
Abstract
This study aimed to compare the effects of two high-intensity interval training modalities on body composition and muscular fitness in obese young adults and examined the characteristics of energy expenditure (EE) after training. Thirty-six obese young adults (eleven female, age: 22.1 ± 2.3 years, BMI: 25.1 ± 1.2 kg/m2) were to Whole-body high-intensity interval training group (WB-HIIT) (n = 12), jump rope high-intensity interval training group (JR-HIIT) (n = 12), or non-training control group (CG) (n = 12). WB-HIIT and JR-HIIT groups performed an 8-week HIIT protocol. WB-HIIT, according to the program of unarmed resistance training, JR-HIIT use rope-holding continuous jump training, each execution of 4 sets of 4 × 30 s training, interval 30 s, inter-set interval 1min, and the control group maintained their regular habits without additional exercise training. Body composition and muscular strength were assessed before and after 8 weeks. Repeated measures analysis of variance and clinical effect analysis using Cohen’s effect size were used, with a significance level of p < 0.05. In comparison with the CG group in both experimental groups, Body Mass and BMI significantly reduced (p < 0.05), and Muscular strength significantly improved (p < 0.05).WB-HIIT versus JR-HIIT: Fat Mass (− 1.5 ± 1.6; p = 0.02 vs − 2.3 ± 1.2; p < 0.01) and % Body Fat (− 1.3 ± 1.7; p = 0.05 vs − 1.9 ± 1.9; p < 0.01) the effect is more pronounced in the JR-HIIT group; Muscle Mass (1.5 ± 0.7; p < 0.01 vs − 0.8 ± 1.1; p = 0.07) the effect is more pronounced in the WB-HIIT group. Estimated daily energy intake (122 ± 459 vs 157 ± 313; p > 0.05). Compared to the CG, body composition was significantly improved in both intervention groups. All three groups had no significant changes in visceral adipose tissue (p > 0.05). Significant differences in Lipid and Carbohydrate oxidation and energy output were observed between the two groups, as well as substantial differences in WB-HIIT and JR-HIIT VO2, ventilation, and energy consumption minute during the 0–5 min post-exercise period (p > 0.05). WB-HIIT and JR-HIIT interventions effectively improve the body composition of young adults with obesity, while WB-HIIT additionally improves muscular fitness. After exercise, WB-HIIT produces higher excess post-exercise oxygen consumption and associated lipid and carbohydrate metabolism than JR-HIIT.
Similar content being viewed by others


Introduction
By 2022, 2.5 billion adults (43%) had excess body weight, of whom 890 million (16%) were obese. In 2019, excess body mass index was responsible for 5 million deaths from non-communicable diseases such as cardiovascular and neurological diseases1. Obesity has become one of the global public health problems, and there is an association between physical activity and body weight in adults2. Physical activity is one of the most important ways of preventing and treating excessive weight and excess adiposity, and the World Health Organization recommends that adults engage in at least 150 min of moderate-intensity physical activity or 75 min of vigorous-intensity physical activity per week3. Despite the well-known benefits of moderate- to vigorous-intensity physical activity (PA), 31% of adults worldwide do not match the PA recommended by the World Health Organization (WHO)4. There are many barriers to adult participation in physical activity, such as environment, cost, equipment, and lack of time, and it is essential to provide adults with convenient, efficient, and easy-to-perform forms of exercise5.
Recently HIIT has received a lot of attention as an effective way to improve body composition, lipid metabolism6, and cardiorespiratory fitness in overweight and obese people7, and to improve exercise adherence8, a form of exercise that is safe, reliable, and well-tolerated9. However, classic HIIT modalities, including running, cycling, or rowing, still lack convenience for adults. These modalities could hurt exercise adherence, as “lack of enjoyment” is a commonly cited barrier to regular PA10. Whole-body HIIT (WB-HIIT) has recently received scholarly attention, WB-HIIT using weights as resistance can be an exciting and cost-effective alternative. It can help overcome exercise barriers such as lack of time, cost, limited facilities, and transportation difficulties11. WB-HIIT has the same effect as traditional high-intensity interval training, improving body composition and cardiorespiratory fitness, and more importantly, improving muscular endurance and strengthening skeletal muscle health12.
Schaun et al.13 demonstrated that 8 min of all-out style WB-HIIT (e.g., burpees, mountain climbers, squats, and jumping jacks) conducted 3 times per week for 16 weeks, elicited similar improvements in VO2max as MICT (30-min treadmill running, 3/week) in health men. Scoubeau et al.14 demonstrated that 8 weeks of home-based WB-HIIT elicited greater muscle endurance (~ 28%) improvement in inactive adults. Scott et al.15 demonstrated that 12 weeks of home-based WB-HIIT improve the structural and endothelial enzymatic properties of skeletal muscle in adults with obesity. Poon et al.16 demonstrated that WB-HIIT is relatively strenuous and triggers greater acute cardiometabolic stress than MICT compared to both MICT and ERG-HIIT training modalities. Jump ropes have been proposed to elevate PA and improve health in obese populations, requiring minimal, inexpensive equipment and limited space17. Additionally, several studies demonstrated that jump rope HIIT (JR-HIIT) can reduce inflammatory factors and improve body composition and cardiovascular health indicators in populations with obesity18,19.
Previous studies have shown that HIIT can effectively improve physical health, but the mechanism and effect of HIIT exercise after fat loss have not been clearly explained. Sturdy et al.20 research findings on kettlebell complexes and high-intensity functional training showed that there were no significant differences in EPOC produced after exercise, although significant associations were revealed for mean HR as well as post-exercise VE and Bla. Jiang et al.21 Demonstrate that HIIT post-exercise brings greater EPOC under isoenergetic constraints, especially in the first 10 min after exercise (HIIT:45.91 kcal and MICT: 34.39 kcal). Currently, controversial research exists on the effects of HIIT post-exercise on the production of EPOC in populations living with obesity. Different high-intensity interval training modalities have different effects on producing EPOC after exercise. Different forms of HIIT research are well worth exploring22. Both WB-HIIT and JR-HIIT are fast explosive exercises performed with their own weight, involving more muscle groups. We speculate that the reason why WB-HIIT and JR-HIIT improve body composition and achieve fat loss may be due to the mobilization of multi-joint training during exercise, which promotes the body’s energy expenditure.
WB-HIIT and JR-HIIT have been conducted more frequently in adolescents and healthy adults, but there is a lack of relevant studies on adults affected by obesity. Therefore, we will explore the effects of both WB-HIIT and JR-HIIT post-training on energy expenditure, body composition, and muscle fitness in adults with obesity.
Materials and methods
Participants and study design
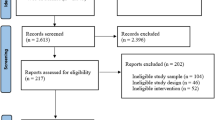
Thirty-six eligible young adults were recruited from a university, with the following inclusion criteria: (1) aged 18–30 years; (2) obesity determined by body mass index (BMI) > 24.0 kg/m223; (3) no regular PA or structured sports training within the last 6 months; (4) having a condition limiting participation to maximal physical test and training (e.g., cardiovascular or lung disease, neuromuscular or musculoskeletal disorder). Following an explanation of the purpose and constraints of the study, all participants sign the written informed consent. This trial is registered on the Chinese clinical trial registry (ChiCTR2100048737; Date of registration:15 July 2021). The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the medical ethics committee of the Department of Medicine of Shenzhen University (PN-202400005; Date of registration:7 February 2024). This study was conducted between February and July of 2024. A flowchart and study design of this study is depicted in Fig. 1.

Participants Flowchart. Abbreviations: WB-HIIT, whole-body high-intensity interval training; JR-HIIT, jump rope high-intensity interval training; CG, no-training control.
Sample size
The sample size calculation using G*Power 3.1 (Version 3.1; Dusseldorf, Germany) was based on suggested previous findings of the adaptations in fat mass to HIIT (effect size of 0.45) in obese adults24. A two-tailed power calculation at an alpha of 0.05 and a power of 0.80 suggested that a minimum of 30 participants, 10 for each group, were required in this study. Given the ~ 20% dropout rate, the sample size was inflated to 12 participants per group.
Randomization and blinding
The randomly allocated sequence was a computer, SPSS 20.0 (SPSS Inc, Chicago, IL, USA)-generated and sealed in sequentially numbered opaque envelopes. C.M. generated the random allocation sequence, Y.B.Q enrolled the participants, and Z.C.Q assigned the participants to interventions. This study is stratified by two age levels (18–24 years, 25–30 years), two genders (males and females), and two levels of BMI (24.0–25.0 kg/m2, > 25.0 kg/m2), with a total of 8 strata (2 × 2 × 2). As the participants were enrolled, we determined the stratum to which they belonged and were then separated and randomized to either WB-HIIT, JR-HIIT, or CG (after baseline testing, participants were assigned using the next envelope in the sequence). BIA and muscular fitness testers were blinded to group allocation.
Anthropometry and body composition
Participants were asked to fast 10 min before taking their anthropometry and body composition measurements, and to avoid strenuous physical training for 48 h. The standing height (in cm to the nearest 0.5 cm) was measured without shoes using a wall-mounted scale. Body mass (BM), body mass index (BMI), body fat percentage (%BF), Fat mass (FM), Muscle mass (MM), and estimated visceral adipose tissue area (VAT) were analyzed by bioelectrical impedance analysis (BIA). BIA can be a reliable tool for measuring body composition and VAT; its reliability has been widely verified. The Inbody 770 Body Composition Monitor (Biospace Co., Seoul, Korea, 2021) was used to obtain foot-to-foot BIA measures per the manufacturer’s guidelines, with participants standing barefoot on the footplates. Before the measurement, all the participants entered their gender, age, and height (cm). Furthermore, to ensure measurement accuracy, each subject was measured three times, and the average was calculated (Table 1).
Assessment of muscular strength
Hand grip measurement procedure was adapted from the standardized procedure and script for muscular strength testing by Xu25. Grip strength was measured by an adjustable spring-loaded digital hand dynamometer (EH101, CAMRY, Guangdong, China) with a resolution of 0.1 kg. In each measurement, the Knob was adjusted to the appropriate position according to the size of the participant’s hand and squeezed the handle as hard as possible for approximately 3-s; three attempts were completed for a dominant hand with 30-s resting intervals between measurements. The researcher then recorded the highest measurement26.
The back strength test was conducted using the electronic back strength meter (BCS-400, HFD Tech Co., Beijing, China). The participant stood upright on the chassis of the back strength meter with both arms and hands straight and hanging down in front of the same side of the thigh so that the handle was in contact with the tips of the two fingers and the chain length was fixed at this height27. During the test, participants straightened both legs, tilted the upper body slightly forward, about 30 degrees, straightened both arms, held the handle tightly, palms inward, and pulled upward with maximum force. Test 2 times with 1-min rest interval, and record the maximum value, in kg.
Energy metabolism measurement
EPOC was measured using a portable gas metabolic analyzer COSMED k5 (K5, Italy). First, subjects’ quiet heart rate index tests were completed using Polar heart rate bands (Polar team pro, Polar, Kempele, Finland).
Gas exchange data were assessed for 30 min post-exercise while participants remained seated alone in a quiet room. This duration was selected as preliminary data showed that VO2 returned to baseline within 30 min post-exercise. Mean VO2, HR, and VE were determined as the average value from the entire 30 min post-exercise period; in addition, VO2, and VE were estimated at 5, 15, and 30 min by taking an average of the 5 (0–5 min), 10 (5–15 min), and 15 min (15–30) of data preceding each timepoint. Mean exercise intervention assessment results include the intervention period and 30 min after the end of the intervention, excluding the warm-up component.
We chose to collect 1 VO2 and VCO2 during each period of the intervention, and the total amount of VO2 and VCO2 over a fixed period was calculated by accumulating them and substituting them into the substrate metabolism equation28:
-
①
Carbohydrate oxidation rate (mg/kg/min) = 4.5850 VCO2 (ml/kg/min) − 3.2255 VO2 (ml/kg/min).
-
②
Lipid oxidation rate (mg/kg/min) = 1.6946 VO2 (ml/min/kg) − 1.7012 VCO2 (ml/kg/min).
-
③
Lipid energy output (cal/kg/min) = lipid oxidation rate (mg/kg/min) × 9;
-
④
Total energy output (cal/kg/min) = lipid oxidation rate (mg/kg/min) × 9 + carbohydrate oxidation rate (mg/kg/min) × 4;
-
⑤
Percentage of energy from lipid = Lipid energy output/Total energy output (%).
WB-HIIT and JR-HIIT protocol
WB-HIIT and JR-HIIT performed three sessions on non-consecutive days per week for 8 weeks. Before the training session, there is a 3-min warm-up and cool-down period. The WB-HIIT content was integrated by investigators based on a previous study14 and provided to participants through four videos created by our team. Participants performed 4 sets of exercises in one session including 4 × 30-s all-out whole-body exercises interspaced with 30-s of rest and 1-min rest between each set. Each exercise was proposed with a basic (1–2 set) and advanced variant (3–4) to promote progression, and the total duration of each session was about 25-min (Table 2). Participants in the JR-HIIT group performed 4 sets of jump rope in one session; each set included 4 × 30-s exercise interspaced with 30-s rest and 1-min rest between each set. Jump rope intensity at 100 jumps/min for 1–4 weeks progressed to 110 jumps/min for 5–6 weeks and 120 jumps/min for 7–8 weeks. The cadence of jumps was controlled by recording a rhythmic MP3. All JR-HIIT sessions were monitored by personal trainers who verified adherence to the training protocol. The selected JR-HIIT protocol refers to previous research in populations with obesity19. Heart rate (HR) during training was monitored by a heart rate belt (Polar team Oh1, Polar, Kemele, Finland) and recorded the average and maximal HR (HRmax) of each session and the time spent in different intensity zones, expressed in percentage of the estimated HRmax based on age (220—age): light (60–70%), moderate (70–80%), high (> 80% HRmax) intensity (Supplementary Table S1).
Dietary and exercise control
Daily energy intake was estimated with validated 24-h dietary recalls (3 weekdays and 1 weekend day) during the initial and the end of the training program. It was carried out by all participants with the help of their parents and/or the investigators. Energy intake based on the dietary records was calculated with commercial software (Boohee Health Software, Boohee Info Technology Co., Shanghai, China), averaged, and reported as kilocalories per day (kcal/day). Subjects were asked to maintain their current diet throughout the study.
Statistical analysis
All analyses were performed using the SPSS Statistical Software Package (v20.0; SPSS Inc., Chicago, IL, USA). Distributional assumptions were verified using the Kolmogorov–Smirnov test, and non-parametric methods were utilized where appropriate. All data passed the normality and homogeneity tests. An ANOVA repeated measures test was used to compare the baseline data of the three groups and to compare changes in the different variables between groups. A two-way analysis of variance (ANOVA) with repeated measures (3 groups: WB-HIIT vs. JR-HIIT vs. CG × 2 times: pre- vs. post-intervention). A post hoc test (with Bonferroni) was applied if the main factor was significant. Partial eta squared (η2) was used as effect size to measure the main and interaction effects, which was considered small when < 0.06 and large when > 0.1429. The within-group effect size was revealed by calculating Cohen’s d. Values of d = 0.2, 0.5, and 0.8 indicate small, medium, and large effect sizes30.
Results
Of the 105 subjects who entered the run-in phase, 36 were randomized. The other 69 participants were not randomized because of not meeting inclusion criteria (n = 24), having regular exercise (n = 17), having no time to participate (n = 8), and having other comorbidities (n = 20). During the 8-week intervention period, no adverse events were reported, but seven subjects were unable to complete the training program (Fig. 1). Specifically, three subjects reported that the training was not enjoyable (WB-HIIT = 1; JR-HIIT = 2); 2 reported they had no time to continue (WB-HIIT = 2); 1 had a personal reason to quit (JR-HIIT = 1); and 1 person not participant the post-test (CG = 1). Thus, 29 participants concluded the training program (WB-HIIT: 9; JR-HIIT: 9; CG: 11).
Following the training program, Body Mass (2.6%; p < 0.01), Body Mass Index (2.6%; p < 0.01), Fat Mass (6.8%; p = 0.02), and % Body Fat (3.9%; p = 0.05) decreased, while Muscle Mass (5.5%; p < 0.01), Hand Grip (8.8%; p < 0.01) and Back Strength (23.3%; p < 0.01) increased in the WB-HIIT group. Body Mass (4.0%; p < 0.01), Body Mass Index (4.2%; p < 0.01), Fat Mass (9.9%; p < 0.01), % Body Fat (5.8%; p < 0.01), Visceral Adipose Tissue (6.4%, p = 0.02) and Muscle Mass (2.7%; p = 0.07) decreased, while Hand Grip (6.3%, p < 0.01) and Back Strength (10.6%, p = 0.01) increased in the JR-HIIT group. Participants’ descriptive variables are summarized in Table 3 and Fig. 2.
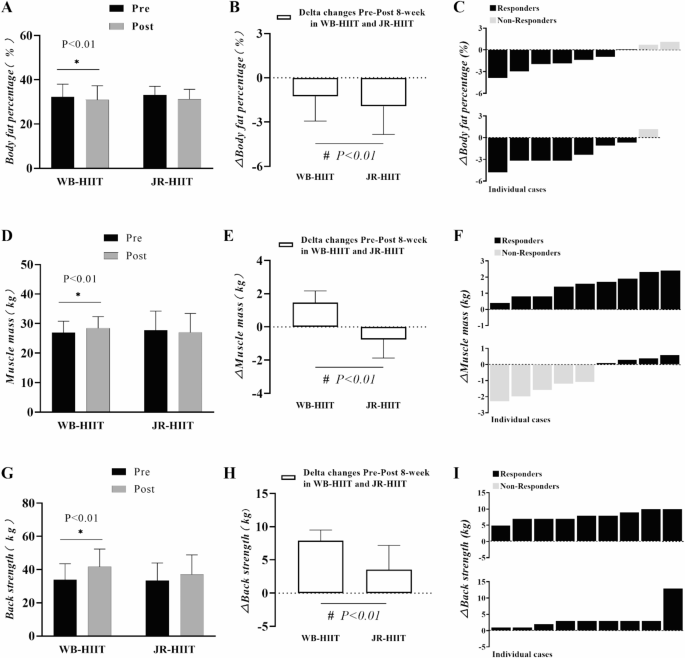
Pre-post changes (A, D, G), delta (mean) (B, E, H), and delta (individual) (C, F, I) of body fat percentage, muscle mass, and back strength in obese young adults. * Denotes significant differences pre versus post within the group at level p < 0.01; # Denotes significant differences between WB-HIIT versus JR-HIIT at level p < 0.01.
Anthropometry and body composition
Table 3 presents data and statistical analysis of body composition at baseline and post-intervention. There were no differences in body mass (p = 0.758), BMI (p = 0.205), fat mass (p = 0.782), muscle mass (p = 0.700), hand grip (p = 0.339), and back strength (p = 0.502) at baseline in the three groups.
Following the 8-week intervention, the body mass (WB-HIIT = − 1.9 kg, 95% CI: − 2.1 to − 0.9, p < 0.05; JR-HIIT = − 2.8 kg, 95% CI: − 3.9 to − 1.8, p < 0.05), BMI (WB-HIIT = − 0.7 kg/m2, 95% CI − 1.0 to − 0.3, p < 0.05; JR-HIIT = − 1.0 kg/m2, 95% CI − 1.4 to − 0.7, p < 0.05), Fat mass (WB-HIIT = − 1.5 kg, 95% CI − 2.4 to − 0.7, p < 0.05; JR-HIIT = − 2.3 kg, 95% CI − 3.2 to − 1.4, p < 0.05), and %body fat (WB-HIIT = − 1.3%, 95% CI − 2.3 to − 0.2, p < 0.05; JR-HIIT = − 1.9%, 95% CI − 3.0 to − 0.9, p < 0.05) were reduced in all intervention groups. Muscle mass (1.5 kg, 95% CI 0.8–2.1, p < 0.05) had a significant increase in WB-HIIT, while a significant decrease (− 0.8 kg, 95% CI − 1.4 to − 0.1, p < 0.05) in JR-HIIT. In comparison to the CG, body composition had significantly improved in both intervention groups. All three groups had no significant changes in visceral adipose tissue (p > 0.05).
Muscular strength
The muscular strength of hand grip (WB-HIIT = 3.3 kg, 95% CI 2.4–4.2, p < 0.05; JR-HIIT = 2.2 kg, 95% CI 1.4–3.3, p < 0.05), and back strength (WB-HIIT = 7.9 kg, 95% CI 5.0–8.4, p < 0.05; JR-HIIT = 3.6 kg, 95% CI 2.2–5.6, p < 0.05) were increased in all three groups. When compared to JR-HIIT and CG, the back strength in WB-HIIT was significantly higher (p < 0.05).
EPOC after WB-HIIT and JR-HIIT
There were no significant differences in oxygen uptake between subjects at Base, during exercise, and at rest(p > 0.05), with total EPOC being significantly higher in the WB-HIIT(6.61 ± 2.12) than in the JR-HIIT (4.73 ± 0.92, p < 0.05); EPOC/BM WB-HIIT (88.69 ± 24.04, p < 0.05) was significantly higher than JR-HIIT (64.42 ± 10.01, p < 0.05) (Table 4).
VO2 and RQ after WB-HIIT and JR-HIIT
Comparative analyses between the WB-HIIT and JR-HIIT groups showed significant differences in VO2 from 0 to 5 min after training (p < 0.05). Comparative studies between WB-HIIT and JR-HIIT groups showed substantial differences in RQ from 5 to 15 min after training (p < 0.05). Throughout the exercise intervention phases, significant differences were found in the within-group comparison analyses for the Train, 0-5min, and 5-15min phases when compared to baseline(p < 0.05) (Fig. 3).
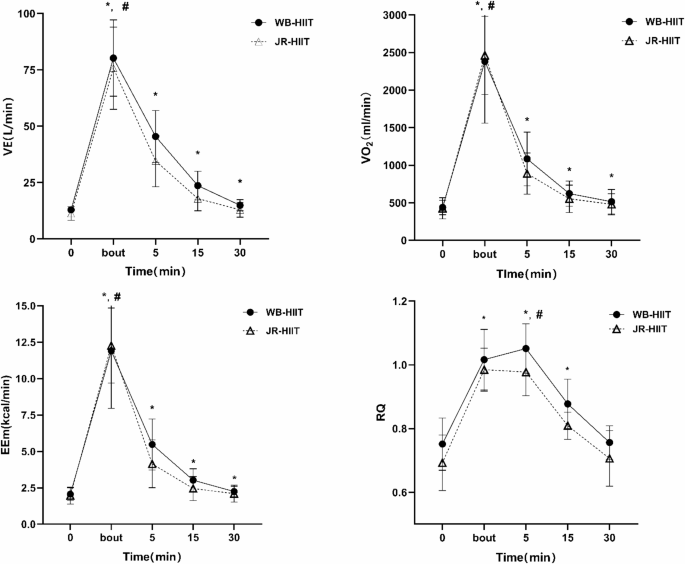
* Denotes significant differences pre versus post within the group at level p < 0.01; # Denotes significant differences between WB-HIIT versus JR-HIIT at level p < 0.01.
Ventilation and heart rate after
Comparative analyses between the WB-HIIT and JR-HIIT groups showed significant differences in VE from 0 to 5 min after training (p < 0.05). Throughout the exercise intervention phases, significant differences were found in the within-group comparison analyses for the Train, 0-5min, 5-15min, and 15-30min phases when compared to baseline (p < 0.05).
During training metabolic substrate
Analysis of glycolipid metabolism and energy output metrics in the two different groups during the intervention period revealed no significant differences in the rate of oxidation of glycolipids and energy output during the intervention period (Table 5).
After training metabolic substrate
Lipid oxidation rate was significantly higher in the WB-HIIT (2.04 ± 0.52) than in the JR-HIIT (0.95 ± 0.36, p < 0.05); lipid energy output was considerably higher in the WB-HIIT (18.32 ± 4.68) than in the JR-HIIT (8.53 ± 3.23. p < 0.05).
Carbohydrate oxidation rate was significantly higher in the JR-HIIT (7.17 ± 3.96) than in the WB-HIIT (12.13 ± 4.77, p < 0.05); The percentage of energy from lipid (%) was significantly higher in the WB-HIIT (0.4225 ± 0.15) than in the JR-HIIT (0.1588 ± 0.07, p < 0.05); There was no significant difference between the two groups in terms of total energy expenditure (Table 5).
Discussion
This study examined the effects of two HIIT modalities on body composition and muscular strength in obese adults and compared the energy metabolism characteristics (e.g. VO2, EPOC, etc.) during and after training. Essentially, results showed that similar fat loss following WB-HIIT and JR-HIIT, and muscle mass increase in WB-HIIT was greater in comparison with JR-HIIT. Moreover, whole-body high-intensity interval training leads to further improvements in muscular strength after 8 weeks of exercise training.
Similar to our findings from Scott et al. obesity-affected adults who received 1-min work intermixed with 1-min rest WB-HIIT 3 times a week for 12 weeks, with HRmax ≥ 80%, significantly reduced body weight, BMI, and fat mass16. Another study further supports these conclusions that 20 weeks of WB-HIIT effectively improves the body composition of women impacted by obesity31. JR-HIIT seemed to have a better effect on reducing fat mass (− 9.9% vs.–6.6%). This finding is consistent with prior studies reporting decreases in body mass after jumping rope in obese adolescent populations19. Increased skeletal muscle mass (5.6%) is another benefit of WB-HIIT’s improved body composition. Muscle mass helps to increase basal metabolic rate and increase energy expenditure32. Another advantage of WB-HIIT compared with traditional HIIT is that it can increase skeletal muscle content and improve strength performance, which is consistent with the results of Scoubeau14. However, Van Baak et al. found that traditional functional and sprint HIIT forms have no significant impact on muscle endurance33. This difference may be due to differences in experimental design, particularly in terms of the level of supervision (supervised versus unsupervised environment) and training load parameters. Menz et al. adds resistance exercise to its training program to increase VO2max and muscle strength in overweight or obese adults34.
Obesity has been shown to decrease skeletal muscle through young and old adulthood35. Hand grip and back strength were commonly used for muscular fitness assessment26. Resistance training (RT) is a traditional mode that improves muscular strength, hypertrophy, and other muscle fitness. However, our results suggested that both WB-HIIT and JR-HIIT can effectively increase the hand grip, which reflected the improvement of total body strength and total body muscle mass. Moreover, WB-HIIT had a better effect on back strength increase (23.3%) with obesity adults, and in line with the increase of muscle mass (1.5 kg). Although the training load is moderate (i.e., body weight), WB-HIIT involves fast concentric and eccentric contractions by upper and lower limbs, combined with the high blood lactate concentration attained during WB-HIIT, which could have triggered the slight increase in muscle mass36,37,38,39,40. Higher training intensity increases the activation level of the nervous system and the recruitment efficiency of the neuromuscular, thereby strengthening muscle fiber contraction and improving muscular strength. In addition, the activation of the stretch-activated ion channel (SAC) and the increase in protein synthesis after WB-HIIT results in an increase the muscle size and activation of muscle fiber contraction41,42. These may be the potential mechanisms for WB-HIIT to enhance muscular strength.
In this study, we analyzed the potential mechanism of fat reduction effect of WB-HIIT and JR-HIIT from the perspective of energy metabolism. It has been pointed out that the difference in EPOC after exercise may be the reason why HIIT has a higher effect on fat reduction43,44. In this study, VO2, EPOC and RQ were measured during and after exercise in subjects using a gas metabolism analyzer (K5). Consistent with the Sturdy RE et al. study reports the HIFT 14 participants’ post-exercise responses demonstrated higher (0.91–6.67 L) EPOC20. The Haltom RW et al. study reported that performing two sets of 20 repetitions of 8 full-body workouts, with intensity and intervals similar to the WB-HIIT we used, triggered ~ 10 L of EPOC within 1 h of exercise, differing in that it was carried out in healthy males, and in the non-obese group45. Jiang et al. study reported that in obese men, HIIT (4343.17 ± 1723.03 ml) delivered much higher EPOC than isocaloric MICT (3049.78 ± 1217.93 ml) after exercise, with EPOC occurring predominantly in the 0–10 min period, which is similar to the present study’s results21.
A comparison of two different forms of high-intensity interval training, WB-HIIT and JR-HIIT, revealed that WB-HIIT produced higher EPOC than JR-HIIT, and higher lipid oxidation rate and energy output after exercise than JR-HIIT, especially at 0–5 min post-exercise, with significant differences between the VO2 and VE groups, which also demonstrated that resistance deadweight training could lead to more energy expenditure after exercise. Zouhal H showed that EPOC is higher after HIIT training by molecular mechanisms and that HIIT rapidly mobilizes fast-twitch muscle fibers and uncouples mitochondrial respiration, which increases pulmonary ventilation and catecholamine levels and consequently enhances EPOC46.
Potential mechanism of EPOC to promote fat loss, EPOC is affected by exercise intensity and duration47, WB-HIIT overcomes self-weighted exercise with high intensity and short intervals, which accelerates the time of stretching-shortening of the skeletal muscle, and thus enhances the body’s energy expenditure48, and at the same time induces an increase in post-exercise EPOC, which promotes fat burning49. Previous studies have shown that physical activity causes a significant increase in resting metabolism for up to 24 h after exercise, and the body’s ability to maintain energy expenditure beyond the original state level is referred to as EPOC50, which allows the body to consume more energy after a short period of activity. Greer BK et al. have shown that the body can consume more energy after a short period of activity by performing RT and HIIT training on females with a long-term background of aerobic exercise. RT and HIIT training stimulate an increase in EPOC51; Jung WS et al. normal obese women perform interval exercise at 80% VO2max higher than the energy expenditure after low-intensity exercise52. The high-intensity mixed neuromuscular training program (DoIT) has been demonstrated to effectively mitigate cardiometabolic health risks and reduce cardiovascular disease incidence in overweight/obesity women, while simultaneously enhancing musculoskeletal health indicators in this population53,54. In the current study, the two non-traditional HIIT modalities share fundamental similarities with DoIT, employing bodyweight resistance and incorporating specifically designed training protocols tailored to meet the physiological requirements of overweight/obese individuals, thereby facilitating the development of fundamental exercise patterns and promoting physiological adaptation. The implementation of simplified, accessible, and diversified training modalities offers an optimized exercise experience for overweight/obesity populations, thereby enhancing exercise adherence and long-term compliance.
HIIT training can improve long-term hippocampus function55. Post training provides metabolic benefits through systemic adaptations (e.g., cardiovascular remodeling, enhanced mitochondrial function), regulation of inflammatory cytokines (e.g., IL-6, TNF-α) levels, and reduction of atherosclerosis risk, which may persist for a long time56,57. High compliance is the key to maintaining the effect. Studies have found that supervised group training can increase the compliance rate to more than 90%, which can better motivate subjects to actively participate in training. The combined application of HIIT and reasonable diet can produce additive effects, and giving more positive feedback to subjects is also a better maintenance strategy.
This study did not strictly control the participants’ dietary intake, which may have a potential impact on the EPOC measured by the participants. The study found that the thermal effect of the subjects’ food intake before the experiment can improve the VO2 of the body during the recovery period and affect the measurement of EPOC58. Carbohydrate and protein intake before exercise promotes enhanced glycogen synthesis and is beneficial to metabolism during exercise, thereby increasing EPOC production59. However, it was also found in other studies that under strict control of food intake, eating before exercise had no significant effect on EPOC60. Currently, the potential influence of diet on EPOC measurement may be influenced by food intake and individual differences. High proportion of fast muscle fibers is more likely to increase skeletal muscle content through training, while slow muscle fibers dominate the muscle building efficiency is lower61. The lack of dietary control is also a limitation of this study. The intensity of individual responses to testosterone, growth hormone, and insulin-like growth factor (IGF-1) directly affects the rate of protein synthesis and thus muscle performance62. At the same time, due to the influence of program design, WB-HIIT can fully activate muscles and induce structural adaptation, while JR-HIIT has a high metabolic efficiency, but it is limited by the single action and mechanical stimulation intensity, which is difficult to match the specific needs of resistance training for muscle hypertrophy.
The present study verified the feasibility of two different exercise formats that required less space and equipment costs and were suitable for the majority of the population, and also compared the energy metabolism characteristics of the two formats during and after exercise, providing a valuable reference for subsequent related studies. Some limitations are worth discussing. The calorie consumption was not equalized in the training protocol. The subjects’ diet was not strictly controlled, and the thermic effect of food ingested before the experiment might have affected the measurements of the subjects’ EPOC. We used the BIA which has the advantages of portability and low cost, and its reliability has been widely confirmed, but the stability is lacking, and we will use dual-energy X-ray absorptiometry (DXA) to improve the accuracy in subsequent studies. Additionally, the sample size was relatively small, potentially increasing the variability of the results. In the future, it is necessary to expand the sample size and prolong the intervention time to determine the long-term effects and to explore the intervention effects of different forms of HIIT on overweight and obese populations from a more in-depth mechanistic point of view and different dose–response relationship studies.
Conclusions
Despite the very low training volume, WB-HIIT and JR-HIIT protocols performed three times per week improved body composition and muscular fitness after 8-week training and thus may serve as an interesting and time-efficient exercise strategy in young adults with obesity. Hence, whole-body exercise modality seems to affect the training responses regarding muscular strength, and this improvement was due to a greater increased muscle mass. More importantly, these results reinforce the benefits of HIIT regimes that employ body weight as a training load. The Whole-body high-intensity interval training compared to other traditional forms of exercise high-intensity interval training programs increases post-exercise EPOC and EE at the same exercise intensity. These whole-body or jump rope training protocols may be performed in a variety of different settings (e.g., schools, public parks, indoors, etc.) and do not require sophisticated equipment.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight#%20. Accessed 2010. 14. 21.
Donnelly, J. E. et al. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 41, 459–471 (2009).
Jakicic, J. M. et al. Physical activity and the prevention of weight gain in adults: A systematic review. Med. Sci. Sports Exerc. 51, 1262–1269 (2019).
Bull, F. C. et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54, 1451–1462 (2020).
Reichert, F. F., Barros, A. J., Domingues, M. R. & Hallal, P. C. The role of perceived personal barriers to engagement in leisure-time physical activity. Am. J. Public Health 97, 515–519 (2007).
Newsome, A. N. M. et al. ACSM worldwide fitness trends: Future directions of the health and fitness industry. ACSM’s Health Fit. J. 28(11–25), 2024. https://doi.org/10.1249/fit.0000000000001017 (2025).
Batrakoulis, A. et al. Comparative efficacy of 5 exercise types on cardiometabolic health in overweight and obese adults: A systematic review and network meta-analysis of 81 randomized controlled trials. Circ. Cardiovasc. Qual. Outcomes 15, e008243. https://doi.org/10.1161/circoutcomes.121.008243 (2022).
Batrakoulis, A. & Fatouros, I. G. psychological adaptations to high-intensity interval training in overweight and obese adults: A topical review. Sports (Basel, Switzerland) https://doi.org/10.3390/sports10050064 (2022).
Gremeaux, V. et al. Long-term lifestyle Intervention with optimized high-intensity interval training improves body composition, cardiometabolic risk, and exercise parameters in patients with abdominal obesity. Am. J. Phys. Med. Rehabilit. 91, 941–950. https://doi.org/10.1097/PHM.0b013e3182643ce0 (2012).
Desai, M. N., Miller, W. C., Staples, B. & Bravender, T. Risk factors associated with overweight and obesity in college students. J. Am. Coll. Health 57, 109–114 (2008).
Machado, A. F., Baker, J. S., Figueira Junior, A. J. & Bocalini, D. S. High-intensity interval training using whole-body exercises: Training recommendations and methodological overview. Clin. Physiol. Funct. Imaging 39, 378–383 (2019).
Broad, A. A., Howe, G. J., McKie, G. L., Vanderheyden, L. W. & Hazell, T. J. The effects of a pre-exercise meal on postexercise metabolism following a session of sprint interval training. Appl. Physiol. Nutr. Metab. = Physiol. Appl. Nutr. Metab. 45, 411–420. https://doi.org/10.1139/apnm-2019-0510 (2020).
Schaun, G. Z., Pinto, S. S., Silva, M. R., Dolinski, D. B. & Alberton, C. L. Whole-body high-intensity interval training induce similar cardiorespiratory adaptations compared with traditional high-intensity interval training and moderate-intensity continuous training in healthy men. J. Strength Condition. Res. 32, 2730–2742 (2018).
Scoubeau, C., Carpentier, J., Baudry, S., Faoro, V. & Klass, M. Body composition, cardiorespiratory fitness, and neuromuscular adaptations induced by a home-based whole-body high intensity interval training. J. Exerc. Sci. Fit. 21, 226–236 (2023).
Scott, S. N. et al. Home-hit improves muscle capillarisation and eNOS/NAD(P)Hoxidase protein ratio in obese individuals with elevated cardiovascular disease risk. J. Physiol. 597, 4203–4225 (2019).
Poon, E. T., Chan, K. W., Wongpipit, W., Sun, F. & Wong, S. H. Acute physiological and perceptual responses to whole-body high-intensity interval training compared with equipment-based interval and continuous training. J. Sports Sci. Med. 22, 532–540 (2023).
Tomeleri, C. M. et al. Resistance training improves inflammatory level, lipid and glycemic profiles in obese older women: A randomized controlled trial. Exp. Gerontol. 84, 80–87 (2016).
Kim, E. S. et al. Improved insulin sensitivity and adiponectin level after exercise training in obese Korean youth. Obesity 15, 3023–3030 (2007).
Eskandari, M. et al. Effects of interval jump rope exercise combined with dark chocolate supplementation on inflammatory adipokine, cytokine concentrations, and body composition in obese adolescent boys. Nutrients 12, 3011 (2020).
Sturdy, R. E. & Astorino, T. A. Post-exercise metabolic response to kettlebell complexes versus high intensity functional training. Eur. J. Appl. Physiol. https://doi.org/10.1007/s00421-024-05579-z (2024).
Jiang, L., Zhang, Y., Wang, Z. & Wang, Y. Acute interval running induces greater excess post-exercise oxygen consumption and lipid oxidation than isocaloric continuous running in men with obesity. Sci. Rep. 14, 9178 (2024).
Moniz, S. C., Islam, H. & Hazell, T. J. Mechanistic and methodological perspectives on the impact of intense interval training on post-exercise metabolism. Scand. J. Med. Sci. Sports 30, 638–651 (2020).
Chen, C. & Lu, F. C. Department of Disease Control Ministry of Health, P. R. C. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed. Environ. Sci. Suppl. 17, 1–36 (2004).
Zhang, H. et al. Comparable effects of high-intensity interval training and prolonged continuous exercise training on abdominal visceral fat reduction in obese young women. J. Diab. Res. 2017, 5071740 (2017).
Xu, T. et al. Hand grip strength should be normalized by weight not height for eliminating the influence of individual differences: Findings from a cross-sectional study of 1511 healthy undergraduates. Front. Nutr. 9, 1063939 (2022).
Lockie, R. G. et al. Waist circumference and waist-to-hip ratio in law enforcement agency recruits: Relationship to performance in physical fitness tests. J. Strength Condition. Res. 34, 1666–1675 (2020).
Zemkova, E., Poor, O. & Pecho, J. peak rate of force development and isometric maximum strength of back muscles are associated with power performance during load-lifting tasks. Am. J. Mens Health 13, 1557988319828622 (2019).
Sindorf, M. A. G. et al. Excess post-exercise oxygen consumption and substrate oxidation following high-intensity interval training: effects of recovery manipulation. Int. J. Exerc. Sci. 14, 1151–1165 (2021).
Levine, T. R. & Hullett, C. R. Eta squared, partial eta squared, and misreporting of effect size in communication research. Hum. Commun. Res. 28, 612–625. https://doi.org/10.1111/j.1468-2958.2002.tb00828.x (2002).
Muller, K. Statistical power analysis for the behavioral sciences. Technometrics 31, 499–500 (1989).
Batrakoulis, A. et al. High intensity, circuit-type integrated neuromuscular training alters energy balance and reduces body mass and fat in obese women: A 10-month training-detraining randomized controlled trial. PLoS ONE 13, e0202390 (2018).
Zurlo, F., Larson, K., Bogardus, C. & Ravussin, E. Skeletal muscle metabolism is a major determinant of resting energy expenditure. J. Clin. Invest. 86, 1423–1427 (1990).
van Baak, M. A. et al. Effect of different types of regular exercise on physical fitness in adults with overweight or obesity: Systematic review and meta-analyses. Obes. Rev.: Off. J. Int. Assoc. Study Obes. 22(Suppl 4), e13239. https://doi.org/10.1111/obr.13239 (2021).
Menz, V. et al. Functional versus running low-volume high-intensity interval training: Effects on VO(2)max and muscular endurance. J. Sports Sci. Med. 18, 497–504 (2019).
Maffiuletti, N. A. et al. Differences in quadriceps muscle strength and fatigue between lean and obese subjects. Eur. J. Appl. Physiol. 101, 51–59 (2007).
Duchateau, J., Stragier, S., Baudry, S. & Carpentier, A. Strength training. In search of optimal strategies to maximize neuromuscular performance. Exerc. Sport Sci. Rev. 49, 2–14 (2021).
Arntz, F. et al. Effect of plyometric jump training on skeletal muscle hypertrophy in healthy individuals: A systematic review with multilevel meta-analysis. Front. Physiol. 13, 888464 (2022).
Claflin, D. R. et al. Effects of high- and low-velocity resistance training on the contractile properties of skeletal muscle fibers from young and older humans. J. Appl. Physiol. 1985(111), 1021–1030 (2011).
Carvalho, L. et al. Muscle hypertrophy and strength gains after resistance training with different volume-matched loads: A systematic review and meta-analysis. Appl. PhysiolNutr. Metab. 47, 357–368 (2022).
Bellissimo, G. F. et al. The acute physiological and perceptual responses between bodyweight and treadmill running high-intensity interval exercises. Front. Physiol. 13, 824154 (2022).
Stary, C. M. & Hogan, M. C. Cytosolic calcium transients are a determinant of contraction-induced HSP72 transcription in single skeletal muscle fibers. J. Appl. Physiol. 1985(120), 1260–1266 (2016).
Hansen, C. G., Ng, Y. L., Lam, W. L., Plouffe, S. W. & Guan, K. L. The Hippo pathway effectors YAP and TAZ promote cell growth by modulating amino acid signaling to mTORC1. Cell Res. 25, 1299–1313 (2015).
Børsheim, E. & Bahr, R. Effect of exercise intensity, duration and mode on post-exercise oxygen consumption. Sports Med. 33, 1037–1060 (2003).
Hazell, T. J., Olver, T. D., Hamilton, C. D. & Lemon, P. W. R. Two minutes of sprint-interval exercise elicits 24-hr oxygen consumption similar to that of 30 min of continuous endurance exercise. Int. J. Sport Nutr. Exerc. Metab. 22, 276–283 (2012).
Haltom, R. W. et al. Circuit weight training and it s effects on excess postexercise oxygen consumption. Med. Sci. Sports Exerc. 31 (1999).
Zouhal, H., Jacob, C., Delamarche, P. & Gratas-Delamarche, A. Catecholamines and the effects of exercise, training and gender. Sports Med. 38, 401–423 (2008).
Scoubeau, C., Bonnechere, B., Cnop, M., Faoro, V. & Klass, M. Effectiveness of whole-body high-intensity interval training on health-related fitness: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 19, 9559 (2022).
Callahan, M. J., Parr, E. B., Hawley, J. A. & Camera, D. M. Can high-intensity interval training promote skeletal muscle anabolism?. Sports Med. 51, 405–421 (2021).
LaForgia, J., Withers, R. & Gore, C. Effects of exercise intensity and duration on the excess post-exercise oxygen consumption. J. Sports Sci. 24, 1247–1264 (2007).
Gaesser, G. A. & Brooks, G. A. Metabolic bases of excess post-exercise oxygen consumption: A review. Med. Sci. Sports Exerc. 16, 29–43 (1984).
Greer, B. K., O’Brien, J., Hornbuckle, L. M. & Panton, L. B. EPOC comparison between resistance training and high-intensity interval training in aerobically fit women. Int. J. Exerc. Sci. 14, 1027–1035 (2021).
Jung, W. S., Hwang, H., Kim, J., Park, H. Y. & Lim, K. Comparison of excess post-exercise oxygen consumption of different exercises in normal weight obesity women. J. Exerc. Nutrit. Biochem. 23, 22–27 (2019).
Batrakoulis, A. et al. Hybrid-type, multicomponent interval training upregulates musculoskeletal fitness of adults with overweight and obesity in a volume-dependent manner: A 1-year dose-response randomised controlled trial. Eur. J. Sport Sci. 23, 432–443. https://doi.org/10.1080/17461391.2021.2025434 (2023).
Batrakoulis, A. et al. High-intensity interval neuromuscular training promotes exercise behavioral regulation, adherence and weight loss in inactive obese women. Eur. J. Sport Sci. 20, 783–792. https://doi.org/10.1080/17461391.2019.1663270 (2020).
Blackmore, D. G. et al. Long-term improvement in hippocampal-dependent learning ability in healthy, aged individuals following high intensity interval training. Aging Dis. https://doi.org/10.14336/ad.2024.0642 (2024).
Hawley, J. A., Hargreaves, M., Joyner, M. J. & Zierath, J. R. Integrative biology of exercise. Cell 159, 738–749. https://doi.org/10.1016/j.cell.2014.10.029 (2014).
Batacan, R. B. Jr., Duncan, M. J., Dalbo, V. J., Tucker, P. S. & Fenning, A. S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 51, 494–503. https://doi.org/10.1136/bjsports-2015-095841 (2017).
Tsuji, K., Xu, Y., Liu, X. & Tabata, I. Effects of short-lasting supramaximal-intensity exercise on diet-induced increase in oxygen uptake. Physiol. Rep. https://doi.org/10.14814/phy2.13506 (2017).
Ormsbee, M. J., Bach, C. W. & Baur, D. A. Pre-exercise nutrition: the role of macronutrients, modified starches and supplements on metabolism and endurance performance. Nutrients 6, 1782–1808. https://doi.org/10.3390/nu6051782 (2014).
Broad, A. A., Howe, G. J., McKie, G. L., Vanderheyden, L. W. & Hazell, T. J. The effects of a pre-exercise meal on postexercise metabolism following a session of sprint interval training. Appl. Physiol. Nutrit. Metab. = Physiol. Appliquee Nutrit. Metab. 45, 411–420. https://doi.org/10.1139/apnm-2019-0510 (2020).
Aagaard, P. et al. A mechanism for increased contractile strength of human pennate muscle in response to strength training: Changes in muscle architecture. J. Physiol. 534, 613–623. https://doi.org/10.1111/j.1469-7793.2001.t01-1-00613.x (2001).
Van Every, D. W., D’Souza, A. C. & Phillips, S. M. Hormones, hypertrophy, and hype: An evidence-guided primer on endogenous endocrine influences on exercise-induced muscle hypertrophy. Exerc. Sport Sci. Rev. 52, 117–125. https://doi.org/10.1249/jes.0000000000000346 (2024).
Acknowledgements
Thanks to the School of Physical Education of Shenzhen University and the relevant participants for their support. This study was funded by the Science and Technology Innovation Project of the General Administration of Sport of China (ID: 22KICX035).
Author information
Authors and Affiliations
Contributions
YBQ:Data curation, Formal Analysis, Writing–review and editing, Methodology, Visualization, Writing–original draft. CM: Conceptualization, Data curation, Writing–review and editing, Funding acquisition, Supervision, Visualization, Writing–original draft. ZCQ: Formal Analysis, Supervision, Writing–review and editing. WXD: Investigation, Methodology, Writing–review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
BaiQuan, Y., Meng, C., Congqing, Z. et al. The effects and post-exercise energy metabolism characteristics of different high-intensity interval training in obese adults. Sci Rep 15, 13770 (2025). https://doi.org/10.1038/s41598-025-98590-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-98590-z
