
Abstract
This study aimed to estimate the effects of preoperative psychological health on postoperative outcomes in patients undergoing surgery for cervical spondylotic radiculopathy. This retrospective cohort study included data from patients enrolled in the Canadian Spine Outcomes and Research Network who underwent anterior cervical discectomy and fusion for radiculopathy. Preoperative psychological health was measured with the Patient Health Questionnaire-8 (PHQ-8), and depression and severe psychological symptomology were measured with the Mental Component Score of the Short Form Survey-12 (MCS). Surgical outcomes comprised trajectory subgroups for neck pain and arm pain (numeric rating scales) and disability (neck disability index) measured preoperatively and 3, 12, and 24 months after surgery. For each outcome, patients were dichotomized as following either a poor or a fair-to-excellent trajectory. Average treatment effects were estimated with doubly robust propensity score models using inverse probability of treatment weights accounting for multiple confounders. We included data from 352 patients (43.8% female). Approximately half (52.1%) of patients were identified as depressed based on the PHQ-8, while 61.8% and 33.1% were classified as experiencing depression or severe psychological symptomology, respectively, on the MCS. In fully adjusted models, patients with PHQ-8-measured depression were at increased risk of poor postoperative outcomes for disability (risk ratio[95% CI] = 6.73[1.85 to 24.45]) and neck pain (RR[95% CI] = 1.90[1.09 to 3.32]). Patients with MCS-measured depression were at elevated risk of a poor disability outcome (RR[95% CI] = 2.77[1.30 to 5.90]). Patients reporting severe psychological symptomatology had an increased likelihood of poor disability, neck pain, and arm pain outcomes (RR[95% CI] = 1.82 [1.17 to 2.82] to 2.84[1.58 to 5.09]). These findings highlight the high prevalence of negative psychological features and their impacts on neck surgery outcomes. Future research should prioritize the development and evaluation of preoperative interventions to optimize psychological well-being and improve surgical outcomes in this population.
Similar content being viewed by others


Introduction
Neck disorders are a leading source of disability worldwide1 and the second most common reason for primary care musculoskeletal consultations2. Cervical spondylotic radiculopathy is a common neck disorder with an estimated annual incidence of 83.2 cases per 100,000 persons3. Characterized by pain, numbness, and sensory and motor deficits in the affected arm, cervical radiculopathy can adversely impact quality of life and functional ability if not treated effectively4,5,6.
Several treatment options exist for cervical spondylotic radiculopathy, including nonoperative therapies and surgery7. Approximately 1/4 to 1/3 of patients require operative treatment3,8, usually in the form of anterior cervical discectomy and fusion (ACDF)9,10. While most patients benefit from this surgery, recent evidence shows that clinical outcomes are heterogeneous, and psychological factors such as depression and depression risk can predict some of the variability11. This accords with other studies showing that psychological health is associated with the clinical outcomes of surgery for lumbar spinal stenosis surgery12, and the pain experience in general13,14. However, it is unknown whether the relationships between psychology and surgical outcomes are associational (i.e., predictive) or if psychological factors affect the levels of pain and disability experienced by patients following cervical spine surgery.
Randomized trials are widely regarded as the benchmark method for determining the effect of a treatment or exposure due to their ability to balance confounding and prognostic variables within exposure groups15. However, it can be challenging, unethical, or impossible to assign participants to some exposures (e.g., depression). Advances in epidemiological methods have improved the accuracy of estimating effects from observational data and can yield results consistent with those from randomized trials16.
Considering the potential impact of psychological health on patients with spinal disorders, it is crucial to determine whether psychological features are simply associated with postoperative pain and disability or if they directly impact these surgical outcomes. Therefore, we analyzed data from a national spine surgery registry to evaluate the effects of preoperative psychological health factors on neck surgery outcomes. Specifically, we estimated the average treatment effects of depression and severe psychological symptomology on the two-year trajectories of arm pain, neck pain, and disability in patients undergoing ACDF for cervical spondylotic radiculopathy.
Methods
Study design and participants
We undertook a retrospective cohort study with data from the Canadian Spine Outcomes and Research Network, a national network of surgical spine centres across Canada. Psychological health variables were measured at the preoperative baseline, and pain and disability outcomes were measured preoperatively and then 3, 12, and 24 months after surgery.
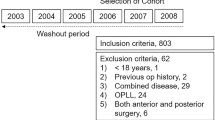
In July 2021, we accessed data from patients with spine surgeon-diagnosed cervical radiculopathy who had undergone single or multi-level ACDF from January 2015 to March 2021. Data from patients diagnosed with tumours, infections, inflammatory arthritis, fractures, or myelopathy were excluded. Local ethics boards approved the data collection at each spine centre, and all patients gave written informed consent. Research Ethics Boards approved the current study protocol at the University of New Brunswick (2019-161) and Horizon Health Network (2019-2797). The research was conducted in accordance with the Declaration of Helsinki.
Psychological health exposures
We examined three evaluations of preoperative psychological health that comprised two measures of depression and one measure of severe psychological symptomology. Depression was measured prior to surgery using the Patient Health Questionnaire-8 (PHQ-8). The PHQ-8 has previously been validated for use in the general17 and spine surgery populations18. Scores ≥ 10 on the PHQ-8 indicate patients at moderate-to-severe risk of depression, a classification with 88% sensitivity and specificity for major depression19.
Health-related quality of life was measured using the Short-Form 12-Item Health Status Survey version 2 (SF-12), which is reliable and valid in people living with non-cancer-related pain20,21. This scale yields a mental component summary (MCS) score ranging from 0 to 100, with higher scores indicating better mental health. Patients with MCS scores less than 46 were categorized as experiencing depression, while those with MCS scores less than 37 were classified as having severe psychological symptomology22. The validity of these MCS cutpoints was established through comparisons to the outcomes of the structured composite international diagnostic interview, version 2.122.
Clinical outcomes
Pain and disability scores were recorded at the preoperative baseline and 3, 12, and 24 months postoperatively. Neck pain and arm pain intensity were assessed using an 11-point numeric pain rating scale (NPRS) with scores ranging from zero “no pain” to 10 “worst pain imaginable”. The NPRS has previously been validated for use in patients with various pain sources23,24 and is reliable for use in patients with cervical radiculopathy25,26. Estimated NPRS minimal important change values range from 2.2 points for patients with cervical radiculopathy25 to 2.5 points for patients undergoing cervical spine fusion27.
Disability was quantified using the neck disability index. Scored on a 100-point scale28, this index is the most widely used and validated tool to assess neck-related disability29, with an intra-class correlation of 0.88 in patients with cervical radiculopathy or myelopathy30. Studies of patients undergoing ACDF for cervical radiculopathy estimate minimal important changes to be 16.0–27.6%31.
Final pain and disability outcomes were represented by established trajectories of arm pain, neck pain, and neck pain-related disability from the preoperative baseline to 24 months after surgery. The full details of this analysis have been reported previously11. Briefly, we constructed latent class growth models that identified three trajectory subgroups for each outcome (Fig. 1). To be included in the model, patients were required to have valid outcome data reported for at least two of the four designated measurement points (i.e., baseline, 3 months, 12 months, 24 months). Depending on the outcome, 8.5% to 9.0% of patients were excluded for missing data. Average follow-up at each point was: 99.9% at baseline, 92.7% at 3 months, 84.7% at 12 months, and 75.6% at 24 months.

Estimated perioperative trajectories and prevalence estimates of (A) disability, (B) neck pain, and (C) arm pain outcomes from preoperative baseline to 24 months post-surgery. Shaded areas represent 95% confidence intervals.
Each model identified a “poor” outcome subgroup with a 15.5% to 23.5% prevalence. For the current analysis, we collapsed the “good” and “excellent” subgroups for arm and neck pain and the “fair” and “excellent” subgroups for disability to create contrasts with patients assigned to the “poor” outcome subgroup.
Potential confounders and additional variables
Baseline demographic, health, and clinical data were collected on all patients as part of a standardized assessment, and all data were maintained in the central CSORN registry. Self-reported variables comprised age, sex, highest level of education attained, and current smoking status. Surgical wait time was calculated as the days from surgical consultation to the date of surgery. Physical health-related quality of life was estimated with the physical component score of the SF-1232.
Data analysis
All statistical analyses were performed using STATA/SE version 18 (StataCorp, College Station, TX). To estimate the average treatment effects of depression and severe psychological symptomatology on the trajectories of arm pain, neck pain, and disability, we combined exposure (propensity score) and outcome (regression) modelling to construct doubly robust effect estimates33.
First, we estimated covariate balancing propensity scores to balance the exposure groups on key confounders34. We examined for covariate balance by ensuring that standardized differences for all confounders were less than 0.1 between the exposure groups and variance ratios were between 0.5 and 2.035,36. We visually inspected the distribution of propensity scores with overlap plots35. Propensity scores were converted to inverse probability of treatment weights for application in subsequent regression models.
Average treatment effects were estimated with weighted robust Poisson Regression models. Results were reported with adjusted risk ratios (RR) and marginal risk estimates showing the probability of poor outcomes for each exposure group. When binary outcomes are common, robust Poisson models are preferred as they yield more precise and less inflated estimates than logistic regression37,38.
Owing to the uncertainty of the causal path between the psychological variables and postoperative pain and disability39, we applied two adjustment sets. First, we conditioned on a limited number of confounders to minimize potential overadjustment bias40: age, sex, education, and smoking status. Second, we constructed more inclusive models that additionally controlled for the physical component of health-related quality of life, surgical wait time, the number of spinal levels operated on, and the preoperative scores of neck pain intensity (arm pain models), arm pain intensity (neck pain models), or neck and arm pain intensity (disability models).
Sensitivity analyses
We conducted sensitivity analyses to investigate potential bias owing to unmeasured confounding and extreme inverse probability of treatment weights. The potential for unmeasured confounding in all significant models was estimated with E-value methodology41. E-values quantify the impact, on the risk ratio scale, that an unmeasured confounder would need to fully explain away the estimated effect, conditional on the measured covariates. To evaluate the effect of extreme weights on variance inflation, we truncated the inverse probability weights at 5% and 95% and repeated all models after applying the alternate weights42.
Results
We included data from 352 patients (43.8% female; mean [SD] age = 50.9 [9.5] years) treated at one of 12 participating spine centres. Propensity score model diagnostics were acceptable; standardized differences between patients with and without the psychological health characteristics of interest were < 0.01, and variance ratios ranged from 0.78 to 1.65, indicating balance on all confounders. Overlap plots showed an adequate balance of propensity scores between the exposure groups. The preoperative characteristics of the study sample are reported in Table 1. Risk ratios of the effect of the psychological health variables on disability, neck pain, and arm pain for limited and fully adjusted models are reported in Fig. 2, with corresponding poor outcome probabilities reported in Figs. 3 and 4.

Effects of psychological health states on the risk of poor outcome for disability, neck pain, and arm pain. (2A) Models adjusted for age, sex, education level, and smoking status. (2B) Models adjusted for age, sex, education level, smoking status, physical component score, surgical wait time, number of spinal levels operated on, and baseline pain. PHQ-8 = Patient Health Questionnaire; MCS = Mental Component Score; RR = Risk ratio; CI = confidence interval; E-valueEST = E-value for the estimate; E-valueCI = E-value for the confidence interval.

Probability of poor outcomes in control and at-risk groups undergoing ACDF for cervical radiculopathy from models adjusted for age, sex, education level, and smoking status. At-risk groups include moderate-severe risk of depression (PHQ-8), severe psychological symptomatology (MCS), and depression (MCS). PHQ-8 = Patient Health Questionnaire; MCS = Mental Component Score.

Probability of poor outcomes in control and at-risk groups undergoing ACDF for cervical radiculopathy from models adjusted for age, sex, education level, smoking status, physical component score, surgical wait time, number of spinal levels operated on, and baseline pain. At-risk groups include moderate-severe risk of depression (PHQ-8), severe psychological symptomatology (MCS), and depression (MCS). PHQ-8 = Patient Health Questionnaire; MCS = Mental Component Score.
Effects of psychological health
Depression (PHQ-8)
Approximately half (52.1%) of the patients were identified as being at moderate-to-severe risk of depression. The limited adjustment models showed that moderate-to-severe risk of depression greatly increased the risk of poor outcome for disability (RR [95% CI] = 14.07 [4.42 to 44.85]) and approximately doubled the risk of poor outcome for neck pain (RR [95% CI] = 2.35 [1.42 to 3.89]) and arm pain (RR [95% CI] = 1.91 [1.22 to 2.00]) (Figs. 2, 3). The fully adjusted models yielded similar estimates for disability (RR [95% CI] = 6.73 [1.85 to 24.45]) and neck pain (RR [95% CI] = 1.90 [1.09 to 3.32]), while the arm pain results shifted to include the null (Figs. 2, 4).
Depression (MCS)
Nearly 2 in 3 patients (61.4%) reported MCS scores consistent with a depressive state. Depression increased the risk of poor disability outcome in the limited (RR [95% CI] = 3.46 [1.59 to 7.50]) and fully-adjusted models (RR [95% CI] = 2.77 [1.30 to 5.90]). The remaining model results were non-significant (Figs. 2, 3, 4).
Severe psychological symptomatology (MCS)
Approximately 1 in 3 patients (32.6%) reported MCS scores consistent with severe psychological symptomatology. Severe symptomatology increased the risk of poor disability (RR [95% CI] = 3.91 [2.25 to 6.62]), neck pain (RR [95% CI] = 2.35 [1.54 to 3.59]), and arm pain (RR [95% CI] = 1.92 [1.28 to 2.87]) in limited adjustment models (Figs. 2, 3). Similar results were identified in the fully adjusted models for disability (RR [95% CI] = 2.84 [1.58 to 5.09]), neck pain (RR [95% CI] = 2.08 [1.38 to 3.13]) and arm pain (RR [95% CI] = 1.82 [1.17 to 2.82]) (Figs. 2, 4).
Sensitivity analyses
For the limited adjusted models, the E-values for the estimates ranged from 3.23 to 27.63, and E-values for the confidence interval ranged from 1.74 to 8.31 (Fig. 2). In fully adjusted models, E-values ranged from 3.04 to 12.94 for the estimates and from 1.40 to 3.10 for the confidence intervals (Fig. 2). This indicates that substantial unmeasured confounding (RR ≥ 3.04), above and beyond the impact of measured confounders, would be needed to explain away the observed effects, but weaker confounding could not. Lower levels of unmeasured confounding (RR ≥ 1.40), above and beyond the measured confounders, would be required to shift the confidence interval to include the null.
There were minimal differences between effect estimates using the standard and truncated inverse probability weights, indicating no apparent weight-induced bias on model results. Consequently, we elected to report the results from models applying the standard weights.
Discussion
This study aimed to estimate the average treatment effects of preoperative psychological health factors on postoperative trajectories of pain and disability among patients undergoing ACDF for cervical radiculopathy. We found that patients identified with PHQ-8-measured depression and MCS-measured severe psychological symptomatology were at increased risk of poor outcomes for postoperative disability, arm pain, and neck pain. Similarly, patients with MCS-measured depression were at increased risk of following a poor disability trajectory. Although the effects of MCS-measured depression on postoperative neck and arm pain were non-significant, the effects were similar in magnitude to the other psychological health exposures. Compared to the MCS cut-point for depression, MCS scores indicating severe psychological symptomatology yielded larger and more consistent effect estimates, suggesting a potential dose–response relationship between psychological health and poor outcome risk. In other words, patients with worse psychological health were at greater risk of experiencing poor outcomes. These results were confirmed by sensitivity analyses demonstrating the models’ robustness to bias from extreme weights and residual confounding.
The relationships between pain, disability, and depression are complex43. The current findings support previous research indicating that depression is strongly associated with perceived disability44, and worse disability outcomes following other spinal surgeries12,45,46,47,48. Better mental health status has been similarly linked to better clinical outcomes following ACDF and other spine surgeries.12,46,48,49,50,51,52 We have advanced knowledge gained by studies to date through more robust control of confounding and less biased estimates of effect.
The current results and prior evidence support the routine measurement of psychological health factors in patients who are potential candidates for ACDF. The information gained may help inform surgical decision-making and identify patients who could benefit from preoperative interventions to improve psychological health. However, collecting health information in clinical practice requires a balanced approach that does not overly burden patients or exceed available resources. In our experience, the psychological health screening tools used in the current study (PHQ-8 and SF-12) can be efficiently implemented, even in busy surgical practices.
Future research is needed to better define the effect of psychological health on spinal surgery outcomes. Although randomized trials are traditionally viewed as the optimal design to establish effects, it is not possible to assign patients to different levels of psychological health. However, it will be possible to design and undertake trials to evaluate the potential impact of modifying psychological health before spine surgery, and this will be an important priority for future research efforts. Additionally, it remains uncertain whether the findings of this study are unique to patients undergoing neck surgery or whether they may generalize to patients experiencing other spinal disorders or pain conditions. Future studies evaluating the impacts of psychological health on both surgical and non-surgical outcomes will be essential in answering this question.
The current study had several limitations to consider when interpreting these results. Confounding is a primary concern in all observational studies aimed at estimating the effects of exposures on outcomes of interest53. To address confounding, we applied doubly robust methods incorporating propensity scores with inverse probability weights with regression adjustment. Since there is always uncertainty around the true causal structure, we considered two adjustment strategies: a limited and a more inclusive set of potential confounders, each with advantages and shortcomings. For example, if the limited adjustment set excluded key covariates, the model results would be impacted by confounding bias. Conversely, if the more inclusive adjustment set included potential mediators on the causal pathway between psychological health and the outcomes of interest (e.g., preoperative pain intensity, surgical wait time) or colliders, the results could be susceptible to overadjustment bias40. However, each strategy produced consistent results; 8 of 9 models yielded the same statistical outcome, and there were no substantive shifts in the magnitude of the effect estimates. We also performed sensitivity analyses investigating the potential impact of bias owing to the weighting strategy and the impact of unmeasured confounding, thus enhancing confidence in model outcomes.
Additional study limitations relate to information bias. Although our exposure measures employed standard screening approaches to estimating psychological health, we did not employ criterion diagnostic methods (e.g., diagnostic interviews). Screening tools such as those used in the current study are often used in epidemiological research when more time- and resource-intensive measures are not possible, and they likely represent a more feasible option for application in surgical practice. Nevertheless, when compared to a criterion, screening tools are a potential source of misclassification owing to measurement error. Similarly, we relied on patient-reported measures for covariates (e.g., smoking history, level of education) that may be prone to recall or social-desirability bias.
Conclusions
Most patients with cervical radiculopathy exhibited signs of depression or severe psychological symptomology prior to surgery. Patients with lower levels of preoperative psychological health were at increased risk of experiencing a poor outcome following ACDF. These results highlight the need to routinely collect psychological health information and potentially intervene to improve psychological health prior to spinal surgery.
Data availability
The datasets generated during and/or analysed during the current study are not publicly available due to legal and ethical restrictions but may be available from the Canadian Spine Outcomes and Research Network for researchers meeting the criteria for access to confidential data. Interested parties can contact the corresponding author, Jeffrey Hebert (j.hebert@unb.ca), who will facilitate requests.
Abbreviations
- ACDF:
-
Anterior cervical discectomy and fusion
- PHQ-8:
-
Patient Health Questionnaire-8
- SF-12:
-
Short-Form 12-Item Health Status Survey version 2
- MCS:
-
Mental component summary
- NPRS:
-
Numeric pain rating scale
- RR:
-
Risk ratio
References
GBD 2021 Neck Pain Collaborators. Global, regional, and national burden of neck pain, 1990–2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 6, e142–e155. https://doi.org/10.1016/S2665-9913(23)00321-1 (2024).
Binder, A. I. Cervical spondylosis and neck pain. Br. Med. J. 334, 527–531. https://doi.org/10.1136/bmj.39127.608299.80 (2007).
Radhakrishnan, K., Litchy, W. J., O’Fallon, W. M. & Kurland, L. T. Epidemiology of cervical radiculopathy. Brain 117, 325–335. https://doi.org/10.1093/brain/117.2.325 (1994).
Caridi, J. M., Pumberger, M. & Hughes, A. P. Cervical radiculopathy: a review. Musculoskel. J. Hospital Spec. Surg. 7, 265–272. https://doi.org/10.1007/s11420-011-9218-z (2011).
Carette, S. & Fehlings, M. G. Cervical radiculopathy. N. Engl. J. Med. 353, 392–399 (2005).
Mansfield, M., Smith, T., Spahr, N. & Thacker, M. Cervical spine radiculopathy epidemiology: a systematic review. Musculoskel. Care. 2020, 1–13. https://doi.org/10.1002/msc.1498 (2020).
Onks, C. A. & Billy, G. Evaluation and treatment of cervical radiculopathy. Primary Care: Clin. Office Pract. 40, 837–848. https://doi.org/10.1016/j.pop.2013.08.004 (2013).
Sampath, P., Bendebba, M., Davis, J. & Ducker, T. Outcome in patients with cervical radiculopathy. Prospective, multicenter study with independent clinical review. Spine (Phila Pa 1976) 199, 24. https://doi.org/10.1097/00007632-199903150-00021 (1999).
Iyer, S. & Kim, H. J. Cervical radiculopathy. Curr. Rev. Musculoskelet. Med. 9, 272–280. https://doi.org/10.1007/s12178-016-9349-4 (2016).
Andresen, A. K. et al. Patient-reported outcomes and patient-reported satisfaction after surgical treatment for cervical radiculopathy. Glob. Spine J. 8, 703–708. https://doi.org/10.1177/2192568218765398 (2018).
Hébert, J. J. et al. Prediction of 2-year clinical outcome trajectories in patients undergoing anterior cervical discectomy and fusion for spondylotic radiculopathy. Spine (Phila Pa 1976) 2022, 13. https://doi.org/10.3171/2022.7.SPINE22592 (2022).
Hebert, J. J. et al. Preoperative factors predict postoperative trajectories of pain and disability following surgery for degenerative lumbar spinal stenosis. Spine (Phila Pa 1976) 45, 1421–1430. https://doi.org/10.1097/brs.0000000000003587 (2020).
Linton, S. J. & Bergbom, S. Understanding the link between depression and pain. Scand. J. Pain. 2, 47–54. https://doi.org/10.1016/j.sjpain.2011.01.005 (2011).
Turk, D. C. A diathesis-stress model of chronic pain and disability following traumatic injury. Pain Res. Manag. 7, 9–19. https://doi.org/10.1155/2002/252904 (2002).
Akobeng, A. K. Understanding randomised controlled trials. Arch. Dis. Child. 90, 840–844. https://doi.org/10.1136/adc.2004.058222 (2005).
Moneer, O. et al. Agreement of treatment effects from observational studies and randomized controlled trials evaluating hydroxychloroquine, lopinavir-ritonavir, or dexamethasone for covid-19: Meta-epidemiological study. BMJ 2022, 377. https://doi.org/10.1136/bmj-2021-069400 (2022).
Kroenke, K. et al. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 114, 163–173. https://doi.org/10.1016/j.jad.2008.06.026 (2009).
Purvis, T. E., Neuman, B. J., Riley, L. H. & Skolasky, R. L. Comparison of PROMIS Anxiety and Depression, PHQ-8, and GAD-7 to screen for anxiety and depression among patients presenting for spine surgery. J. Neurosurg. Spine. 30, 524–531. https://doi.org/10.3171/2018.9.SPINE18521 (2019).
Kroenke, K., Spitzer, R. L. & Williams, J. B. W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x (2001).
Hayes, C., Bhandari, N., Kathe, N. & Payakachat, N. Reliability and validity of the medical outcomes study short form-12 version 2 (SF-12v2) in adults with non-cancer pain. Healthcare. 5, 22. https://doi.org/10.3390/healthcare5020022 (2017).
Cheak-Zamora, N. C., Wyrwich, K. W. & McBride, T. D. Reliability and validity of the SF-12v2 in the medical expenditure panel survey. Qual. Life Res. 18, 727–735. https://doi.org/10.1007/s11136-009-9483-1 (2009).
Gill, S. C., Butterworth, P., Rodgers, B. & Mackinnon, A. Validity of the mental health component scale of the 12-item Short-Form Health Survey (MCS-12) as measure of common mental disorders in the general population. Psychiatry Res. 152, 63–71. https://doi.org/10.1016/j.psychres.2006.11.005 (2007).
Karcioglu, O., Topacoglu, H., Dikme, O. & Dikme, O. A systematic review of the pain scales in adults: Which to use?. Am. J. Emerg. Med. 36, 707–714. https://doi.org/10.1016/j.ajem.2018.01.008 (2018).
Ware, L. J., Epps, C. D., Herr, K. & Packard, A. Evaluation of the revised faces pain scale, verbal descriptor scale, numeric rating scale, and Iowa pain thermometer in older minority adults. Pain Manag. Nurs. 7, 117–125. https://doi.org/10.1016/j.pmn.2006.06.005 (2006).
Young, I. A., Cleland, J. A., Michener, L. A. & Brown, C. Reliability, construct validity, and responsiveness of the neck disability index, patient-specific functional scale, and numeric pain rating scale in patients with cervical radiculopathy. Am. J. Phys. Med. Rehabil. 89, 831–839. https://doi.org/10.1097/PHM.0b013e3181ec98e6 (2010).
Cleland, J. A., Fritz, J. M., Whitman, J. M. & Palmer, J. A. The reliability and construct validity of the neck disability index and patient specific functional scale in patients with cervical radiculopathy. Spine (Phila Pa 1976) 31, 598–602. https://doi.org/10.1097/01.brs.0000201241.90914.22 (2006).
Carreon, L. Y., Glassman, S. D., Campbell, M. J. & Anderson, P. A. Neck disability index, short form-36 physical component summary, and pain scales for neck and arm pain: the minimum clinically important difference and substantial clinical benefit after cervical spine fusion. Spine J. 10, 469–474. https://doi.org/10.1016/j.spinee.2010.02.007 (2010).
Vernon, H. & Mior, S. The neck disability index: a study of reliability and validity. J. Manipul. Physiol. Ther. 14, 409–415 (1991).
Vernon, H. The neck disability index: State-of-the-art, 1991–2008. J. Manipul. Physiol. Ther. 31, 491–502. https://doi.org/10.1016/j.jmpt.2008.08.006 (2008).
Gupte, G., Peters, C. M., Buchowski, J. M. & Zebala, L. P. Reliability of the neck disability index and Japanese orthopedic association questionnaires in adult cervical radiculopathy and myelopathy patients when administered by telephone or via online format. Spine J. 19, 1154–1161. https://doi.org/10.1016/J.SPINEE.2019.03.002 (2019).
Parker, S. L., Godil, S. S., Shau, D. N., Mendenhall, S. K. & Mcgirt, M. J. Assessment of the minimum clinically important difference in pain, disability, and quality of life after anterior cervical discectomy and fusion: clinical article. J. Neurosurg. Spine 18, 154–160. https://doi.org/10.3171/2012.10.SPINE12312 (2013).
Ware, J. E., Kosinski, M. & Keller, S. D. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 34, 220–233. https://doi.org/10.1097/00005650-199603000-00003 (1996).
Kang, J. D. Y. & Schafer, J. L. Demystifying double robustness: a comparison of alternative strategies for estimating a population mean from incomplete data. Stat. Sci. 22, 523–539. https://doi.org/10.1214/07-STS227 (2007).
Imai, K. & Ratkovic, M. Covariate balancing propensity score. J. R. Stat. Soc. Ser. B Stat. Methodol. 76, 243–263. https://doi.org/10.1111/rssb.12027 (2014).
Austin, P. C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 28, 3083–3107. https://doi.org/10.1002/sim.3967 (2009).
Rubin, D. B. Using propensity scores to help design observational studies: application to the tobacco litigation. Health Serv. Outcomes Res. Methodol. 2, 169–188. https://doi.org/10.1023/A:1020363010465/METRICS (2001).
Greenland, S. Interpretation and choice of effect measures in epidemiologic analyses. Am. J. Epidemiol. 125, 761–768. https://doi.org/10.1093/OXFORDJOURNALS.AJE.A114593 (1987).
Chen, W., Qian, L., Shi, J. & Franklin, M. Comparing performance between log-binomial and robust Poisson regression models for estimating risk ratios under model misspecification. BMC Med. Res. Methodol. 2018, 18. https://doi.org/10.1186/s12874-018-0519-5 (2018).
Yao, C. et al. Exploring the bidirectional relationship between pain and mental disorders: a comprehensive Mendelian randomization study. J. Headache Pain. 24, 82. https://doi.org/10.1186/s10194-023-01612-2 (2023).
Schisterman, E. F., Cole, S. R. & Platt, R. W. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology 20, 488–495. https://doi.org/10.1097/EDE.0b013e3181a819a1 (2009).
VanderWeele, T. J. & Ding, P. Sensitivity in observational research: Introducing the E-value. Ann. Intern. Med. 2017, 167. https://doi.org/10.7326/M16-2607 (2017).
Cole, S. R. & Hernán, M. A. Constructing inverse probability weights for marginal structural models. Am. J. Epidemiol. 168, 656–664. https://doi.org/10.1093/aje/kwn164 (2008).
Wong, J. J. et al. Association between depressive symptoms or depression and health outcomes for low back pain: a systematic review and meta-analysis. J. Gen. Intern. Med. 37, 1233–1246. https://doi.org/10.1007/s11606-021-07079-8 (2022).
Börsbo, B., Peolsson, M. & Gerdle, B. The complex interplay between pain intensity, depression, anxiety and catastrophising with respect to quality of life and disability. Disabil. Rehabil. 31, 1605–1613. https://doi.org/10.1080/09638280903110079 (2009).
Held, U. et al. Association between depression and anxiety on symptom and function after surgery for lumbar spinal stenosis. Sci. Rep. 12, 2821. https://doi.org/10.1038/s41598-022-06797-1 (2023).
Trief, P. M., Grant, W. & Fredrickson, B. A prospective study of psychological predictors of lumbar surgery outcome. Spine (Phila Pa 1976) 25, 2616–2621. https://doi.org/10.1097/00007632-200010150-00012 (2000).
Adogwa, O. et al. Preoperative Zung Depression Scale predicts outcome after revision lumbar surgery for adjacent segment disease, recurrent stenosis, and pseudarthrosis. Spine J. 12, 179–185. https://doi.org/10.1016/j.spinee.2011.08.014 (2012).
Aalto, T. J. et al. Preoperative predictors for postoperative clinical outcome in lumbar spinal stenosis: systematic review. Spine (Phila Pa 1976) 31, 648–663. https://doi.org/10.1097/01.brs.0000231727.88477.da (2006).
Godlewski, B., Stachura, M. K., Twardowska-Staszek, E., Czepko, R. A. & Czepko, R. Effect of social factors on surgical outcomes in cervical disc disease. Anesthiol. Pain Med. 2018, 8. https://doi.org/10.5812/aapm.84140 (2018).
Peolsson, A., Vavruch, L. & Öberg, B. Predictive factors for arm pain, neck pain, neck specific disability and health after anterior cervical decompression and fusion. Acta Neurochir. (Wien). 148, 167–173. https://doi.org/10.1007/s00701-005-0660-x (2006).
Alvin, M. D. et al. The impact of preoperative depression and health state on quality-of-life outcomes after anterior cervical diskectomy and fusion. Glob. Spine J. 6, 306–313. https://doi.org/10.1055/s-0035-1562932 (2016).
Phan, K. et al. Relationship between depression and clinical outcome following anterior cervical discectomy and fusion. J. Spine Surg. 3, 133. https://doi.org/10.21037/JSS.2017.05.02 (2017).
Hernán, M. A., Hernández-Diaz, S., Werler, M. M. & Mitchell, A. A. Causal knowledge as a prerequisite for confounding evaluation: an application to birth defects epidemiology. Am. J. Epidemiol. 155, 176–184. https://doi.org/10.1093/aje/155.2.176 (2002).
Author information
Authors and Affiliations
Contributions
EEC: Analysis, interpretation, drafting and editing, final approval of submission. EB, SUD, NW, ER: Interpretation, review and editing, final approval of submission. NM, NA, EA, CS, MMHY, EC, MHW, JP, SDC, RCM, BL, AN, HH, YRR, CF, ND, CB: Data acquisition, interpretation, review and editing, final approval of submission. JJH: Design, analysis, interpretation, review and editing, final approval of submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cunningham, E.E., Bigney, E., Dombrowski, S.U. et al. Preoperative psychological health impacts pain and disability outcomes following anterior cervical discectomy and fusion for cervical radiculopathy. Sci Rep 15, 14861 (2025). https://doi.org/10.1038/s41598-025-97575-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-97575-2
