
Abstract
Antimicrobial resistance (AMR) poses a major global health threat, yet the effectiveness of national action plans (NAPs) remains uncertain. Here we developed a multidimensional One Health governance index through a structured Delphi expert consultation to evaluate AMR governance across 193 countries (2017–2022), integrating 269 policy documents, expert-weighted indicators and multinational survey and surveillance datasets. Difference-in-differences and joinpoint regression analyses were used to link governance to antimicrobial use, AMR prevalence and AMR-related mortality. Global governance scores improved from 30.7 to 44.5/100, although implementation and monitoring lagged behind policy design, particularly in animal and environmental sectors. A significant increase in AMR prevalence scores was observed only 5 years after NAP adoption (two-stage difference-in-differences, β = 2.43, 95% confidence interval (CI) 1.02–3.85, P < 0.05), underscoring the delayed impact of policy. Multisector engagement (early-adopting countries, β = 0.05, 95% CI 0.02–0.08, P < 0.01) and antimicrobial use surveillance system (early-adopting countries, β = 0.05, 95% CI 0.03–0.07, P < 0.01) showed the strongest associations with improvement in AMR outcomes. As the 2026 Global Action Plan update approaches, sustained financing and integrated One Health surveillance, with stronger environmental and agricultural engagement, are essential for translating NAPs into sustained reductions in resistance.
Similar content being viewed by others


Main
AMR represents a multidimensional threat to global health and was responsible for an estimated 4.71 million deaths worldwide in 20211,2. Without effective interventions, the annual mortality attributable to AMR is predicted to rise to 8.22 million by 20502, with projected economic losses of up to 3.8% of global gross domestic product, which could lead to an increase of 28 million people in extreme poverty3.
Recognizing the need for a coordinated global response, the 68th World Health Assembly formally adopted the Global Action Plan (GAP) on Antimicrobial Resistance in 2015, calling on all countries to develop and implement NAPs grounded in One Health4,5. The plan outlines five strategic objectives focusing on human, animal and environmental health, promoting countries to operationalize them through NAPs5. This governance architecture was substantially strengthened in 2021 with the establishment of the Quadripartite collaboration, incorporating the United Nations Environment Programme (UNEP) into the existing partnership between the World Health Organization (WHO), the Food and Agriculture Organization (FAO) and the World Organization for Animal Health. Importantly, this expansion elevated the environmental dimension of AMR governance to parity with human and animal health priorities6.
Global attention increased following the development and operationalization of NAPs for AMR, but their rollout has progressed more slowly than anticipated1. Although 178 countries have established NAPs, only 68% are currently being implemented, and 11% have dedicated funding7. Recognizing these implementation gaps, 2024 emerged as a milestone in the global AMR response when the second United Nations High-Level Meeting on AMR adopted a political declaration comprising 106 commitments7, followed by the 4th Global High-Level Ministerial Conference on AMR, which prioritized the shift ‘from declarations to implementation’8.
Tracking progress on outcomes is critical for assessing the influence of the GAP framework and ensuring effective implementation of NAPs. However, current analyses of AMR governance effectiveness remain limited, as they largely rely on textual comparisons of NAP documents or results from the Tracking AMR Country Self-Assessment Survey (TrACSS)9,10,11. While some studies provide detailed comparisons of AMR governance across countries, they typically provide cross-sectional snapshots without adequately capturing longitudinal trends in policy implementation or assessing the actual effectiveness of national strategies12,13,14,15. As emphasized in the WHO’s 2021 review of the GAP on AMR, there remains an evidence gap concerning how national policies influence tangible AMR-related outcomes, such as reductions in AMR-related disease burden, pathogen prevalence and antimicrobial use (AMU)16.
To address these gaps, we developed a multidimensional governance-outcome evaluation index and analyzed global trends from 2017 to 2022. In this study, AMR governance refers to policy design, implementation and monitoring mechanisms that enable countries to develop, operationalize and sustain effective responses to AMR. Our outcomes include AMU, AMR prevalence and AMR-related disease burden. By integrating multidimensional governance indicators with longitudinal AMR outcome data, this study quantitatively assesses progress in national AMR governance across policy design, implementation and monitoring. It further examines whether national AMR governance has contributed to measurable improvements in AMR-related outcomes since the adoption of the GAP, and identifies the governance dimensions most strongly associated with these improvements. A summary of our findings and their policy implications is presented in Table 1.
Results
NAP coverage and governance index structure
As of January 2025, our database consisted of 200 publicly available NAPs from 148 countries (Fig. 1a). Of these, 45 countries had published a second version, and 7 had released third versions (Supplementary Table 15). Before the launch of the GAP, only 17 countries had issued an AMR NAP. The earliest plan we identified was published by Greece in 2008. Although the first edition of the GAP urged all member states to develop their NAPs within 2 years, only about a third (77 countries) had done so by the end of 2017, reflecting limited early uptake and uneven policy engagement. Geographically, NAP adoption varied considerably across WHO regions. Adoption reached 100% in the South-East Asia Region (SEARO, 11 out of 11) and the Eastern Mediterranean Region (EMRO, 21 out of 21), followed by the Western Pacific Region (WPRO, 23 out of 27, 85%) and the European Region (EURO, 43 out of 53, 81%). By contrast, only 35 out of 47 countries in the African Region (AFRO, 74%) and 15 of 35 countries in the Region of the Americas (AMRO, 43%) had published NAPs.

a, Year of launch of the first publicly available AMR NAP by country (n = 148). The timeline (right) summarizes the cumulative number of countries with available NAPs by year, with notable pre-GAP (before 2015) adopters marked. b, Conceptual framework linking AMR governance and outcomes. The governance index (left) includes three domains (policy design, implementation and monitoring), with the three outcome domains (AMU, AMR prevalence and disease burden) to the right. Bacterial priority tiers for AMR prevalence are as defined in the WHO Bacterial Priority Pathogens List 202445. Base map generated using the Standard Map Service platform provided by the Ministry of Natural Resources of China (http://bzdt.ch.mnr.gov.cn/).
The AMR governance index comparison is presented in Fig. 1b. ‘Policy design’ captures political commitment and strategic planning; ‘implementation’ assesses operational capacity against the five GAP objectives; and ‘monitoring’ evaluates progress, including reporting and policy adjustments, to ensure that NAPs function as dynamic, adaptive instruments rather than static documents.
Three outcome domains are linked to the governance index: AMU, AMR prevalence and disease burden (Fig. 1b). AMU covers human, animal and environmental sectors following a One Health approach. AMR prevalence includes drug-resistant pathogen combinations under the WHO’s critical-, high- and medium-priority tiers, while the disease burden includes both AMR-associated deaths and AMR-attributable deaths. The complete governance–outcome framework is provided in Supplementary Table 12.
AMR governance scores by domains, sectors and regions
Between 2017 and 2022, global AMR governance scores increased steadily (Fig. 2a, Extended Data Fig. 1 and Supplementary Fig. 1). In 2022, the global average AMR governance score was 44.5 (s.d. 21.7), with considerable variation across countries. However, progress was uneven across governance domains: while policy design and monitoring improved notably over time, the implementation domain and its associated subdomains progressed more slowly (Fig. 2b); in 2022, policy design scored significantly higher than both implementation and monitoring (P < 0.001; Extended Data Fig. 2). Sector-specific scores also revealed notable disparities: the human health sector scored highest (mean 56.1, s.d. 28.4), followed by the animal health sector (45.5, 29.6) and the environmental sector (18.3, 17.4) (Extended Data Fig. 3). The large standard deviation values indicate considerable variation across countries within each sector; regionally, AMR governance scores improved steadily from 2017 to 2022 (Fig. 2c). However, implementation in EMRO, EURO and AMRO showed no significant upward trends (P > 0.05; Extended Data Fig. 4).

a, Heatmap showing annual global mean scores for 14 AMR governance subdomains, grouped into three domains: policy design (I 1.1–1.4), implementation (I 2.1–2.7) and monitoring (I 3.1–3.3). b, Linear trends in the annual global mean scores for each governance domain. Points indicate annual global mean scores. Lines show ordinary least-squares linear regression fits over time, with shaded bands indicating 95% CIs for lines. Statistical significance of temporal trends was assessed using two-sided tests of the regression slope. c, Regional trajectories of overall AMR governance scores across six WHO regions (2017–2022). Solid lines represent annual regional mean scores, and shaded bands indicate ±1 s.d. around the mean. d, Regional trends for all 14 subdomains across six WHO regions and the global average (2017–2022).
At the subdomain level, globally, sustainability (subdomain indicator (I) 1.3) declined temporarily after 2020 but recovered by 2022, while hygiene and prevention (I 2.6) targeting AMR declined after 2019 (Fig. 2d). Although it had rebounded by 2022 in most regions, it did not return to pre-2019 levels. In 2022, public awareness (I 2.5) was the weakest subdomain globally (mean 28.3, s.d. 20.1), while research innovation (I 2.7) showed the largest variability across countries (mean 45.5, s.d.39.5). Policy adjustment (I 3.2) continued to improve across regions (mean 34.0, s.d. 28.0), whereas effectiveness (I 3.3), which assesses how effectively the GAP guides AMR governance including policy design and implementation, ranked as the second-lowest subdomain globally (mean 28.0, s.d. 23.8). As shown in Fig. 2d, SEARO consistently led across all policy design subdomains from 2017 to 2022, while EMRO demonstrated the most rapid improvement. By contrast, AMRO remained the lowest-performing region throughout the period (Extended Data Fig. 5). Despite progress in reporting (I 3.1) in SEARO and EMRO, gains in EMRO’s implementation and policy adjustment (I 3.2) declined continuously from 2020 to 2022. Although EURO overall demonstrates strong governance performance, countries in Eastern Europe and Central Asia (EECA) lagged behind other EURO countries on the total index and across most subdomains, except for accountability (I 1.4) (Extended Data Fig. 6).
Temporal and regional patterns of AMU and AMR prevalence
Between 2000 and 2021, global AMU and AMR prevalence scores declined continuously (Supplementary Figs. 2 and 3). AMU scores declined modestly globally, with no obvious changes in the EURO and EMRO regions between 2015 and 2021.
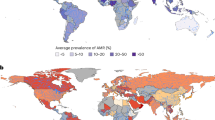
Between 2000 and 2021, AMR prevalence scores varied markedly by region. The highest performance was observed in the AFRO and EURO regions, with the lowest scores in SEARO and EMRO (Fig. 3a,b). Within EURO, EECA showed lower AMR prevalence scores and higher AMU scores than other WHO European countries (Extended Data Fig. 6c).

a, Annual trajectories of AMU scores by WHO region (2000–2021). b, Annual trajectories of AMR prevalence scores by WHO region (2000–2021). Dotted lines indicate the release of the GAP in 2015. Solid lines represent annual regional mean scores, and shaded bands indicate ±1 s.d. around the mean.
Associations between NAP adoption and AMR-related outcomes
Across all three estimators in the staggered-adoption difference-in-differences (DID) framework, a delayed but measurable improvement in AMR prevalence emerged several years after adoption (Fig. 4a). The stacked event-study model showed a significant effect in year 4 (β = 0.83, 95% CI 0.09–1.57, P < 0.05), which increased considerably in year 5 (β = 1.90, 95% CI 0.76–3.03, P < 0.05). This was supported by the two-way fixed-effects ordinary least squares (TWFE OLS; β = 2.07, 95% CI 0.77–3.37, P < 0.05) and two-stage DID models (β = 2.43, 95% CI 1.02–3.85, P < 0.05), with the largest estimated effect of policy on resistance trends observed in the fifth year post-adoption. Effect sizes continued to increase over subsequent years. By contrast, NAP adoption was not associated with detectable post-adoption changes in AMU score or AMR-associated and AMR-attributable deaths (Fig. 4b–d). Sector-disaggregated analysis showed no statistically significant differences in post-adoption effects across human, animal and agricultural crop production AMU (Extended Data Fig. 7).

a–d, Heterogeneous DID estimates of the effects of NAP adoption on AMR prevalence score (a), AMU score (b), AMR-attributable deaths (c) and AMR-associated deaths (d). The unit of study is the country–year observation. The analytical sample includes n = 193 countries for a, c and d, and n = 172 countries for b. For each country, the year of NAP adoption is defined as event time zero (t = 0); negative values indicate years before adoption, positive values indicate years after adoption, and t = −1 serves as the reference year. Control countries were those that had not yet adopted or had never adopted NAPs, whereas countries contributed to the treatment group from the year of NAP adoption onward. Points represent estimated treatment effects for each year relative to the reference year (t = −1), with error bars indicating 95% CIs. Three models are shown: the two-stage DID, the stacked event-study DID and TWFE OLS. e, Joinpoint regression analysis of global and regional AMR trends (2000–2021), showing APCs by time segment. Key inflection points are indicated by stars.
Furthermore, Fig. 4e illustrates temporal changes in the average AMR prevalence score across different regions. Following the launch of the GAP in 2015, the global decline in AMR prevalence notably decelerated. The annual percent change (APC) in global AMR prevalence slowed from −1.32% during 2005–2015 to −0.52% during 2015–2019 (P < 0.05), and stabilized at (APC −0.21%, P < 0.05) during 2019–2021.
In EURO, which initiated a regional AMR action plan in 2011, AMR prevalence declined even earlier after 2011, with minimal changes observed after the GAP launch (APC −0.04%, P > 0.05), indicating ongoing reductions in resistance and potential for policy reinforcement and implementation. Most regions showed similar slowdowns following 2015. However, both the AFRO and SEARO regions maintained significant negative trends in AMR prevalence after the GAP launch (APC −0.74% and APC −0.76%, respectively, P < 0.05), indicating ongoing reductions in resistance and potential for policy reinforcement and implementation.
Governance subdomains associated with the change of AMR prevalence
Figure 5 illustrates the governance subdomains significantly associated with national improvements in AMR prevalence scores. Among 17 early-adopting countries (those with NAPs launched before the GAP; mean ΔAMR in 2021: 5.84, 95% CI 3.16–8.52), four subdomains showed significant positive associations with AMR improvement: strategic vision (I 1.1; β = 0.09, 95% CI 0.02–0.16), multisector engagement (I 1.2; β = 0.05, 95% CI 0.02–0.08), AMU surveillance system (I 2.1; β = 0.05, 95% CI 0.03–0.07) and AMR surveillance system (I 2.2; β = 0.06, 95% CI 0.00–0.12). In the 29 countries achieving the greatest gains in AMR prevalence score (mean ΔAMR in 2021: 10.80, 95% CI 9.16–12.44), multisector engagement (I 1.2; β = 0.05, 95% CI 0.02–0.09) and AMU surveillance system (I 2.1; β = 0.04, 95% CI 0.02–0.07) remained the strongest positive predictors.

a, Associations in 17 early-adopting countries with NAPs launched before the GAP. b, Associations in 29 countries with the greatest AMR prevalence improvements. Each point represents the estimated association (regression coefficient) between a governance subdomain score and the change in AMR prevalence score; error bars indicate 95% CIs. P values were obtained from two-sided tests of the null hypothesis that the coefficient was equal to zero.
Discussion
This study provides a longitudinal analysis linking AMR governance to real-world outcomes at the global level, framed within a One Health approach. Global AMR governance scores rose steadily from 2017 to 2022, although progress varied across domains. Policy design advanced substantially worldwide, reflecting a growing recognition of AMR as a critical issue and a commitment to long-term strategic planning. Nevertheless, implementation and monitoring remain comparatively weak, with persistent structural gaps across regions. Limited investment in AMR-related education and communication has left public awareness (I 2.5) underdeveloped, while hygiene and prevention (I 2.6) and AMU/AMR surveillance systems have also shown slow progress. The environmental sector has demonstrated limited advancement. Fluctuating trends in sustainability (I 1.3) and hygiene and prevention (I 2.6) may partly reflect disruptions caused by COVID-19 pandemic, during which infection-prevention measures were emphasized, and overwhelmed staff capacity and systematic breakdowns in infection prevention and control protocols constraining AMR-specific efforts17,18. Furthermore, policy adjustment (I 3.2) remains stagnant, with limited evidence-based policymaking. Norway exemplifies best practice, using Norwegian Surveillance System for Antimicrobial Drug Resistance/Norwegian Veterinary Institute monitors AMR in bacteria from feed, food and animals (NORM/NORM-VET) data to refine its AMR policies, such as cutting hospital broad-spectrum antibiotic use by 22% by 2020, aligning with GAP objectives for data-driven governance and prudent AMU19. Effectiveness (I 3.3) scores remain lower than other indicators but have increased slightly over time, reflecting the gradual integration of GAP objectives into countries’ AMR governance, with an increasing number of countries incorporating these objectives and action points as time progresses5,20. Notably, as a guiding document for countries to develop their NAPs and AMR governance strategies, the GAP does not inherently define the merit of alignment with its objectives. Instead, the relatively low effectiveness scores are more likely to be attributable to the limited implementation of AMR governance measures, which in turn results in suboptimal outcomes relative to both GAP objectives and countries’ respective action plans, which underscores the essential need for more comprehensive implementation of national AMR governance frameworks in the future. Achieving full convergence will require sustained political commitment, long-term investment and continuous policy refinement given the relatively low current result.
Our analysis further highlights substantial regional heterogeneity. EURO maintained strong governance performance, while EMRO, SEARO and AMRO lagged behind. Public awareness (I 2.5), hygiene and prevention (I 2.6), sustainability (I 1.3) and surveillance capacity (I 2.1 and I 2.2) remain underdeveloped and uneven. SEARO led in policy design, especially in strategic planning (I 1.1) and multisector engagement (I 1.2), a finding that aligns with a WHO-led situation analysis21. EMRO achieved rapid gains in reporting (I 3.1), while AMRO showed only limited progress in both implementation and reporting (I 3.1).
Taken together, although AMR governance is strengthening, insufficient implementation, sectoral imbalance and uneven regional progress constrain its effectiveness, underscoring the need for region-specific support and sustained financing.
This study reveals that policy impacts of NAPs on AMR are not immediate but follow a delayed trajectory, with measurable reductions in AMR prevalence typically emerging 4–5 years after NAP adoption. This lag probably reflects underlying biological dynamics, as resistant strains and resistance genes can persist for several years before declining following reduced antimicrobial pressure22. In parallel, this lag is consistent with the time required for AMR policies to translate into behavioral change, institutional reform and, ultimately, decreases in AMR prevalence23. Global reviews note that measurable improvements depend on long-term shifts in prescribing norms, regulatory enforcement and system-level investment11,24. Country examples illustrate this temporal pattern. China showed measurable improvements in AMR governance 3 years after adopting its NAP, accompanied by policy measures such as expanded AMR surveillance networks, programs to strengthen hospital diagnostic and treatment capacity, and programs to reduce veterinary AMU25. Correspondingly, measurable declines in AMR prevalence emerged 5 years after policy adoption, consistent with the expected lag. Similarly, global reviews note that measurable improvements depend on long-term institutional and behavioral change11,24. Earlier and more proactive responses are associated with earlier gains; in Europe, for instance, the AMR trajectories began to plateau following the launch of the regional action plan in 201126. Interestingly, this pattern manifested even more rapidly in Senegal, where measurable improvements were observed within 2 years of adopting its NAP in 2017, probably accelerated by targeted external support from the Fleming Fund and Multi Patterner Trust Fund27.
While AMR prevalence shows a delayed improvement following NAP adoption, we observe no significant decrease in AMU, consistent with findings from Charani et al.24. This may be attributable to the progressive strengthening of national AMU surveillance capacities, and subsequent improvements in reporting systems may have led to more complete AMU data rather than lack of reduction in use28. Alternatively, the pattern may indicate a shift toward more rational antimicrobial prescribing, reducing unnecessary use while maintaining clinical use, which would improve the quality of antimicrobial stewardship without requiring large reductions in total AMU volume29.
Among governance subdomains, multisectoral engagement (I 1.2) and AMU surveillance system (I 2.1) were the most consistent predictors of reductions in AMR prevalence across both early-adopting countries and those with the greatest declines in resistance. Early-adopting countries achieved notable reductions in AMR prevalence by establishing a clear vision, systematically tracking AMU and coordinating priorities across human, animal and environmental sectors. This association provides evidence that countries capable of systematically tracking AMU also tend to possess stronger regulatory capacity and stewardship mechanisms that act on the data generated. Likewise, multisectoral engagement (I 1.2) reflects the extent to which different sectors coordinate their priorities and resources to translate policy commitments into cross-sectoral implementation. These findings highlight how different governance features may carry weight in different contexts, with some serving as early enablers of progress and others reflecting the core capacities most closely tied to sustained improvements.
By contrast, several traditional interventions appear to show limited impact on reducing resistance. This is probably attributable less to intrinsic ineffectiveness and more to systemic implementation constraints. Interventions such as professional education or public awareness campaigns may require a longer time to yield outcomes. Others, such as hygiene, prevention and stewardship, often remain underfunded, inconsistently implemented, or narrowly focused on a single sector. These weaknesses underscore why the adoption of NAPs and GAPs has so far yielded only modest effects, with measurable AMR prevalence improvements often observable only several years after adoption. Hence, a globally coordinated, scientifically guided framework across the human, animal, agricultural and environmental sectors is needed to enable countries to take ownership in translating interventions into tangible improvements in AMR-related outcomes—for example, by reducing AMU through the Reduce the Need for Antimicrobials on Farms for Sustainable Agrifood Systems Transformation (RENOFARM) initiatives30.
The 2026 revision of the GAP provides a pivotal opportunity to strengthen global AMR governance by consolidating and expanding implementation7, creating a unique window to translate commitments into reforms that deliver measurable and lasting impact.
Without comprehensive investment across all NAP domains, countries are unlikely to reverse resistance trends. EECA countries continue to lag behind other EURO countries in key governance domains—particularly multisectoral coordination, AMR/AMU surveillance and effectiveness—potentially due to underfunding, fragmented collaboration, limited data integration and weak implementation of AMR governance measures. Conversely, stronger AMR governance and implementation in Western and Northern Europe have demonstrated measurable declines in AMR prevalence. These patterns further indicate that progress concentrated in policy design without parallel advances in implementation has been associated with slower and less substantial reductions in resistance.
A stepwise, context-specific approach is required; early-stage NAP countries should begin by establishing robust multisectoral governance structures to coordinate across sectors and sustain them through NAP cycles and a nationwide AMU data collection system. As capacity develops, the focus should shift toward strengthening AMR surveillance systems, improving AMU data collection to higher resolution, and addressing major gaps, such as awareness-raising, hygiene and prevention. In more mature economies, priorities should move beyond basic capacity (for example, multisectoral collaboration and AMU data collection) toward a strategic vision with clear goals, measurable milestones and defined outcomes, ensuring the sustainability of AMR efforts through legislation, institutionalization and policy coherence that protect the gains achieved. The UK’s 20-year (2020–2040) AMR Vision exemplifies this transition, supported by a national plan focused on infection prevention and control, data-driven action and expanded integrated AMR surveillance across environmental and food sectors31. At the global level, the adopted political declaration sets concrete targets, such as reducing AMR-related deaths by 10% by 2030, embedding sustainable stakeholder engagement and accountable governance into the global AMR response7. Across all contexts, situational analyses should guide the prioritization of high-impact and feasible interventions, with particular focus on the most persistent gaps. Ultimately, the goal is comprehensive and sustained investment across all domains of NAPs to achieve lasting progress against AMR.
In addition, the crop production and environmental sectors require more equitable attention within GAP and NAPs. The relatively low scores in the environmental sectors, which in this analysis also encompass crop production, illustrate a critical blind spot. Evidence shows that environmental pathways, such as wastewater, effluents and agricultural runoff, along with crop production practices, contribute directly to resistance dissemination32. Emerging evidence further identified growing interconnections between climate change and AMR33. Climate and socioeconomic factors jointly contribute to increasing AMR burdens with geographic variations projected under different climate scenarios34. Other ecological studies have shown that rising ambient temperatures are associated with elevated levels of antibiotic resistance, particularly in colder regions35,36. These climate–environment interactions underscore the urgency of addressing environmental AMR dynamics, yet evidence in this area remains limited, leaving critical drivers of resistance insufficiently addressed. While the ongoing FAO initiative includes an action stream on AMR in the agri-environment and UNEP provides policy guidance on AMR pollution management, greater technical and financial investment is required to address these gaps and build sustainable environmental AMR surveillance and management systems at both global and national levels30,37. Practical interventions, such as strengthening water, sanitation and hygiene (WASH) systems to reduce infection transmission, represent a cost-effective means of lowering antimicrobial demand and complementing governance, stewardship and surveillance efforts38.
Integrated surveillance under the umbrella of the national multisectoral AMR coordination mechanism is essential for unified data sharing and informing policymaking. Countries should steadily strengthen their national integrated AMR/AMU surveillance systems, such as the Danish Integrated Antimicrobial Resistance Monitoring and Research Programme (DANMAP). Established through collaboration among veterinary, food and health authorities, it monitors resistance in bacteria of those sectors and links AMU data via VETSTAT. Its standardized sampling, harmonized testing and centralized databases enable cross-sectoral comparison and provide evidence for targeted policy interventions39,40. Subsequently, emphasis should be placed on progressively extending integration to crop agriculture and the environment, in line with guidance from the Quadripartite Technical Group on Integrated AMR/AMU surveillance, and participating in global AMR/AMU data-sharing platforms. Genomic surveillance of resistance genes has strong potential to complement conventional systems to enhance future integrated monitoring. It enables early detection of AMR threats, provides higher-resolution insights into transmission dynamics across humans, animals and the environment, and supports timely, evidence-based interventions41.
Global AMR research and development (R&D) capacity remains unevenly polarized, with high-income countries concentrating resources and outputs, while low- and middle-income economies (LMIEs), facing the greatest burden of AMR, are constrained by limited scientific infrastructure and capacity. AMR R&D must embed principles of prudent and responsible AMU and prioritize preventive strategies, including vaccine development and non-antibiotic interventions. Such approaches would generate sustainable One Health solutions and reduce reliance on antimicrobials42. Stronger public–private partnerships are also needed to harness industry expertise and accelerate translation of research into accessible solutions.
Previous global assessments of AMR governance, including Zhou et al.15 and Patel et al.12,13, have provided valuable cross-sectional snapshots of governance maturity using fuzzy analytic hierarchy process (AHP), arithmetic mean and principal component analysis, respectively, across 146–161 countries. The most recent study by Patel et al.13 systematically mapped AMR governance and linked governance scores to disease burden, identifying that disparities in policy maturity and implementation tools—particularly infection prevention and control, surveillance systems and antimicrobial stewardship—were most strongly correlated with lower burden of drug-resistant infections. However, their single-year studies could not capture temporal dynamics, policy evolution or the lagged effects of governance interventions on AMR outcomes.
Our study uses dynamic, outcome-focused policy evaluation. It uses a longitudinal design covering 2017–2022 across 193 countries, integrating reconciled multisectoral data from comprehensive sources to examine governance trajectories over time rather than relying on cross-sectional status. The analysis applies a One Health-framed multidimensional governance index that combines expert consultation (Delphi method) with quantitative weighting (entropy method). This approach preserves policy interpretability while supporting comparability across years, addressing limitations of methods such as principal component analysis, arithmetic averaging and fuzzy AHP approaches commonly used in cross-sectional studies.
Although the Patel et al.13 study linked governance to disease burden using cross-sectional correlation, this approach cannot inform evidence-based prioritization of governance investments. Our study moves beyond descriptive governance mapping by linking governance to three outcome domains: AMU, AMR prevalence and disease burden. Using DID and panel regression models that account for policy timing and implementation lags, we provide direct evidence that sustained NAP implementation can achieve measurable reductions in AMR prevalence, with effects typically emerging only after 4–5 years—delayed impacts that cross-sectional designs cannot detect. By clarifying which governance subdomains and intervention priorities drive measurable improvements, for which outcomes and on what implementation timeline, our longitudinal approach provides essential evidence for realistic policy evaluation cycles and evidence-based prioritization of governance investments at national and global levels.
Several limitations should be noted. First, the expert panel’s composition may limit its ability to capture context-specific implementation barriers. Despite sensitivity analyses showing minimal impact on final weights, the predominance of participants from China may have introduced a residual regional bias, thereby limiting the framework’s generalizability, particularly in underrepresented regions. A more geographically balanced panel would better account for regional heterogeneity in AMR governance challenges. Furthermore, limitations arise from the data sources used to construct the governance scores; the governance assessment relied heavily on available NAPs and self-reported TrACSS questionnaires. Given cross-country variations in AMR understanding and reporting capacity, these sources may be subject to optimism bias, as countries potentially overestimate their implementation progress.
Second, data availability constrained both the framework’s composition and the analytical scope. Despite comprehensive searches, only 148 of the 178 countries reported by WHO to have adopted NAPs could be identified and analyzed, and relatively few countries had long post-adoption windows. This potential gap, combined with the study period (2017–2021), which captures predominantly early implementation phases, limits our ability to assess whether observed improvements represent sustained trends or temporary effects. The lack of countries with extended post-adoption observation windows (more than 5 years) may bias estimates if early adopters systematically differ from later ones in governance capacity or baseline AMR burden. A longer follow-up is essential to determine whether governance efforts translate into durable reductions in AMR.
In addition, data limitations across sectors meant that the framework could not fully represent the One Health dimension of AMU. Although an objective weighting approach was used to mitigate subjective bias, the entropy-based weights themselves may have been influenced by extrapolated or imputed data, potentially failing to capture real-world heterogeneity. A specific challenge arose in constructing an indicator for environmental exposure. Following expert consultation, the framework was designed to capture AMR broadly, but data accessibility limited our measurement to agricultural crop production AMU, representing only one environmental exposure pathway. This narrow focus weakens the outcome indicators’ alignment with One Health principles, as it excludes other critical environmental pathways such as pharmaceutical manufacturing and animal-production effluents. An ideal, fully integrated framework would encompass comprehensive environmental exposure data to capture these broader contamination and feedback pathways. Future work should leverage standardized and continuously updated datasets, such as the Global Antimicrobial Resistance and Use Surveillance System (GLASS) and the International FAO Antimicrobial Resistance Monitoring System (InFARM), to enhance comparability and integration with policy metrics.
Fourth, although COVID-19 is not the focus of this study, its overlap with 40% of our primary study period (2017–2021) presents a major analytical challenge. While overall AMU levels appeared stable, shifts toward broader-spectrum and reserve antibiotics during this period may have influenced observed resistance patterns, as reported in previous studies43,44. The full impact of these pandemic-related disruptions could not be fully quantified or reflected in the AMU data imputation and needs to be further investigated. Although we implemented strategies to control for pandemic effects in both DID and panel regression analyses, these adjustments cannot fully eliminate potential confounding. The pandemic period also increases the risk of violations of the parallel-trends assumption in the DID framework, particularly if AMU/AMR trends differentially shifted unevenly between early and late NAP adopters. Future research should explicitly examine pandemic impacts across pre-, during- and post-pandemic phases to disentangle policy effects from pandemic-related disruptions. Finally, although we applied the Benjamini–Hochberg correction to address multiple testing, residual risk of false positives remains and findings should be interpreted with caution.
Although the adoption of NAPs has expanded globally, meaningful reductions in AMR require sustained and multisectoral implementation, coordination and surveillance over multiple years. Countries must prioritize integrated One Health surveillance and ensure targeted and sustained financing tailored to their specific contexts and capacities. By leveraging current political momentum and shifting the focus from declarations to action, the global community can advance toward measurable improvements in AMR-related outcomes.
Methods
Study design
This study used a longitudinal, country-level design to evaluate AMR governance and its association with AMR-related outcomes over time. We first constructed an indicator-based index to characterize national AMR governance across multiple domains (Extended Data Fig. 8a). We then examined temporal changes in governance and evaluated associations between governance trajectories and AMR-related outcomes to assess policy effectiveness and identify governance components associated with improvement.
Data sources
We assembled a longitudinal country-level dataset spanning 2000–2021 across 193 entities, including 190 United Nations Member States together with the Cook Islands, the State of Palestine, and Bermuda (Non-Self-Governing Territories), hereinafter referred to as countries. We evaluated several alternative regional classification schemes and ultimately adopted the WHO regional characterization, as it more effectively captures heterogeneity across regions. In Asia in particular, the WHO framework distinguishes the Eastern Mediterranean, South-East Asia and Western Pacific regions, reflecting important differences in AMR governance trajectories. Details of the countries included and their regional classifications are provided in Supplementary Tables 1 and 2.
Governance indicators for 193 countries were derived from national AMR policy documents, the TrACSS, United Nations Children’s Fund (UNICEF), the Global AMR R&D Hub (https://dashboard.globalamrhub.org/) and the GLASS database (Supplementary Tables 13 and 14). The study period (2017–2022) was determined based on the availability of TrACSS survey data; the 2016 questionnaire contained insufficient items and was therefore excluded. Data collection was completed in November 2024. From 832 national policy documents, 269 documents (200 NAPs and 69 related policy or legal documents) were retained for in-depth analysis. Native-language NAPs (n = 118 in 39 languages) were translated using Google Translate (Extended Data Fig. 8b and Supplementary Table 15). Four researchers (W.C., Y. Zeng, Z.C. and J.Q.) reviewed these documents independently and rated governance indicators on the basis of Cochrane Systematic Review standards, with discrepancies resolved through group discussion or third-party arbitration (M.L.)46. Full search strategy, list of indicators, coding rules and standardization methods are included in the Supplementary Information.
AMR-related outcome data (2000–2021) combined AMR prevalence, AMU and AMR-related mortality. AMR prevalence was defined as resistance rates among pathogens listed in the WHO Bacterial Priority Pathogens List (2024)45, with national estimates obtained from the Global Burden of Disease (GBD) 2021 AMR study2, supplemented by data from the Institute for Health Metrics and Evaluation HealthData VizHub platform (https://vizhub.healthdata.org/microbe/) and rifampicin-resistant tuberculosis (TB) estimates from WHO Global TB Reports (https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/data). AMR-associated deaths were defined as deaths caused directly by AMR infections, while AMR-attributable deaths referred to deaths in which AMR contributed but was not the direct cause; both mortality measures were derived from the GBD cause-of-death framework2. AMU indicators consisted of three components: human AMU, animal AMU and agricultural crop-production AMU. Human AMU data (defined daily doses per 1,000 population per day) were obtained from global antibiotic consumption estimates for 2000–2018 from Browne et al.47. Animal AMU data (mg per population correction unit) were sourced from estimates by Mulchandani et al.48 and were available only for 2020. Agricultural crop-production AMU data (tons of active ingredient per hectare) were calculated from agricultural use of fungicides and bactericides in crop production from FAOSTAT (https://www.fao.org/faostat/en/#data/RP) normalized by arable land area. An overview of outcome indicator data inputs is provided in Supplementary Table 16.
Missing data handling
Countries or territories with structurally missing data for either animal AMU or agricultural crop-production AMU across all study years were excluded from composite AMU score construction to avoid systematic bias arising from incomplete sectoral representation. For the remaining 172 countries, missing AMU data were handled using component-specific imputation strategies designed to preserve within-country temporal structure and cross-country heterogeneity.
Missing human AMU values for 2019–2021 were projected using country-specific autoregressive integrated moving average (ARIMA) models fit independently to each country’s observed AMU trajectory from 2000 to 2018 via the auto.arima() function in the ‘forecast’ package. This approach preserves the country-specific temporal patterns in antimicrobial consumption by extrapolating trends independently rather than borrowing information across countries. Point estimates were used in AMU score construction.
Animal AMU time series for 2000–2021 were constructed by backcasting and forecasting from observed 2020 values using country-specific APCs derived from each country’s sociodemographic index (SDI) trajectory from GBD 2021 SDI dataset49. We assumed that temporal changes in animal AMU approximately follow each country’s sociodemographic development trajectory. Socioeconomic development, urbanization and dietary transition are key drivers of livestock intensification and veterinary antimicrobial consumption; these processes are well captured by the GBD SDI50,51,52. Using the 2020 observed AMU value as a baseline, yearly values were generated via exponential backcasting and forecasting:
where \({A}_{i,2020}\) represents the observed animal AMU value for country i in 2020 and \({\mathrm{APC}}_{i}\) is derived from the SDI trajectory for country i.
Agricultural crop-production AMU was derived from national reports of fungicide and bactericide use in the FAOSTAT database (https://www.fao.org/faostat/en/#data/RP), normalized by arable land area (tons of active ingredient per hectare, t ha−1). Only three countries (Serbia, Sudan and Montenegro) had limited missing values, which were imputed using within-country resampling from available observations to preserve country-specific distributional characteristics. Countries with no observed crop-production AMU values were not imputed and were excluded from the AMU composite score.
Missing data imputations for AMU were conducted in R (version 4.3.2). Key packages included ‘tidyverse’ (data processing), ‘forecast’ (ARIMA modeling) and ‘dplyr’ (data restructuring).
Delphi consultation and governance framework development
We developed a structured governance evaluation framework informed by a synthesis of existing assessment tools and conceptual models proposed in previous research and policy reports11,12,15,16,53.
An international expert panel (n = 38; Supplementary Table 8) from diverse areas (clinical medicine, veterinary medicine, environmental science and so on) was formed. Between June and November 2024, the panel refined the framework via virtual roundtable discussion and two Delphi survey rounds, generating a draft indicator list that was finalized through structured questionnaires54. Candidate indicators were identified a priori based on international policy frameworks, including the WHO GAP on AMR, NAPs and existing surveillance and governance literature. Experts scored each indicator using a five-point Likert scale ranging from 1 (‘very unimportant’) to 5 (‘very important’). In addition to importance scoring, experts reported two self-assessed components to quantify the reliability of their judgments: (1) the basis of judgment, reflecting the relative contribution of theoretical knowledge, practical experience, peer understanding and intuition; and (2) familiarity with each indicator55.
The judgment basis coefficient (Ca) was calculated as a weighted sum of the four judgment bases, with weights assigned according to the expert’s self-rated reliance: ‘little’, ‘moderate’ or ‘great deal’ (rated on a scale from 1 to 3). Likewise, the familiarity coefficient (Cs) was derived on the basis of the expert’s familiarity level, mapped to a numerical value from 0.10 (unfamiliar) to 0.90 (very familiar). Weighting criteria are shown in Supplementary Table 3. An expert authority coefficient (Cr) was then calculated as the average of Ca and Cs, where a Cr value greater than 0.70 is generally considered an acceptable indicator of reliability. Descriptive statistics was performed using SPSS 26.0, including the mean, s.d. and coefficient of variation, were used to summarize the central tendency and dispersion of expert ratings56]. Indicators were retained for further analysis only if they achieved a priori consensus criteria, defined as a mean importance score ≥3.5 and a coefficient of variation ≤0.25. To assess agreement among experts, Kendall’s coefficient of concordance (W) was calculated for each Delphi round. The value of W ranges from 0 (no agreement) to 1 (perfect agreement), with a two-sided significance test conducted at α = 0.05. A statistically significant W value (P < 0.05) was considered indicative of acceptable inter-expert agreement57. Indicators meeting the consensus criteria after two rounds were included in the final governance framework. Detailed Delphi results are presented in Supplementary Tables 4–7.
To assess potential regional and income-related bias in expert judgments, we noted that 65.8% of experts were based in China and 34.2% were from other countries. Based on the World Bank classification in 2021, 68.4% were from LMIEs and 31.6% from high-income economies. Region-stratified (China versus Others) and income-stratified (LMIE versus non-LMIE) sensitivity analyses were performed to evaluate the robustness of indicator ratings and weights. Given the non-normal distribution of ratings, between-group comparisons were performed using Wilcoxon rank-sum tests with adjustment for multiple comparisons using Bonferroni and false discovery rate procedures. Analyses were performed in Python (version 3.11.14). LMIE versus non-LMIE and China versus Others comparisons indicate that nearly all indicators were rated equivalently across regions, supporting the global relevance and generalizability of the Delphi-derived AMR governance indicator framework (Supplementary Information).
The final index framework comprises 3 primary governance domains, that is, policy design, implementation and monitoring, divided into 14 subdomains and 46 indicators, and 3 primary AMR-related outcomes, that is, AMU, AMR prevalence and disease burden (Supplementary Table 12). Given the complexity of sectoral contribution to AMR governance, our study classified food safety within the animal sector, while plant production and waste management are included in the environment sector.
Weighting algorithms and integration method
To derive indicator weights for the AMR governance index, AMU and AMR prevalence scores, we used a combined subjective–objective weighting strategy, balancing expert-judged relevance with data-driven variability58,59,60. Subjective weights were obtained through a Delphi-based AHP61, while objective weights were computed using the entropy method62. The two sets of weights were subsequently integrated using a deviation-maximization method to balance expert judgment and data-driven variability. All expert response aggregation, weight computation and integration procedures were implemented in Microsoft Excel (version 16.78) following standardized calculation protocols.
Subjective weighting using Delphi-based AHP
Construction of the judgment matrix
The AHP, introduced by Saaty, is a structured technique widely applied for determining subjective weights in complex multicriteria decision-making scenarios by decomposing the decision problem into a hierarchical framework61. Traditional AHP derives pairwise comparison matrices directly from expert pairwise scoring, and the resulting comparisons populate an \(n\times n\) reciprocal judgment matrix A:
where \({a}_{{ij}}\) represents the relative importance of indicator i compared with indicator j.
However, with 78 indicators in our framework (governance, AMR prevalence and AMU), a full pairwise comparison round would have required \(78\times 77/2\,=\text{3,003}\) individual judgments per expert, creating excessive cognitive burden and making full completion unlikely in a multicountry Delphi panel. To reduce respondent workload and maximize response retention across rounds, we adopted a rating-based AHP approach, in which experts evaluated each indicator using a 1–5 Likert importance scale instead of performing pairwise comparisons.
Following the rating-to-ratio approach commonly applied in Delphi–AHP hybrids63, the relative importance ratings were converted into ratio-scale values as default AHP value to populate the pairwise elements of judgment matrix. This ratio-based transformation has been widely used in Delphi–AHP hybrids, allowing direct numerical ratings to approximate pairwise preference strength while maintaining AHP compatibility64,65.
Derivation of subjective weights
Using the square root method, the principal right-eigenvector of matrix A was extracted and normalized to obtain the subjective weight vector \({\boldsymbol{W}}\), following the standard AHP eigenvalue method:
where \({\lambda }_{\max }\) is the maximum eigenvalue of the matrix, and wj(sub) denotes the subjective weight of indicator 𝑗 derived from AHP.
Consistency testing
To ensure logical coherence of the derived judgment matrix, internal consistency was evaluated using the standard AHP indices:
where CI is the consistency index, n is matrix order and RI is Saaty’s Random Consistency Index. A CR value less than 0.1 was deemed acceptable, indicating reliable judgments; matrices exceeding this threshold underwent revision for improved consistency66. All judgment matrices constructed using the rating-based approach satisfied the AHP consistency criterion (CR <0.10), confirming that the transformation from Likert ratings to ratio-scale comparisons preserved acceptable transitivity and logical coherence.
Objective weighting using the entropy method
The entropy weight method, based on Shannon’s information theory, provides an objective approach to weighting indicators by leveraging inherent data characteristics, thereby minimizing subjective biases62. Within information theory, entropy quantifies uncertainty, with lower entropy indicating greater variability and therefore higher information content, necessitating larger weights67. Original indicator data were first normalized. For policy indicators, positive normalization was applied:
For AMR pattern indicators, inverse normalization was used:
where \({z}_{{ij}}\) represents the normalized value. The weight contribution of each observation was then calculated as
The entropy of each indicator j was computed as
where m is the number of samples and k is the normalization constant. Then, the divergence coefficient for indicator j is calculated as
Finally, the objective weight wj(obj) of each indicator was derived by normalizing divergence coefficients across all indicators:
Integrated weighting method
To systematically integrate subjective and objective weighting schemes and balance their respective advantages, we used a deviation maximization method68,69. This integration process aims to maximize the dispersion of integrated weights, thereby preserving meaningful distinctions among indicators. Specifically, integrated weights were determined by solving the following optimization problem:
where the mean integrated weight \({\underline{\rm{w}}}\) is given by
Subject to the constraints:
This approach ensures that the final integrated weights comprehensively reflect both expert judgment and data-driven evidence.
Indicator weights for the AMR governance index, AMU and AMR prevalence scores are presented in Supplementary Tables 17 and 18. To maintain interpretability across metrics, governance data were positively standardized and converted to a 100-point scale, a common approach for compiling composite indices13,70, while AMU and AMR prevalence scores were reverse-standardized so that higher scores indicate more favorable conditions (that is, lower use or lower resistance).
Statistical analysis
To estimate the association between NAP adoption and AMR-related outcomes under staggered policy implementation, a DID framework allowing heterogeneous treatment effects was applied separately to all outcome variables—AMU score, AMR prevalence score, and AMR-attributable and AMR-associated deaths—using three approaches: TWFE OLS71, the two-stage DID72 and the stacked event-study DID73. Control countries were those that had not yet adopted or never adopted NAPs. Event time was recoded relative to each country’s adoption year, and extreme lead/lag years were grouped (≤–11/≥+8) to ensure adequate sample size. Robustness was assessed through four complementary strategies: (1) three DID estimators that address staggered adoption and treatment heterogeneity; (2) adjustment for ten structural covariates (for example, health expenditure, population density and so on); (3) alternative event windows (±5 years); and (4) three strategies to account for pandemic-era confounding (2020–2021). All robustness analyses yielded consistent results, validating the main findings. Full outputs are provided in the Supplementary Information. All DID analyses were conducted in Stata 18 (StataCorp.).
Joinpoint regression analysis was applied to identify statistically significant inflection points in temporal trends of AMR prevalence scores at the global level and across WHO regions. The model fits log-linear segments to identify statistically significant joinpoints (years in which trend slopes change) using permutation tests and evaluates their timing relative to the 2015 release of the GAP on AMR. For each segment, APC estimates were calculated to quantify the rate and direction of change, with statistical significance indicated at P < 0.05.
To capture heterogeneous post-GAP changes in AMR prevalence relative to historical trends, we constructed a deviation-based outcome (ΔAMR), defined as the difference between observed AMR prevalence during 2015–2021 and values projected from country-specific linear trends fit to the 2000–2014 pre-GAP period. Latent class growth modeling was applied to ΔAMR trajectories using the lcmm package. Models with one to seven classes were evaluated using information criteria, posterior classification probabilities, class-size distributions and interpretability, with a minimum class-size threshold of 10% (refs. 74,75). The final trajectory classification was used to guide downstream subgroup analyses (Extended Data Fig. 9 and Supplementary Information).
From a governance perspective, 17 countries that had adopted NAPs before the 2015 GAP release were selected (Supplementary Table 25). From the outcome perspective, 29 countries that showed the greatest improvements in AMR prevalence were selected via latent class growth modeling trajectory analysis (Supplementary Table 26). To examine governance factors associated with AMR improvements in selected country groups, we estimated country fixed-effects panel regression models with governance subdomain scores as predictors28. Model choice between fixed- and random-effects specifications was guided by the Hausman test (P < 0.001). Clustered robust standard errors were used for inference. For analyses involving multiple governance subdomains, raw P values and Benjamini–Hochberg false discovery rate-adjusted q values were reported to account for multiple comparisons. Analyses were performed in R (version 4.3.2). Details of panel model selection and pandemic-period robustness analyses are provided in the Supplementary Information.
Inclusion and ethics statement
This study was executed through a global, cross-institutional partnership committed to centering equity and local relevance in addressing AMR. Scientists from LMIEs (Pakistan, Bangladesh, China and so on) and high-income countries (the USA, Switzerland, the UK and so on) took part in the study’s execution and Delphi survey. The LMIE researchers ensured the study’s alignment with needs in developing regions, while their counterparts from high-income settings and international organizations provided technical and experiential support. By clarifying the division of roles and responsibilities upfront, the partnership achieved fair allocation of research data, intellectual property and authorship rights.
We have integrated local and regional research relevant to this study into our citations, including the response to AMR in SEARO9 and the review by Yang et al.25 of China’s cross-sector AMR policies. We also incorporated region-specific evidence from WHO’s South-East Asia AMR situational analysis21 and UNEP’s environmental AMR response37, ensuring citations reflect local expertise and contextualize our findings within existing regional evidence.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All data used in this study are publicly available. Governance indicators were extracted from AMR NAPs and related policy documents, TrACSS (https://amrcountryprogress.org/), UNICEF immunization data (https://data.unicef.org/resources/dataset/immunization/), the Global AMR R&D Hub (https://dashboard.globalamrhub.org/) and the WHO GLASS database (https://worldhealthorg.shinyapps.io/glass-dashboard/). NAPs were obtained from the FAO AMR-LEX database (https://amr-lex.fao.org/main/profile/en), the WHO library of AMR NAPs (https://www.who.int/teams/surveillance-prevention-control-AMR/national-action-plan-monitoring-evaluation/library-of-national-action-plans), the AMR NAP Translation Project (https://sites.google.com/view/amrnaptranslations/introduction) and manual retrieval from national government sources. AMR prevalence, AMU (human, animal and agricultural) and AMR-related mortality were obtained from publicly accessible datasets including Browne et al.47, Mulchandani et al.48, FAOSTAT (https://www.fao.org/faostat/en/#data/RP), the GBD AMR study (https://vizhub.healthdata.org/microbe/) and WHO Global TB Reports (https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/). Detailed data sources are provided in the Supplementary Information). The analysis-ready datasets required to reproduce all analyses and figures, including governance indicators, outcome variables, imputed values using numeric country identifiers, and datasets used for sensitivity and robustness analyses, are available via GitHub at https://github.com/SkylarZeng/global_amr_governance_2017-2022.
Code availability
All scripts used to process data and reproduce the analyses are available via GitHub at https://github.com/SkylarZeng/global_amr_governance_2017-2022.
References
Antimicrobial resistance: an agenda for all. Lancet 403, 2349 (2024).
Naghavi, M. et al. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. Lancet 404, 1199–1226 (2024).
World Bank. Antimicrobial resistance (AMR) https://www.worldbank.org/en/topic/health/brief/antimicrobial-resistance-amr (accessed 15 March 2025).
Musicha, P. et al. Time to define One Health approaches to tackling antimicrobial resistance. Nat. Commun. 15, 8782 (2024).
WHO. Global Action Plan on Antimicrobial Resistance https://www.who.int/publications/i/item/9789241509763 (accessed 15 March 2025).
UNEP joins alliance to implement One Health approach. 2022; published online March 21; https://www.unep.org/news-and-stories/press-release/unep-joins-alliance-implement-one-health-approach (accessed 15 March 2025).
United Nations. Political Declaration of the High-level Meeting on Antimicrobial Resistance (2024).
From declaration to action: antimicrobial resistance initiatives centre stage at Jeddah conference. UN News https://news.un.org/en/story/2024/11/1156986 (accessed 15 March 2025).
Sihombing, B. et al. Response to antimicrobial resistance in South-East Asia Region. Lancet Reg. Health Southeast Asia 18, 100306 (2023).
Sabbatucci, M. et al. Tracking progress on antimicrobial resistance by the quadripartite country self-assessment survey (TrACSS) in G7 countries, 2017–2023: opportunities and gaps. Pharmacol. Res. 204, 107188 (2024).
Chua, A. Q., Verma, M., Hsu, L. Y. & Legido-Quigley, H. An analysis of national action plans on antimicrobial resistance in Southeast Asia using a governance framework approach. Lancet Reg. Health West. Pac. 7, 100084 (2021).
Patel, J. et al. Measuring the global response to antimicrobial resistance, 2020–21: a systematic governance analysis of 114 countries. Lancet Infect. Dis. 23, 706–718 (2023).
Patel, J. et al. Global policy responses to antimicrobial resistance, 2021-22: a systematic governance analysis of 161 countries and territories. Lancet Infect. Dis. 26, 55–66 (2025).
Zhang, X.-X. et al. Towards a global One Health index: a potential assessment tool for One Health performance. Infect. Dis. Poverty 11, 57 (2022).
Zhou, N. et al. Global antimicrobial resistance: a system-wide comprehensive investigation using the Global One Health Index. Infect. Dis. Poverty 11, 92 (2022).
WHO. Comprehensive Review of the WHO Global Action Plan on Antimicrobial Resistance - Volume 1: Report (2021).
Sullivan, C. et al. Combating Antimicrobial Resistance during the COVID-19 Pandemic: Perceived Risks and Protective Practices (Office of the Assistant Secretary for Planning and Evaluation, 2025).
Knight, G. M. et al. Antimicrobial resistance and COVID-19: intersections and implications. eLife 10, e64139 (2021).
NORM/NORM-VET 2020. Usage of Antimicrobial Agents and Occurrence of Antimicrobial Resistance in Norway (Norwegian Institute of Public Health & Norwegian Veterinary Institute, 2021).
Munkholm, L. & Rubin, O. The global governance of antimicrobial resistance: a cross-country study of alignment between the global action plan and national action plans. Glob. Health 16, 109 (2020).
WHO. Situational Analysis of Antimicrobial Resistance in the South-East Asia Region, 2018: an Update on Two Years Implementation of National Action Plans (2019).
Andersson, D. I. & Hughes, D. Antibiotic resistance and its cost: is it possible to reverse resistance?. Nat. Rev. Microbiol. 8, 260–271 (2010).
Mathew, P., Sivaraman, S. & Chandy, S. Communication strategies for improving public awareness on appropriate antibiotic use: bridging a vital gap for action on antibiotic resistance. J. Family Med. Prim. Care 8, 1867–1871 (2019).
Charani, E. et al. An analysis of existing national action plans for antimicrobial resistance—gaps and opportunities in strategies optimising antibiotic use in human populations. Lancet Glob. Health 11, e466–e474 (2023).
Yang, D. et al. Antimicrobial resistance in China across human, animal, and environment sectors—a review of policy documents using a governance framework. Lancet Reg. Health West. Pac. 48, 101111 (2024).
European Commission. Communication from the Commission on a Community Strategy Against Antimicrobial Resistance (2001); https://health.ec.europa.eu/publications/communication-commission-com2001-333-final_en
Request for Proposals: Senegal AMR Surveillance Programme. The Fleming Fund https://www.flemingfund.org/wp-content/uploads/fa734d33fbce6e0a853afa4ee0c912aa.pdf (accessed 12 November 2025).
Eighth Annual Report on Antimicrobial Agents Intended for Use in Animals (WOAH, 2024).
Ruiz, J. et al. Antimicrobial stewardship programme in critical care medicine: a prospective interventional study. Med. Intensiva 42, 266–273 (2018).
FAO. Reduce the Need for Antimicrobials for Sustainable Agrifood System Transformation (RENOFARM) (2024); https://doi.org/10.4060/cd1715en
Department of Health and Social Care. UK 20-Year Vision for Antimicrobial Resistance (2019). https://www.gov.uk/government/publications/uk-20-year-vision-for-antimicrobial-resistance
Larsson, D. G. J. & Flach, C.-F. Antibiotic resistance in the environment. Nat. Rev. Microbiol. 20, 257–269 (2022).
Bavel et al. Intersections between climate change and antimicrobial resistance: a systematic scoping review. Lancet Planet. Health 8, e1118–e1128 (2024).
Li, W. et al. Changing climate and socioeconomic factors contribute to global antimicrobial resistance. Nat. Med. 31, 1798–1808 (2025).
Li, W. et al. Estimating the effect of increasing ambient temperature on antimicrobial resistance in China: a nationwide ecological study with the difference-in-differences approach. Sci. Total Environ. 882, 163518 (2023).
Li, W. et al. Association between antibiotic resistance and increasing ambient temperature in China: an ecological study with nationwide panel data. Lancet Reg. Health West. Pac. 30, 100628 (2023).
UNEP. Bracing for Superbugs: Strengthening Environmental Action in the One Health Response to Antimicrobial Resistance (2023).
Woolhouse, M. E. J. One Health approaches to tackling antimicrobial resistance. Sci. One Health 3, 100082 (2024).
Hammerum, A. M. et al. Danish integrated antimicrobial resistance monitoring and research program. Emerg. Infect. Dis. 13, 1632–1639 (2007).
Bager, F. DANMAP: monitoring antimicrobial resistance in Denmark. Int. J. Antimicrob. Agents 14, 271–274 (2000).
Baker, K. S. et al. Evidence review and recommendations for the implementation of genomics for antimicrobial resistance surveillance: reports from an international expert group. Lancet Microbe 4, e1035–e1039 (2023).
Liu, J. et al. One Health for all: synergistic solutions advancing SDG3 through sustainable science and inclusive innovation. Sci. One Health 4, 100130 (2025).
Farzana, R. et al. The impact of the COVID-19 pandemic on antimicrobial usage: an international patient-level cohort study. JAC Antimicrob. Resist. 7, dlaf037 (2025).
Rozman, U. et al. Impact of the COVID-19 pandemic on the consumption of antibiotics and the emergence of AMR: case study in a general hospital. Front. Public Health https://doi.org/10.3389/fpubh.2025.1584574 (2025).
Sati, H. et al. The WHO Bacterial Priority Pathogens List 2024: a prioritisation study to guide research, development, and public health strategies against antimicrobial resistance. Lancet Infect. Dis. 25, 1033–1043 (2025).
Higgins, J. P. T. et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (Cochrane, 2023).
Browne, A. J. et al. Global antibiotic consumption and usage in humans. 2000–18: a spatial modelling study. Lancet Planet. Health 5, e893–e904 (2021).
Mulchandani, R., Wang, Y., Gilbert, M. & Boeckel, T. P. V. Global trends in antimicrobial use in food-producing animals: 2020 to 2030. PLoS Glob. Public Health 3, e0001305 (2023).
Institute For Health Metrics And Evaluation. Global Burden of Disease Study 2021 (GBD 2021) Socio-Demographic Index (SDI) 1950–2021 (2024).
Van Boeckel, T. P. et al. Global trends in antimicrobial use in food animals. Proc. Natl Acad. Sci. USA 112, 5649–5654 (2015).
Gilbert, W., Thomas, L. F., Coyne, L. & Rushton, J. Review: Mitigating the risks posed by intensification in livestock production: the examples of antimicrobial resistance and zoonoses. Animal 15, 100123 (2021).
van Berkum, S. How urban growth in the global south affects agricultural dynamics and food systems outcomes in rural areas: a review and research agenda. Sustainability 15, 2591 (2023).
Anderson, M., Schulze, K., Cassini, A., Plachouras, D. & Mossialos, E. A governance framework for development and assessment of national action plans on antimicrobial resistance. Lancet Infect. Dis. 19, e371–e384 (2019).
Hasson, F., Keeney, S. & McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 32, 1008–1015 (2000).
Lu, Y., Liu, C., Yu, D. & Wells, Y. Conditions required to ensure successful detection and management of mild cognitive impairment in primary care: a Delphi consultation study in China. Front. Public Health https://doi.org/10.3389/fpubh.2022.943964 (2022).
Von Der Gracht, H. A. Consensus measurement in Delphi studies. Technol. Forecast. Soc. Change 79, 1525–1536 (2012).
Liu, W., Hu, M. & Chen, W. Identifying the service capability of long-term care facilities in China: an e-Delphi study. Front. Public Health https://doi.org/10.3389/fpubh.2022.884514 (2022).
Yingming, W. Using the method of maximizing deviation to make decision for multiindices. J. Syst. Eng. Electron. 8, 21–26 (1997).
Wang, X. & Zhang, L. A combined weighting model based on maximizing deviation for multiple attribute decision-making. Adv. Mater. Sci. Eng. 2022, 7679851 (2022).
Al-Aomar, R. A combined AHP-entropy method for deriving subjective and objective criteria weights. Int. J. Ind. Eng. Theory Appl. Pract. https://doi.org/10.23055/ijietap.2010.17.1.330 (2010).
Saaty, R. W. The analytic hierarchy process—what it is and how it is used. Math. Model. 9, 161–176 (1987).
Shannon, C. E. A mathematical theory of communication. Bell Syst. Tech. J. 27, 379–423 (1948).
Vidal, L.-A., Marle, F. & Bocquet, J.-C. Using a Delphi process and the analytic hierarchy process (AHP) to evaluate the complexity of projects. Expert Syst. Appl. 38, 5388–5405 (2011).
Moslem, S., Alkharabsheh, A., Ismael, K. & Duleba, S. An integrated decision support model for evaluating public transport quality. Appl. Sci. 10, 4158 (2020).
Ishizaka, A. & Labib, A. Review of the main developments in the analytic hierarchy process. Expert Syst. Appl. 38, 14336–14345 (2011).
Pant, S., Kumar, A., Ram, M., Klochkov, Y. & Sharma, H. K. Consistency indices in analytic hierarchy process: a review. Mathematics 10, 1206 (2022).
Chen, P. Effects of the entropy weight on TOPSIS. Expert Syst. Appl. 168, 114186 (2021).
Wu, Z. & Chen, Y. The maximizing deviation method for group multiple attribute decision making under linguistic environment. Fuzzy Sets Syst. 158, 1608–1617 (2007).
Hongjiu, L. & Yanrong, H. An evaluating method with combined assigning-weight based on maximizing variance. Sci. Program. 2015, 290379 (2015).
Lim, S. S. et al. Measuring the health-related Sustainable Development Goals in 188 countries: a baseline analysis from the Global Burden of Disease Study 2015. Lancet 388, 1813–1850 (2016).
Goodman-Bacon, A. Difference-in-differences with variation in treatment timing. J. Econom. 225, 254–277 (2021).
Gardner, J. Two-stage differences in differences. Preprint at https://doi.org/10.48550/arXiv.2207.05943 (2022).
Cengiz, D., Dube, A., Lindner, A. & Zipperer, B. The effect of minimum wages on low-wage jobs. Q. J. Econ. 134, 1405–1454 (2019).
Lennon, H. et al. Framework to construct and interpret latent class trajectory modelling. BMJ Open 8, e020683 (2018).
Sinha, P., Calfee, C. S. & Delucchi, K. L. Practitioner’s guide to latent class analysis: methodological considerations and common pitfalls. Crit. Care Med. 49, e63–e79 (2021).
Acknowledgements
This work was supported by the National Key Research and Development Program of China (grant no. 2024YFE0199000 to Y. Zhu). We are grateful to all experts who participated in the Delphi consultation for their constructive input and feedback. We also thank our affiliated organizations for their continued support and guidance throughout this study. The funder had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
W.C., Y. Zeng, J.W., X.G., J.U., J.S. and Y. Zhu conceived the study. W.C., Y. Zeng, J.Zh., J.W., M.L., Z.C., J.Q. and X. Zhou contributed to index development. E.K., C.L., Y.Che., G.Y., N.Z., C.Z., H.M.T., M.M.G., T.R., Z.Z., Y.X., H.C., C.S. and S.C. reviewed the index and provided structural feedback. W.C., Y. Zeng, Z.C., J.Q. and M.L. collected, curated and reviewed national policy documents. Data coding, translation and validation were led by W.C., Y. Zeng, J.Zh., J.W., M.L., Z.C. and J.Q. Statistical analyses and modeling were performed by W.C., Y. Zeng, J.Zh., W.G. and X.T. J.U., R.B., J.R.F., S.C., Y.Cha., X. Zhang and J.S. provided critical methodological input and international expert perspectives. Y.X., H.C., C.S., C.Z., H.M.T., M.M.G. and T.R. provided clinical, veterinary, agricultural or environmental expertise. W.C., Y. Zeng, J.Zh., J.W. and W.G. drafted the initial manuscript. All authors reviewed, edited and approved the final version of the manuscript. All authors had access to the data, approved the analyses and accept responsibility for the integrity and accuracy of the work.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks Anne Harant, Chaelin Kim and Lianping Yang for their contribution to the peer review of this work. Primary Handling Editor: Ming Yang, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Global distribution of AMR governance scores, 2017–2022.
World maps showing country-level AMR governance scores in (A)2017, (B)2018, (C)2019, (D)2020, (E)2021, (F)2022. Abbreviations: AMR=antimicrobial resistance. Base map generated using the Standard Map Service platform provided by the Ministry of Natural Resources of China (http://bzdt.ch.mnr.gov.cn/).
Extended Data Fig. 2 Distributions of AMR governance scores by domain/subdomain and WHO region in 2022.
Box plots summarize governance scores in 2022 for each governance domain (policy design, implementation, monitoring) and subdomain, stratified by WHO region. (A) Overall distributions of governance domain scores. P values shown in (A) are from two-sided Wilcoxon signed-rank test comparing domain scores. (B) Distributions of policy design subdomain scores (I1.1–I1.4) by WHO region. (C) Distributions of implementation subdomain scores (I2.1–I2.7) by WHO region. (D) Distributions of monitoring subdomain scores (I3.1–I3.3) by WHO region. Centre line indicates the median; box bounds indicate the 25th and 75th percentiles. I 1.1–I 3.3 represent the following indicators: I1.1 strategic vision; I1.2 multi-sector engagement; I1.3 sustainability; I1.4 accountability; I2.1 antimicrobial use surveillance system; I2.2 antimicrobial resistance surveillance system; I2.3 optimization of antimicrobial use; I2.4 professional education; I2.5 public awareness; I2.6 hygiene and prevention; I2.7 research and innovation; I3.1 reporting; I3.2 policy adjustment; and I3.3 effectiveness. Abbreviations: AMR=antimicrobial resistance. WHO=World Health Organization.
Extended Data Fig. 3 AMR Governance scores by sector in 2022.
Box plots compare AMR governance scores for indicators related to the human, animal, and environmental sectors in 2022. Centre line indicates the median; box bounds indicate the 25th and 75th percentiles. Group comparisons were assessed using two-sided Wilcoxon signed-rank test. Abbreviations: AMR=antimicrobial resistance.
Extended Data Fig. 4 Regional linear trends in AMR governance domains, 2017–2022.
For each WHO region, lines show estimated linear trends in governance domain scores over 2017–2022. Points indicate annual global mean scores. Lines show ordinary least-squares linear regression fits over time, with shaded bands indicating 95% confidence intervals for lines. Statistical significance of temporal trends was assessed using two-sided tests of the regression slope. Abbreviations: AMR=antimicrobial resistance. WHO=World Health Organization.
Extended Data Fig. 5 Heatmaps of AMR governance subdomain scores by WHO region, 2017–2022.
Heatmaps display annual mean scores for each AMR governance subdomain (rows) across 2017–2022 (columns) within each WHO region. Abbreviations: AMR=antimicrobial resistance. AMU=antimicrobial use. WHO=World Health Organization.
Extended Data Fig. 6 Comparison of AMR governance profiles between Eastern European and Central Asian countries and other WHO European countries.
(A) Radar plot comparing governance subdomain scores between Eastern European and Central Asian countries and other WHO European countries in 2022. (B) Time trends (2017–2022) for each governance subdomain in the two groups. (C) Time trends for AMR governance score, AMU score, and AMR prevalence score in the two groups. Abbreviations: AMR=antimicrobial resistance. AMU=antimicrobial use. WHO=World Health Organization.
Extended Data Fig. 7 Event-study estimates of NAP adoption on sector-specific AMU outcomes.
(A) Human AMU score. (B) Animal AMU score. (C) Agricultural crop production AMU score. The analytical sample includes n = 172 countries. For each country, the year of NAP adoption is defined as event time zero (t = 0); negative values indicate years before adoption, positive values indicate years after adoption, and t = −1 serves as the reference year. Control countries were those that had not yet adopted or had never adopted NAPs, whereas countries contributed to the treatment group from the year of NAP adoption onwards. Points represent estimated treatment effects for each year relative to the reference year (t = −1), with error bars indicating 95% confidence intervals. Three models are shown: the two-stage DID, the stacked event-study DID, and TWFE OLS. Abbreviations: AMU=antimicrobial use. DID=difference-in-differences. NAP=national action plan. OLS=ordinary least squares. TWFE=two-way fixed effects.
Extended Data Fig. 8 Construction of the AMR governance framework and policy document collection workflow.
(A)Development process of the AMR governance framework (B)Flowchart of AMR policy documents collection process Abbreviations: AMR=antimicrobial resistance. FAO=Food and Agriculture Organization of the United Nations. NAP=national action plan. OIE=Office International des Epizooties. UNEP=United Nations Environment Programme. WHO=World Health Organization. WOAH=World Organisation for Animal Health.
Extended Data Fig. 9 Trajectory groups of AMR prevalence score change, 2015–2021.
Three group-based trajectories of ΔAMR over time, with countries classified into high-growth, moderate-growth, and negative-growth groups using a latent class growth model. ΔAMR is defined as the observed AMR prevalence score (2015–2021) minus a counterfactual predicted from a linear trend fitted over 2000–2014. Thin lines indicate individual country trajectories, thick lines indicate the group mean trajectory. Shaded bands represent mean ± 1 standard deviation at each year. Abbreviations: AMR=antimicrobial resistance.
Supplementary information
Supplementary Information (download PDF )
Supplementary Tables 1–26 and Supplementary Figs. 1–12.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, W., Zeng, Y., Zheng, J. et al. Evaluation of antimicrobial resistance governance across 193 countries to inform the 2026 Global Action Plan update. Nat Med 32, 1362–1373 (2026). https://doi.org/10.1038/s41591-026-04257-1
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41591-026-04257-1
