
Abstract
The purpose of this study was to investigate the effects of combining blood flow restriction training (BFRT) with electrical muscle stimulation (EMS) on muscle functions and sports performance in football players with knee osteoarthritis (KOA). This parallel randomized controlled trial was conducted on 64 football players diagnosed with KOA at Chengdu Sport University. Participants were enrolled based on predefined eligibility criteria and randomly allocated to four groups: the control group (CTR, n = 16), BFRT-alone group (BFRT, n = 16), EMS-alone group (EMS, n = 16), and BFRT combined with EMS group (CMB, n = 16). Data were gathered via the 10-meter sprint, 20-meter sprint, countermovement jump (CMJ), and Illinois agility test (IAT) to assess sports performance. Additionally, peak torque (PT) was used to measure muscle strength, the root mean square (RMS) was used to assess muscle activation, and the cross-sectional area (CSA) was used to evaluate muscle volume. The data were statistically analyzed via SPSS software, and a p-value < 0.05 was considered significant. Following the 8-week intervention, the CMB group showed a more pronounced change in the 10-m sprint compared to the CTR group (p < 0.001) and exhibited significant differences in the 20-m sprint (CTR: p < 0.001, BFRT: p = 0.015, EMS: p < 0.001), CMJ (CTR: p < 0.001, BFRT: p = 0.019, EMS: p < 0.001), and IAT (CTR: p < 0.001, BFRT: p = 0.009, EMS: p = 0.018), outperforming the other three groups. To PT, the CMB groups demonstrated significant superiority over the other three groups (CTR: p < 0.001, BFRT: p < 0.001, EMS: p < 0.001), while the BFRT group exhibited a notable difference in PT than the EMS group (p = 0.032). Concerning RMS, the EMS and CMB groups showed significant differences from the CTR (EMS: p < 0.001, CMB: p < 0.001) and BFRT (EMS: p = 0.019, CMB: p < 0.001) groups, whereas the change in the BFRT group was more significant than that in the CTR group (p = 0.007). For CSA, the BFRT and CMB groups presented notable differences from the CTR (BFRT: p = 0.008, CMB: p = 0.002)and EMS (BFRT: p = 0.014, CMB: p = 0.004) groups. In summary, the results suggest that BFRT combined with EMS can increase muscle strength in male football players with KOA through improving muscle volume and neuromuscular recruitment under low-intensity resistance training, thereby increasing explosive power and agility.
Similar content being viewed by others
Introduction
Osteoarthritis (OA) is a common degenerative joint disease that can seriously affect the patient’s quality of life and burden the patient’s family and society1. OA not only causes joint pain, stiffness, deformity, and dysfunction, but also significantly increases the risk of cardiovascular events, deep vein thromboembolism, hip fracture, and all-cause mortality2. Currently, there are over 300 million OA patients worldwide3and the overall prevalence of primary OA in individuals over 40 years old in China is as high as 46.3%4. Knee osteoarthritis (KOA) is a notably common type of OA, and its global incidence has increased significantly in recent years. KOA is defined as a degenerative disease caused by mechanical and biological damage to the homeostasis of articular chondrocytes, the extracellular matrix, and the subchondral bone of the knee joint, with joint pain, stiffness, swelling, and loss of major joint functions as the main symptoms5. Pain serves as the main symptom of KOA, diminishing a patient’s sports performance and muscle functions, as well as indirectly increasing the incidence of cardiovascular events6. The extensive physical activity in young patients surpasses the joints’ capacity for repair and maintenance, subjecting the joints to an unfavorable biomechanical environment and hastening the degeneration of the articular cartilage7. Consequently, unlike the high incidence of late-stage OA in elderly individuals, early-stage OA is common in young individuals with exercise habits8.
Engaging in high-intensity exercise significantly increases the risk of injuries such as knee ligament tears, meniscal injuries, and fractures involving the articular surface, all of which are well-established risk factors for KOA, thereby accelerating joint deterioration and increasing the incidence of KOA9,10. Specifically, athletes engaged in sports that subject the knee joint to substantial biomechanical stress, such as rapid acceleration and sudden deceleration, or those engaged in elite-level competitions over an extended period are more prone to developing KOA11. Football is one of the sports that places the greatest biomechanical pressure on the knee joint12. During football matches, professional players cover distances of up to ten kilometers or more, often accompanied by abrupt acceleration and abrupt stops, which can readily subject the knees to high-intensity pressure13,14. Prolonged high-pressure exercise among football players can lead to secondary knee osteoarthritis, stemming from the intricate interplay of biological, mechanical, and biochemical factors14,15. KOA is presently recognized as an occupational ailment among football players. The anterior cruciate ligament and meniscus are two common injuries in football, both of which play pivotal roles in the onset of KOA because of their association with an increased risk of bone marrow lesions in the knee joint, a precursor to KOA16.
The treatment of KOA can be divided into surgical and non-surgical approaches. Surgical treatments include arthroscopic procedures such as anterior cruciate ligament reconstruction, knee osteotomy, and meniscectomy17. For patients with advanced KOA suffering severe joint damage and pain, artificial joint replacement is generally considered the terminal treatment option18. Pharmacological treatments typically involve the use of acetaminophen, nonsteroidal anti-inflammatory drugs, glucosamine, diacerein, and traditional Chinese medicine. However, long-term use of these medications can lead to side effects such as liver and kidney damage, abdominal distension, and diarrhea19. Non-pharmacological treatments encompass exercise, physical therapy, and health education. Health education helps patients understand the disease process, prognosis, and treatment options for KOA. It also aims to prevent activities that exacerbate KOA symptoms, such as mountain climbing and squatting, while encouraging good lifestyle habits and self-management practices like weight control and regular exercise20. Physical therapies, including transcutaneous electrical nerve stimulation (TENS), pulsed electromagnetic field therapy, ultrasound, and acupuncture, can alleviate symptoms and enhance the function of patients with KOA by reducing knee joint load, improving joint range of motion, and increasing neuromuscular control21,22. The lack of targeted therapeutic rehabilitation training is often a factor leading to the further development of KOA23and exercise therapy has been listed as the preferred treatment for KOA by various guidelines24. Exercise, with its broad applicability and ease of implementation, effectively enhances pain management and joint mobility without adverse reactions25. Muscle weakness is an obvious characteristic of patients with KOA. Strength training is one of the most effective ways to combat muscle weakness, as it can significantly improve the strength of thigh muscles such as the quadriceps and promote the recovery of knee joint function26. The American College of Sports Medicine (ACSM) recommends that resistance training to enhance muscle strength should involve a resistance load of at least 60%-70% of the single-repetition maximum load (1-repetition maximum, 1RM)27. To increase muscle volume, a positive load of 70%-85% of the 1RM is suggested. However, this high load is often challenging to achieve for patients with knee osteoarthritis or those who have undergone early knee surgery. Therefore, exploring more effective rehabilitation strategies for knee joint diseases remains crucial.
Blood flow restriction training (BFRT), also known as KAATSU training, was invented by Yoshiaki Soto. This training involves using a compression cuff to apply pressure to the proximal end of a limb while performing low-load resistance exercises. BFRT has been shown to effectively promote muscle strength growth and muscle hypertrophy28. When combined with low-load resistance training (30% 1RM), BFRT can achieve effects similar to those of high-load resistance training29. The mechanisms of BFRT include increased secretion of anabolic hormones, increased muscle protein synthesis signaling pathways, muscle tissue ischemia, and hypoxia, which lead to cellular hydration and swelling30. While BFRT primarily induces muscle growth through metabolic stress and increased mechanical tension, its impact on neuromuscular function and muscle activation improvement is not significant31. Evidence synthesis indicates a dichotomous effect profile of BFRT on delayed onset muscle soreness (DOMS). During high restrictive pressures (typically ≥ 80% arterial occlusion pressure) combined with eccentric exercises, BFRT exhibits a pro-inflammatory tendency characterized by amplified DOMS symptoms, including heightened pain perception and extended recovery of muscular strength, among other factors. This response is mechanistically linked to augmented mechanical and metabolic stress, potentiating localized inflammation and reactive oxygen species generation. Conversely, post-conditioning BFR demonstrates a protective effect against DOMS. This modality attenuates pain intensity, accelerates recovery of range of motion (ROM), reduces creatine kinase (CK) elevation, and mitigates muscle strength decline, likely via modulation of reperfusion-mediated edema resolution and nociceptor desensitization32. Nonetheless, substantial research indicates that BFRT has the potential to improve strength and performance when incorporated into a resistance training regimen in healthy athletes33. Electrical muscle stimulation (EMS) is another treatment that uses low-frequency pulse currents to stimulate nerves or muscles, inducing passive muscle contraction to improve muscle function and treat neuromuscular diseases and injuries34. EMS can be divided into normal muscle electrical stimulation therapy and denervation muscle electrical stimulation therapy according to whether the muscles used have normal innervation, which can increase muscle strength and delay muscle atrophy, respectively35. Owing to its noninvasiveness, practicality, and ease of operation, EMS is widely used in the rehabilitation field for conditions such as central or peripheral nerve injuries and musculoskeletal system diseases36. Combining BFRT with EMS can help prevent muscle mass loss during limb disuse and enhance muscle strength and hypertrophy when incorporated into strength training37,38.
The injuries sustained in football significantly impact athletes’ muscle function and sports performance, as well as pose a serious threat to their careers. While extensive research has focused on injuries among the relatively small number of professional football players, there has been limited focus on injuries affecting millions of amateur players. Thus, this study aimed to investigate the effects of combining BFRT with EMS on muscle strength, muscle activation, muscle volume, and sports performance. It was hypothesized that both modalities would increase muscle function and sports performance and that their combined use would additively augment the effects of sports performance indicators in amateur football players with KOA.
Methods
Participants
Based on our previous research39,40it was determined that at least 10–14 participants per group are required to detect significant changes. Therefore, a total of 64 male football players from the Football Academy of Chengdu Sport University, all of whom were certified as second-level athletes by the General Administration of Sport of China, participated in this study. The first participant entered the study on March 19, 2023, enrollment was completed on December 1, 2023, and the last participant was assessed on January 5, 2024. This study confirmed that informed consent was obtained from all participants. The inclusion criteria required participants to be diagnosed with KOA via cartilage-sensitive magnetic resonance imaging (MRI) by a doctor to present non-specific symptoms including activity-related pain and effusion, etc., as well as no recent fresh, unscabbed open wounds. The exclusion criteria encompass participants with documented allergies to pressurized materials, inability to complete the required intervention exercises for personal reasons, intolerance to experimentally applied pressure or electrical stimulation intensities, and the incidence of other adverse reactions. Four participants withdrew from this study because of injury and competition tasks, leaving 60 participants who completed this experiment.
Study design
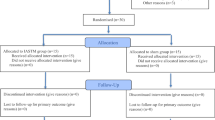
The entire study was conducted at Chengdu Sport University (Chengdu, China). All procedures were reviewed and approved by the Ethics Committee of Chengdu Sport University and were conducted according to the principles of the Declaration of Helsinki. This study was registered with the Chinese Clinical Trial Registry with registration number ChiCTR2300072984 (29/06/2023). The experimental flow chart is shown in Fig. 1, and the intervention and assessment schedules are presented in Table 1. The participants were randomly divided into four groups by the random number remainder grouping method, namely, the control group (CTR, n = 16), BFRT-alone group (BFRT, n = 16), EMS-alone group (EMS, n = 16), or BFRT combined with EMS group (CMB, n = 16). Operation steps: (1) 64 participants numbered 1 to 64. (2) The random number generator function in SPSS 22.0 (SPSS Inc., USA) software was used to generate random numbers so that each participant would obtain a random number. (3) The random number was divided by the number of groups four to find the remainder. If the remainder is 1, they would be assigned to the CTR group, if the remainder is 2, they would be assigned to the EMS group, if the remainder is 3, they would be assigned to the BFRT group, and if they are divisible, they would be assigned to the CMB group.

The Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
Intervention
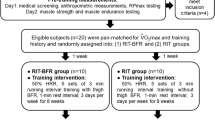
The CTR group followed the RT program, which was conducted once daily over four days each week for eight weeks. The RT program performed the high-bar squat training at 25% 1RM. A metronome controlled the rhythm of the squat at 10 times/min (3 s concentric/3 s eccentric). In each set, the participants squat 30 reps in total and rest for 1 min after every 10 reps, and the total time for each set is 5 min. The participants repeat three sets with 2 min between sets. At the end of the second, fourth, and sixth weeks of intervention, the 1RM was reassessed periodically to adjust for exercise intensity appropriately. The BFRT group performed the same RT program as the CTR group did. According to the leg circumference inflated to the appropriate pressure (≤ 50 cm, 200 mmHg; 51–55 cm, 250 mmHg; 56–59 cm, 300 mmHg; ≥60 cm, 350 mmHg)41a 5-cm wide tourniquet cuff (B-strong, USA) was placed at the groin crease during each set of squats. Each session comprised three cycles of 5 min of inflation and 2 min of deflation. The EMS group performed the same RT program as the CTR group and BFRT group did. Before performing the RT program, an exercise pointer was used to accurately locate the most obvious point of muscle contraction. Two negative electrodes (5 × 5 cm) were placed approximately 10 cm below the groin crease, and the other two positive electrodes (5 × 5 cm) were placed as close as possible to the movement points of the vastus lateralis and medial muscles. The electrical muscle stimulator (Twin Stim Plus: Tens Unit 7000, USA) was set to a duty cycle of 3 s ON (stimulation) and 3 s OFF (no stimulation), a pulse width of 400 µs, a stimulation intensity of 50 mA, and a stimulation frequency of 75 Hz42. The CMB group performed the same RT program as the other three groups did. BFRT and EMS were carried out simultaneously during the RT program in the same way as above (Fig. 2). This study assigned code names to different groups to ensure that participants in each group were unaware of the names of the interventions involved.
The participants’ name, age, sex, and knee joint symptoms were recorded. All participants fully understood the entire trial process and the contraindications and indications for the use of the experimental equipment and signed informed consent forms. The participants gathered raw data on several parameters: the times for the 10-m sprint, 20-m sprint, and Illinois agility test (IAT); the height of the countermovement jump (CMJ); as well as measurements related to muscle, including peak torque (PT) for knee extension, root mean square (RMS) and cross-sectional area (CSA) of the rectus femoris (RF). Before the official intervention, the participants underwent 2 days of adaptive training according to their respective groups to familiarize themselves with the testing procedures and the interventions of each group. All interventions were conducted at the same time of day and at the same adequate temperature and relative air humidity ranges (26˚C-28˚C and 65–70%, respectively) in the Institute of Sports Medicine and Health at Chengdu Sport University. After the 8-week intervention, the participants were measured again for sports performance, muscle strength, muscle activation, and muscle volume. Before the data collection period, an expert trained researchers in the procedures, and they carried out these evaluations without knowledge of this study’s objectives and the participant’s group membership.

Flowchart of intervention procedures for each group. Notes: BFRT: blood flow restriction training, EMS: electrical muscle stimulation.
Outcome measurement
Speed
Speed ability was assessed by completion times of 10-m and 20-m sprints collected by a telemetric photocell timing system (Witty System, Microgate, Italia). The photocell gates were placed at a height of 0.3 m from the ground. The participants started each test with a standing split stance with the toes of the front foot 0.3 m behind the first gate and placed the other two gates at 10 m and 20 m, respectively. Each competitor selects a sprint start time and a full-load sprint in two tests. Three tests are conducted, with a 3-min rest between tests, and the shortest times of 10-m and 20-m sprints were used as the final sprint times to evaluate speed ability43.
Jump
The CMJ was measured to evaluate jumping ability. The participants stood upright with arms on hips, hands on waist, and feet positioned hip-width apart. The participants were asked to perform a rapid downward movement at a self-selected depth and then a rapid upward movement to jump as high as possible44. The CMJ height was measured using the Jump Tester (CSTF-ZT, Tongfang Health Technology, China) to assess jumping ability. The participants were tested three times, and the best CMJ height was retained for analysis.
Agility
The IAT is a reliable and valid protocol for assessing the ability of male team athletes to change direction quickly45. The test was performed in an area of 10 × 5 m consisting of four cones, with another four cones placed in the center of the test area at a distance of 3.3 m from each other. The test began with participants lying face down with their hands at shoulder level. After the trial started, the participants began to run as fast as possible. When they crossed the finish line without knocking down any cones, the experiment was deemed complete, and the time was recorded. The IAT time was measured to evaluate agility ability using the telemetric photocell timing system (Witty System, Microgate, Italia). Each participant performed three trials, and the shortest IAT time was used for analysis.
Muscle strength
Muscle strength was assessed by extracting PT of knee extension using an isokinetic dynamometer (Con-Trex MJ, CMV AG, Switzerland). The participants were seated with the backrest at 90° and strapped across the chest, waist, and thighs. The dynamometer was aligned with the knee joint axis, and the participant’s dominant leg was immobilized approximately 3 cm proximal to the medial malleolus. The method used to determine the dominance limb was self-report46. The test included concentric knee extension and flexion at 60°/s. Four repetitions of increasing intensity were performed as a warm-up program to familiarize the procedure, followed by five maximal-effort repetitions of knee extension, and quadriceps strength was assessed by measuring PT during knee extension. Provide programmed verbal encouragement and visual feedback on real-time data during contractions to enable participants to contract as quickly and forcefully as possible.
Muscle activation
Muscle functional activity was recorded via a wireless surface electromyography (sEMG) system (Myon 320, Schwarzenberg, Switzerland) while isokinetic strength testing was performed. The target muscle was the RF on the dominant limb. According to the surface EMG for non-invasive assessment of muscles (SENIAM) project recommendations, the electrodes corresponding to the vastus medialis were placed at 80% of the line between the anterior superior iliac spine and the anterior joint space of the anterior border of the medial ligament. The electrodes corresponding to the vastus lateralis muscle were placed 2/3 along the line from the anterior iliac superior to the lateral patella. The electrodes corresponding to the RF muscle were placed at 50% of the line between the anterior superior iliac spine and the upper part of the patella. Before electrode placement, specific areas were shaved, and the participants’ skin was cleaned with alcohol. The distance between the two bipolar Ag-AgCl surface electrodes was 20–30 nm. To process the raw data with a sampling frequency of 2000 Hz, the sEMG data were rectified, filtered, smoothed, and normalized via proEMG software (Myon 320, Schwarzenberg, Switzerland). The RMS standard value was selected as the time domain analysis index of the sEMG signal to evaluate quadriceps muscle activation for statistical analysis.
Muscle volume
The muscle CSA of the RF was measured to assess muscle volume via real-time B-mode ultrasonography (CX50, Philips Medical Systems, Netherlands). During the ultrasound assessment, the participant was placed in a supine position with the hip and ankle joints in neutral positions and the knee joint fully extended. The probe was placed perpendicular to the skin without applying pressure, and the rectus femoris marking point was half the distance between the anterior superior iliac spine and the inferior edge of the patella47.
Statistical analyses
Data were presented as the means ± standard deviations (SDs) with 95% confidence intervals (CIs) unless otherwise stated. A paired samples t-test was used to analyze the differences (Delta) in the data before and after the intervention. Possible differences between each pair of groups in the Delta changes in every outcome measure were tested through independent t-tests. The effect sizes were expressed as Cohen’s d to indicate the mean difference within and between groups, with values of ≤ 0.2 as small effects, 0.5 as medium effects, and 0.8 as large effects48. Statistical significance was set at p < 0.05. All the statistical analyses were performed via SPSS Statistics version 24.0 (IBM Corp, Chicago, IL, USA) by researchers blinded to participant allocation.
Results
Speed
The sprint performance data before and after the intervention were shown in Fig. 3A and B. No differences were observed for 10-m sprint and 20-m sprint times between the groups before the intervention. A within-group decrease in 10-m sprint time was observed only in the CMB group (Δ = -0.051 ± 0.032, p < 0.001, ES = -1.596) after the intervention. Similarly, the CMB group had a significant difference in the 10-m sprint compared with the CTR group (p < 0.001, ES = 1.319), whereas the BFRT group (p = 0.136, ES = 0.542) and EMS group (p = 0.109, ES = 0.584) were not significantly different from the CTR group. Within-group decreases in 20-m sprint time were observed in the CMB group (Δ = -0.208 ± 0.057, p < 0.001, ES = -3.657), the BFRT group (Δ = -0.123 ± 0.036, p < 0.001, ES = -3.411), and the EMS group (Δ = -0.069 ± 0.025, p < 0.001, ES = -2.787) after the intervention. The CMB group presented significant differences in 20-m sprint time compared with the BFRT group (p = 0.015, ES = 0.913), the EMS group (p < 0.001, ES = 1.455), and the CTR group (p < 0.001, ES = 2.067). Similarly, the BFRT group (p < 0.001, ES = 1.442) and the EMS group (p = 0.017, ES = 0.891) had more substantial decreases in 20-m sprint time compared with the CTR group. Notably, no significant difference between the BFRT group and the EMS group was observed (p = 0.076, ES = -0.649). The statistical results were presented in Tables 2 and 3.

Between-group comparisons of sports performance at baseline and after the 8th week of interventions. (A) 10-m sprint, (B) 20-m sprint, (C) CMJ, (D) IAT. CTR: Control group, BFRT: BFR-alone group, EMS: EMS-alone group, CMB: BFR combined with EMS group, CMJ: countermovement jump, IAT: Illinois agility test. (a) Comparison with CTR group, p < 0.05, (b) comparison with BFRT group, p < 0.05, (c) comparison with EMS group, p < 0.05, (d) comparison with CMB group, p < 0.05.
Jump
The jump performance data before and after the intervention were shown in Fig. 3C. No differences in CMJ height were observed between the groups before the intervention. Within-group increases in CMJ height were observed in the CMB group (Δ = 4.354 ± 1.232, p < 0.001, ES = 3.535), the BFRT group (Δ = 2.596 ± 0.886, p < 0.001, ES = 2.931), and the EMS group (Δ = 2.453 ± 0.874, p < 0.001, ES = 2.807) after the intervention. The CMB group presented significant differences in CMJ height compared with the BFRT group (p = 0.019, ES = -0.876), the EMS group (p < 0.001, ES = -1.402), and the CTR group (p < 0.001, ES = -2.700). Similarly, the BFRT group (p < 0.001, ES = -1.567) and the EMS group (p < 0.001, ES = -1.137) presented more notable increases in CMJ height compared with the CTR group. In contrast, no significant difference between the BFRT group and the EMS group was observed (p = 0.207, ES = 0.456). The statistical results were presented in Tables 2 and 3.
Agility
The agility performance data before and after the intervention were shown in Fig. 3D. No differences were observed in the IAT time between the groups before the intervention. Within-group decreases in IAT time were observed in the CMB group (Δ = -0.432 ± 0.110, p < 0.001, ES = -3.844), the BFRT group (Δ = -0.231 ± 0.111, p < 0.001, ES = -2.075), and the EMS group (Δ = -0.285 ± 0.115, p < 0.001, ES = -2.488) after the intervention. The CMB group presented significant differences in IAT time compared with the BFRT group (p = 0.009, ES = 0.993), the EMS group (p = 0.018, ES = 0.884), and the CTR group (p < 0.001, ES = 2.562). Similarly, the BFRT group (p < 0.001, ES = 1.573) and the EMS group (p < 0.001, ES = 1.663) had more substantial decreases in IAT time compared with the CTR group. However, no significant difference between the BFRT group and the EMS group was observed (p = 0.778, ES = 0.100). The statistical results were presented in Tables 2 and 3.
Muscle strength
The muscle strength data before and after the intervention were shown in Fig. 4. No differences were observed in the PT values between the groups before the intervention. Within-group increases in PT values were observed in the CMB group (Δ = 41.769 ± 7.824, p < 0.001, ES = 5.339), the BFRT group (Δ = 26.688 ± 4.526, p < 0.001, ES = 5.872), and the EMS group (16.923 ± 4.881, p < 0.001, ES = 3.467) after the intervention. The CMB group presented significant differences in PT values compared with the BFRT group (p < 0.001, ES = -1.334), the EMS group (p < 0.001, ES = -1.966), and the CTR group (p < 0.001, ES = -4.323). A more substantial increase in PT was also detected in the BFRT group than in the EMS group (p = 0.032, ES = 0.797) and the CTR group (p < 0.001, ES = -2.937). Similarly, there was a significant PT change in the EMS group compared with the CTR group (p < 0.001, ES = -1.724). The statistical results were presented in Tables 2 and 3.

Between-group comparisons of muscle strength at baseline and after the 8th week of interventions. CTR: Control group, BFRT: BFR-alone group, EMS: EMS-alone group, CMB: BFR combined with EMS group, PT: Peak torque of dominant knee extension. (a) Comparison with CTR group, p < 0.05, (b) comparison with BFRT group, p < 0.05, (c) comparison with EMS group, p < 0.05, (d) comparison with CMB group, p < 0.05.
Muscle activation
The muscle activation data before and after the intervention were shown in Fig. 5. No differences were observed in the RMS values between the groups before the intervention. Within-group increases in RMS values were observed in the CMB group (Δ = 20.749 ± 3.856, p < 0.001, ES = 5.381), the BFRT group (Δ = 2.833 ± 3.921, p < 0.001, ES = 0.722), and the EMS group (Δ = 18.378 ± 2.821, p < 0.001, ES = 6.514) after the intervention. The CMB group and the EMS group presented significant differences in RMS values compared with the BFRT group (CMB group: p < 0.001, ES = -1.252, EMS group: p = 0.019, ES = -0.876) and the CTR group (CMB group: p < 0.001, ES = -2.327, EMS group: p < 0.001, ES = -1.979), whereas there were no significant differences between the CMB group and the EMS group (p = 0.220, ES = -0.443). A more significant increase in the RMS value was also detected in the BFRT group than in the CTR group ( p = 0.007, ES = -1.029). The statistical results were presented in Tables 2 and 3.

Between-group comparisons of muscle activation at baseline and after the 8th week of interventions. CTR: Control group, BFRT: BFR-alone group, EMS: EMS-alone group, CMB: BFR combined with EMS group, RMS: root mean square of RF on the dominant side. (a) Comparison with CTR group, p < 0.05, (b) comparison with BFRT group, p < 0.05, (c) comparison with EMS group, p < 0.05, (d) comparison with CMB group, p < 0.05.
Muscle volume
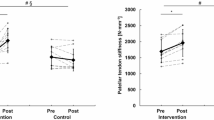
The muscle volume data before and after the intervention were shown in Fig. 6. No differences were observed in the CSA values between the groups before the intervention. Within-group increases in CSA values were observed in the CMB group (Δ = 3.713 ± 0.769, p < 0.001, ES = 4.831), the BFRT group (Δ = 2.881 ± 0.592, p < 0.001, ES = 4.862), and the EMS group (Δ = 1.164 ± 0.519, p < 0.001, ES = 2.243) after the intervention. Compared with those in the EMS group and the CTR group, the CSA values in the CMB group (EMS group: p = 0.004, ES = 3.399, CTR group: p = 0.002, ES = -1.204) and the BFRT group (EMS group: p = 0.014, ES = 0.918, CTR group: p = 0.008, ES = -1.014) were significantly different, whereas there were no significant differences between the CMB group and the BFRT group (p = 0.525, ES = -0.227). Similarly, there were no significant differences between the EMS group and the CTR group (p = 0.789, ES = -0.096). The statistical results were presented in Tables 2 and 3.

Between-group comparisons of muscle volume at baseline and after the 8th week of interventions. CTR: Control group, BFRT: BFR-alone group, EMS: EMS-alone group, CMB: BFR combined with EMS group, CSA: Cross-sectional area of RF on the dominant side. (a) Comparison with CTR group, p < 0.05, (b) comparison with BFRT group, p < 0.05, (c) comparison with EMS group, p < 0.05, (d): Comparison with CMB group, p < 0.05.
Discussion
This study focused on male football players with KOA who are unable to perform high-load strength training. By choosing low-load resistance training combined with BFRT and EMS, this study explored whether the combination of BFRT and EMS can compensate for the lack of application effect of either intervention method and thereby improve the sports performance of football players with KOA. In addition, the effects of 8 weeks of BFRT, EMS, and BFRT combined with EMS intervention on muscle strength, muscle activation, and muscle volume in football players with KOA have also been reported.
Knee injury or surgery, aging, lower bone density, sex, and obesity are well-recognized risk factors for KOA49. Engaging in continuous physical activity that can easily lead to knee injuries has been identified as a major risk factor for the early onset of KOA50. A meta-analysis indicated that sports exerting excessive loads on the hip and knee joints substantially increase the risk of OA51. Contact sports such as American football, ice hockey, and handball involve numerous high-impact movements that promote the development of KOA49. Multiple epidemiological surveys have revealed that the knee joint is the most frequently injured site among football players. Injury history and insufficient hip control are common triggering factors for knee joint injuries. Furthermore, football is among the sports with the greatest biomechanical stress on the knee joint. Higher-level professional football players have a greater proportion of knee varus alignment than does the general population, and knee varus increases the risk of osteoarthritis and inflammation52. The main activities in football include running, accelerating, decelerating, changing directions and jumping without the ball, dribbling, shooting, and confronting between players with and without the ball53. Multiple studies have confirmed that KOA is the most common chronic injury among professional football players during and after their careers54,55. The biomechanical changes caused by KOA symptoms in football cause a decrease in sports performance, including explosive power and agility, thereby affecting the results of teams and players in competitions. Muscles play important roles in maintaining the stability and flexibility of the knee joint. Changes in thigh muscle strength and muscle mass are also related to the incidence of KOA56. Currently, there are no drugs supported by high-quality evidence that can improve the clinical symptoms related to KOA and slow its progression. Therefore, it is crucial to find non-surgical and non-pharmacological methods that effectively improve thigh muscle function. Long-term KOA, neuromuscular diseases, and metabolic diseases all lead to a reduction in the CSA and muscle strength of the quadriceps and an increase in quadriceps intramuscular adipose tissue57,58. These muscle changes lead to the deterioration of lower limb function and decreased exercise performance in KOA patients. Symptoms of KOA frequently result in diminished muscle strength, hence elevating the risk of knee injury and impairing athletic performance in patients with KOA59,60. Conventional strength training and plyometric exercises can improve muscle strength, running speed, anaerobic capacity, and aerobic capacity in heavy-lift football players, but the substantial loads are challenging for KOA football players, hindering their ability to improve muscle strength and athletic performance without causing considerable pain and other symptoms61. Therefore, this study utilized low-intensity resistance training at 25% of 1RM, an intensity that markedly diminishes the occurrence of pain sensations in KOA patients during training. The integration of BFRT and EMS in an 8-week low-intensity squat regimen enhanced speed, jumping ability, and agility in KOA football players unable to engage in high-intensity training. After combining BFRT and EMS, low-intensity squat exercises can improve the speed, jump, and agility of football players with KOA who are unable to engage in high-intensity training. Importantly, this improvement in sports performance is notably superior to combining BFRT or EMS interventions alone. These results can improve the situation where knee osteoarthritis pain prevents football players from engaging in high-intensity strength training, affecting the contraction of lower limb muscles and causing abnormal knee joint movements during exercise. Moreover, fulfilling certain standard agility training tasks remains a difficulty for KOA football players62. The integration of low-intensity resistance training with BFRT and EMS can enhance agility and positively influence explosive power, aerobic endurance, and other attributes, representing a multifaceted intervention strategy with extensive improvement benefits.
Although Kraemer et al.63 have shown that traditional resistance training with a weight of ≥ 70% 1RM is sufficient to induce muscle hypertrophy and improve muscle strength effectively. This study took into account that KOA athletes generally suffer from knee joint pain during heavy weight resistance and selected only low-intensity (25% 1RM) squat training as a strength training method. The role of muscle growth in muscle strength is supported mainly by cross-sectional and retrospective studies. Although strong evidence demonstrating the necessity of increased muscle size for strength gains is lacking, cross-sectional data suggest that athletes have greater lean muscle mass than controls or non-athletes do64. Takarada et al.65 found that BFRT combined with low-intensity (50% 1RM) resistance training and high-intensity (80% 1RM) resistance training had similar effects on improving muscle strength and muscle circumference growth, and both effects were significant. It is better than low-intensity (50% 1RM) resistance training alone, and it is believed that training combined with BFRT can produce training effects similar to those of high-intensity strength training. Enhancing muscle strength relies not only on CSA enlargement but also on improved innervation and heightened recruitment of motor units. Thus, increasing muscle strength involves increasing muscle size and motor unit activation. The mechanism by which EMS promotes muscle strength growth is closely related to the stimulation intensity and stimulation frequency. Pantović et al.66 showed that EMS has the same training effect as traditional high-intensity resistance training in improving muscle strength. EMS can improve the control of motor nerves by the central system and coordinate the agonist and antagonist muscles, thereby promoting the recruitment of motor units and activating more muscle fibers to improve muscle strength. BFRT-induced metabolic stress (hypoxia/acidosis) stimulates insulin-like growth factor-1 (IGF-1) release, activating phosphatidylinositol 3-kinase/protein kinase B/mechanistic target of rapamycin (PI3K/Akt/mTORC1) signaling, while EMS directly phosphorylates Akt/mTORC1 via electrically evoked contractions. Their combination significantly amplifies phosphorylation of downstream effectors (S6 kinase 1 and ribosomal protein S6), augmenting muscle protein synthesis (MPS)67. EMS chronically shifts myosin heavy chain isoforms from fast-twitch (myosin heavy chain (MyHc) IIb/ MyHc-IIx) to slow-twitch (MyHc-IIa/MyHc-I) phenotypes68. BFRT preferentially recruits high-threshold type II fibers via metabolic stress69. Jointly, they optimize fiber transition (IIb to IIa to I) and recruitment, improving strength and endurance. EMS inhibits ubiquitin-proteasome pathways and autophagy markers (e.g., microtubule-associated protein 1 light chain 3) to reduce muscle protein breakdown (MPB)70whereas BFRT indirectly suppresses catabolism via mTORC1 activation71. Their synergy maintains net protein accretion. This mechanism overcomes individual limitations (e.g., BFRT inefficacy without contraction, EMS-induced fatigue at high frequencies), accelerating functional recovery after KOA. These results revealed that 8 weeks of BFRT combined with EMS can effectively improve PT during knee flexion and extension, the cross-sectional area of the rectus femoris, and the degree of muscle recruitment. The intervention effect was better than that of BFRT or EMS alone. Strength training is a viable approach for addressing symptoms associated with the older KOA population72. However, this population frequently encounters pain and other symptoms during strength training due to excessive load, which impairs the efficacy of treatment. This study confirmed that EMS combined with BFRT strength training can improve thigh muscle strength deficits in KOA football players by enhancing muscle recruitment and increasing muscle CSA at a lower strength training intensity, effectively preventing further muscle strength loss. Therefore, we believe that the positive effects of BFRT combined with EMS can also be applied to the older KOA population, but attention should be paid to the implementation parameters of BFRT and EMS, and further research is still needed to confirm its effectiveness.
The results of this study revealed that 8 weeks of BFRT combined with EMS resulted in significant changes in the CSA of RF compared with the EMS and low-intensity resistance exercise. Greater muscle size contributes to increased muscle strength, which is positively associated with various aspects of athletic performance. Maximal size and strength are associated with increased power and are associated with many factors related to sports performance, such as sprinting and jumping73. These results also confirmed that 8 weeks of BFRT combined with EMS led to greater improvements in 10-m sprint, 20-m sprint, and CMJ performance than did the use of BFRT or EMS alone. The average sprint time in football is approximately 2 s, and the sprint distance is approximately 14 m, which means that athletes in football matches may not necessarily reach their maximum speed in a short sprint74. Therefore, the ability to accelerate quickly to achieve high sprint speeds is an important component of a football player’s performance. Although the jumping ability of football is not as high as that of basketball and other sports, actions such as fighting for high-altitude balls and pitching and attacking goals also have certain requirements for jumping ability. In addition, jumping ability is an important indicator used to measure explosive power. Muscle strength and jumping ability demonstrated a notable positive correlation. Lamont et al.75 showed that 6 weeks of resistance training can improve 30-cm depth jump performance. This study revealed that BFRT combined with EMS can improve the explosive power of football players with KOA under low-intensity resistance training. In addition to sprinting, football involves multiple continuous direction changes that require high agility. It consists of dynamic movements such as running forward and backward and moving in multiple directions76. Agility represents the ability to quickly and accurately change the direction of whole-body movement when stimulated77. Football players with KOA experience decreased sensitivity due to pain and other reasons, which is related to a decrease in neuromuscular recruitment. EMS has been widely used to improve neuromuscular recruitment. In traditional active training, the brain sends electrical pulse signals to motor nerves to cause muscle contraction. In contrast, the EMS sends electrical pulse signals from the electrical stimulator. The current is distributed and transmitted through the electrode patch, passing through the skin, reaching the nervous system, activating the motor nerves, and then controlling muscle contraction. Fil et al.78 found that 4 weeks of EMS (30–35 Hz, 250–350 µs) can increase EMG electrical signals and muscle strength, thereby preventing muscle atrophy after stroke. This finding is consistent with our results. Both BFRT combined with EMS and EMS alone can improve neuromuscular recruitment of the rectus femoris and effectively shorten the duration of the IAT. Unfortunately, because the intervention duration of this study was 8 weeks, during the experimental research phase, the original female participants were reluctant to participate in strength training due to physiological reasons such as menstruation, so only male football players were recruited. However, the positive effects of this study should also be applicable to female football players. Therefore, these findings suggest that BFRT combined with EMS can improve the explosiveness and agility of football players with KOA to improve sports performance.
This study has several limitations. First, this study included only male football players with KOA, and the results of this study have a certain gender bias. As women’s participation in multiple sports, such as football, increases annually, future studies can recruit female football players with KOA as subjects to clarify the intervention effects for subjects of different genders. Second, this study focused only on the effect on sports performance and lacked long-term follow-up on injury risk, but sports performance is usually negatively correlated with the injury rate. The injuries of the subjects in football during the intervention period can be recorded later to clarify the effect of BFRT combined with EMS on injury prevention. Thirdly, the intervention period of this study was 8 weeks, which is a short intervention period. Subsequent studies on the effects of different intervention periods on sports performance can be conducted to clarify the effects of the intervention period on the effect and refine the parameters of the intervention program.
Conclusions
BFRT combined with EMS during low-intensity squat training enhances muscle strength, explosiveness, and agility in football players with KOA through increased muscle hypertrophy and improved neuromuscular recruitment. This combined modality provides a viable training alternative for athletes with joint limitations who cannot tolerate high-load exercises.
Data availability
The datasets and materials used and analyzed in the current study are available from the corresponding author upon reasonable request.
References
Wang, L. & Ye, Y. Trends and projections of the burden of osteoarthritis disease in China and globally: A comparative study of the 2019 global burden of disease database. Prev. Med. Rep. 37, 102562. https://doi.org/10.1016/j.pmedr.2023.102562 (2024).
Zeng, C. et al. Risk of venous thromboembolism in knee, hip and hand osteoarthritis: a general population-based cohort study. Ann. Rheum. Dis. 79, 1616–1624. https://doi.org/10.1136/annrheumdis-2020-217782 (2020).
Safiri, S. et al. Global, regional and national burden of osteoarthritis 1990–2017: a systematic analysis of the global burden of disease study 2017. Ann. Rheum. Dis. 79, 819–828. https://doi.org/10.1136/annrheumdis-2019-216515 (2020).
Xue, Q. et al. The survey of the prevalence of primary osteoarthritis in the population aged 40 years and over in China. Chin. J. Orthop. 35, 1206–1212. https://doi.org/10.3760/cma.j.issn.0253-2352.2015.12.005 (2015).
Kolasinski, S. L. et al. American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. (Hoboken N J). 72, 220–233. https://doi.org/10.1002/art.41142 (2019).
Wang, Y. et al. Knee osteoarthritis, potential mediators, and risk of all-cause mortality: data from the osteoarthritis initiative. Arthritis Care Res. 73, 566–573. https://doi.org/10.1002/acr.24151 (2021).
Buckwalter, J. A., Martin, J. A. & Brown, T. D. Perspectives on chondrocyte mechanobiology and osteoarthritis. Biorheology 43, 603–609 (2006).
Madry, H. et al. Early osteoarthritis of the knee. Knee Surg. Sports Traumatol. Arthrosc. 24, 1753–1762. https://doi.org/10.1007/s00167-016-4068-3 (2016).
Buckwalter, J. A. Sports, joint injury, and posttraumatic osteoarthritis. J. Orthop. Sports Phys. Ther. 33, 578–588. https://doi.org/10.2519/jospt.2003.33.10.578 (2003).
Driban, J. B. et al. Association of knee injuries with accelerated knee osteoarthritis progression: data from the osteoarthritis initiative. Arthritis Care Res. 66, 1673–1679. https://doi.org/10.1002/acr.22359 (2014).
Saxon, L., Finch, C. & Bass, S. Sports participation, sports injuries and osteoarthritis: implications for prevention. Sports Med. (Auckland N Z). 28, 123–135. https://doi.org/10.2165/00007256-199928020-00005 (1999).
Drawer, S. & Fuller, C. W. Evaluating the level of injury in english professional football using a risk based assessment process. Br. J. Sports Med. 36, 446–451. https://doi.org/10.1136/bjsm.36.6.446 (2002).
Bradley, P. S., Di Mascio, M., Peart, D., Olsen, P. & Sheldon, B. High-intensity activity profiles of elite soccer players at different performance levels. J. Strength. Conditioning Res. 24, 2343–2351. https://doi.org/10.1519/JSC.0b013e3181aeb1b3 (2010).
Dalen, T., Ingebrigtsen, J., Ettema, G., Hjelde, G. H. & Wisløff, U. Player load, acceleration, and deceleration during forty-five competitive matches of elite soccer. J. Strength. Conditioning Res. 30, 351–359. https://doi.org/10.1519/jsc.0000000000001063 (2016).
Roth, T. S. & Osbahr, D. C. Knee injuries in elite level soccer players. Am. J. Orthop. (Belle Mead N J) 47. https://doi.org/10.12788/ajo.2018.0088 (2018).
Beckwée, D. et al. The influence of joint loading on bone marrow lesions in the knee: A systematic review with Meta-analysis. Am. J. Sports Med. 43, 3093–3107. https://doi.org/10.1177/0363546514565092 (2015).
Sihvonen, R. et al. Arthroscopic partial meniscectomy for a degenerative meniscus tear: a 5 year follow-up of the placebo-surgery controlled FIDELITY (Finnish Degenerative Meniscus Lesion Study) trial. Br. J. Sports Med. 54, 1332–1339. https://doi.org/10.1136/bjsports-2020-102813 (2020).
Liao, C. D., Huang, S. W., Huang, Y. Y. & Lin, C. L. Effects of sarcopenic obesity and its confounders on knee range of motion outcome after total knee replacement in older adults with knee osteoarthritis: A retrospective study. Nutrients 13 https://doi.org/10.3390/nu13113817 (2021).
Henricsdotter, C. et al. Changes in ultrasound assessed markers of inflammation following intra-articular steroid injection combined with exercise in knee osteoarthritis: exploratory outcome from a randomized trial. Osteoarthr. Cartil. 24, 814–821. https://doi.org/10.1016/j.joca.2015.12.010 (2016).
Alrushud, A. S., Rushton, A. B., Kanavaki, A. M. & Greig, C. A. Effect of physical activity and dietary restriction interventions on weight loss and the musculoskeletal function of overweight and obese older adults with knee osteoarthritis: a systematic review and mixed method data synthesis. BMJ Open. 7, e014537. https://doi.org/10.1136/bmjopen-2016-014537 (2017).
van Doormaal, M. C. M., Meerhoff, G. A., Vlieland, V., Peter, W. & T. P. M. F. A clinical practice guideline for physical therapy in patients with hip or knee osteoarthritis. Musculoskelet. Care. 18, 575–595. https://doi.org/10.1002/msc.1492 (2020).
Page, C. J., Hinman, R. S. & Bennell, K. L. Physiotherapy management of knee osteoarthritis. Int. J. Rheum. Dis. 14, 145–151. https://doi.org/10.1111/j.1756-185X.2011.01612.x (2011).
Nijs, J., Kosek, E., Van Oosterwijck, J. & Meeus, M. Dysfunctional endogenous analgesia during exercise in patients with chronic pain: To exercise or not to exercise? Pain Phys. 15, Es205-213 (2012).
Bichsel, D., Liechti, F. D., Schlapbach, J. M. & Wertli, M. M. Cross-sectional analysis of recommendations for the treatment of hip and knee osteoarthritis in clinical guidelines. Arch. Phys. Med. Rehabil. 103, 559–569e555. https://doi.org/10.1016/j.apmr.2021.07.801 (2022).
Zeng, C. Y., Zhang, Z. R., Tang, Z. M. & Hua, F. Z. Benefits and mechanisms of exercise training for knee osteoarthritis. Front. Physiol. 12, 794062. https://doi.org/10.3389/fphys.2021.794062 (2021).
Li, Y. et al. The effects of resistance exercise in patients with knee osteoarthritis: a systematic review and meta-analysis. Clin. Rehabil. 30, 947–959. https://doi.org/10.1177/0269215515610039 (2016).
Medicine, A. C. & o., S. American college of sports medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports. Exerc. 41, 687–708. https://doi.org/10.1249/MSS.0b013e3181915670 (2009).
Ferraz, R. B. et al. Benefits of resistance training with blood flow restriction in knee osteoarthritis. Med. Sci. Sports. Exerc. 50, 897–905. https://doi.org/10.1249/mss.0000000000001530 (2018).
Lixandrão, M. E. et al. Magnitude of muscle strength and mass adaptations between high-load resistance training versus low-load resistance training associated with blood-flow restriction: A systematic review and meta-analysis. Sports Med. (Auckland, N.Z.) 48, 361–378 (2018). https://doi.org/10.1007/s40279-017-0795-y
Hwang, P. S. & Willoughby, D. S. Mechanisms behind blood flow-restricted training and its effect toward muscle growth. J. Strength. Conditioning Res. 33 (Suppl 1), S167–s179. https://doi.org/10.1519/jsc.0000000000002384 (2019).
Fatela, P. et al. Acute neuromuscular adaptations in response to low-intensity blood-flow restricted exercise and high-intensity resistance exercise: Are there any differences? J. Strength. Conditioning Res. 32, 902–910. https://doi.org/10.1519/jsc.0000000000002022 (2018).
Rodrigues, S. et al. Effect of blood flow restriction technique on delayed onset muscle soreness: A systematic review. Medicine (Kaunas Lithuania) 58. https://doi.org/10.3390/medicina58091154 (2022).
Wortman, R. J., Brown, S. M., Savage-Elliott, I., Finley, Z. J. & Mulcahey, M. K. Blood flow restriction training for athletes: A systematic review. Am. J. Sports Med. 49, 1938–1944. https://doi.org/10.1177/0363546520964454 (2021).
Nishikawa, Y. et al. The effect of electrical muscle stimulation on quadriceps muscle strength and activation patterns in healthy young adults. Eur. J. Sport Sci. 21, 1414–1422. https://doi.org/10.1080/17461391.2020.1838617 (2021).
Mukherjee, S., Fok, J. R. & van Mechelen, W. Electrical stimulation and muscle strength gains in healthy adults: A systematic review. J. Strength. Conditioning Res. 37, 938–950. https://doi.org/10.1519/jsc.0000000000004359 (2023).
Doucet, B. M., Lam, A. & Griffin, L. Neuromuscular electrical stimulation for skeletal muscle function. Yale. J. Biol. Med. 85, 201–215 (2012).
Slysz, J. T. et al. Blood flow restriction combined with electrical stimulation attenuates thigh muscle disuse atrophy. Med. Sci. Sports. Exerc. 53, 1033–1040. https://doi.org/10.1249/mss.0000000000002544 (2021).
Slysz, J. T. & Burr, J. F. The effects of blood flow restricted electrostimulation on strength and hypertrophy. J. Sport Rehabilitation. 27, 257–262. https://doi.org/10.1123/jsr.2017-0002 (2018).
Li, N., Yang, J. & Liao, Y. The effect of blood flow restriction training combined with electrical muscle stimulation on neuromuscular adaptation: a randomized controlled trial. Front. Physiol. 14, 1182249. https://doi.org/10.3389/fphys.2023.1182249 (2023).
Kohavi, B. et al. Effectiveness of Field-Based resistance training protocols on hip muscle strength among young elite football players. Clin. J. Sport Med. 30, 470–477. https://doi.org/10.1097/jsm.0000000000000649 (2020).
Jia Wei, B. L., Feng, L. & Li, Y. Methodological factors and potential safety problems of blood flow restriction training. China Sport Sci. Technol. 55, 3-12. https://doi.org/10.16470/j.csst.2019021 (2019).
Filipovic, A., Kleinöder, H., Dörmann, U. & Mester, J. Electromyostimulation–A systematic review of the influence of training regimens and stimulation parameters on effectiveness in electromyostimulation training of selected strength parameters. J. Strength. Conditioning Res. 25, 3218–3238. https://doi.org/10.1519/JSC.0b013e318212e3ce (2011).
Trajković, N. et al. Short-Term FIFA 11 + Improves agility and jump performance in young soccer players. Int. J. Environ. Res. Public Health 17. https://doi.org/10.3390/ijerph17062017 (2020).
Hernandez-Martinez, J. et al. Effects of different plyometric training frequencies on physical performance in youth male volleyball players: a randomized trial. Front. Physiol. 14, 1270512. https://doi.org/10.3389/fphys.2023.1270512 (2023).
Hachana, Y. et al. Test-retest reliability, criterion-related validity, and minimal detectable change of the Illinois agility test in male team sport athletes. J. Strength. Conditioning Res. 27, 2752–2759. https://doi.org/10.1519/JSC.0b013e3182890ac3 (2013).
Coren, S. & Porac, C. The validity and reliability of self-report items for the measurement of lateral preference. Br. J. Psychol. 69, 207–211 (1978). https://doi.org/10.1111/j.2044-8295.1978.tb01649.x
Arts, I. M., Pillen, S., Schelhaas, H. J., Overeem, S. & Zwarts, M. J. Normal values for quantitative muscle ultrasonography in adults. Muscle Nerve. 41, 32–41. https://doi.org/10.1002/mus.21458 (2010).
Cohen, J. A power primer. Psychol. Bull. 112, 155–159. https://doi.org/10.1037/0033-2909.112.1.155 (1992).
Freiberg, A., Bolm-Audorff, U. & Seidler, A. The risk of knee osteoarthritis in professional soccer Players—A systematic review with meta-analyses. Deutsches Arzteblatt Int. 118, 49–55. https://doi.org/10.3238/arztebl.m2021.0007 (2021).
Merčun, A., Drobnič, M., Žlak, N. & Krajnc, Z. Knee osteoarthritis in the former elite football players and the ordinary population: A comparative cross-sectional study. Sci. Med. Football. 1–5. https://doi.org/10.1080/24733938.2023.2228279
Bestwick-Stevenson, T., Ifesemen, O. S., Pearson, R. G. & Edwards, K. L. Association of sports participation with osteoarthritis: A systematic review and Meta-Analysis. Orthop. J. Sports Med. 9, 23259671211004554. https://doi.org/10.1177/23259671211004554 (2021).
Fernandes, G. S. et al. Prevalence of knee pain, radiographic osteoarthritis and arthroplasty in retired professional footballers compared with men in the general population: a cross-sectional study. Br. J. Sports Med. 52, 678–683. https://doi.org/10.1136/bjsports-2017-097503 (2018).
Gonçalves, B. V., Figueira, B. E., Maçãs, V. & Sampaio, J. Effect of player position on movement behaviour, physical and physiological performances during an 11-a-side football game. J. Sports Sci. 32, 191–199. https://doi.org/10.1080/02640414.2013.816761 (2014).
Volpi, P., Quaglia, A., Carimati, G., Petrillo, S. & Bisciotti, G. N. High incidence of hip and knee arthroplasty in former professional, male football players. J. Sports Med. Phys. Fit. 59, 1558–1563. https://doi.org/10.23736/s0022-4707.18.08962-4 (2019).
Prien, A. et al. Every second retired elite female football player has MRI evidence of knee osteoarthritis before age 50 years: a cross-sectional study of clinical and MRI outcomes. Knee Surg. Sports Traumatol. Arthroscopy: Official J. ESSKA. 28, 353–362. https://doi.org/10.1007/s00167-019-05560-w (2020).
Felson, D. T. et al. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann. Intern. Med. 133, 635–646. https://doi.org/10.7326/0003-4819-133-8-200010170-00016 (2000).
Kumar, D. et al. Association of quadriceps adiposity with an increase in knee cartilage, meniscus, or bone marrow lesions over three years. Arthritis Care Res. 73, 1134–1139. https://doi.org/10.1002/acr.24232 (2021).
Burakiewicz, J. et al. Quantifying fat replacement of muscle by quantitative MRI in muscular dystrophy. J. Neurol. 264, 2053–2067. https://doi.org/10.1007/s00415-017-8547-3 (2017).
Fältström, A. et al. Poor knee strength is associated with higher incidence of knee injury in adolescent female football players: the Karolinska football injury cohort. Knee Surg. Sports Traumatol. Arthrosc. https://doi.org/10.1002/ksa.12567 (2024).
Newman, M. A., Tarpenning, K. M. & Marino, F. E. Relationships between isokinetic knee strength, single-sprint performance, and repeated-sprint ability in football players. J. Strength. Cond Res. 18, 867–872. https://doi.org/10.1519/13843.1 (2004).
Perez-Gomez, J. et al. Effects of weight lifting training combined with plyometric exercises on physical fitness, body composition, and knee extension velocity during kicking in football. Appl. Physiol. Nutr. Metab. 33, 501–510. https://doi.org/10.1139/h08-026 (2008).
González-Fernández, F. T., Sarmento, H., Castillo-Rodríguez, A., Silva, R. & Clemente, F. M. Effects of a 10-week combined coordination and agility training program on young male soccer players. Int. J. Environ. Res. Public Health. 18. https://doi.org/10.3390/ijerph181910125 (2021).
Kraemer, W. J. et al. American college of sports medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports. Exerc. 34, 364–380. https://doi.org/10.1097/00005768-200202000-00027 (2002).
Ode, J. J., Pivarnik, J. M., Reeves, M. J. & Knous, J. L. Body mass index as a predictor of percent fat in college athletes and nonathletes. Med. Sci. Sports. Exerc. 39, 403–409. https://doi.org/10.1249/01.mss.0000247008.19127.3e (2007).
Takarada, Y. et al. Effects of resistance exercise combined with moderate vascular occlusion on muscular function in humans. J. Appl. Physiol. (Bethesda, Md.: 1985) 88, 2097–2106. https://doi.org/10.1152/jappl.2000.88.6.2097 (2000).
Pantović, M., Popović, B., Madić, D. & Obradović, J. Effects of neuromuscular electrical stimulation and resistance training on knee extensor/flexor muscles. Coll. Antropol. 39 (Suppl 1), 153–157 (2015).
Yoshikawa, M. et al. Effects of combined treatment with blood flow restriction and low-current electrical stimulation on muscle hypertrophy in rats. J. Appl. Physiol. (Bethesda, Md.: 1985) 127, 1288–1296. https://doi.org/10.1152/japplphysiol.00070.2019 (2019).
Gondin, J. et al. Neuromuscular electrical stimulation training induces atypical adaptations of the human skeletal muscle phenotype: a functional and proteomic analysis. J. Appl. Physiol. (Bethesda Md. : 1985). 110, 433–450. https://doi.org/10.1152/japplphysiol.00914.2010 (2011).
Suga, T. et al. Intramuscular metabolism during low-intensity resistance exercise with blood flow restriction. J. Appl. Physiol. (Bethesda Md. : 1985). 106, 1119–1124. https://doi.org/10.1152/japplphysiol.90368.2008 (2009).
Liu, A. Y. et al. Low-frequency electrical stimulation alleviates immobilization-evoked disuse muscle atrophy by repressing autophagy in skeletal muscle of rabbits. BMC Musculoskelet. Disord. 23, 398. https://doi.org/10.1186/s12891-022-05350-5 (2022).
Drummond, M. J. et al. Rapamycin administration in humans blocks the contraction-induced increase in skeletal muscle protein synthesis. J. Physiol. 587, 1535–1546. https://doi.org/10.1113/jphysiol.2008.163816 (2009).
Küçük, H. et al. Strength training intervention for adult individuals with knee osteoarthritis: Establishing fidelity. Front. Physiol. 16. https://doi.org/10.3389/fphys.2025.1583153 (2025).
Suchomel, T. J., Nimphius, S. & Stone, M. H. The importance of muscular strength in athletic performance. Sports Med. (Auckland N Z). 46, 1419–1449. https://doi.org/10.1007/s40279-016-0486-0 (2016).
Reilly, T. Energetics of high-intensity exercise (soccer) with particular reference to fatigue. J. Sports Sci. 15, 257–263. https://doi.org/10.1080/026404197367263 (1997).
Lamont, H. S. et al. Effects of 6 weeks of periodized squat training with or without whole-body vibration on short-term adaptations in jump performance within recreationally resistance trained men. J. Strength. Conditioning Res. 22, 1882–1893. https://doi.org/10.1519/JSC.0b013e3181821a1a (2008).
Stepinski, M., Ceylan, H. I. & Zwierko, T. Seasonal variation of speed, agility and power performance in elite female soccer players: effect of functional fitness. J. Phys. Activity Rev. 1, 16–25. https://doi.org/10.16926/par.2020.08.03 (2020).
Sheppard, J. M. & Young, W. B. Agility literature review: classifications, training and testing. J. Sports Sci. 24, 919–932. https://doi.org/10.1080/02640410500457109 (2006).
Fil, A., Armutlu, K., Atay, A. O., Kerimoglu, U. & Elibol, B. The effect of electrical stimulation in combination with Bobath techniques in the prevention of shoulder subluxation in acute stroke patients. Clin. Rehabil. 25, 51–59. https://doi.org/10.1177/0269215510375919 (2011).
Acknowledgements
The authors would like to express their gratitude to the Football Academy and the Department of Sports Medicine and Health Football Team of Chengdu Sport University for their valuable assistance.
Funding
This study was supported by the Basic Cultivation Project of Sichuan Provincial Expert Workstation and Institute of Sports Medicine and Health of Chengdu Sports University (No: SCZJJCC-16), the China National Natural Science Foundation Cultivation Project of Chengdu Sport University (No: 23YJPY10), and the Key Laboratory of Sports Medicine of Sichuan Province and the State Sports General Administration of China (No: 2023-A022).
Author information
Authors and Affiliations
Contributions
Jinfeng Yang, Na Li, and Yuanpeng Liao conceptualized the study and its methodology. Jinfeng Yang, Xiao Peng, and Yunyan Zhou supervised the intervention. Jinfeng Yang, Na Li, Sheng He, and Jinqi Yang performed the data collection and curation. Jinfeng Yang, Na Li, and Jianxin Chen performed the data analysis. Jinfeng Yang, Na Li, Jinqi Yang, and Jianxin Chen interpreted the results and wrote the original manuscript. Jinfeng Yang, Na Li, and Yuanpeng Liao wrote and critically reviewed the final version. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, J., Li, N., He, S. et al. Effects of blood flow restriction combined with electrical stimulation on muscle functions and performance in university football players with knee osteoarthritis. Sci Rep 15, 34590 (2025). https://doi.org/10.1038/s41598-025-18089-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-18089-5
