
Abstract
The objective of this study is to describe the properties of dosing weight in the neonatal intensive care unit (NICU). Infants were identified from a database of very low birth weight infants. Before regaining birth weight (BW), dosing and birth weight% difference was described. After regaining BW, dosing and measured weight% difference and frequency of dosing weight updates were described. Associations with infant characteristics including comorbid conditions, serum biochemistries, fluid intake, and urine output were evaluated. There were 115 infants over 4,643 infant-days with a median BW of 1060 g (interquartile range [IQR]: 750, 1300) and median time to regain BW of 10 days (IQR: 8, 13). After regaining BW, dosing weight was 4.2% less than measured weight. The gap widened with increasing creatinine and narrowed with increasing urine output. The only factor associated with the frequency of dosing weight updates was day of the week. Dosing weights in the NICU appear to fall into one of three categories: BW prior to regaining BW, practical weight to facilitate medication and nutrition ordering, and “dry” weight, adjusting for fluid overloaded states. We recommend using measured weight to avoid a 4% daily loss in nutrition intake once BW is regained.
Similar content being viewed by others


Introduction
Dosing weight (DW) is an assigned weight that differs from the most recent measured weight (MW), which is typically obtained daily. In the neonatal intensive care unit (NICU), the DW facilitates medication and nutrition ordering by accounting for changes in fluid status, rapid growth, or measurement error1,2. Clinicians may also continue to use the birth weight (BW) as opposed to the MW for variable periods of time3,4, as there are considerable shifts in fluid between intracellular and extracellular compartments after birth5.
The chosen DW has important implications for nutrition management, fluid management, and medication dosing for infants in the NICU. Basing nutrition calculations on BW rather than MW until BW is regained has been associated with higher protein delivery and increased weight and head circumference percentiles at discharge4. DW may also represent a “dry” weight that reflects an assessment of fluid overload or state of edema secondary to acute kidney injury6. Determining the degree of fluid overload is important and has been previously shown to have significant implications in morbidity and mortality, as well as potential need for therapeutic interventions6,7,8.
Assigning an appropriate DW for infants can be challenging for clinicians. There is minimal guidance on how to do so because the factors associated with DW assignment have not been fully explored. As a result, variation in the use of DW exists. A survey of NICUs in the Children’s Hospital Neonatal Consortium demonstrated that 40% of electronic health records used the DW to automatically calculate fluid intake in mL/kg while 60% used the MW9. We aim to describe the DW of infants in the NICU, including how it compares to BW and MW, and whether the frequency and magnitude of DW changes are associated with infant characteristics or nonclinical factors.
Methods
The Institutional Review Board (IRB) of the Ann & Robert H. Lurie Children’s Hospital reviewed the study and determined that it is exempt from IRB review (IRB #2015 − 522). The IRB committee waived the requirement for informed consent due to the retrospective nature of this study. All methods were performed in accordance with the relevant guidelines and regulations. The original dataset was created from three sources (manually abstracted data from Epic electronic health record, data from the Children’s Hospital Neonatal Consortium (CHNC) Database, and data obtained through Lurie Children’s Hospital Data Analytics and Reporting (DAR)) between the spring of 2015 and the fall of 2016. Additional data was obtained through all three sources (Epic, CHNC, DAR) in the spring and summer of 2021. Final analysis for the paper was performed on July 26, 2022 and August 1, 2022. The senior author (GF) had access to information that could identify individual participants during data collection from the electronic health record.
Setting
The Lurie Children’s Hospital NICU is a 64-bed regional, referral level IV NICU in Chicago, IL that cares for critically ill preterm and term infants10. A multidisciplinary team including neonatologists, neonatal fellows, nurse practitioners, pediatric residents, bedside nurses, pharmacists, and dietitians reviews each patient during morning rounds at bedside. Discussions include but are not limited to intake, output, and growth. It is common practice to continue to use BW as the DW for the first two weeks of life or until BW is regained. After BW is regained, the team will review the DW with some regularity and modify the DW as the MW changes with infant growth. Unlike the MW or BW, which are measured values, the DW is an assigned value. Clinicians typically initiate parenteral nutrition at 80–100 mL/kg per day for preterm infants shortly after birth. Subsequently, they advance volume by 20mL/kg per day and introduce enteral feeds according to infant’s clinical status until achieving a goal of 150-160mL/kg of full enteral feeds. After birth, infants remain in a humidified incubator until the infant can maintain euthermia without assistance.
Cohort and data abstraction
The cohort included infants from an existing nutrition and growth dataset of very low birth weight (< 1500 g) infants admitted to the NICU in the first week of life11,12. Infants with congenital anomalies, chromosomal abnormalities, or discharge prior to 28 days of life were excluded.
The dataset included data on infant characteristics, non-clinical factors, growth parameters, and fluid and nutrition intake during the first six weeks of life. Infant characteristics included gestational age, BW, small for gestational age (SGA), patent ductus arteriosus (PDA), necrotizing enterocolitis or spontaneous intestinal perforation (NEC/SIP), intubation on day 28, and blood stream infection (BSI). Non-clinical factors included whether the infant was managed by neonatal nurse practitioners or resident physicians and the day of the week, which is associated with changes in clinical care13. Growth parameters included daily MW, length, and head circumference. Daily fluid and nutrition intake were normalized using daily MW.
Additional data were obtained through the Children’s Hospital Neonatal Consortium database and Data, Analytics, and Reporting of Lurie Children’s Hospital14. These data included all DWs and the day of DW changes, the lowest serum sodium and highest creatinine values, daily urine output reported in mL/kg/hour using MW, and medications that may affect urine output (caffeine, indomethacin or ibuprofen, and maternal antenatal steroids).
Exploratory analyses
To facilitate interpretation of statistical analyses, these variables were centered to the following values: highest creatinine, 1 mg/dL (hospital reference range: 0.25-0.54 mg/dL); lowest sodium, 130 mEq/L (range: 136-149mEq/L); daily fluid intake, 140 mL/kg/day; hourly urine output, 2 mL/kg/hour. Statistical analyses with fluid intake were performed in 10 mL/kg/day units.
The DW-BW and DW-MW percent differences were calculated using the following formula:
The 5th, 25th, 50th, 75th, 95th percentiles for DW-BW and DW-MW differences were graphed daily for the first six weeks of life. Based on the unit practice to use the BW as the DW until BW was regained, subsequent analyses evaluated the DW-BW difference before the infant regained BW and the DW-MW difference on or after the infant regained BW. The time to regain BW was defined as the first of three consecutive days with the MW at or above BW following diuresis.
Analyses of dosing weight before infant regained birth weight
The median number of DW changes was calculated for each infant. Since most infants had only one DW assigned during this period, the average DW-BW difference was described using a histogram and evaluated for associations with infant characteristics and non-clinical factors. Analyses were limited to the highest creatinine, lowest sodium, and average fluid intake and urine output in the first week. Wilcoxon rank sum test and ordinary least square regression were used when appropriate. All statistical significance assumed a two-tailed test with an α of 0.05.
Analyses of dosing weight on or after infant regained birth weight
After the infant regained BW, we evaluated the DW-MW difference. Bivariable analyses determined the association between the daily DW-MW difference with each infant characteristic and non-clinical factor using mixed effects linear regression given data clustering (i.e., repeated measurements per infant)15. Analyses included the highest creatinine and lowest sodium over the entire six weeks. Because DW was typically assigned in the morning during rounds before the total intake and output were determined for each day, 3-day moving averages (3DMA) of daily fluid intake and urine output were calculated to reflect the most recent fluid status of the infant and used in the analyses (e.g., the association between the DW-MW difference and fluid intake on day 21 corresponded to the 3DMA of fluid intake on days 18–20)11,16. Multivariable analyses employed models using backward stepwise reduction with a criterion of p-value less than 0.20. Beta coefficients, along with 95th percent confidence intervals [CI] and p-values were reported.
The DW-MW difference over time is logically the result of the frequency of DW changes and the magnitude of DW assignment on the day of change as the MW increases with infant growth. For example, a large DW-MW difference may accrue because of infrequent DW changes, a large magnitude in the DW-MW difference on the day the DW changes, or both. To distinguish between both effects, we subsequently evaluated the frequency and magnitude of DW-MW difference only on days when DW was changed. Bivariable analyses determined the association with each infant characteristics and non-clinical factors using mixed effects logistic and linear regression when appropriate, followed by multivariable analyses15.
Results
Cohort
The cohort included 115 very low birth weight infants over a total of 4,643 infant-days with DW and MW recorded on 100% and 97.5% infant-days, respectively. Median day of admission was 0 (interquartile range [IQR]: 0, 1) and median day of discharge was 87 (IQR: 55, 128). Median birth weight was 1060 g (IQR: 750, 1300) and median gestational age was 28 and 0/7 weeks (IQR: 25 and 4/7, 30 and 1/7). SGA was present in 13 (11%), NEC/SIP in 21 (18%), day 28 intubation in 40 (35%), and BSI in 19 (17%) infants. PDA was present in 55 (48%) infants – 17 (15%) were untreated, 28 (24%) were only treated medically and 10 (9%) were treated surgically. Mothers of 80 (70%) infants received any steroids; 46 (40%) infants received indomethacin or ibuprofen as treatment or prophylaxis, and 67 (72%) infants received caffeine. Nurse practitioners cared for 46 (40%) infants, while resident physicians cared for 69 (60%) infants.
The median highest creatinine level was 0.92 mg/dL (IQR: 0.81, 1.05) and lowest sodium level was 130 mEq/L (IQR: 126, 134) over the six weeks. Of the 115 infants, 88 (77%) had hyponatremia with a sodium < 135 mEq/L, 55 (48%) had a sodium < 130 mEq/L, and 4 (3%) had a sodium < 120 mEq/L.(17,18) Values limited to the first week of life were similar for creatinine (median: 0.88; IQR: 0.79, 0.99) though less hyponatremic (median: 135; IQR: 132, 137). The median fluid intake was 145 mL/kg/day (IQR: 133, 154); however, intake rapidly increased over the first week before plateauing to just under 150 mL/kg/day (Fig. 1). The median urine output was 2.2 mL/kg/hour (IQR: 1.6, 3.9) and appeared stable over the six weeks (Fig. 2).

Daily fluid intake in mL/kg/day over the first six weeks.

Daily urine output in mL/kg/hour over the first six weeks.
Exploratory analyses
The median time to regain BW in our cohort was 10 days (IQR: 8, 13). There were four infants who never diuresed, and two infants who regained BW prior to admission. Time to regain BW was set to day 1 for the former and day of admission for the latter.
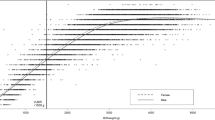
Visual analysis of the DW-BW and DW-MW differences demonstrated that DW tracked BW in the early postnatal period before tracking MW (Figs. 3, 4). In both graphs, there is an inflection point at day 10, the median time to regain BW. The median DW-BW difference prior to day 10 is zero before increasing. The median DW-MW difference stabilizes around − 3 to -4% after day 10. This appeared consistent with the unit practice of using the BW as the DW until BW is regained.

Dosing & birth weights percent difference.

Dosing & measured weights percent difference.
Analyses of dosing weight before infant regained birth weight
About 90% of infants had only one DW assigned (i.e., the initial DW) prior to regaining BW (median 1; IQR: 1, 1). The distribution of the average DW-BW difference is presented in Fig. 5. Though the median DW-BW difference was zero, the difference ranged − 8.2 to 13.5%. This difference was not associated with any infant characteristics or non-clinical factor (Table 1).

Distribution of average dosing-birth weights percent difference.
Analyses of Dosing Weight on or after infant regained Birth Weight
The DW-MW difference on or after the infant regained BW is similar to Fig. 4 after day 10, the median time to regain birth weight (data not shown). Bivariable analyses demonstrated independent associations between DW-MW and BW, intubation, highest creatinine, and 3DMA of daily fluid intake and hourly urine output (Table 2); however, only highest creatinine and the 3DMA of urine output remained significantly associated with DW-MW percent difference in the multivariable model (Table 3). The referent DW-MW percent difference (i.e., intercept) in an infant whose peak creatinine was 1 mg/dL with urine output of 2 mL/kg/hour was − 4.2%. This difference would change by -5.4% for every 1 mg/dL increase in peak creatinine and 0.8% for every 1 mL/kg/hour increase in the 3DMA of urine output. Therefore, an infant with peak creatinine of 2.0 mg/dL and a urine output of 1 mL/kg/hour in the past three days would have an average DW-MW percent difference of -10.4% ([-4.2] + [-5.4] + [0.8*-1]).
The median number of DW changes after the infant regained BW was 6 (IQR: 5, 7). Figure 6 describes the frequency of changes and median DW-MW percent difference by day of the week. DW changes for all 115 infants most frequently occurred on Monday and Friday. As a result, the DW-MW difference narrowed on these days but gradually widened during the remaining days. Bivariable analyses only demonstrated an independent association with day of week (Table 4). Infant characteristics including comorbid conditions and renal function were not associated with a DW change. Multivariable logistic regression demonstrated that the odds of a DW change was increased on Mondays and Fridays (odds ratio [OR]: 8.5; CI: 6.9, 10.5; p < 0.001) and decreased on Saturdays and Sundays (OR: 0.7; CI: 0.5, 0.9; p = 0.01) referent to Tuesday, Wednesday, and Thursday.

Dosing weight changes & dosing-measured weights difference by day of the week.
Limited to days with DW changes, bivariable analyses demonstrated an independent association between DW-MW and BW, NEC/IP, intubation, highest creatinine, lowest sodium, indomethacin or ibuprofen, and day of the week (Table 5); however, only highest creatinine and the 3DMA of fluid intake remained significantly associated with DW-MW difference on days that DW were changed (Table 6). The referent DW-MW percent difference in an infant whose peak creatinine was 1 mg/dL and fluid intake over the past three days was 140 mL/kg/day was − 1.3%. This difference would change by -3.5% for every 1 mg/dL increase in peak creatinine and 0.4% for every 10 mL/kg/day increase in the 3DMA of fluid intake. Therefore, on days that DW was changed an infant with peak creatinine of 0.9 mg/dL and a total fluid intake of 160 mL/kg/day over the past three days would have an average assigned DW-MW difference of -0.2% ([-1.3] + [-3.5*-0.1] + [0.4*2]).
Discussion
Prior to regaining BW, the median DW-BW difference is zero and consistent with our practice of setting the DW to BW; however, there is significant variation without apparent rationale. After the infant has regained BW, the DW changes regularly. The frequency of changes is consistent with our unit’s practice of updating DWs on Mondays and Fridays but independent of any infant characteristic. These periodic changes to the DW made during bedside rounds at the clinicians’ discretion are practical adjustments. They facilitate medication and nutrition ordering by avoiding the need to update dosages each day due to small changes in the MW. The decrease in DW adjustments during the weekend may be secondary to decreased pharmacy coverage on the weekend or inconsistent physician coverage (neonatologists and neonatal fellows worked only one weekend of a three and four-week rotation, respectively).
On days that the DW is assigned, the DW-MW difference is inversely associated with peak creatinine and directly associated with recent fluid intake. Though we cannot determine the intent of clinicians, we suspect that clinicians may be accounting for states of fluid overload and edema associated with renal dysfunction by assigning a “dry” weight. In such edematous infants the DW-MW difference is more negative and widened. We would expect clinicians to manage renal dysfunction (i.e., increased creatinine) with fluid restriction (i.e., decreased fluid), and this is what we see. On days that DW is not updated, the DW-MW difference becomes more negative and widens as MW increases (i.e., infant growth) until the DW is updated again. This difference similarly varies inversely with peak creatinine and directly with urine output. Infants who void appropriately will have a DW-MW difference that is more positive and narrowed as the DW more closely approximates MW.
Therefore, our analysis demonstrates that the DW falls into three broad categories: a BW prior to the infant regaining BW, a practical weight used to facilitate medication and nutrition ordering, and a “dry” weight that adjusts for infants with suspected renal dysfunction and fluid overload. This is not surprising. What is surprising is how little evidence guides the use of DW, including how frequently to update DW, how to appropriately assign a DW for critically ill infants, and whether to use a DW or MW for nutrition orders. A search on PubMed for “(‘dosing weight’) AND (neonatal OR infant)” in August, 2024 yields thirteen publications19. This area requires further research, especially since the DW is used to identify fluid overload, which is associated with morbidity and mortality in critically ill infants20. A clinical decision support system may be able to assist clinicians in assigning a dosing wight and determining a dosing weight since they have already been used to estimate the discharge weight in preterm infants21.
For infants without evidence of renal dysfunction, we recommend that clinicians utilize the MW rather than DW in fluid and nutrition calculations. The average DW-MW difference was − 4%. Clinicians using the DW to calculate fluid and nutrition orders may deliver 4% less calories and 4% less nutrients than if they had used the MW. Though 4% seems small, cumulatively, this will contribute to the nutrient deficit that often accrues in preterm infants22. Early optimization of nutrition delivery is associated with improved outcomes such as improved postnatal growth measurements and higher intellectual functioning in childhood23,24,25.
Another notable finding was that there was a significant rate of hyponatremia, which has been described previously in preterm infants26. At least three-quarters of our infants had hyponatremia with a sodium less than 135 mEq/L and around half had a sodium less than 130 mEq/L; sodium values appeared lower after the first week. Sodium delivery is justifiably kept lower in the early postnatal period to facilitate contraction of the extracellular fluid compartment. After the infant has diuresed in the later postnatal period, these data suggest that further attention to fluid and sodium management is warranted.
As a retrospective review, this study has several limitations. First, we were unable to evaluate all the factors that influence DW assignment. We can only speculate how clinicians decided to assign DW. It is likely that DW assignment is associated with clinician experience, which may affect the objective and subjective assessments of renal injury and fluid overload27, and nursing and parental input of edema. Additional factors not evaluated, such as the dosing and duration of medications (including caffeine, inotropes, vasopressors, diuretics or nephrotoxic antibiotics), and the use of phototherapy and humidified incubators28, may also affect DW assignment. Further prospective studies, including direct observation of clinical rounds, are needed to more accurately determine how clinicians assess the multitude of factors and assign the DW during rounds. A second limitation is that we only evaluated DW in preterm infants. The results may not be generalizable to critically ill term infants undergoing surgery for congenital anomalies, therapeutic hypothermia for hypoxic ischemic encephalopathy or those infants receiving extracorporeal membrane oxygenation, where the increased volume of distribution can affect the pharmacokinetics of hydrophilic medications29.
Clinicians use the DW every day in every NICU for every patient. Such a ubiquitous value requires more evidence guiding its use.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Change history
17 September 2025
The original online version of this Article was revised: In the original version of this article the shaded areas of figures 1, 2, 3, 4 and 6 were rendered incorrectly. The original article has been corrected.
References
Bartlett, J. W., Gillon, J., Hale, J., Jimenez-Truque, N. & Banerjee, R. Incidence of acute kidney injury among infants in the neonatal intensive care unit receiving Vancomycin with either piperacillin/tazobactam or cefepime. J. Pediatr. Pharmacol. Ther. 25(6), 521–527 (2020).
O’Neal, B. C., Schneider, P. J., Pedersen, C. A. & Mirtallo, J. M. Compliance with safe practices for preparing parenteral nutrition formulations. Am J Health Syst Pharm. 59(3):264–269. (2002). http://www.ncbi.nlm.nih.gov/pubmed/11862638
Bertoni, C. B., Prusakov, P., Merandi, J. & Bartman, T. Clinical Decision Support to Improve Dosing Weight Use in Infants with Neonatal Abstinence Syndrome. Pediatr Qual Saf. 4(4):e184 (2015). http://www.ncbi.nlm.nih.gov/pubmed/31572886
Alur, P. et al. Postnatal growth restriction is reduced if Birth Weight is used for nutritional calculations in ELBW infants. Int. J. Pediatr. 2018, 1–6 (2018).
Heimler, R. et al. Relationship between nutrition, weight change, and fluid compartments in preterm infants during the first week of life. J Pediatr. [cited 2015 May 11];122(1):110–4. http://www.ncbi.nlm.nih.gov/pubmed/8419597
Askenazi, D. J. et al. Fluid overload and mortality are associated with acute kidney injury in sick near-term/term neonate. Pediatr Nephrol. 2013 Apr [cited 2014 May 5];28(4):661–6. http://www.ncbi.nlm.nih.gov/pubmed/23224224
Selewski, D. T. et al. The impact of fluid balance on outcomes in critically ill near-term/term neonates: a report from the AWAKEN study group. Pediatr. Res. 85(1), 79–85 (2019).
Sutherland, S. M. et al. Fluid overload and mortality in children receiving continuous renal replacement therapy: The prospective pediatric continuous renal replacement therapy registry. Am J Kidney Dis. 55(2), 316–325 (2010). https://doi.org/10.1053/j.ajkd.2009.10.048
Falciglia, G. H. et al. Low prevalence of clinical decision support to calculate caloric and fluid intake for infants in the neonatal intensive care unit. J Perinatol. 40(3):497–503. (2020). https://doi.org/10.1038/s41372-019-0546-z
American Academy of Pediatrics Committee on Fetus And Newborn. Levels of neonatal care. Pediatrics. 30(3):587–597 (2012). http://www.ncbi.nlm.nih.gov/pubmed/22926177
Falciglia, G. H. et al. Association Between the 7-Day Moving Average for Nutrition and Growth in Very Low Birth Weight Infants. JPEN J Parenter Enteral Nutr. 148607117722927. http://journals.sagepub.com/doi/ (2017). https://doi.org/10.1177/0148607117722927
Falciglia, G. H. et al. Energy and Protein Intake During the Transition from Parenteral to Enteral Nutrition in Infants of Very Low Birth Weight. J Pediatr. 202:38–43 (2018). https://linkinghub.elsevier.com/retrieve/pii/S002234761830903X
Falciglia, G. H., Grobman, W. A. & Murthy, K. Variation in labor induction over the days of the week. Am. J. Perinatol. ;32(1). (2015).
Murthy, K. et al. The Children’s Hospitals Neonatal Database: an overview of patient complexity, outcomes and variation in care. J Perinatol. 34(8):582–586 (2014). http://www.ncbi.nlm.nih.gov/pubmed/24603454
Robson, K. & Pevalin, D. What is Multilevel Modelling and why should I use it? In: (ed Steele, M.) Multilevel Modeling in Plain Language. 1st ed. Los Ageles: Sage (2016).
Dallas Federal Reserve. Research & Data, Databasics: Smoothing Data with Moving Averages. 2016 [cited 2016 Dec 12]. http://www.dallasfed.org/research/basics/moving.cfm
Moritz, M. L. & Ayus, J. C. Preventing neurological complications from dysnatremias in children. Pediatr. Nephrol. 20(12), 1687–1700 (2005).
Henry, D. A. In The Clinic: Hyponatremia. Ann Intern Med. 163(3):ITC1-19 (2015). http://www.ncbi.nlm.nih.gov/pubmed/26237763
PubMed.gov Search. [Accessed 2024 August 22]. https://pubmed.ncbi.nlm.nih.gov/?term=%22dosing+weight%22+AND+%28infant+OR+neonatal%29&size=20
Matsushita, F. Y., Krebs, V. L. J. & de Carvalho, W. B. Association between fluid overload and mortality in newborns: a systematic review and meta-analysis. Pediatr Nephrol. 37(5):983–992 (2022). https://doi.org/10.1007/s00467-021-05281-8
Yalçın, N. et al. Development and validation of machine learning-based clinical decision support tool for identifying malnutrition in NICU patients. Sci Rep. 13(1):5227 (2023). https://doi.org/10.1038/s41598-023-32570-z
Embleton, N. E., Pang, N. & Cooke, R. J. Postnatal malnutrition and growth retardation: an inevitable consequence of current recommendations in preterm infants? Pediatrics. [cited 2014 Jul 9];107(2):270–3. http://pediatrics.aappublications.org/cgi/doi/ (2001). https://doi.org/10.1542/peds.107.2.270
Senterre, T. & Rigo, J. Optimizing early nutritional support based on recent recommendations in VLBW infants allows abolishing postnatal growth restriction. Vol. 53, Journal of Pediatric Gastroenterology and Nutrition. 2011 [cited 2015 May 8]. p. 1. http://www.ncbi.nlm.nih.gov/pubmed/21701404
Martin, Camilia, R., Brown, Yolanda, F. & Ehrenkranz, R. A. National pratices and growth velocity in the first month of life in extremely low gestational age newborns. Changes. 29(2), 997–1003 (2012).
Pongcharoen, T. et al. Influence of prenatal and postnatal growth on intellectual functioning in school-aged children. Arch. Pediatr. Adolesc. Med. 166(5), 411–416 (2012).
Hassan, F., Kumar, V. N., Asghar, I., Jha, L. & Choudhury, I. Prevalence and risk factors of dysnatremia in sick newborns admitted in neonatal intensive care unit: a cross-sectional study. Int. J. Contemp. Pediatr. 7 (12), 2369 (2020).
van Asperen, Y., Brand, P. L. P. & Bekhof, J. Reliability of the fluid balance in neonates. Acta Paediatr. 2012 [cited 2014 May 5];101(5):479–83. http://www.ncbi.nlm.nih.gov/pubmed/22220764
Rutter, N. & Hull, D. Water loss from the skin of term and preterm babies. Arch. Dis. Child. 54(11), 858–868 (1979).
Yalçın, N., Sürmelioğlu, N. & Allegaert, K. Population pharmacokinetics in critically ill neonates and infants undergoing extracorporeal membrane oxygenation: a literature review. BMJ Paediatr Open. 6(1) (2022). http://www.ncbi.nlm.nih.gov/pubmed/36437518
Author information
Authors and Affiliations
Contributions
Dr. Falciglia was responsible for data acquisition and analysis. Dr. Montoya was responsible for drafting of the manuscript. All authors contributed to study concept and design, as well as critical revision of the manuscript.
Corresponding author
Ethics declarations
Competing interests
Dr. Gustave Falciglia has received a phase 1 small business technology transfer grant (STTR) with Medical Predictive Science Corporation (MPSC) through the National Institute of Health (NIH) to create a clinical decision support system to optimize nutrition delivery in the neonatal intensive care unit. He does not have a financial relationship with MPSC outside the grant. All remaining authors declare no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Montoya, C.R., Khan, J.Y., Nelson, D. et al. Factors influencing the determination of dosing weight in the neonatal intensive care unit (NICU). Sci Rep 15, 4652 (2025). https://doi.org/10.1038/s41598-024-75424-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-75424-y
