
Abstract
The EAT-Lancet diet has been recently recommended for its potential health and environmental benefits. Here, leveraging data from the UK Biobank, we performed a comparative analysis to examine the associations of adherence to the EAT-Lancet diet versus traditional plant-based diets with biological aging and further assess the mediating role of metabolomic signatures specific to dietary patterns. Compared with the overall or healthful plant-based diet index, higher adherence to the EAT-Lancet diet was more strongly associated with decreased KDM-BA and PhenoAge acceleration and increased telomere length. In contrast, a higher unhealthful plant-based diet index was associated with accelerated biological aging. We identified substantial metabolomic variation in relation to different dietary patterns. The diet-specific metabolomic signatures mediated 26.9–63.0% of the associations between dietary patterns and biological aging. Our findings suggest the potential benefits of adopting the EAT-Lancet and plant-based diets in promoting healthy aging and highlight the potential of metabolomic signatures for informing personalized nutrition interventions.
Similar content being viewed by others

Introduction
Aging is a multifaceted process characterized by accumulated damage of the cells and tissues, which leads to functional decline and increased vulnerability to chronic diseases and mortality1. With the expanding aging population worldwide, accelerated aging is becoming a tremendous public health challenge. Notably, individuals with the same chronological age may have different biological aging rates and risks of developing age-related disorders. Apart from traditional indicators such as telomere length, several alternative measures have been established to quantify the biological aging process2,3. Among them, the composite clinical parameter-based algorithms have shown excellent capabilities of predicting morbidity and mortality4,5. While chronological aging is inevitable, the biological aging process can be slowed down or reversed through pharmacological and lifestyle interventions for extending lifespan and healthspan6,7. As one of the major modifiable risk factors, diet has a significant impact on age-related health outcomes8. Several studies have reported that adherence to healthy dietary patterns, including the Dietary Approaches to Stop Hypertension (DASH) diet, Alternative Mediterranean Index (aMED) diet, and Healthy Eating Index-2015 (HEI-2015) diet, could slow down the aging process9,10,11,12.
Environmental impact should be a critical consideration when developing a healthy diet as food production is the leading contributor to climate change13,14. For example, about 30% of greenhouse gas emissions and 70% of freshwater use are primarily driven by meat and dairy production15. Recent studies have increasingly focused on dietary patterns that aim to reduce environmental burden while promoting human health, such as plant-based diets16 and the EAT-Lancet diet17. Compared with plant-based diets that are based on distributions of population intake18, the EAT-Lancet diet provides more specific recommendation intake levels for food groups, which is basically characterized by plenty of vegetables, fruits, legumes, whole grains, and nuts, moderate seafood, poultry, and dairy, as well as restricted red meat, sugary foods, and saturated fats. Mounting evidence has suggested health benefits from adhering to the plant-based diets and EAT-Lancet diet in decreasing risks of multiple diseases and mortality19,20,21. However, whether these dietary patterns are associated with biological aging is unclear, and how the EAT-Lancet diet compares with plant-based dietary patterns in relation to biological aging remains to be elucidated. In addition, metabolomic biomarkers represent the downstream end products of gene transcription and translation22,23. Metabolomic signatures linked with adherence to specific dietary patterns may reflect the intake of particular food groups or their constituents, as well as the physiological responses to food-derived metabolites and their interactions with endogenous metabolic processes24. Thus, delineating diet-specific metabolomic profiles may offer mechanistic insights into the possible diet-biological aging association. However, the metabolomic changes associated with EAT-Lancet and plant-based diets as well as their roles in linking these dietary patterns and biological aging have not yet been explored.
In this study, we utilized multiple dimensions of biological aging metrics, including telomere length (TL) and two biological age (BA) algorithms validated in the UK Biobank, to examine the associations of the EAT-Lancet and plant-based diets with biological aging in mid- to late-life. Furthermore, we identified metabolomic signatures specific to different dietary patterns and assessed whether such metabolomic signatures were associated with biological aging. Finally, we evaluated the mediation effect of metabolites in the relationships between dietary patterns and biological aging. The main content of this study is visualized in Fig. 1.

PDI plant-based diet index; hPDI healthy plant-based diet index; uPDI unhealthy plant-based diet index; BMI body mass index; KDM-BA Klemera-Doubal biological age; PhenoAge phenotypic age.
Results
Population characteristics
We included a total of 87,282 participants from the UK Biobank (mean age 56.1 years, 55.3% female) (Table 1). The mean (SD) values at baseline were 24.1 (4.5) for EAT-Lancet diet index, 51.1 (6.0) for PDI, 53.6 (6.5) for hPDI, and 53.9 (6.7) for uPDI. The correlations between the four dietary pattern scores were modest (r ranged from −0.42 to 0.47). Participants with higher EAT-Lancet diet index tended to be women and have healthier lifestyles, lower BMI, a lower prevalence of cardiovascular disease, diabetes, high cholesterol, and hypertension (Table S1). Meanwhile, participants with higher overall PDI and hPDI but lower uPDI scores were more likely to have healthier lifestyle patterns, lower BMI, and accelerated biological aging. Total energy intake was higher among participants with higher overall PDI but lower in those with higher hPDI and uPDI (Tables S2–S4).
Association of individual dietary patterns with biological aging
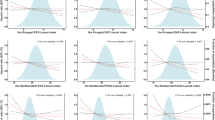
Tables 2 and S5 show the association between four dietary patterns and biological aging. The EAT-Lancet index, PDI, and hPDI were inversely associated with KDM-BA and PhenoAge acceleration but positively associated with TL. Each 1-SD increase in the EAT-Lancet diet index was linked to decreased KDM-BA and PhenoAge acceleration of −0.53 (β = −0.53 [95% CI: −0.57, −0.49]) and −0.43 (β = −0.43 [−0.46, −0.39]) years, respectively, and elevated TL of 0.30% (0.21%, 0.39%). The effect estimates became less remarkable for PDI (KDM-BA acceleration: −0.38 [−0.42, −0.34] years; PhenoAge acceleration: −0.21 [−0.24, −0.18] years; TL: 0.10% [0.01%, 0.19%]) and hPDI (KDM-BA acceleration: −0.33 [−0.37, −0.29] years; PhenoAge acceleration: −0.33 [−0.37, −0.30] years; TL: 0.12% [0.04%, 0.21%]). On the contrary, higher uPDI was associated with an increase in KDM-BA (0.26 [0.22, 0.30] years) and PhenoAge acceleration (0.28 [0.24, 0.31] years) and a decrease in TL (−0.12% [−0.21%, −0.04%]). The dose-response analysis showed nonlinear relationships between the EAT-Lancet diet index and KDM-BA acceleration (Pnonlinearity = 0.001) and TL (Pnonlinearity = 0.015) (Fig. S1) as well as between hPDI and KDM-BA acceleration (Pnonlinearity < 0.001) (Fig. S2). Specifically, higher EAT-Lancet diet scores were associated with progressively greater reductions in KDM-BA acceleration and increases in TL, and the inverse association between hPDI and KDM-BA became stronger with higher hPDI. Similar results were observed when comparing the highest to the lowest quartile of dietary scores, with the most pronounced associations found for the EAT-Lancet diet index (KDM-BA acceleration: −1.22 [−1.33, −1.10] years; PhenoAge acceleration: −1.05 [−1.14, −0.96] years; TL: 0.84% [0.59%, 1.09%]). Among a subset of participants with available revisit biological aging data (median follow-up 4.22 years), we calculated the biological aging rate and detected that each 1-SD increase in the EAT-Lancet diet index was associated with a more modest rate of biological aging (KDM-BA acceleration: −0.09 [95% CI: [−0.14, −0.04] years; PhenoAge acceleration: −0.06 [−0.10, −0.01] years), whereas higher uPDI was related to an accelerated rate of biological aging (PhenoAge acceleration: 0.05 [0.01, 0.09] years) after controlling for the baseline aging acceleration levels (Table S6). Changes in PDI and hPDI showed a nonsignificant association with biological aging rate.
For subgroups of plant-based diets (Table S7), each 1-SD increase in healthy plant-based item intake was associated with decreased KDM-BA (−0.49 [−0.53, −0.45] years) and PhenoAge acceleration (−0.39 [−0.42, −0.35] years and an increase in TL (0.17% [0.08%, 0.26%]). In contrast, unhealthy plant-based item intake showed no significant associations with KDM-BA (−0.03 [−0.07, 0.01] years) or TL (−0.03% [−0.12%, 0.06%]), but was positively associated with PhenoAge acceleration (0.12 [0.09, 0.16] years). Animal-based item intake was related to increased KDM-BA (0.05 [0.01, 0.09] years) and PhenoAge acceleration (0.04 [0.01, 0.08] years), with no association for TL (0.01% [−0.08%, 0.09%]). In component-wise analyses (Table S8), fruits were most strongly associated with decreased KDM-BA and PhenoAge acceleration and increased TL, whereas potatoes and meat were most strongly associated with increased KDM-BA and PhenoAge acceleration and decreased TL.
Joint and interaction effect of genetic susceptibility and dietary patterns
We observed a gradient association between PRS for KDM-BA, PhenoAge, and TL and accelerated biological aging (Table S9). Furthermore, we explored the joint effect of the three PRS and different dietary patterns on biological aging (Fig. 2). Compared to those with high PRS and low EAT-Lancet diet index, participants with low PRS and high EAT-Lancet diet index had the lowest biological aging acceleration (KDM-BA acceleration: −1.94 [−2.14, −1.74] years; PhenoAge acceleration: −2.49 [−2.65, −2.34] years; TL: 4.33% [3.89%, 4.78%]. Similar trends were found for those with low PRS and high PDI or hPDI. On the contrary, participants with low PRS and low uPDI showed the lowest biological aging acceleration. Additionally, no significant interactions were observed between dietary patterns and PRS on biological aging (Pinteraction > 0.05), except for an interaction between PDI and PRS on PhenoAge acceleration (Pinteraction = 0.005).

All models were adjusted for age, sex, Townsend index, BMI, smoking status, healthy drinking, physical activity, healthy sleep score, cardiovascular disease, cancer, diabetes, high cholesterol, hypertension, respiratory disease, and medication for cholesterol-lowering, anti-hypertensive, or anti-diabetes, genetic kinship, and the first 10 genetic principal components. A EAT-Lancet index. B PDI. C hPDI. D uPDI. PDI plant-based diet index; hPDI healthy plant-based diet index; uPDI unhealthy plant-based diet index; BMI body mass index; KDM-BA Klemera-Doubal biological age; PhenoAge phenotypic age.
Metabolomic signatures for individual dietary patterns
Among the 170 metabolites analyzed, multivariable linear regression identified 137 metabolites significantly associated with the EAT-Lancet diet, 96 with PDI, 118 with hPDI, and 118 with uPDI (Fig. S3). In specific food component analyses, fruits exhibited the most extensive associations with metabolites (112/170; 65.9%), whereas miscellaneous animal-based foods showed the narrowest associations (4/170; 2.4%). Subsequently, the elastic net regression analyses on 170 metabolites identified 71, 20, 31, and 43 representative metabolites to construct the metabolomic signatures for the EAT-Lancet diet, PDI, hPDI, and uPDI, respectively (Fig. S4). The metabolomic signature components exhibited considerable heterogeneity across different dietary patterns (Fig. 3). For example, the predominant contributors to the EAT-Lancet diet metabolomic signature included linoleic acid, choline, free cholesterol in IDL, omega-6 fatty acids, cholesteryl esters in medium VLDL, and total triglycerides. By contrast, linoleic acid and sphingomyelins were the leading metabolites constituting the metabolomic signatures for PDI and hPDI, while linoleic acid, valine, and isoleucine contributed most to the uPDI metabolomic signature. Figure S5 demonstrated the associations between selected metabolites and individual dietary patterns. The metabolomic signatures were significantly correlated with the corresponding dietary pattern scores, albeit with low to modest correlations (r = 0.17–0.35, all P < 0.001) (Fig. 4A–D).

A EAT-Lancet index. B PDI. C hPDI. D uPDI. Each panel presented from right to left is the metabolites’ coefficients (weights) in the metabolomic signatures and their associations with biological aging and diet pattern exposure. Coefficients for associations with diet pattern index indicate the SD changes in metabolites per SD increment in dietary intake. Coefficients for biological aging indicate an estimate (β) of biological aging measures per SD increment in metabolites. Colors indicate the direction of association, with red representing positive associations and blue indicating inverse associations. The darkness of the color corresponds to the magnitude of the association. Asterisks denote statistical significance, with one indicating P < 0.05 and two indicating Bonferroni-corrected P < 0.05. PDI plant-based diet index; HPDI healthy plant-based diet index; UPDI unhealthy plant-based diet index; KDM-BA Klemera-Doubal biological age; PhenoAge phenotypic age; BCAA branched-chain amino acids; C cholesterol; CE cholesteryl ester; isoleucine; FC free cholesterol; HDL high-density lipoprotein; IDL intermediate-density lipoprotein; Ile isoleucine; L large; LDL low-density lipoproteins; M medium; PL phospholipid; PUFA polyunsaturated fatty acids; S small; TG triglyceride; VLDL very LDL; XL very large; XS very small; XXL especially large.

A–D Correlations between dietary pattern scores and the corresponding metabolomic signatures; E–H associations between per SD increment in dietary metabolomic signatures and biological aging from different models. Model 1 were adjusted for age and sex; model 2 were expanded to adjust for race, Townsend index, BMI, smoking status, healthy drinking, physical activity, healthy sleep score, cardiovascular disease, cancer, diabetes, high cholesterol, hypertension, respiratory disease, and medication for cholesterol-lowering, anti-hypertensive, or anti-diabetes; model 3, the adjustment of related dietary pattern score was further conducted to examine association independence. PDI plant-based diet index; HPDI healthy plant-based diet index; UPDI unhealthy plant-based diet index; SD standard deviation; BMI body mass index; KDM-BA Klemera-Doubal biological age; PhenoAge phenotypic age.
Association of diet-related metabolomic signatures with biological aging
After multivariable adjustment, the diet-related metabolomic signatures showed significant associations with biological aging (Fig. 4E–H). These associations remained even after adjusting for corresponding dietary pattern scores. Each 1-SD increment in the metabolomic signature for the EAT-Lancet diet, PDI, and hPDI was linked to decreased KDM-BA acceleration of 1.11–1.65 years, decreased PhenoAge acceleration of 0.57–1.31 years, and increased TL of 0.19–0.36%. On the contrary, the uPDI metabolomic signature was associated with an increase in KDM-BA (0.49 years) and PhenoAge acceleration (0.68 years) and a decrease in TL (−0.38%). Supplementary analyses using the metabolomic signature derived from the first repeat assessment yielded consistent results (Fig. S6). Notably, after adjusting for the metabolomic signatures, the associations of four dietary patterns with KDM-BA and PhenoAge acceleration were remarkably attenuated, while the associations with TL became nonsignificant except for the EAT-Lancet diet index (Table S10).
Mendelian randomization analyses
When further using two-sample Mendelian randomization (MR) to explore the potential causal associations between the 80 metabolites used for calculating the four diet-related metabolomic signatures, except for glucose-lactate and spectrometer-corrected alanine (not available from the GWAS studies) and biological aging, we found that the 24, 13, and 36 metabolites were significantly associated with KDM-BA acceleration, PhenoAge acceleration, and TL, respectively, with the largest number of associations observed for lipoprotein subclasses (Table S11). Notably, genetically elevated levels of lipoprotein subclasses were generally associated with increased KDM-BA and PhenoAge acceleration. Sensitivity analyses produced consistent estimates (Table S12).
Mediation analysis of metabolomic signatures and metabolites
Figure 5 shows that the diet-related metabolomic signatures significantly mediated the relationships between different dietary patterns and biological aging. The mediation proportions ranged from 27.1 to 63.0% by the EAT-Lancet diet metabolomic signature, 37.4–39.0% by the PDI metabolomic signature, 26.9–50.7% by the hPDI metabolomic signature, and 28.6–49.6% by the uPDI metabolomic signature. In addition, we examined the mediation effect of individual metabolites (Figs. S7–S10). Among them, creatinine and glycoprotein acetyls (GlycA) were consistently identified as the two significant mediators in the associations of dietary patterns with KDM-BA and PhenoAge acceleration, while certain medium or small HDL and fatty acids acted as significant mediators in the associations with TL. Furthermore, enrichment analyses showed that metabolites with a mediation effect were mainly enriched into the linoleic acid metabolism pathway for the EAT-Lancet diet index, the glyoxylate and dicarboxylate metabolism pathway for PDI, the pyruvate metabolism pathway for hPDI, and the pathways involving phenylalanine, tyrosine, and tryptophan biosynthesis for uPDI (Fig. S11).

A KDM-BA acceleration. B PhenoAge acceleration. C Telomere length. Asterisks denote statistical significance, with one indicating P < 0.05, two indicating P < 0.01, and three indicating P < 0.001. NA: not applicable. PDI plant-based diet index; hPDI healthy plant-based diet index; uPDI unhealthy plant-based diet index; KDM-BA Klemera-Doubal biological age; PhenoAge phenotypic age.
Additional and sensitivity analyses
We conducted a series of stratified analyses according to baseline characteristics (Figs. S12–S15). Significant interactions were observed between the EAT-Lancet diet, PDI, and hPDI with sex, BMI, TDI, smoking, and cardiovascular disease on KDM-BA or PhenoAge acceleration (all Pinteraction < 0.05), with stronger associations in individuals who were males, nonobese, current smokers, and those who had low economic status and cardiovascular disease. There was also an interaction between uPDI and sex on biological aging (all Pinteraction < 0.05).
The results remained consistent in sensitivity analyses when using robust linear regression models, further adjusting for total energy intake and education, and excluding participants with missing covariates (Tables S13–S15). When we performed the analysis using data from the first dietary assessment at recruitment between 2009 and 2010, the associations did not appreciably change (Table S16 and Fig. S16).
Discussion
In this large-scale prospective cohort study, higher adherence to the EAT-Lancet diet, PDI, and hPDI was associated with decreased KDM-BA and PhenoAge acceleration and preserved TL, with the EAT-Lancet diet showing the most pronounced effect estimates. In contrast, higher uPDI was linked to accelerated biological aging. These associations were independent of genetic susceptibility. We further identified specific metabolomic signatures corresponding to different dietary patterns and found that the metabolomic signatures significantly mediated most of the associations between dietary patterns and biological aging acceleration.
Overall and healthful plant-based diets have been associated with improved biological aging, while an unhealthy plant-based diet has been related to accelerated biological aging10,11,12. A cross-sectional study using data from the US National Health and Nutrition Examination Survey (NHANES) 1999–2010 found that per 10-unit higher PDI and hPDI scores were associated with 0.80- and 0.83-year decreases in PhenoAge acceleration and 1.91- and 1.76-year decreases in KDM-BA acceleration; however, a 10-unit higher uPDI score was associated with increased PhenoAge and KDM-BA acceleration of 0.77 and 1.21 years, respectively10. Similar protective effect of hPDI and detrimental effect of uPDI on TL were demonstrated11. Besides plant-based diets, the EAT-Lancet diet is a recently proposed dietary pattern to promote both human and planetary health17. Previous studies suggested that dietary shifts towards the EAT-Lancet reference diet could bring about population health and environment co-benefits. Although the associations of the EAT-Lancet reference diet with multiple diseases have been reported19,25,26, there is sparse information available regarding its relation with biological aging. Our study validated the anti-aging effect of healthful PDI and added that adherence to the EAT-Lancet diet was related to decelerated biological aging, consistent with a previous study using data from NHANES 1999–2018 based on 24-hour dietary questionnaires at a single time27. Notably, since different BA predictors have the potential to capture different biological aging dimensions, our findings of significant associations between dietary patterns and all three BA metrics indicate multi-faceted impact of diet on biological aging process, highlighting the importance of adopting overall dietary patterns to improve healthy aging. The observed nonlinear associations between the EAT-Lancet diet and hPDI on KDM-BA acceleration or telomere length indicate that greater adherence to these healthy dietary patterns may exert a stronger protective effect on biological aging.
This study is among the first to comparatively examine the relations of PDI and the EAT-Lancet diet with biological aging. In the current study, we detected more pronounced effect estimates for the EAT-Lancet diet index than for PDI, which might be partially explained by their discrepancies in recommended food components and intakes levels. For example, compared with plant-based diets that contain low amounts of all animal foods, the EAT-Lancet diet recommends moderate intakes of seafood, poultry, and dairy, with emphasis on fish intake. Several studies have suggested that adding fish to a healthy plant-rich diet could benefit cognitive aging28,29. This additional benefit might be associated with supplementation of omega-3 fatty acids like eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) that are known for their anti-aging properties30,31. In addition, plant-based diets are on the basis of population intake distributions rather than predefined cutoffs, which potentially lead to micronutrient deficiencies such as essential vitamins and minerals32,33. Our findings support the recommendations of the EAT-Lancet diet from the perspective of delaying aging process. Together with its lower environmental impacts, the EAT-Lancet reference diet might be considered as a superior choice in promoting both planetary sustainability and human health.
For specific food components, we found that fruit intake was associated with lower KDM-BA and PhenoAge acceleration and longer TL, whereas meat intake showed the opposite pattern, consistent with previous studies. In the Melbourne Collaborative Cohort Study, Hodge et al. reported that a fruit-rich dietary pattern was most strongly associated with healthy aging, whereas a red meat-rich pattern was least favorable34. Similarly, in the SUpplémentation en VItamines et Minéraux AntioXydants cohort, Assman et al. reported that higher consumption of fruits and vegetables was favorably associated with healthy aging, whereas greater meat intake showed an unfavorable association35. Interestingly, we observed that a higher potato intake was associated with increased KDM-BA and PhenoAge acceleration, and shorter TL, which might be partly explained by the cooking methods and metabolic effects. In the UK, fried potatoes are consumed most frequently36, followed by boiled/baked potatoes and mashed potatoes. A recent large U.S. cohort study reported that fried potato intake was associated with an increased risk of type 2 diabetes, whereas boiled, baked, or mashed potatoes showed no such association37. Similarly, consumption of fried potatoes was associated with higher mortality risk38. Deep-fried potatoes produce substantial amounts of Maillard reaction products, including advanced glycation end products and heterocyclic amines39, and commercially prepared French fries often contain industrial trans fats40. These compounds have been consistently linked to aging-related conditions such as diabetes and cardiovascular disease41.
Our subgroup analysis found that the associations between dietary patterns and KDM-BA or PhenoAge acceleration were stronger in men, nonobese individuals, ever-smokers, and individuals with cardiovascular disease. This finding implied that adherence to healthy dietary patterns might yield more benefits for these subgroups. The discrepancy in interactions between population characteristics and dietary patterns on three biological aging indicators may be related to different aspects of biological aging explained by these indicators. Furthermore, we did not observe a gene-diet interaction, and participants with low PRS and greater adherence to the EAT-Lancet diet, PDI, hPDI or low uPDI had the lowest biological aging acceleration. This result emphasized the universal benefits of adopting healthy dietary patterns, regardless of genetic background, in resisting biological aging and preventing aging-related diseases.
It is recognized that the metabolomic profiles can reflect pronounced body responsiveness to the combined effects of endogenous genetic variabilities and exogenous environmental exposures. In recent years, studies have shown metabolomic markers of healthy dietary patterns based on different assessment methods. Our study validated and extended previous findings by simultaneously quantifying metabolic biomarkers associated with the EAT-Lancet and plant-based diets through large-scale metabolomics data. We found substantial metabolomic variation in relation to four dietary patterns, with a larger number of metabolites identified to be associated with the EAT-Lancet diet as compared with plant-based diets. Among the selected metabolites, lipoproteins were predominantly linked to the EAT-Lancet diet and uPDI, while amino acids represented the primary features linked to PDI and hPDI, suggesting distinct diet-derived metabolites or metabolic pathways involved underlying different dietary patterns.
The metabolomic signatures, established by integrating metabolites specific to individual dietary patterns, had significant associations with dietary pattern scores. Notably, these metabolomic signatures were associated with biological aging, even after adjusting for the corresponding dietary patterns, showing the potential of metabolomic signatures to complement traditional dietary assessments. Previous studies have indicated that a comprehensive metabolomic profile represents a promising indicator for assessing biological aging and aging-related diseases. Our study expands on previous results and manifests the mediating role of metabolomic signature in the associations between dietary patterns and biological aging, with a mediation proportion ranging from 26.9 to 63.0%. This finding suggests the metabolomic signature may help enhance our understanding of the anti-aging effect of healthy dietary patterns and contribute to personalized nutrition towards healthy aging promotion.
This study offers important insights into the associations between the EAT-Lancet and plant-based diets, metabolomic response to these dietary patterns, and biological aging in mid- to late-life. By leveraging data from the five baseline dietary assessments, we could account for seasonal differences in food component intake and reduce information bias inherent in a single survey. The UK Biobank is currently the largest cohort with extensive metabolomics data. The repeated assessments enable us to internally validate the metabolomic signature and calculate BA change over time to enhance the reliability of our results. However, several limitations should be acknowledged. First, there were variations in the number of 24-h online dietary questionnaires completed by participants. However, previous studies have suggested that these questionnaires demonstrate moderate to strong agreement42; besides, our sensitivity analysis among participants with the first questionnaire assessment showed consistent results. Second, the cross-sectional nature of our study precludes causal inference of the observed associations. As a supplementary analysis, we used repeated blood measurements to assess the longitudinal change in KDM-BA and PhenoAge acceleration over time and found significant associations between dietary patterns and the rate of biological aging acceleration. Third, the NMR platform measures only a limited subset of plasma metabolites and may not fully capture diet-related metabolomic signatures. Moreover, diet has the potential to modulate circulating proteins, and part of the diet-disease associations may be mediated by the plasma proteome43. Future studies integrating a broader spectrum of metabolites along with proteomic profiling are warranted to provide a more comprehensive understanding of the molecular mechanisms linking diet to biological aging. Fourth, the construction and validation of the diet-related metabolomic signature was based on the same cohort in this study. Ideally, independent external validation is needed to confirm the reproducibility and applicability of our findings. Fifth, there was a median difference of ~1.8 years between dietary assessment and blood specimen collection. Nevertheless, existing evidence has indicated relatively stable dietary habits in this middle-aged and elderly group over a 4–5 year span. Lastly, the UK Biobank participants are primarily white European individuals and generally healthier than the general UK population. Therefore, the generalizability of our results to other diverse populations might be limited.
In conclusion, this study demonstrated that higher adherence to the EAT-Lancet and plant-based diets was associated with decreased biological aging regardless of genetic susceptibility. The diet-specific metabolomic signatures mediated most of the associations between corresponding dietary patterns and biological aging. These findings underscore the potential benefits of adopting EAT-Lancet and plant-based dietary patterns for healthy aging and highlight the promise of metabolomic signatures in guiding personalized nutrition strategies.
Methods
Study design and population
The UK Biobank is a population-based cohort study that enrolled over 500,000 participants aged 37–73 years in 22 assessment centers across England, Scotland, and Wales between 2006 and 2010. At baseline assessment, participants completed a touch screen questionnaire and underwent a series of physical measurements and biological sample collection. Details of the study design and data collection procedures have been reported previously44. The UK Biobank received approval from the North West Multicenter Research Ethics Committee, and all participants provided electronic informed consent. The study was conducted in accordance with the Declaration of Helsinki.
For the robust estimates of dietary intake, participants who completed the online 24 h dietary recall questionnaire on at least two occasions were included (Fig. S17). We excluded those with implausible energy intake (<800 or >4200 kcal/day in men and <600 or >3500 kcal/day in women)45. Participants with missing information on biological aging biomarkers were further excluded. Finally, a total of 87,282 participants were included for the analyses of the associations between dietary patterns and biological aging. Further analyses of metabolomic signatures in the diet-biological aging association were performed among participants with complete metabolites data (n = 48,049).
Assessment of EAT-Lancet and plant-based diet index
Dietary information was collected via the Oxford WebQ questionnaire, a validated 24-h dietary assessment tool covering 206 food items and 32 beverages, on five separate occasions from April 2009 to June 201246. Among the 87,282 participants with at least 2 dietary assessments, 37.9%, 33.6%, 24.1%, and 4.4% completed 2, 3, 4, and 5 assessments, respectively. Total energy and macronutrient intakes were calculated using the UK Nutrient Databank food composition tables. In order to reduce within-subject variation47, dietary intakes were averaged across all available assessments for each participant to calculate four dietary pattern scores: the EAT-Lancet diet index, PDI, hPDI, and uPDI.
The EAT-Lancet diet index consisted of 14 food components (7 emphasized and 7 limited components) as defined previously (Table S17)48. For each component, adherence was scored from 0 to 3 (higher scores for greater adherence to emphasized foods and the reverse for limited foods), and summed to yield a total index ranging from 0 to 42, with higher index indicating greater adherence to the EAT-Lancet dietary pattern. We calculated the PDI, hPDI, and uPDI using the established method conceptualized by Satija et al.18,49. We categorized foods into 17 groups and further classified them into larger categories: healthy plant-based foods, less healthy plant-based foods, and animal foods (Table S18). Given the controversial health effect of alcohol, alcoholic beverages were not included in the plant-based indices but were adjusted for in the regression models50. The intakes of individual food groups were ranked into quintiles. In terms of overall PDI, quintiles of healthful and unhealthful plant-based food groups were assigned scores of 1–5, and reversely for animal-based food groups. Following the criteria, hPDI reversely assigned scores to unhealthful food groups and uPDI reversely assigned scores to healthful food groups. The scores of 17 food groups were summed up to obtain the overall scores ranging from 17 to 85 for all three plant-based dietary patterns.
Metabolomics measurement
Measurements of plasma metabolomics from a randomly selected subset of approximately 280,000 UK Biobank participants (~15,000 participants underwent a repeat assessment visit) were performed between June 2019 and April 2020 (phase 1) and between April 2020 and June 2022 (phase 2). Nuclear magnetic resonance (NMR)-based metabolomic profiling was conducted by Nightingale Health Laboratories. Detailed methodologies for sample collection and metabolite quantification have been described in previous studies51. These phases assessed 251 metabolic biomarkers (170 in absolute concentrations and 81 in derived ratios), which cover lipoprotein lipids in 14 subclasses, fatty acids and their compositions, as well as various low-molecular weight metabolites, such as amino acids, ketone bodies, and glycolysis metabolites quantified in molar concentration units. We included a subset of 170 metabolic biomarkers that were directly measured for subsequent analyses (Table S19). Metabolites with less than 10% missing values were included52, and the remaining missing data for each metabolite were imputed using half of the minimum detectable value. All metabolites underwent a rank-based inverse normal transformation prior to analysis. Specifically, the observations were transformed to the probability scale using the empirical cumulative distribution function, and the transformed values were then converted to Z-scores on the real number line using the probit function.
Assessment of biological age and age acceleration
Two best-trained BA algorithms, including KDM-BA and PhenoAge, were applied. These algorithms have been developed from the National Health and Nutrition Examination Survey (NHANES)53 and validated with available data from the UK Biobank54 (see Table S20 for the corresponding data field IDs). The blood specimens collected at baseline were analyzed using Beckman Coulter LH750 instruments within 24 h. Detailed procedures and quality control are available on the website (https://biobank.ndph.ox.ac.uk/showcase/showcase/docs/serum_biochemistry.pdf).
An individual’s KDM-BA prediction corresponds to the chronological age at which their physiological state would be considered approximately normal. The KDM-BA was derived from regressions of nine biomarkers [e.g., systolic blood pressure, forced expiratory volume in 1 s (FEV1), total cholesterol, glycated hemoglobin, blood urea nitrogen, albumin, creatinine, C-reactive protein, and alkaline phosphatase] on chronological age within a reference population. The PhenoAge algorithm, initially developed using elastic-net Gompertz regression of mortality on 42 biomarkers among NHANES participants, can be interpreted as the age at which an individual’s mortality risk aligns with the predicted average mortality risk for that age55. In this study, we calculated an individual’s PhenoAge using chronological age and nine biomarkers, including lymphocyte percentage, mean cell volume, glucose, red cell distribution width, white blood cell count, albumin, creatinine, C-reactive protein, and alkaline phosphatase54,56.
KDM-BA and PhenoAge values were calculated using the R package “BioAge” (https://github.com/dayoonkwon/BioAge). Age acceleration was calculated as the residual by regressing KDM-BA and PhenoAge on chronological age54. Individuals with age acceleration values greater than 0 indicated an advanced state of biological aging, while those with age acceleration values less than 0 indicated a delayed state of biological aging57.
Measurements of leukocyte TL
Leukocyte TL at the baseline survey was measured by quantitative PCR, a widely accepted and well-validated technique58. This measure (data-field: 22191) was a ratio of TL repeat number (T) against a reference single-copy gene (S) to express a T/S ratio, where T and S were computed by either the calibrator sample at each run, consisting of pooled DNA from 20 participants or the standard curve. Strict and pre-defined quality control (QC) criteria were applied for the measurement of TL at both the sample and run levels. All samples that failed QC were re-measured until valid measurements were obtained or the sample was considered exhausted or unsatisfactory. Besides, deliberate repeats and blinded duplicates were applied to measure reproducibility and stability of the measurement. A detailed description of the measurement and QC procedure of TL in the UKB participants was published elsewhere58.
Polygenic risk scores
Polygenic risk scores (PRS) were constructed according to single-nucleotide polymorphisms (SNPs) associated with KDM-BA acceleration, PhenoAge acceleration, and leukocyte TL in individuals of European ancestry from previous genome-wide association studies59,60. Detailed information on SNPs genotyping, imputation, and quality control in the UK Biobank has been described previously61. Table S21 summarizes the selected SNPs used for PRS construction. The number of effect alleles was weighted by the strengths of associations with biological aging metrics, and then summed to derive a PRS for KDM-BA, PhenoAge, and TL, respectively62. Participants were categorized into low (tertile 1), medium (tertile 2), and high genetic risk (tertile 3) according to PRS tertiles.
Covariates
Information on demographic characteristics, lifestyle factors, and medication use was collected through self-report questionnaires. The demographic characteristics included age, sex, race and Townsend deprivation index (TDI). TDI was assessed in terms of unemployment, car and homeownership, and household overcrowding, with a higher score indicating a higher degree of deprivation63. Lifestyle factors included smoking status (never, previous, or current), alcohol consumption (healthy drinking or no), physical activity (active or inactive), and healthy sleep score. Prevalent diseases that encompassed cardiovascular disease, cancer, diabetes, high cholesterol, hypertension, and respiratory disease were ascertained from self-reports and disease registers. Weight, height, and waist circumference were measured by trained technicians, and body mass index (BMI) was calculated as weight in kg divided by height in m2. Healthy drinking was defined as alcohol consumption ≤14 g/day for women and ≤28 g/day for men64. Physical activity was classified as active or inactive based on whether an individual met the criteria of 150 min of moderate activity per week, 75 min of vigorous activity, or an equivalent combination. A healthy sleep score of 0–5 was derived from five sleep factors, including insomnia (sometimes or never), sleep duration (7–8 h), chronotype (morning person), daytime sleepiness (sometimes or never), and snoring (no)65. Participants received 1 point for each healthy category, with higher scores indicating healthier sleep patterns.
Statistical analysis
Baseline characteristics of the study participants were expressed as mean (SD), and categorical variables were expressed as number (percentage). T-test and the χ² test were employed to test group differences for continuous and categorical variables, respectively. Multiple imputation by chained equations was utilized to impute the missing covariate data.
We conducted multivariable linear regression models to estimate the associations of four dietary pattern scores with KDM-BA, PhenoAge acceleration, and TL, and reported the regression coefficient (β) and corresponding 95% CIs. The percent changes of TL were expressed using the following formula: [exp (β)−1] × 100%, to facilitate comparison across different aging measures according to previous studies57,66,67. The dietary pattern scores were analyzed as categorical (in quartiles) and continuous variables (per SD) after standardization. Model 1 was adjusted for age and sex. Model 2 was further adjusted for race, TDI, BMI, smoking status, healthy drinking, physical activity, healthy sleep score, cardiovascular disease, cancer, diabetes, high cholesterol, hypertension, respiratory disease, and medication use for diabetes, high cholesterol, and hypertension. The P value for the trend test across dietary pattern groups was calculated using integer values. We also employed restricted cubic spline analyses with three knots to examine the dose-response relationship. To investigate potential sources of heterogeneity across the three plant-based diets, we further examined plant-based subgroups (including healthy plant-based, unhealthy plant-based, and animal-based food groups) and specific food components in relation to biological aging. Additionally, to mitigate possible temporal ambiguity, we calculated the biological aging rate by dividing the change in KDM-BA and PhenoAge acceleration by the follow-up time (i.e., Δ biological aging acceleration/follow-up time [years]) in a subgroup of participants with both baseline and revisit blood measurements, and assessed its association with dietary pattern scores.
To examine the joint association between dietary pattern scores and genetic susceptibility on biological aging, participants were classified into 12 groups, with those at high genetic risk who had low dietary scores as reference. The interaction between dietary patterns scores and genetic risk was assessed by adding a cross-product term in the models that were additionally adjusted for genetic kinship and the first 10 genetic principal components.
Multivariable linear regressions were used to examine the associations of metabolites with different dietary patterns, food subgroups and specific food components analyses were adjusted for multiple testing using the Bonferroni correction method. To identify the representative metabolites and metabolomic signature related to dietary patterns, we used baseline metabolomics data as the training set (n = 48,049) and first repeat metabolomics data (n = 3512) as the testing set. The metabolomic signatures for different dietary patterns were quantified following a two-step process. At the first step, we regressed dietary pattern scores on the 170 metabolites using elastic net regression model and then applied the trained model to the testing sets. Elastic net regression is a classification algorithm that integrates the advantages of lasso and ridge methods, enabling it to address multicollinearity, reduce overfitting and perform effective variable selection68,69. The optimal lambda parameter was established through a 10-fold cross-validation, selecting the lambda that resulted in a mean squared error within one standard error of the minimum. Subsequently, we calculated the metabolomic signature based on the weighted sum of the selected metabolites (coefficients≠0), and each weight corresponded to the coefficients from the elastic net regression. The stability of the results was validated using follow-up metabolomics data. Multivariable linear regressions were used to investigate the associations between the diet-related metabolomic signature and identified metabolites, and biological aging markers, with adjustment for the full covariates in the models. The metabolic signature scores corresponding to the four dietary patterns were standardized to ensure comparability. To evaluate the contribution of metabolomic signatures and specific metabolites to the association between dietary patterns and biological aging, a mediation analysis was conducted using the R package “mediation” with 1000 simulations and a quasi-Bayesian approach to estimate variance. The direct and indirect effects and mediation proportions were computed with covariates adjusted in Model 2. Negative mediation proportions were truncated at a lower limit of 0%, as it represents the minimum threshold for a mediation proportion70. In addition, to explore the underlying biological mechanisms, we performed KEGG pathway analysis on the metabolites that significantly mediated the association between dietary patterns and biological aging using MetaboAnalyst 6.0.
Stratified analyses were conducted to test the potential modification effects on the associations between dietary patterns, metabolomic signature, and biological aging by age (<60 vs ≥60 years), sex (female vs male), BMI (<30 vs ≥30 kg/m2), socioeconomic status (low: TDI < −2.38 vs high: TDI ≥ −2.38) smoking (never, previous, or current), healthy drinking (yes vs no), physically active (yes vs no), cardiovascular disease (yes vs no), diabetes (yes vs no), high cholesterol (yes vs no), and hypertension (yes vs no). The interactions of stratifying factors and dietary pattern scores or metabolomic signatures were tested by the likelihood ratio test.
Several sensitivity analyses were carried out to evaluate the robustness of the results. First, robust linear regression models were used to avoid inappropriate estimation of the residual scale from linear regression in assessing the association between dietary patterns and biological aging71. Second, we repeated the analyses after additional adjustment for total energy intake and education. Third, we restricted the analyses to participants with complete covariates. Fourth, to reduce the possibility of reverse causation, we performed an analysis among participants who completed the first dietary assessment at the recruitment between 2009 and 2010.
MR analyses were performed to explore the potential causal associations between the identified metabolites and biological aging. Genetic instruments for the metabolites contributing to the four diet-related metabolomic signatures were obtained from published genome-wide association study (GWAS) summary statistics, except for glucose-lactate and spectrometer-corrected alanine, for which no GWAS data were available72. Summary statistics for KDM-BA acceleration (n = 98,446)59, PhenoAge acceleration (n = 107,640)59, and leukocyte TL (n = 418,401)73 were derived from prior GWAS studies in individuals of European ancestry. We selected single-nucleotide polymorphisms (SNPs) associated with each metabolite at genome-wide significance (P < 5 × 10−8), and then applied stringent linkage disequilibrium (LD) clumping (10,000 kb window, r2 < 0.001) to retain independent variants. Cochran’s Q statistic and Egger intercept were used to test for heterogeneity and horizontal pleiotropy, respectively. To assess the robustness of the results, we conducted sensitivity analyses using alternative methods. Benjamini–Hochberg method was used to control the false discovery rate (FDR) in all analyses. All analyses were performed using R (version 4.4.4). A two-tailed P < 0.05 was considered statistically significant.
Data availability
For the UK Biobank study, the datasets generated and analyzed are available at (https://www.ukbiobank.ac.uk/). Our research has been conducted under application number 77740. 4.
Code availability
Relevant analyses in this study were conducted using R version 4.4.4. No customized code was developed. The analytic code used in this work is available from the corresponding author upon reasonable request.
References
Moqri, M. et al. Biomarkers of aging for the identification and evaluation of longevity interventions. Cell 186, 3758–3775 (2023).
Jylhävä, J., Pedersen, N. L. & Hägg, S. Biological age predictors. EBioMedicine 21, 29–36 (2017).
Bao, H. et al. Biomarkers of aging. Sci. China Life Sci. 66, 893–1066 (2023).
Li, X. et al. Longitudinal trajectories, correlations and mortality associations of nine biological ages across 20-years follow-up. Elife 9, e51507 (2020).
Belsky, D. W. et al. Eleven telomere, epigenetic clock, and biomarker-composite quantifications of biological aging: do they measure the same thing?Am. J. Epidemiol. 187, 1220–1230 (2018).
Campisi, J. et al. From discoveries in ageing research to therapeutics for healthy ageing. Nature 571, 183–192 (2019).
Barzilai, N., Cuervo, A. M. & Austad, S. Aging as a biological target for prevention and therapy. JAMA. 320, 1321–1322 (2018).
Longo, V. D. & Anderson, R. M. Nutrition, longevity and disease: from molecular mechanisms to interventions. Cell 185, 1455–1470 (2022).
Wang, X. et al. Associations of healthy eating patterns with biological aging: National Health and Nutrition Examination Survey (NHANES) 1999–2018. Nutr. J. 23, 112 (2024).
Wang, J. et al. Healthful plant-based diets are negatively associated with the rate of biological aging: a national study based on US adults. Nutr. Res. 132, 112–124 (2024).
Li, X. et al. Association of healthy and unhealthy plant-based diets with telomere length. Clin. Nutr. 43, 1694–1701 (2024).
Wang, S. et al. Association between plant-based dietary pattern and biological aging trajectory in a large prospective cohort. BMC Med. 21, 310 (2023).
Whitmee, S. et al. Safeguarding human health in the anthropocene epoch: report of the Rockefeller Foundation-Lancet Commission on planetary health. Lancet 386, 1973–2028 (2015).
Tilman, D. & Clark, M. Global diets link environmental sustainability and human health. Nature 515, 518–522 (2014).
Herrero, M. et al. Biomass use, production, feed efficiencies, and greenhouse gas emissions from global livestock systems. Proc. Natl. Acad. Sci. USA 110, 20888–20893 (2013).
Musicus, A. A. et al. Health and environmental impacts of plant-rich dietary patterns: a US prospective cohort study. Lancet Planet Health 6, e892–e900 (2022).
Willett, W. et al. Food in the anthropocene: the EAT-Lancet commission on healthy diets from sustainable food systems. Lancet 393, 447–492 (2019).
Satija, A. et al. Plant-based dietary patterns and incidence of type 2 diabetes in US men and women: results from three prospective cohort studies. PLoS Med. 13, e1002039 (2016).
Cai, H. et al. Health outcomes, environmental impacts, and diet costs of adherence to the EAT-Lancet diet in China in 1997-2015: a health and nutrition survey. Lancet Planet Health 8, e1030–e1042 (2024).
Chen, H. et al. Plant-based and planetary-health diets, environmental burden, and risk of mortality: a prospective cohort study of middle-aged and older adults in China. Lancet Planet Health 8, e545–e553 (2024).
Jafari, S. et al. Plant-based diets and risk of disease mortality: a systematic review and meta-analysis of cohort studies. Crit. Rev. Food Sci. Nutr. 62, 7760–7772 (2022).
Rattray, N. J. W. et al. Metabolic dysregulation in vitamin E and carnitine shuttle energy mechanisms associate with human frailty. Nat. Commun. 10, 5027 (2019).
Jacob, M., Lopata, A. L., Dasouki, M. & Abdel Rahman, A. M. Metabolomics toward personalized medicine. Mass Spectrom. Rev. 38, 221–238 (2019).
Noerman, S. & Landberg, R. Blood metabolite profiles linking dietary patterns with health-toward precision nutrition. J. Intern. Med. 293, 408–432 (2023).
Lu, X. et al. Adherence to the EAT-Lancet diet and incident depression and anxiety. Nat. Commun. 15, 5599 (2024).
Ye, Y. X. et al. Adherence to a planetary health diet, genetic susceptibility, and incident cardiovascular disease: a prospective cohort study from the UK Biobank. Am. J. Clin. Nutr. 120, 648–655 (2024).
Huang, S., Hu, H. & Gong, H. Association between the planetary health diet Index and biological aging among the U.S. population. Front. Public Health 12, 1482959 (2024).
van Soest, A. P. M., van de Rest, O., Witkamp, R. F., van der Velde, N. & de Groot, L. The association between adherence to a plant-based diet and cognitive ageing. Eur. J. Nutr. 62, 2053–2062 (2023).
Zhu, A., Yuan, C., Pretty, J. & Ji, J. S. Plant-based dietary patterns and cognitive function: a prospective cohort analysis of elderly individuals in China (2008-2018). Brain Behav. 12, e2670 (2022).
Samieri, C. et al. Fish intake, genetic predisposition to Alzheimer disease, and decline in global cognition and memory in 5 cohorts of older persons. Am. J. Epidemiol. 187, 933–940 (2018).
Bischoff-Ferrari, H. A. et al. Individual and additive effects of vitamin D, omega-3 and exercise on DNA methylation clocks of biological aging in older adults from the DO-HEALTH trial. Nat. Aging. https://doi.org/10.1038/s43587-024-00793-y (2025).
Kent, G., Kehoe, L., Flynn, A. & Walton, J. Plant-based diets: a review of the definitions and nutritional role in the adult diet. Proc. Nutr. Soc. 81, 62–74 (2022).
Bakaloudi, D. R. et al. Intake and adequacy of the vegan diet. A systematic review of the evidence. Clin. Nutr. 40, 3503–3521 (2021).
Hodge, A. M., O’Dea, K., English, D. R., Giles, G. G. & Flicker, L. Dietary patterns as predictors of successful ageing. J. Nutr. Health Aging 18, 221–227 (2014).
Assmann, K. E. et al. Association between adherence to the Mediterranean diet at midlife and healthy aging in a cohort of French adults. J. Gerontol. A Biol. Sci. Med. Sci. 73, 347–354 (2018).
Wan, X. et al. Potato consumption, polygenic scores, and incident type 2 diabetes: an observational study. Food Res. Int. 170, 112936 (2023).
Mousavi, S. M. et al. Total and specific potato intake and risk of type 2 diabetes: results from three US cohort studies and a substitution meta-analysis of prospective cohorts. BMJ. 390, e082121 (2025).
Veronese, N. et al. Fried potato consumption is associated with elevated mortality: an 8-y longitudinal cohort study. Am. J. Clin. Nutr. 106, 162–167 (2017).
Hellwig, M. & Henle, T. Baking, ageing, diabetes: a short history of the Maillard reaction. Angew Chem Int. Ed. Engl. 53, 10316–10329 (2014).
Cahill, L. E. et al. Fried-food consumption and risk of type 2 diabetes and coronary artery disease: a prospective study in 2 cohorts of US women and men. Am. J. Clin. Nutr. 100, 667–675 (2014).
Rungratanawanich, W., Qu, Y., Wang, X., Essa, M. M. & Song, B. J. Advanced glycation end products (AGEs) and other adducts in aging-related diseases and alcohol-mediated tissue injury. Exp. Mol. Med. 53, 168–188 (2021).
Bradbury, K. E., Young, H. J., Guo, W. & Key, T. J. Dietary assessment in UK Biobank: an evaluation of the performance of the touchscreen dietary questionnaire. J. Nutr. Sci. 7, e6 (2018).
Zhu, K. et al. Proteomic signatures of healthy dietary patterns are associated with lower risks of major chronic diseases and mortality. Nat. Food. https://doi.org/10.1038/s43016-024-01059-x (2024).
Sudlow, C. et al. UK Biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 12, e1001779 (2015).
Lv, Y. et al. Plant-based diets, genetic predisposition and risk of non-alcoholic fatty liver disease. BMC Med. 21, 351 (2023).
Greenwood, D. C. et al. Validation of the Oxford WebQ online 24-hour dietary questionnaire using biomarkers. Am. J. Epidemiol. 188, 1858–1867 (2019).
Hu, F. B. et al. Dietary fat and coronary heart disease: a comparison of approaches for adjusting for total energy intake and modeling repeated dietary measurements. Am. J. Epidemiol. 149, 531–540 (1999).
Stubbendorff, A. et al. Development of an EAT-Lancet index and its relation to mortality in a Swedish population. Am. J. Clin. Nutr. 115, 705–716 (2022).
Satija, A. et al. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in U.S. adults. J. Am. Coll. Cardiol. 70, 411–422 (2017).
GBD 2020 Alcohol Collaborators. Population-level risks of alcohol consumption by amount, geography, age, sex, and year: a systematic analysis for the Global Burden of Disease Study 2020. Lancet 400, 185–235 (2022).
Würtz, P. et al. Quantitative serum nuclear magnetic resonance metabolomics in large-scale epidemiology: a primer on -Omic technologies. Am. J. Epidemiol. 186, 1084–1096 (2017).
Wu, H. et al. Dietary pattern modifies the risk of MASLD through metabolomic signature. JHEP Rep. 6, 101133 (2024).
Liu, Z. et al. A new aging measure captures morbidity and mortality risk across diverse subpopulations from NHANES IV: a cohort study. PLoS Med. 15, e1002718 (2018).
Gao, X. et al. Accelerated biological aging and risk of depression and anxiety: evidence from 424,299 UK Biobank participants. Nat. Commun. 14, 2277 (2023).
Parker, D. C. et al. Association of blood chemistry quantifications of biological aging with disability and mortality in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 75, 1671–1679 (2020).
Jiang, M. et al. Accelerated biological aging elevates the risk of cardiometabolic multimorbidity and mortality. Nat. Cardiovasc. Res. 3, 332–342 (2024).
Cui, F. et al. Early-life exposure to tobacco, genetic susceptibility, and accelerated biological aging in adulthood. Sci. Adv. 10, eadl3747 (2024).
Codd, V. et al. Measurement and initial characterization of leukocyte telomere length in 474,074 participants in UK Biobank. Nat. Aging 2, 170–179 (2022).
Kuo, C. L., Pilling, L. C., Liu, Z., Atkins, J. L. & Levine, M. E. Genetic associations for two biological age measures point to distinct aging phenotypes. Aging Cell 20, e13376 (2021).
Li, C. et al. Genome-wide association analysis in humans links nucleotide metabolism to leukocyte telomere length. Am. J. Hum. Genet. 106, 389–404 (2020).
Bycroft, C. et al. The UK Biobank resource with deep phenotyping and genomic data. Nature 562, 203–209 (2018).
Rutten-Jacobs, L. C. et al. Genetic risk, incident stroke, and the benefits of adhering to a healthy lifestyle: cohort study of 306 473 UK Biobank participants. BMJ. 363, k4168 (2018).
Foster, H. M. E. et al. The effect of socioeconomic deprivation on the association between an extended measurement of unhealthy lifestyle factors and health outcomes: a prospective analysis of the UK Biobank cohort. Lancet Public Health 3, e576–e585 (2018).
Wang, B. et al. Association of combined healthy lifestyle factors with incident dementia in patients with type 2 diabetes. Neurology 99, e2336–e2345 (2022).
Li, J. et al. Nuclear magnetic resonance-based metabolomics with machine learning for predicting progression from prediabetes to diabetes. Elife 13, e98709 (2024).
Cao, W. et al. Association between telomere length in peripheral blood leukocytes and risk of ischemic stroke in a Han Chinese population: a linear and non-linear Mendelian randomization analysis. J. Transl. Med. 18, 385 (2020).
Miri, M. et al. Association of greenspace exposure with telomere length in preschool children. Environ. Pollut. 266, 115228 (2020).
Zou, H. & Hastie, T. Regularization and variable selection via the elastic net. J. R. Stat. Soc. Series B Stat. Methodol. 67, 301–320 (2005).
Tian, F. et al. Plasma metabolomic signature of healthy lifestyle, structural brain reserve and risk of dementia. Brain 148, 143–153 (2025).
Ye, C. J. et al. Mendelian randomization evidence for the causal effect of mental well-being on healthy aging. Nat. Hum. Behav. 8, 1798–1809 (2024).
White, A. J. et al. Air pollution, particulate matter composition and methylation-based biologic age. Environ. Int. 132, 105071 (2019).
Zhang, S. et al. A metabolomic profile of biological aging in 250,341 individuals from the UK biobank. Nat. Commun. 15, 8081 (2024).
Kessler, M. D. et al. Common and rare variant associations with clonal haematopoiesis phenotypes. Nature 612, 301–309 (2022).
Acknowledgements
We thank all participants and staff of the UK Biobank cohort for their dedication and contribution to this study.
Funding
This study was supported by the National Natural Science Foundation of China (82170870, 82120108008, and 82404337), Science and Technology Commission of Shanghai Municipality (22015810500 and 24ZR1443400), and Major Science and Technology Innovation Program of Shanghai Municipal Education Commission (2019–01-07–00-01-E00059). The funders of the study had no role in study design, data collection, analysis, decision to publish, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
Yingli Lu and Bin Wang conceived and designed the study. Jie Li and Jiang Li performed the statistical analysis and drafted the manuscript. Xiaoqing Xu and Kun Zhang participated in data collection. Lu Qi and Ningjian Wang critically revised the manuscript. All authors read and approved the final manuscript. Yingli Lu is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, J., Li, J., Xu, X. et al. EAT-Lancet and plant-based diets, plasma metabolomic signatures, and biological aging. npj Aging 12, 9 (2026). https://doi.org/10.1038/s41514-025-00306-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41514-025-00306-0
