
Abstract
We investigated the role of uric acid in the pathogenesis of severe malaria (SM) in two independent cohorts of children with SM. Hyperuricemia (blood uric acid ≥ 7 mg dl−1) was present in 25% of children with SM and was associated with increased in-hospital mortality and postdischarge mortality in both cohorts. Increased blood uric acid levels were also associated with worse scores in overall cognition in children with SM < 5 years old in both cohorts. Hemolysis of infected red blood cells and impaired renal excretion of uric acid were the primary drivers of hyperuricemia in SM. Hyperuricemia was associated with multiple complications of SM, including acute kidney injury, acidosis, impaired perfusion, coma and intestinal injury with increases in the abundance of Gram-negative uricase-producing pathobionts (Escherichia and Shigella) in the stool. Clinical trials evaluating uric acid-lowering medications as adjunctive therapy for children with SM should be considered to improve survival and protect neurodevelopment.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$32.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout






Similar content being viewed by others
Data availability
De-identified data are available on request to the corresponding author. All data requests that comply with limitations contained in the informed consent form signed by the participants of the trial will be granted access to the data within 1 month of the request.
Code availability
Code used in the primary analysis is available on the following GitHub repository: https://github.com/caitbond8/Uric_acid_sev_malaria_statistical_code.
References
World Health Organization. World malaria report 2023. www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2023 (2023).
Balikagala, B. et al. Evidence of artemisinin-resistant malaria in Africa. N. Engl. J. Med. 385, 1163–1171 (2021).
Van Loon, W. et al. In vitro confirmation of artemisinin resistance in Plasmodium falciparum from patient isolates, Southern Rwanda, 2019. Emerg. Infect. Dis. 28, 852–855 (2022).
White, N. J., Turner, G. D., Medana, I. M., Dondorp, A. M. & Day, N. P. The murine cerebral malaria phenomenon. Trends Parasitol. 26, 11–15 (2010).
Lopera-Mesa, T. M. et al. Plasma uric acid levels correlate with inflammation and disease severity in Malian children with Plasmodium falciparum malaria. PLoS ONE 7, e46424 (2012).
Quashie, N. B., Ranford-Cartwright, L. C. & de Koning, H. P. Uptake of purines in Plasmodium falciparum-infected human erythrocytes is mostly mediated by the human equilibrative nucleoside transporter and the human facilitative nucleobase transporter. Malar. J. 9, 36 (2010).
Guermonprez, P. et al. Inflammatory Flt3l is essential to mobilize dendritic cells and for T cell responses during Plasmodium infection. Nat. Med. 19, 730–738 (2013).
Van de Hoef, D. L. et al. Plasmodium falciparum-derived uric acid precipitates induce maturation of dendritic cells. PLoS ONE 8, e55584 (2013).
Orengo, J. M. et al. Plasmodium-induced inflammation by uric acid. PLoS Pathog. 4, e1000013 (2008).
Orengo, J. M. et al. Uric acid is a mediator of the Plasmodium falciparum-induced inflammatory response. PLoS ONE 4, e5194 (2009).
Mishra, J. & Jatav, J. K. To study the correlation or association of serum uric acid level with morbidities and mortality in sepsis patient and its prognostic significance. J. Assoc. Physicians India 70, 11–12 (2022).
Sreekanth & Maldar, A. Hyperuricemia as an early marker in predicting mortality and morbidity in patients with Sepsis. J. Assoc. Physicians India 70, 11–12 (2022).
Pehlivanlar-Kucuk, M., Kucuk, A. O., Ozturk, C. E., Er, M. C. & Ulger, F. The association between serum uric acid level and prognosis in critically Ill patients, uric acid as a prognosis predictor. Clin. Lab. 64, 1491–1500 (2018).
John, C. C. et al. Cerebral malaria in children is associated with long-term cognitive impairment. Pediatrics 122, e92–e99 (2008).
Bangirana, P. et al. Severe malarial anemia is associated with long-term neurocognitive impairment. Clin. Infect. Dis. 59, 336–344 (2014).
Latourte, A., Bardin, T. & Richette, P. Uric acid and cognitive decline: a double-edge sword? Curr. Opin. Rheumatol. 30, 183–187 (2018).
Tana, C., Ticinesi, A., Prati, B., Nouvenne, A. & Meschi, T. Uric acid and cognitive function in older individuals. Nutrients 10, 975 (2018).
Vasquez, M. et al. Xanthine oxidase levels and immune dysregulation are independently associated with anemia in Plasmodium falciparum malaria. Sci. Rep. 13, 14720 (2023).
Conroy, A. L. et al. Angiopoietin-2 levels are associated with retinopathy and predict mortality in Malawian children with cerebral malaria: a retrospective case-control study. Crit. Care Med. 40, 952–959 (2012).
Lovegrove, F. E. et al. Serum angiopoietin-1 and -2 levels discriminate cerebral malaria from uncomplicated malaria and predict clinical outcome in African children. PLoS ONE 4, e4912 (2009).
Conroy, A. L. et al. Host biomarkers are associated with response to therapy and long-term mortality in pediatric severe malaria. Open Forum Infect. Dis. 3, ofw134 (2016).
Charles, B. A. et al. A genome-wide association study of serum uric acid in African Americans. BMC Med. Genet. 4, 17 (2011).
Chen, G. et al. Refining genome-wide associated loci for serum uric acid in individuals with African ancestry. Hum. Mol. Genet. 29, 506–514 (2020).
Ensembl. Human (CRCh38.p14), variant: rs12498742. useast.ensembl.org/Homo_sapiens/Variation/Population?r=4:9941928-9942928;v=rs12498742;vdb=variation;vf=261683788#gnomadgenomesv3.1.2_table (accessed 15 August 2023).
Sorensen, L. B. Role of the intestinal tract in the elimination of uric acid. Arthritis Rheum. 8, 694–706 (1965).
Namazzi, R. et al. Acute kidney injury interacts with coma, acidosis, and impaired perfusion to significantly increase risk of death in children with severe malaria. Clin. Infect. Dis. 75, 1511–1519 (2022).
Sarangam, M. L. et al. Intestinal injury biomarkers predict mortality in pediatric severe malaria. mBio 13, e0132522 (2022).
John, C. C., Park, G. S., Sam-Agudu, N., Opoka, R. O. & Boivin, M. J. Elevated serum levels of IL-1ra in children with Plasmodium falciparum malaria are associated with increased severity of disease. Cytokine 41, 204–208 (2008).
Watson, J. A. et al. Improving the diagnosis of severe malaria in African children using platelet counts and plasma PfHRP2 concentrations. Sci. Transl. Med. 14, eabn5040 (2022).
Conroy, A. L. et al. Cerebrospinal fluid biomarkers provide evidence for kidney–brain axis involvement in cerebral malaria pathogenesis. Front. Hum. Neurosci. 17, 1177242 (2023).
Datta, D. et al. Elevated cerebrospinal fluid tau protein concentrations on admission are associated with long-term neurologic and cognitive impairment in Ugandan children with cerebral malaria. Clin. Infect. Dis. 70, 1161–1168 (2020).
Labcorp. Albumin, cerebrospinal fluid. www.labcorp.com/tests/012229/albumin-cerebrospinal-fluid (accessed 1 September 2023).
Gallego-Delgado, J., Ty, M., Orengo, J. M., van de Hoef, D. & Rodriguez, A. A surprising role for uric acid: the inflammatory malaria response. Curr. Rheumatol. Rep. 16, 401 (2014).
Yin, H., Liu, N. & Chen, J. The role of the intestine in the development of hyperuricemia. Front. Immunol. 13, 845684 (2022).
Xu, X. et al. Hyperuricemia increases the risk of acute kidney injury: a systematic review and meta-analysis. BMC Nephrol. 18, 27 (2017).
Jiang, Y. X. et al. Association between hyperuricemia and acute kidney injury in critically ill patients with sepsis. BMC Nephrol. 24, 128 (2023).
Bayram, D. et al. The effects of allopurinol on metabolic acidosis and endothelial functions in chronic kidney disease patients. Clin. Exp. Nephrol. 19, 443–449 (2015).
Guo, Y. et al. Impaired intestinal barrier function in a mouse model of hyperuricemia. Mol. Med. Rep. 20, 3292–3300 (2019).
Lapsia, V. et al. Elevated uric acid increases the risk for acute kidney injury. Am. J. Med. 125, 302 (2012).
Fathallah-Shaykh, S. A. & Cramer, M. T. Uric acid and the kidney. Pediatr. Nephrol. 29, 999–1008 (2014).
De Oliveira, E. P. & Burini, R. C. High plasma uric acid concentration: causes and consequences. Diabetol. Metab. Syndr. 4, 12 (2012).
Zheng, T. et al. Laboratory predictors of COVID-19 mortality: a retrospective analysis from Tongji Hospital in Wuhan. Mediators Inflamm. 2021, 6687412 (2021).
Feldman, I., Natsheh, A. & Breuer, G. S. Hyperuricemia and adverse outcomes in patients hospitalized for COVID-19 disease. Clin. Med. Res. 21, 87–94 (2023).
Liu, S., Zhong, Z. & Liu, F. Prognostic value of hyperuricemia for patients with sepsis in the intensive care unit. Sci. Rep. 12, 1070 (2022).
Lee, H. W. et al. Serum uric acid level as a prognostic marker in patients with acute respiratory distress syndrome. J. Intensive Care Med. 34, 404–410 (2019).
Yu, Y., Liu, Q., Li, H., Wen, C. & He, Z. Alterations of the gut microbiome associated with the treatment of hyperuricaemia in male rats. Front. Microbiol. 9, 2233 (2018).
Lv, Q. et al. Association of hyperuricemia with immune disorders and intestinal barrier dysfunction. Front. Physiol. 11, 524236 (2020).
Driscoll, A. J. et al. The effect of antibiotic exposure and specimen volume on the detection of bacterial pathogens in children with pneumonia. Clin. Infect. Dis. 64, S368–S377 (2017).
Liu, X. et al. Commensal Enterococcus faecalis W5 ameliorates hyperuricemia and maintains the epithelial barrier in a hyperuricemia mouse model. J. Dig. Dis. 25, 44–60 (2024).
Sun, Y. et al. Wild-type Escherichia coli Nissle 1917 improves hyperuricemia by anaerobically degrading uric acid and maintaining gut microbiota profile of mice. J. Funct. Foods 112, 105935 (2024).
Opoka, R. O. et al. High postdischarge morbidity in Ugandan children with severe malarial anemia or cerebral malaria. J. Pediatr. Infect. Dis. Soc. 6, e41–e48 (2017).
Phiri, K. S. et al. Post-discharge malaria chemoprevention in children admitted with severe anaemia in malaria-endemic settings in Africa: a systematic review and individual patient data meta-analysis of randomised controlled trials. Lancet Glob. Health 12, e33–e44 (2024).
Lee, H. R., Park, J. H., Han, S. W. & Baik, J. S. Cognition, olfaction and uric acid in early de novo Parkinson’s disease. J. Mov. Disord. 11, 139–144 (2018).
Annanmaki, T., Pessala-Driver, A., Hokkanen, L. & Murros, K. Uric acid associates with cognition in Parkinson’s disease. Parkinsonism Relat. Disord. 14, 576–578 (2008).
Kim, T. S. et al. Decreased plasma antioxidants in patients with Alzheimer’s disease. Int. J. Geriatr. Psychiatry 21, 344–348 (2006).
Hooper, D. C. et al. Uric acid, a peroxynitrite scavenger, inhibits CNS inflammation, blood–CNS barrier permeability changes, and tissue damage in a mouse model of multiple sclerosis. FASEB J. 14, 691–698 (2000).
Bowman, G. L., Shannon, J., Frei, B., Kaye, J. A. & Quinn, J. F. Uric acid as a CNS antioxidant. J. Alzheimers Dis. 19, 1331–1336 (2010).
Shao, X. et al. Uric acid induces cognitive dysfunction through hippocampal inflammation in rodents and humans. J. Neurosci. 36, 10990–11005 (2016).
Tian, T. et al. Detrimental effects of long-term elevated serum uric acid on cognitive function in rats. Sci. Rep. 11, 6732 (2021).
L’Ecuyer, S. et al. Targeting uric acid prevents brain injury and anxiety in a rat model of hemorrhagic shock. Shock 56, 298–307 (2021).
Ruiz, A., Gautschi, I., Schild, L. & Bonny, O. Human mutations in SLC2A9 (Glut9) affect transport capacity for urate. Front. Physiol. 9, 476 (2018).
Sarma, P. S., Mandal, A. K. & Khamis, H. J. Allopurinol as an additive to quinine in the treatment of acute complicated falciparum malaria. Am. J. Trop. Med. Hyg. 58, 454–457 (1998).
World Health Organization. Uric acid: optical methods; automated chemistry analyser if available. edl.who-healthtechnologies.org/recommendations/2350uric (2020; accessed 8 April 2024)
Fabre, S. et al. Accuracy of the HumaSens(plus) point-of-care uric acid meter using capillary blood obtained by fingertip puncture. Arthritis Res. Ther. 20, 78 (2018).
World Health Organization. Severe malaria. Trop. Med. Int. Health 19, 7–131 (2014).
KDIGO. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2, 1–138 (2012).
Namazzi, R. et al. Acute kidney injury, persistent kidney disease, and post-discharge morbidity and mortality in severe malaria in children: a prospective cohort study. EClinicalMedicine 44, 101292 (2022).
Batte, A. et al. Methods to estimate baseline creatinine and define acute kidney injury in lean Ugandan children with severe malaria: a prospective cohort study. BMC Nephrol. 21, 417 (2020).
Schriefer, A. E. et al. A multi-amplicon 16S rRNA sequencing and analysis method for improved taxonomic profiling of bacterial communities. J. Microbiol. Methods 154, 6–13 (2018).
Mandal, R. K. et al. Gut bacteroides act in a microbial consortium to cause susceptibility to severe malaria. Nat. Commun. 14, 6465 (2023).
McMurdie, P. J. & Holmes, S. phyloseq: an R package for reproducible interactive analysis and graphics of microbiome census data. PLoS ONE 8, e61217 (2013).
Bryan, D. M., Daniela, W. & Amy, D. W. Modeling microbial abundances and dysbiosis with β-binomial regression. Ann. Appl. Stat. 14, 94–115 (2020).
Barnett, D., Arts, I. & Penders, J. microViz: an R package for microbiome data visualization and statistics. J. Open Source Softw. 6, 3201 (2021).
Chang, C. C. et al. Second-generation PLINK: rising to the challenge of larger and richer datasets. GigaScience 4, 7 (2015).
Zheng, X. et al. A high-performance computing toolset for relatedness and principal component analysis of SNP data. Bioinformatics 28, 3326–3328 (2012).
Taliun, D. et al. Sequencing of 53,831 diverse genomes from the NHLBI TOPMed program. Nature 590, 290–299 (2021).
Das, S. et al. Next-generation genotype imputation service and methods. Nat. Genet. 48, 1284–1287 (2016).
Mullen E. Mullen Scales of Early Learning (American Guidance Services Inc., 1995).
Jordan, C. M., Johnson, A. L., Hughes, S. J. & Shapiro, E. G. The Color Object Association Test (COAT): the development of a new measure of declarative memory for 18- to 36-month-old toddlers. Child Neuropsychol. 14, 21–41 (2008).
Goldman, D. Z., Shapiro, E. G. & Nelson, C. A. Measurement of vigilance in 2-year-old children. Dev. Neuropsychol. 25, 227–250 (2004).
Kaufman A. S. & Kaufman, N. L. Kaufman Assessment Battery for Children Manual. Second Edition (American Guidance Service, 2004).
Greenberg, L. M. & Waldmant, I. D. Developmental normative data on the Test of Variables of Attention (T.O.V.A.). J. Child Psychol. Psychiatry 34, 1019–1030 (1993).
Baron, R. M. & Kenny, D. A. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 51, 1173–1182 (1986).
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Methodol. 57, 289–300 (1995).
Acknowledgements
We are grateful to the participants and caregivers in this trial and to the study team. This work was funded by the National Institutes of Health (NIH)/National Institutes of Health National Institute of Neurological Disorders and Stroke (R01NS055349 to C.C.J.), the Fogarty International Center (D43 TW010928 to C.C.J.), a Ralph W. and Grace M. Showalter Young Investigator Award to A.L.C., NIH/National Institute of Allergy and Infectious Diseases (R01AI165946 to A.L.C.), NIH/National Institute of Neurological Disorders and Stroke (1R01NS105910 to A.R.), NIH/National Heart Lung and Blood Institute (1R01HL150145 to A.R. and 3R01HL150145-02S1 to M.V.), NIH (R21AI151349 to A.R. and A.L.C.), NIH/National Institute of Allergy and Infectious Disease (R01AI148525 to N.W.S. and C.C.J.), NIH National Center for Advancing Translational Sciences (TL1TR002531), Clinical and Translational Sciences Award to O.J.B. and a fellowship award from the NIH/National Institute of Diabetes and Digestive and Kidney Diseases (grant 5T32DK120524-05 to C.L.). The funders had no role in study design, data collection, analysis, interpretation or the decision to publish.
Author information
Authors and Affiliations
Contributions
C.B. wrote the primary draft of the manuscript and all revisions. C.B., A.L.C. and Y.Z. conducted primary study statistical analysis. O.B. and N.W.S. conducted and analyzed microbiome data. D.D. performed and analyzed brain biomarker testing. R.N. was the primary study pediatrician and supervisor. R.O.O. oversaw the conduct of the primary study. G.L.-C., K.U. and D.B. performed study analysis and quality control of uric acid testing data. A.B. and T.M.E.-A. provided analysis and interpretation of renal complications of hyperuricemia. M.A. and A.R. performed testing and analysis of xanthine oxidase levels. C.L., M.A. and T.-H.S.-A. conducted and analyzed studies on genetic testing. C.C.J. obtained primary funding for the study and was responsible for study conduct, analysis and interpretation. A.L.C. supervised, analyzed and interpreted laboratory testing and was responsible for the interpretation of how lab findings related to clinical outcomes in the study. All authors contributed to the writing and revision of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks Hans Ackerman, Terrie Taylor and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Sonia Muliyil, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Genes associated with uric acid levels at admission.
a, Uric acid measurement time points in children with severe malaria (SM) and community controls (CC). Transporters of uric acid reabsorption. b, Association between 14 variants and uric acid levels during severe malaria infection, adjusted for age, sex, site and disease severity (Lambaréné Organ Dysfunction Score). Red square and error bars represent a significant association with uric acid levels. c, Prevalence of SLC2A9 variant rs12498742 (location chr4: 9942428:A:G) G allele in cohort 2, Africa, and global populations (gnomAD genomes v3.1.2). d, Uric acid levels at admission and 1-month follow-up according to rs12498742 genotype in children who were admitted with severe malaria are shown in the box-whisker plots (box, median and IQR; whiskers, 1.5× IQR from the box edges; plus sign (+), mean). P-values shown in d are derived from the Kruskal–Wallis test. The figure is created with BioRender.com.
Extended Data Fig. 2 Hyperuricemia is associated with intestinal injury in severe malaria, and both hyperuricemia and intestinal injury are associated with increased abundance of specific pathobionts.
a, Diagram of high levels of uric acid damaging intestinal endothelium and leading to production of biomarkers of intestinal injury (TFF3 and I-FABP). Intestinal injury is defined as TFF3 >4.078 ng/mL and/or I-FABP >15.433 ng/mL (values >99th percentile of CC). b, Stacked bar chart comparing frequency of intestinal injury in children with hyperuricemia vs. normal uric acid. Two-sided p-value from chi-squared test. c, Differential abundance analysis of bacteria in stool in 417 children from cohort 2 shown in a radial phylogenetic tree. Significant increases in bacteria on admission are shown by white circle. Family is shown at the distal level. d, Stacked bar chart comparing frequency of families associated with higher bacterial abundance in children with hyperuricemia vs. normal uric acid. e, Relative abundance of bacteria (log-transformed) shown in the box plots box-whisker plots (box, median and IQR; whiskers, 1.5× IQR from the box edges; plus sign (+), mean). Two-sided p-values from the Wilcoxon rank sum test in children with intestinal injury (n = 67) vs. without intestinal injury (n = 349) are presented in box plot if significant after correcting for multiplicity using Benjamini–Hochberg false discovery rate (five comparisons). Detailed statistical test results and exact p-values are provided in Supplementary Table 19, corresponding to e. The figure is created with BioRender.com.
Extended Data Fig. 3 Association between uric acid levels and probability of in-hospital mortality in cohort 2.
a, Loess regression curve showing the probability of death as a function of uric acid levels in patients with severe malaria. Knots were selected at 3.8 mg/dL based on where the trend in the probability of death shifts from negative to positive and at 7 mg/dL to represent the threshold for hyperuricemia. b, Adjusted odds ratios (aOR) and 95% confidence intervals (CI) for the association between uric acid levels and in-hospital mortality using two-sided logistic regression with restricted cubic splines with knots at 3.8 and 7.0 mg/dL (based on loess smoothing), adjusted for age, sex and site. Odds ratios represent the risk associated with a 1-unit increase in uric acid within each spline segment.
Extended Data Fig. 4 Causal mediation pathway analysis between hyperuricemia and in-hospital mortality in cohort 2.
a, Causal pathway diagrams with adjusted odds ratios (OR) from binary logistic regression, adjusted for age, sex and site. Two-sided p-values shown in diagram and are not adjusted for multiple comparisons. b, The indirect and direct effects of hyperuricemia on in-hospital mortality with potential mediators, showing point estimates with 95% confidence intervals (error bars), obtained from causal mediation analysis. Sample sizes (independent biological samples from individual patients) were n = 595 for AKI and hyperuricemia; n = 594 for intestinal injury, metabolic acidosis and coma; and impaired n = 593 for perfusion. The percentage mediated (indirect effect divided by total effect) is presented to the right of the diagram in the diagram. All mediation analyses are adjusted for age, sex and site, with p-values from two-sided tests. All mediators were statistically significant (p < 0.05). For the relationship between AKI and mortality, mediation analysis was also performed for hyperuricemia as the potential mediator. AKI, acute kidney injury.
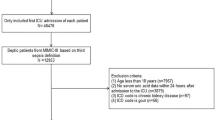
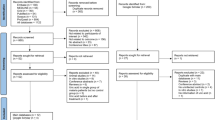
Extended Data Fig. 5 Flowchart of study participants with cognitive tests during follow-up among children included in the uric acid substudy.
Cohort 1 included four cognitive testing time points following enrollment and administered different cognitive tests for children <5 years of age and >5 years of age. As some children remained in the study but had missed cognitive testing at a given time point, the number of children remaining in a study is included on the upper righthand side of boxes, ‘following n’. Cohort 2 had one cognitive testing follow-up time point and only included children <5 years of age.
Supplementary information
Supplementary Information (download PDF )
Supplementary Tables 1–19 and Supplementary Methods.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bond, C., Bednarski, O.J., Datta, D. et al. Elevated uric acid levels, mortality and cognitive impairment in children with severe malaria. Nat Med 31, 777–787 (2025). https://doi.org/10.1038/s41591-024-03430-8
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41591-024-03430-8
This article is cited by
-
Gut bacterial dysbiosis in pediatric severe malaria associates with post-discharge mortality
Nature Communications (2025)
