly, LBM remained largely stable, with slight gains in leg and arm FFM in some patients, resulting in minimal changes in skeletal muscle index and no cases of sarcopenia. Also, in elderly diabetic patients with obesity, semaglutide therapy led to a moderate but clinically relevant reduction in BW and BMI after 3 months. BC analysis revealed that these changes were primarily driven by significant reductions in FBM and FBM percentage, while BMC and extracellular fluid balance remained unaffected. Importantly, SMM declined slightly in absolute terms, yet its proportion relative to total BW was preserved. Detailed segmental analysis further confirmed the stability of both upper and lower limb muscle mass as well as the ratio of lower-to-upper extremity musculature, indicating that semaglutide facilitated selective adiposity reduction while maintaining muscular distribution [41].
Type 2 diabetes and GLP-1 RA treatment response
It is also important to note that therapeutic responses may differ between patients with and without T2DM, a difference likely driven by several interrelated mechanisms [42]. Physiologically, insulin resistance and compensatory hyperinsulinemia in T2DM may attenuate the incretin effect of GLP-1 RAs through impaired insulin signaling or reduced GLP-1 receptor responsiveness. Also, as an anabolic hormone, insulin promotes fat storage, and chronic hyperinsulinemia, commonly observed in T2DM, further stimulates lipogenesis while suppressing lipolysis, thereby counteracting BW reduction. Additionally, improved glycemic control with GLP-1 RAs in T2DM patients may reduce glycosuria, a process known as “glycemic buffering”, which reduces caloric loss through urine and offsets part of the energy deficit induced by treatment [43,44,45]. Concomitant use of weight-promoting medications, such as insulin or sulfonylureas, may further blunt the weight loss effects of GLP-1 RAs [45]. Additional contributors may include a longer duration of obesity, older age, lower adherence to exercise, and possible behavioral factors in the T2DM population [46]. Finally, individual differences in baseline metabolic rate and prior exposure to dietary or behavioral weight loss strategies may influence the magnitude of BW reduction achieved with GLP-1 RAs, highlighting the complexity of therapeutic response in patients with T2DM [45].
Sex differences in GLP-1 RA treatment response
Beyond diabetes status, growing evidence also highlights the importance of sex differences in obesity, particularly regarding their impact on the effectiveness and tolerability of GLP-1 RA treatment. Female sex is widely recognized as an independent factor associated with greater BW loss achievement following treatment with GLP-1 RAs, a superiority observed in the majority of studies [47, 48]. This phenomenon may be partly explained by biological differences such as variations in sex hormone levels, pancreatic β-cell composition, and gene expression patterns related to insulin secretion and glucose metabolism [49]. For example, estrogen signaling has been shown to enhance the anorexigenic effects of GLP-1 RAs by modulating central pathways involved in food reward, which could account for the more pronounced weight loss observed in premenopausal women [49, 50]. Additionally, epigenetic differences, such as increased methylation of protective genes, such as DUSP9, in females, may influence insulin sensitivity and drug response [49, 51]. However, clinical outcomes are complicated by behavioral factors, including lower adherence rates reported among women, which may obscure the true extent of sex-related efficacy differences [52]. Given the heterogeneity in study populations and the predominance of post hoc analyses, further prospective research is essential to clarify these mechanisms and to evaluate whether personalized, sex-specific approaches to GLP-1 RA therapy could improve obesity treatment outcomes. All but one of the studies included in the systematic review did not provide sex-disaggregated data, limiting the interpretation of the impact of GLP-1 RAs on the measured outcomes. A prospective study assessed the impact of six months of liraglutide treatment on BC and cardiometabolic parameters in patients with metabolic syndrome, with analyses stratified by sex and compared to a control group treated with sibutramine. Both men and women receiving liraglutide showed significant improvements in BW loss, AC, and FBM, particularly trunk fat mass, a key parameter measured by BIA. Importantly, women exhibited a more pronounced reduction in AC and FMT, whereas men demonstrated significant decreases in overall BW and total FBM, as well as in regional fat, particularly in the arms. These results reflect sex-specific patterns of fat distribution and differential response to liraglutide, with reductions in visceral adiposity strongly correlated with decreases in AC across both sexes. In turn, the overall BW loss, defined as achieving 5% and 10% reduction, was similar between men and women. Nonetheless, the distinct regional and quantitative differences in fat loss between the sexes highlight the need to consider sex-specific effects in obesity treatment [53].
Study limitations
This meta-analysis has several limitations that should be considered when interpreting the findings. Most notably, the number of included studies providing detailed data on both BC and cardiometabolic parameters was relatively limited. While strict inclusion criteria ensured methodological quality, they may have reduced the breadth of eligible evidence, limiting the scope of subgroup analyses and the generalizability of certain findings. A second important limitation relates to the substantial heterogeneity observed across studies. This variability likely reflects differences in study populations, such as the presence or absence of T2DM, degree of obesity, sex distribution, and comorbid conditions, as well as differences in intervention characteristics, including the type, dose, and duration of GLP-1 RA therapy. Although random-effects models were employed to account for between-study variance, some unmeasured confounders may have influenced the results. Also, LBM reduction was often assessed using BIA or DXA, both of which have limitations in distinguishing between muscle, organ mass, and extracellular fluid. As a result, interpretations regarding skeletal muscle preservation or loss must be made with caution, particularly in the absence of direct assessments of muscle strength or function. Moreover, differences in outcome reporting, such as the use of absolute versus relative changes, or inconsistent definitions of endpoints like visceral adiposity or insulin resistance, further limited the ability to standardize data extraction and synthesis. Also, several studies lacked full disclosure of variance measures or raw data, preventing the inclusion of potentially relevant findings. Finally, publication bias cannot be excluded, especially given the increasing clinical interest in GLP-1RAs and the greater likelihood of publishing studies with favorable outcomes. Despite attempts to minimize bias through a systematic and comprehensive search strategy, unpublished or negative studies may have been overlooked.
Conclusions
This meta-analysis highlights the substantial and multidimensional clinical benefits of GLP-1 RAs therapy in individuals with overweight or obesity, with or without T2DM. Across all treatment durations, GLP-1 RAs consistently produced significant improvements in anthropometric parameters, including BW, BMI, and WC, while also inducing favorable alterations in BC through pronounced reductions in FBM and VAT. Importantly, the reduction in LBM was modest relative to the overall BW loss, suggesting that GLP-1 RAs favor selective adipose tissue reduction over loss of lean tissue. The most pronounced improvements in BC were observed after 3 and 6 months of treatment, whereas after 12 months these beneficial effects tended to diminish. Notably, the observed variability in efficacy between agents, particularly in the early phases of treatment, emphasizes the importance of individualized therapeutic strategies, tailored to specific clinical goals, baseline metabolic profiles, and patient preferences. Looking ahead, further research should aim to define the most effective combinations of pharmacotherapy and lifestyle interventions, with a focus on preserving lean mass and sustaining long-term metabolic health.
Data availability
No datasets were generated or analyzed during the current study.
References
Islam ANMS, Sultana H, Nazmul Hassan Refat M, Farhana Z, Abdulbasah Kamil A, Meshbahur Rahman M. The global burden of overweight-obesity and its association with economic status, benefiting from STEPs survey of WHO member states: A meta-analysis. Prev Med Rep. 2024;46:102882.
Rubino F, Cummings DE, Eckel RH, Cohen RV, Wilding JPH, Brown WA, et al. Definition and diagnostic criteria of clinical obesity. Lancet Diab Endocrinol. 2025;13:221–62.
Masood B, Moorthy M. Causes of obesity: a review. Clin Med (Lond). 2023;23:284–91.
Powell-Wiley TM, Poirier CP, Burke VCLE, Després JP, Gordon-Larsen P, Lavie CJ, et al. Obesity and Cardiovascular Disease. Circulation. 2021;143:e984–1010.
Scully T, Ettela A, LeRoith D, Gallagher EJ. Obesity, Type 2 Diabetes, and Cancer Risk. Front Oncol. 2021;10:615375.
Sarwer DB, Hanson AJ, Voeller J, Steffen K. Obesity and Sexual Functioning. Curr Obes Rep. 2018;7:301–7.
Elmaleh-Sachs A, Schwartz JL, Bramante CT, Nicklas JM, Gudzune KA, Jay M. Obesity Management in Adults A Review. JAMA. 2023;330:2000–15.
Liu QK. Mechanisms of action and therapeutic applications of GLP-1 and dual GIP/GLP-1 receptor agonists. Front Endocrinol (Lausanne). 2024;15:1431292.
Drucker DJ. Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab. 2018;27:740–56.
Hammad BF, Zafar N, Ullah M, Faisal SJ, Iftikhar F, Waheed H, et al. Exploring the multifaceted roles of GLP-1 receptor agonists; a comprehensive review. Front Clin Diab Health. 2025;6:1590530.
Zheng Z, Zong Y, Ma Y, Tian Y, Pang Y, Zhang C, et al. Glucagon-like peptide-1 receptor: mechanisms and advances in therapy. Signal Transduct Target Ther. 2024;9:234.
Szekeres Z, Nagy A, Jahner K, Szabados E. Impact of Selected Glucagon-like Peptide-1 Receptor Agonists on Serum Lipids, Adipose Tissue, and Muscle Metabolism-A Narrative Review. Int J Mol Sci. 2024;25:8214.
An SM, Cho SH, Yoon JC. Adipose Tissue and Metabolic Health. Diab Metab J. 2023;47:595–611.
Gurjar AA, Kushwaha S, Chattopadhyay S, Das N, Pal S, China SP, et al. Long acting GLP-1 analog liraglutide ameliorates skeletal muscle atrophy in rodents. Metabolism. 2020;103:154044.
Abdulla H, Phillips B, Smith K, Wilkinson D, Atherton PJ, Idris I. Physiological mechanisms of action of incretin and insulin in regulating skeletal muscle metabolism. Curr Diab Rev. 2014;10:327–35.
Xiang J, Qin L, Zhong J, Xia N, Liang Y. GLP-1RA Liraglutide and Semaglutide Improves Obesity-Induced Muscle Atrophy via SIRT1 Pathway. Diab Metab Syndr Obes. 2023;16:2433–46.
Jiao R, Lin C, Cai X, Wang J, Wang Y, Lv F, et al. Characterizing body composition modifying effects of a glucagon-like peptide 1 receptor-based agonist: A meta-analysis. Diab, Obes Metab. 2025;27:259–67.
Karakasis P, Patoulias D, Fragakis N, Mantzoros CS. Effect of glucagon-like peptide-1 receptor agonists and co-agonists on body composition: Systematic review and network meta-analysis. Metab - Clin Exp. 2025;164:156113.
Reed RL, Pearlmutter L, Yochum K, Meredith KE, Mooradian AD. The relationship between muscle mass and muscle strength in the elderly. J Am Geriatr Soc. 1991;39:555–61.
Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393:2636–46.
Gatto A, Liu K, Milan N, Wong S. The Effects of GLP-1 Agonists on Musculoskeletal Health and Orthopedic Care. Curr Rev Musculoskelet Med. 2025;18:469–80.
Zakaria H, Alshehhi S, Caccelli M, Ozkan C, Kattan J, Jafaar Z, et al. Effectiveness of a hybrid approach in integrating GLP-1 agonists and lifestyle guidance for obesity and pre-diabetes management: RWE retrospective study. Metab Open. 2024;22:100283.
Yu D, Zou M, Pan Q, Song Y, Li M, Zhang X, et al. Effects of liraglutide or lifestyle interventions combined with other antidiabetic drugs on abdominal fat distribution in people with obesity and type 2 diabetes mellitus evaluated by the energy spectrum ct: A prospective randomized controlled study. Front Endocrinol. 2022;13:951570.
Muñoz MPS, Blandón JDR, Gutierrez ISC, Mendoza CMM, Aguiñaga MSA, Orozco CAO. Liraglutide effectiveness in preoperative weight-loss for patients with severe obesity undergoing bariatric-metabolic surgery. Updates Surg. 2024;76:2277–83.
Capristo E, Panunzi S, De Gaetano A, Raffaelli M, Guidone C, Iaconelli A, et al. Intensive lifestyle modifications with or without liraglutide 3mg vs. sleeve gastrectomy: A three-arm non-randomised, controlled, pilot study. Diab Metab. 2018;44:235–42.
Rodríguez Jiménez B, Rodríguez de Vera Gómez P, Belmonte Lomas S, Mesa Díaz ÁM, Caballero Mateos I, Galán I, et al. Transforming body composition with semaglutide in adults with obesity and type 2 diabetes mellitus. Front Endocrinol (Lausanne). 2024;15:1386542.
Xiang J, Ding XY, Zhang W, Zhang J, Zhang YS, Li ZM, et al. Clinical effectiveness of semaglutide on weight loss, body composition, and muscle strength in Chinese adults. Eur Rev Med Pharm Sci. 2023;27:9908–15.
Pantanetti P, Ronconi V, Sguanci M, Palomares SM, Mancin S, Tartaglia FC, et al. Oral Semaglutide in Type 2 Diabetes: Clinical–Metabolic Outcomes and Quality of Life in Real-World Practice. J Clin Med. 2024;13:4752.
Volpe S, Lisco G, Fanelli M, Racaniello D, Colaianni V, Lavarra V, et al. Oral semaglutide improves body composition and preserves lean mass in patients with type 2 diabetes: a 26-week prospective real-life study. Front Endocrinol. 2023;14:1240263.
Anyiam O, Phillips B, Quinn K, Wilkinson D, Smith K, Atherton P, et al. Metabolic effects of very-low calorie diet, Semaglutide, or combination of the two, in individuals with type 2 diabetes mellitus. Clin Nutr. 2024;43:1907–13.
Chen S, Wang X, Jin Y, Chen X, Song Q, Wei G, et al. Assessment of Changes in Body Composition After 3 Months of Dulaglutide Treatment. Diab Metab Syndr Obes. 2024;17:1301–8.
Seko Y, Sumida Y, Tanaka S, Mori K, Taketani H, Ishiba H, et al. Effect of 12-week dulaglutide therapy in Japanese patients with biopsy-proven non-alcoholic fatty liver disease and type 2 diabetes mellitus. Hepatol Res. 2017;47:1206–11.
Zhang Y, Qu Z, Lu T, Shao X, Cai M, Dilimulati D, et al. Effects of a Dulaglutide plus Calorie-Restricted Diet versus a Calorie-Restricted Diet on Visceral Fat and Metabolic Profiles in Women with Polycystic Ovary Syndrome: A Randomized Controlled Trial. Nutrients. 2023;15:556.
Agcakaya E, Mutlu HH, Erbakan A, Sargin M. Comparison of the Impact of SGLT2-Inhibitors and Exenatide on Body Fat Composition. J Coll Physicians Surg Pak. 2023;33:308–13.
Cuthbertson DJ, Irwin A, Gardner CJ, Daousi C, Purewal T, Furlong N, et al. Improved Glycaemia Correlates with Liver Fat Reduction in Obese, Type 2 Diabetes, Patients Given Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists. PLOS ONE. 2012;7:e50117.
Mittag-Roussou V, Wagenpfeil S, Lammert F, Stokes CS. Noninvasive monitoring of liver fat during treatment with GLP-1 analogues and SGLT-2 inhibitors in a real-world setting. Endocrinol Diab Metab. 2020;3:e00131.
Mechanick JI, Butsch WS, Christensen SM, Hamdy O, Li Z, Prado CM, et al. Strategies for minimizing muscle loss during use of incretin-mimetic drugs for treatment of obesity. Obes Rev. 2025;26:e13841.
Stefanakis K, Kokkorakis M, Mantzoros CS. The impact of weight loss on fat-free mass, muscle, bone and hematopoiesis health: Implications for emerging pharmacotherapies aiming at fat reduction and lean mass preservation. Metabolism. 2024;161:156057.
Moiz A, Filion KB, Tsoukas MA, Yu OHY, Peters TM, Eisenberg MJ. The expanding role of GLP-1 receptor agonists: a narrative review of current evidence and future directions. eClinicalMedicine. 2025;86:103363.
Perna S, Guido D, Bologna C, Solerte SB, Guerriero F, Isu A, et al. Liraglutide and obesity in elderly: efficacy in fat loss and safety in order to prevent sarcopenia. A perspective case series study. Aging Clin Exp Res. 2016;28:1251–7.
Ozeki Y, Masaki T, Kamata A, Miyamoto S, Yoshida Y, Okamoto M, et al. The Effectiveness of GLP-1 Receptor Agonist Semaglutide on Body Composition in Elderly Obese Diabetic Patients: A Pilot Study. Medicines. 2022;9:47.
Vosoughi K, Salman Roghani R, Camilleri M. Effects of GLP-1 agonists on proportion of weight loss in obesity with or without diabetes: Systematic review and meta-analysis. Obes Med. 2022;35:100456.
Janssen JAMJL. Hyperinsulinemia and Its Pivotal Role in Aging, Obesity, Type 2 Diabetes, Cardiovascular Disease and Cancer. Int J Mol Sci. 2021;22:7797.
Janssen JAMJL. Overnutrition, Hyperinsulinemia and Ectopic Fat: It Is Time for A Paradigm Shift in the Management of Type 2 Diabetes. Int J Mol Sci. 2024;25:5488.
Hong B, Kim H, Lee D, Kim K. Weight Loss Effects of Once-Weekly Semaglutide 2.4 mg in Adults with and Without Type 2 Diabetes: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2025;18:1058.
Jensterle M, Rizzo M, Haluzík M, Janež A. Efficacy of GLP-1 RA Approved for Weight Management in Patients With or Without Diabetes: A Narrative Review. Adv Ther. 2022;39:2452–67.
Marassi M, Cignarella A, Russo GT, Nollino L, Strazzabosco M, Marzullo P, et al. Sex differences in the weight response to GLP-1RA in people with type 2 diabetes. A long-term longitudinal real-world study. Pharmacol Res. 2025;219:107866.
Börchers S, Skibicka KP. GLP-1 and Its Analogs: Does Sex Matter?. Endocrinology. 2025;166:bqae165.
Rentzeperi E, Pegiou S, Koufakis T, Grammatiki M, Kotsa K. Sex Differences in Response to Treatment with Glucagon-like Peptide 1 Receptor Agonists: Opportunities for a Tailored Approach to Diabetes and Obesity Care. J Pers Med. 2022;12:454.
Muscogiuri G, Verde L, Vetrani C, Barrea L, Savastano S, Colao A. Obesity: a gender-view. J Endocrinol Invest. 2024;47:299–306.
Gannon M, Kulkarni RN, Tse HM, Mauvais-Jarvis F. Sex differences underlying pancreatic islet biology and its dysfunction. Mol Metab. 2018;15:82.
Weiss T, Carr RD, Pal S, Yang L, Sawhney B, Boggs R, et al. Real-World Adherence and Discontinuation of Glucagon-Like Peptide-1 Receptor Agonists Therapy in Type 2 Diabetes Mellitus Patients in the United States. Patient Prefer Adherence. 2020;14:2337–45.
Freitas FPC, Rodrigues CEM. Effect of liraglutide on cardiometabolic profile and on bioelectrical impedance analysis in patients with obesity and metabolic syndrome. Sci Rep. 2023;13:13090.
Gao L, Huang H, Zhang L, Zhang N, Fu Y, Zhu D, et al. Comparison of Beinaglutide Versus Metformin for Weight Loss in Overweight and Obese Non-diabetic Patients. Exp Clin Endocrinol Diab. 2022;130:358–67.
Jensterle M, Kocjan T, Kravos NA, Pfeifer M, Janez A. Short-term intervention with liraglutide improved eating behavior in obese women with polycystic ovary syndrome. Endocr Res. 2015;40:133–8.
Jensterle M, Kravos NA, Pfeifer M, Kocjan T, Janez A. A 12-week treatment with the long-acting glucagon-like peptide 1 receptor agonist liraglutide leads to significant weight loss in a subset of obese women with newly diagnosed polycystic ovary syndrome. Hormones (Athens). 2015;14:81–90.
Jensterle M, Salamun V, Kocjan T, Vrtacnik Bokal E, Janez A. Short term monotherapy with GLP-1 receptor agonist liraglutide or PDE 4 inhibitor roflumilast is superior to metformin in weight loss in obese PCOS women: a pilot randomized study. J Ovarian Res. 2015;8:32.
Li CJ, Yu Q, Yu P, Yu TL, Zhang QM, Lu S, et al. Changes in liraglutide-induced body composition are related to modifications in plasma cardiac natriuretic peptides levels in obese type 2 diabetic patients. Cardiovasc Diabetol. 2014;13:36.
Akyay Ö, Selek A, Tarkun İ, Şahi̇n T, Cantürk Z, Arslan B, et al. Evaluation of Exenatide Versus Insulin Glargine Treatment’s Impact on Brown Adipose Tissue Markers and Epicardial Adipose Tissue. Med J Bakirkoy. 2023;19:276–82.
Elkind-Hirsch KE, Chappell N, Seidemann E, Storment J, Bellanger D. Exenatide, Dapagliflozin, or Phentermine/Topiramate Differentially Affect Metabolic Profiles in Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2021;106:3019–33.
Feng WH, Bi Y, Li P, Yin TT, Gao CX, Shen SM, et al. Effects of liraglutide, metformin and gliclazide on body composition in patients with both type 2 diabetes and non-alcoholic fatty liver disease: A randomized trial. J Diab Investig. 2019;10:399–407.
Volpe S, Lisco G, Fanelli M, Racaniello D, Colaianni V, Triggiani D, et al. Once-Weekly Subcutaneous Semaglutide Improves Fatty Liver Disease in Patients with Type 2 Diabetes: A 52-Week Prospective Real-Life Study. Nutrients. 2022;14:4673.
Nakaguchi H, Kondo Y, Kyohara M, Konishi H, Oiwa K, Terauchi Y. Effects of liraglutide and empagliflozin added to insulin therapy in patients with type 2 diabetes: A randomized controlled study. J Diab Investig. 2020;11:1542–50.
Rondanelli M, Perna S, Astrone P, Grugnetti A, Solerte SB, Guido D. Twenty-four-week effects of liraglutide on body composition, adherence to appetite, and lipid profile in overweight and obese patients with type 2 diabetes mellitus. Patient Prefer Adherence. 2016;10:407–13.
Uchiyama S, Sada Y, Mihara S, Sasaki Y, Sone M, Tanaka Y. Oral Semaglutide Induces Loss of Body Fat Mass Without Affecting Muscle Mass in Patients With Type 2 Diabetes. J Clin Med Res. 2023;15:377–83.
Volpe S, Lisco G, Racaniello D, Fanelli M, Colaianni V, Vozza A, et al. Once-Weekly Semaglutide Induces an Early Improvement in Body Composition in Patients with Type 2 Diabetes: A 26-Week Prospective Real-Life Study. Nutrients. 2022;14:2414.
McCrimmon RJ, Catarig AM, Frias JP, Lausvig NL, le Roux CW, Thielke D, et al. Effects of once-weekly semaglutide vs once-daily canagliflozin on body composition in type 2 diabetes: a substudy of the SUSTAIN 8 randomised controlled clinical trial. Diabetologia. 2020;63:473–85.
Pantanetti P, Cangelosi G, Alberti S, Di Marco S, Michetti G, Cerasoli G, et al. Changes in body weight and composition, metabolic parameters, and quality of life in patients with type 2 diabetes treated with subcutaneous semaglutide in real-world clinical practice. Front Endocrinol (Lausanne). 2024;15:1394506.
Sandsdal RM, Juhl CR, Jensen SBK, Lundgren JR, Janus C, Blond MB, et al. Combination of exercise and GLP-1 receptor agonist treatment reduces severity of metabolic syndrome, abdominal obesity, and inflammation: a randomized controlled trial. Cardiovasc Diabetol. 2023;22:41.
Vedtofte L, Bahne E, Foghsgaard S, Bagger JI, Andreasen C, Strandberg C, et al. One Year’s Treatment with the Glucagon-Like Peptide 1 Receptor Agonist Liraglutide Decreases Hepatic Fat Content in Women with Nonalcoholic Fatty Liver Disease and Prior Gestational Diabetes Mellitus in a Randomized, Placebo-Controlled Trial. J Clin Med. 2020;9:3213.
Yabe D, Kawamori D, Seino Y, Oura T, Takeuchi M. Change in pharmacodynamic variables following once-weekly tirzepatide treatment versus dulaglutide in Japanese patients with type 2 diabetes (SURPASS J-mono substudy). Diab, Obes Metab. 2023;25:398–406.
Funding
The authors received no external funding. The authors received no financial support from pharmaceutical companies for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
Conceptualization: Dawid Gruszczyński, Aleksandra Derwich-Rudowicz, Nadia Sawicka-Gutaj; Literature search: Michal Krenz, Anita Kumar, Pei-Yin Lu; Formal analysis: Dawid Gruszczyński, Kacper Nijakowski; Writing - original draft preparation: Dawid Gruszczyński, Kacper Nijakowski; Writing - review and editing: Nadia Sawicka-Gutaj; Supervision: Marek Ruchała, Nadia Sawicka-Gutaj.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sawicka-Gutaj, N., Gruszczyński, D., Nijakowski, K. et al. GLP-1 agonists and changes in body mass and composition in adults with overweight or obesity with or without type 2 diabetes mellitus: a systematic review and meta-analysis. Int J Obes (2026). https://doi.org/10.1038/s41366-026-02088-1
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41366-026-02088-1
