
Abstract
Raising a child with developmental disabilities (DDs) involves both rewards and challenges, with family management styles influencing the quality of life (QoL) of both children and families, particularly during crises. This study identified family management styles and their relationships with the QoL of children and adolescents and family functioning during the COVID-19 pandemic. Conducted between September 2020 and October 2021, the study included 200 Korean parents of individuals with DDs under the age of 21. Online data collection assessed family management styles, family functioning, and children’s QoL. Cluster analysis and analysis of variance were used to identify family management styles and to compare demographics, family functioning, and QoL across groups, respectively. Three clusters were identified: “Thriving” (n = 20), “Somewhat Resilient” (n = 118), and “Struggling” (n = 62). The Thriving cluster demonstrated effective condition management, a positive outlook, and high parental cooperation. The Somewhat Resilient cluster displayed moderate functioning. The Struggling cluster demonstrated the greatest challenges and the lowest capacity for managing the condition. Significant differences in children’s QoL, family functioning, and demographic variables were observed across clusters. These findings highlight how families manage DDs during the pandemic and the need for tailored interventions based on family management styles.
Similar content being viewed by others

Introduction
Developmental disabilities, such as autism spectrum disorder and intellectual disabilities, are long-term conditions that affect an individual’s cognitive, physical, psychological, language, or self-care abilities; affected individuals often require ongoing care, support, or assistance throughout their lives1. A previous report has indicated that approximately 240 million children worldwide have developmental disabilities1, with further evidence indicating that this number is increasing2,3.
Family plays a pivotal role in ensuring the health and optimal development of a child with developmental disabilities by performing complex caregiving tasks throughout the child’s life4 Researchers have identified that families of children and adolescents with chronic conditions have unique management styles5,6,7 Knafl and Deatrick5 state that family management style is shaped by how a family perceives, evaluates, and manages the consequences of a child’s condition. These styles significantly impact various aspects of the quality of life of children and adolescents and family functioning5,6,8. Given that individuals with developmental disabilities often reside with their parents for an extended period9, rather than living independently, the importance of family management styles becomes even more pronounced.
Quality of life is a multidimensional concept encompassing the core domains including emotional, physical, and material well-being, personal development, self-determination, interpersonal relations, social inclusion, and rights, which are especially crucial for individuals with developmental disabilities10. Studies suggest the relationships among family management styles and various domains of quality of life in children with chronic conditions as well as overall family functioning6,8,11,12,13.
Knafl et al.8 identified four family management styles among 414 families of children with various chronic conditions (e.g., diabetes, cystic fibrosis, arthritis) and examined relationships between these styles and certain aspects of children’s quality of life. The investigators determined four family management styles using the k-means clustering analysis method: family-focused, somewhat family-focused, condition-focused, and somewhat condition-focused. Families with a family-focused style effectively integrated the tasks of managing the child’s condition into their daily family schedule, minimizing their impact on both the family and the child. By contrast, families with a condition-focused pattern demonstrated that managing the child’s condition required substantial exertion and influenced their day-to-day family routine8.
The authors also found the family-focused style as the most favorable family management style, with children in these families exhibiting the lowest levels of behavioral problems associated with the emotional well-being domain and the highest ability to perform age-appropriate roles associated with the personal development domain of quality of life, compared to the other three family management types. Furthermore, families with family-focused styles exhibited better family functioning than those with condition-focused styles8.
Deatrick6 identified four distinct family management styles among families of adolescent survivors of childhood brain tumors. Adolescents from families exhibiting the most positively regarded family management style demonstrated the highest scores in physical and emotional well-being compared to those from families with other styles. Family functioning was also found to be strongest in families exhibiting this favorable management style.
Similarly, family management styles among 277 parents of children with chronic diseases were shown to influence the psychosocial challenges11 while those among 93 families of children with epilepsy were associated with the children’s quality of life12. Additionally, Im and Jung13 observed four family management styles (stable-resilient, less committed, parents’ mission, and challenging management) and associations between these styles and family functioning among 146 families of children with atopic diseases in South Korea. The styles varied from “stable-resilient,” where child management was integrated into daily life with confidence and effective parental interaction, to “less committed,” with limited involvement and low cooperation. Additionally, “parents’ mission” reflected a joint commitment as a core parenting duty, while “challenging” indicated significant barriers and disrupted management integration.
Considering the effects of the varying responses of families raising children and adolescents with chronic conditions on the child and family functioning, healthcare providers should acquire an in-depth understanding of how these families integrate the management of a child’s condition into their daily lives. Especially, exploring family management from a typology perspective is indispensable. Typologies provide an integrated view of the complex dynamics of family life and enhance understanding of the relationships between subgroup variables and other factors, making them particularly valuable for studying family management styles in caregiving for children with chronic conditions including developmental disabilities8. This could enable healthcare providers to deliver tailored interventions that target specific family styles. Furthermore, an in-depth understanding of family management styles can enhance societal awareness about the unique caregiving demands of families8. This understanding can foster community support and alleviate the stigma associated with families raising children with developmental disabilities.
Nevertheless, to date, no study has examined the shared traits and distinctions in how families manage the condition of their children with developmental disabilities. Such chronic conditions exert a long-lasting impact on families, who are likely to encounter distinct experiences and exhibit varied management styles compared to families of children with chronic medical conditions, such as diabetes and atopic diseases, but without intellectual disabilities.
Moreover, management among families of children with developmental disabilities during crisis situations such as COVID-19 warrants increased attention. The pandemic has further intensified family challenges, as restrictions on healthcare access, social services, and educational support have disrupted family routines and caregiving structures14. Families of children with developmental disabilities have faced heightened stress, limited external support, and greater caregiving burdens, making effective family management even more critical15. Given the escalating difficulties these families have encountered during the COVID-19 pandemic, understanding the complexities of family management styles is more crucial than ever. Moreover, experts project a significant probability of recurring global crises akin to COVID-19 in the future16. Consequently, advancing a comprehensive understanding of family experiences during the pandemic is imperative for providing information on future crisis preparedness and intervention strategies.
Investigating these relationships can offer invaluable insights into the complex intersection of the children’s and adolescents’ condition, family management, and the quality of life of children and adolescents and family functioning in families of children and adolescents with developmental disabilities. This study examined family management styles in families of children and adolescents with developmental disabilities and the quality of life of children and adolescents and family functioning according to the identified styles during the COVID-19 pandemic. This study focused on addressing the following research questions:
-
(1)
How can families of children and adolescents with developmental disabilities be categorized based on their family management styles during the pandemic?
-
(2)
What are the key characteristics of the groups identified based on family management styles during the pandemic?
-
(3)
Do the quality of life of children and adolescents and family functioning differ across the family management styles identified in this study during the pandemic?
Methods
Study design and participants
The current study represents the second phase of a research project led by the first author, investigating family management among Korean families of children and adolescents with developmental disabilities during the COVID-19 pandemic. The first phase examined the influence of contextual factors on family management within this population during the pandemic (Under review). This online cross-sectional study was conducted in South Korea between September 2020 and October 2021. Eligible participants included parents who had access to the Internet and lived with their children diagnosed with developmental disabilities aged 4–21 years.
Measurements
Demographics
We assessed parent and child demographics, comprising age, sex, parental education, religion, family income, and types of developmental disabilities. Family income was divided into “more than 5,500,000 KRW” and “less than 5,500,000 KRW,” aligning with the average monthly household income in Korea (KRW, South Korean won)17. Child diagnosis was classified as either “autism spectrum disorder” or “other developmental disabilities” (e.g., attention-deficit/hyperactivity disorder, cerebral palsy, down syndrome), recognizing that families of children with autism spectrum disorder face more difficulties than those of children with other types of developmental disabilities18.
Family management styles
Family management styles were measured using the Korean version19 of the Family Management Measure (Korean FaMM)20. The Korean FaMM comprises 53 items across six subscales, with each item assessed on a five-point Likert scale. Families scoring higher in the Daily Life, Condition Management Ability, and Parental Mutuality domains experience less difficulty managing children with chronic illnesses. Conversely, those with higher scores in the Condition Management Effort, View of Condition Impact, and Family Life Difficulty domains face greater challenges in managing such children. Cronbach’s alpha for this measure ranged from 0.72 to 0.91 in Knafl et al.’s20 study and from 0.43 to 0.87 in this study. In the final analysis, we excluded two subscales that demonstrated lower reliability: Condition Management Effort (0.50) and View of Condition Impact (0.43).
Family functioning
To assess family functioning, we employed the Korean version of the General Functioning Scale of the Family Assessment Device, as adapted by Lee21, and originally developed by Epstein et al.22 The scale comprises 12 items rated on a four-point Likert scale. Scoring involved converting reverse-scored items; lower scores indicate pathological family functioning, and higher scores denote healthier family functioning. Cronbach’s alpha for this scale was 0.81 in Lee’s21 study and 0.86 in this study.
Quality of life of children and adolescents
The KidsLife scale23 was utilized to assess the quality of life of children and adolescents. This instrument was developed based on Schalock et al.’s10 conceptualization of quality of life in individuals with intellectual disabilities and consists of 96 items across eight domains: Personal Development, Emotional Well-being, Physical Well-being, Material Well-being, Self-Determination, Interpersonal Relations, Social Inclusion, and Rights. Each item is evaluated using a four-point Likert scale. The aggregate raw score on each domain is normalized to a standard score, accounting for the child’s age. Elevated scores indicate a higher quality of life.
The investigators adhered to the translation methodology outlined by Sousa and Rojjanasrirat24 to adapt the measurement tool to the Korean language. Before this, permission was obtained from the author of the KidsLife instrument for its use. Subsequently, the items were translated and back-translated. To establish the content validity of the KidsLife questionnaire, an expert panel of 11 members—including doctors, nursing professors, nurses, special educators, and parents involved in the care of children with developmental disabilities—was convened. The content validity index at the item level for all 96 items exceeded 0.80, indicating satisfactory validity25,26. Cronbach’s alpha for the KidsLife scale was reported to range from 0.78 to 0.91 among children with autism spectrum disorder27. In the current study, Cronbach’s alpha was 0.84–0.91.
Data analysis
The data were analyzed using IBM SPSS Statistics, version 26, and R, version 4.3.2 software (SPSS Inc., Chicago, IL, USA). A k-means clustering analysis was utilized to classify family groups according to the four subscales of the Korean FaMM in that this statistical method is appropriate for person-oriented analyses involving continuous data and relatively small sample sizes28,29. This method segregates cases into k clusters, aiming to maximize inter-cluster disparities and minimize intra-cluster variance, as per specified variables30. Two specific approaches were adopted for the k-means cluster analysis: hierarchical clustering and the elbow method. Hierarchical clustering involved Ward’s linkage method and Euclidean distance, along with the construction of a dendrogram. Concurrently, the elbow method was employed to validate the number of clusters. The elbow method was particularly chosen since it identifies the point at which a cluster set explains most of the data variance31. This involved examining the within-group sum of squares relative to the cluster count (Fig. 1).

Elbow plot according to the number of clusters.
A one-way analysis of variance (ANOVA) and Bonferroni test were employed for post-hoc analysis and to compare demographic characteristics, family functioning, and children’s quality of life across the clusters. For categorical variables, the chi-square (χ2) test or Fisher’s exact test was performed, and the Bonferroni corrected p-value was calculated for post-hoc analysis. Post-hoc power analyses, based on observed effect sizes (η² = 0.15–0.71) from the one-way ANOVA F test, confirmed that a sample size of n = 200 generated sufficient statistical power (1 − β > 0.8) to reliably detect medium-to-large effect sizes32.
Ethical considerations
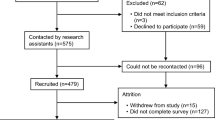
The procedure for data collection followed the ethical standards outlined in the Declaration of Helsinki. This study was approved by Korea University Institutional Review Board (KUIRB-2020-0322-01). Data were collected after obtaining institutional review board approval. The research team approached a representative from the National Center for Disabled Children and Developmental Disabilities, as well as gatekeepers from over 30 Korean support groups for children and adolescents with developmental disabilities, to obtain permission to post research flyers on their websites. These flyers contained a link to an online survey hosted on SurveyMonkey and included details regarding the study’s aims, criteria for participation, and ethical considerations. Interested parents of children and adolescents with developmental disabilities could access the survey online, which comprised a consent form and a self-report questionnaire. Informed consent was obtained from all subjects. To ensure the reliability and ethical integrity of the study, several procedures were conducted to ascertain any fraudulent responses. Suspicious responses were flagged and verified according to specific criteria such as if the respondent’s completion speed was too quick, and if the answer to other questions was the same. Additionally, IP addresses were cross-verified to prevent multiple submissions from the same user. The participants were given a mobile coupon gift valued at 10,000 KRW upon their completion of the questionnaire.
Results
Sample characteristics
The participants were 200 Korean parents, of whom a significant majority were mothers (92.0%), and all were married. Children and adolescents with developmental disabilities had an average age of 11.17 years (standard deviation [SD] = 4.23), with boys comprising a larger proportion (67.0%) than girls (Table 1). Considering all diagnoses of children and adolescents, the most common diagnosis among them was autism spectrum disorder, accounting for 58% of the cases, followed by intellectual disability (35%).
Cluster analysis results
Figure 1 presents the elbow plot. The ideal cluster number, ascertained through dendrogram analysis and clustering coefficient evaluation, was three. Thus, family management styles were categorized into three distinct groups via k-means clustering methods. In other words, three family management styles were identified among families of children and adolescents with developmental disabilities during the COVID-19 pandemic.
Cluster 1: Thriving
Of the 200 participants, 20 (10%) were grouped in Cluster 1, exhibiting the highest mean scores in the domains of Condition Management Ability (mean = 47.40, SD = 5.57) and Parental Mutuality (mean = 34.45, SD = 5.95) compared with the other two clusters (Table 2; Fig. 2). These scores suggest that the parents perceived themselves as being capable of managing their child’s condition and were satisfied with their collaboration with their partner in managing the child’s condition. However, the Family Life Difficulty domain, indicating the difficulty that having a child with developmental disabilities poses to family life, exhibited the lowest mean score in Cluster 1 (mean = 34.60, SD = 6.93). Considering that this group is characterized by the maximizing of positive aspects and minimizing of negative aspects of family management, Cluster 1 was designated as “Thriving”.

Cluster visualization for the four subscales of the Family Management Measure.
Cluster 2: Somewhat resilient
A total of 118 participants (59%) were assigned to Cluster 2, which exhibited the highest scores in the Child’s Daily Life domain (mean = 13.48, SD = 3.00), suggesting a more positive perception of their children’s experiences. The mean scores for Condition Management Ability (mean = 39.05, SD = 4.53), Parental Mutuality (mean = 24.47, SD = 3.90), and Family Life Difficulty (mean = 45.21, SD = 4.74) in Cluster 2 were intermediate, falling between those of Clusters 1 and 3. Consequently, Cluster 2 was termed “Somewhat Resilient.”
Cluster 3: Struggling
Cluster 3, including 62 participants (31%), recorded the highest average score for Family Life Difficulty (mean = 59.37, SD = 5.13) and the lowest mean scores on the other domains: Child’s Daily Life (mean = 7.71, SD = 2.27), Condition Management Ability (mean = 31.31, SD = 6.06), and Parental Mutuality (mean = 22.63, SD = 6.78). Given the pronounced negative features and the relative paucity of positive aspects in family management observed within this group, Cluster 3 was named “Struggling.”
Differences in demographic characteristics across clusters
Table 1 illustrates the demographic differences among the three clusters. Cluster 1 demonstrated the highest mean parental age at 44.2 years (SD = 4.96) with statistical differences observed among the clusters (F = 5.513, p < 0.005). Significant differences were also found in education level and religion (Education: χ2 = 15.530, p < 0.001; Religion: χ2 = 7.095, p = 0.029). There was a difference in family income among the clusters (χ2 = 6.290, p = 0.043).
Regarding child age, Cluster 1 had the highest mean age of 13.35 years (SD = 5.19), and the clusters exhibited significant differences (F = 13.892, p < 0.001). Cluster 3 households showed the highest percentage of children with autism (66.1%) among the clusters (χ2 = 10.707, p = 0.005). Gender differences in both parents and children were not observed across clusters.
Differences in family functioning across clusters
The mean family functioning score for all participants was 33.41 (SD = 5.88), and the differences among the clusters were statistically significant (F = 19.21, p < 0.001) (Table 3). Post-hoc analysis showed that Cluster 1’s mean score was the highest (mean = 40.45, SD = 5.37), with Clusters 2 (mean = 32.86, SD = 4.87) and 3 (mean = 32.16, SD = 6.33) having statistically similar means.
Differences in children’s quality of life across clusters
The mean score for children’s overall quality of life across the sample was 59.11 (SD = 20.51), with significant differences observed among the three clusters (F = 22.02, p < 0.001) (Table 3). Subsequent post-hoc tests demonstrated that Cluster 1 showed the highest mean score for children’s overall quality of life (mean = 80.50, SD = 16.00), followed by Clusters 2 (mean = 60.60, SD = 17.10) and 3 (mean = 49.37, SD = 21.93).
For all subscales of the children’s quality of life instrument, except for Physical Well-being, notable differences were observed among the clusters. Cluster 1 had the highest mean scores across the six subscales: Social Inclusion, Emotional Well-being, Material Well-being, Rights, Personal Development, and Interpersonal Relationships, compared with the other two clusters. For four subscales—Social Inclusion, Self-Determination, Personal Development, and Interpersonal Relationships—the mean score of Cluster 2 exceeded that of Cluster 3.
Discussion
This study enhances our understanding of family management styles in families of children and adolescents with developmental disabilities, particularly during the COVID-19 pandemic. We identified three distinct family management styles: Thriving, Somewhat Resilient, and Struggling. Furthermore, this study confirmed the significant relationship between family management styles and children’s and adolescents’ quality of life and family functioning.
Families exhibiting the Thriving style displayed an exceptional ability to manage their children’s conditions and maintain a positive outlook toward their children with developmental disabilities; moreover, they showed greater cohesive support, aligned perspectives, and satisfaction in managing their child’s condition compared with the other two family styles. Additionally, these families recorded the lowest scores on the Family Life Difficulty domain, suggesting a minimal impact of the child’s condition on their daily lives. Consequently, families in the Thriving cluster do not perceive managing a child with a developmental disability as an overwhelming challenge and have integrated this management into their daily routines. This style is similar to the family-focused one described in previous research, which highlights families’ proficient management of their child’s condition with minimal disruption to their family life8.
Moreover, the Thriving cluster demonstrated the highest levels of family functioning with all aspects of quality of life in children and adolescents with developmental disabilities surpassing the other two styles. These findings align with previous studies that have identified positive correlations between ease of family management and health-related quality of life or family functioning among various groups, including families of adolescent survivors of childhood brain tumors10 and children with atopic diseases13.
Additionally, we found that parents in the Thriving cluster reported having a religion compared to other clusters. Studies of families of children with developmental disabilities have found that religion has a positive impact on families regardless of ethnicity or race33,34,35. This is a salient family characteristic for healthcare providers to consider when approaching these families.
Alongside crucial demographic characteristics that influence family management styles, it is imperative to consider social crises like the COVID-19 pandemic when assessing family functioning among families of children with developmental disabilities. Researchers have recommended adopting a normality perspective to improve the quality of life of children and families dealing with chronic illnesses and disabilities36. During the COVID-19 pandemic, maintaining a sense of normality has become crucial for families of children with developmental disabilities because of the considerable disruptions in family dynamics. The mandatory home isolation regulations interrupted direct healthcare services and created challenges in addressing the health, social, and educational needs of children with developmental disabilities14,37. As in other countries, the closure of daily programs and social services in Korea intensified these families’ challenges37,38. Additionally, the pandemic has caused widespread financial strain, particularly affecting these families owing to inadequate healthcare and education and impacting their employment and financial stability14.
Research comparing pre- and post-pandemic conditions among families of children with developmental disabilities has corroborated the detrimental effects of the pandemic. In this study, the FaMM scores were lower than those documented in van Riper et al.’s39 pre-pandemic investigation of Korean families of children diagnosed with down syndrome. This discrepancy suggests a potential negative impact of the COVID-19 pandemic on family management dynamics.
Although families of children and adolescents with developmental disabilities faced difficulties during the pandemic14,15,40, positive family management abilities, such as condition management skills—which scored highest among those in the Thriving cluster—may have helped mitigate these difficulties. However, our study has found that only a few families (n = 20, 10%) are categorized in this cluster. Conversely, the Struggling cluster, characterized by less favorable perspectives toward the child and limited family capabilities in managing the child’s condition, was more prevalent, with three times more families as in the Thriving cluster. These families exhibited the highest levels of family difficulties and discordance between parents in managing the affected children and the lowest levels of child and family quality of life among the three clusters. This finding is consistent with Knafl et al.’s8 condition-focused style, where an emphasis on the child’s condition necessitates substantial exertion, significantly disrupts family routines, and is associated with lower family functionality.
The current results highlight differences in parents’ educational levels among the three clusters, with the Struggling cluster exhibiting higher education levels compared to the other groups. Studies show mixed findings regarding the relationship between parents’ education levels and family functioning among families of children with developmental disabilities. For instance, Hsiao41 and Nikolić et al.42 reported significant relationships between higher parental education levels and better family functioning among families of children with autism spectrum disorder and intellectual disabilities, respectively. However, Salomone et al.43 revealed an association between higher education levels of caregivers of children with autism spectrum disorder and their mental health difficulties. Parents with higher levels of education may hold elevated expectations for their children with developmental disabilities44, which, if unmet, could contribute to more critical perceptions of their child and family functioning. Additionally, most children in the Struggling cluster were diagnosed with autism spectrum disorder compared to the Thriving cluster. Families of children with autism spectrum disorder face more difficulties than those with other types of disabilities18. Healthcare providers should consider how family and child characteristics influence the formation of family management styles.
The families in the Struggling cluster require critical support from healthcare providers to enhance their capabilities and the parents’ positive perception of the child’s condition. Furthermore, healthcare providers must devise interventions aimed at assisting families in prioritizing their routines without becoming overly preoccupied with the child’s condition.
Finally, the Somewhat Resilient cluster comprised the most number of families in this study (n = 118), with their scores on the Korean FaMM scale and the child and family outcomes falling between those of the Thriving and Struggling clusters. That is, although they demonstrated more positive family management compared with those in the Struggling cluster, their management was less favorable than that observed in the Thriving cluster. The families in this cluster are potentially moving toward either the Thriving or Struggling cluster. To guide such families toward the Thriving style, healthcare professionals should assist in preserving positive aspects of family management, including parents’ acceptance of their child’s condition, their self-management ability, and strong family cooperation.
Furthermore, the finding that the Somewhat Resilient cluster featured younger parental and child ages suggests a potential for this group to exhibit adaptive tendencies akin to either the Thriving or Struggling clusters. Considering the role of early interventions in fostering long-term stable family competency45, healthcare professionals are advised to prioritize support for young families.
Considering the multitude of contemporary societal challenges, notably the COVID-19 pandemic, as well as the frequently highlighted increased vulnerability of families of children who have developmental disabilities46, the provision of support to these families is becoming increasingly important.
Implications for families
Families of children and adolescents with developmental disabilities can strengthen their functioning by integrating their child’s condition into daily routines and utilizing community or religious support, which may be particularly beneficial in overcoming pandemic-related challenges. During crises such as the pandemic, families within the Somewhat Resilient cluster should strive for resilience, as they are at risk of experiencing either positive growth or significant struggles. Struggling families, who may have faced heightened difficulties during the pandemic, require professional support to enhance their management capabilities and overall well-being, including specialized training and counseling.
Implications for healthcare providers and policymakers
Healthcare providers should acknowledge that family management experiences often deteriorate during crises, such as pandemics, among families of children and adolescents with developmental disabilities. However, variations in family management styles may lead to differences in family functioning and the child’s quality of life. To address this, providers should offer tailored interventions based on family management styles, reinforcing strengths in Thriving families while delivering targeted support to Struggling families. Additionally, healthcare providers should consider various family contexts, including parental education levels and the type of developmental disability, to ensure the provision of appropriate and effective healthcare services. Adopting a strengths-based perspective can further build resilience and enhance family well-being.
Furthermore, the current results offer evidence-based recommendations for policymakers to develop family-centered policies that address the distinct needs of families managing developmental disabilities. For example, families of children and adolescents with developmental disabilities who are more likely to be categorized under Struggling family management styles would benefit from intensive specialized training to enhance their ability to effectively manage their child’s condition. Additionally, providing respite care could help reduce caregiver stress and improve their perception of their child and family unit. These interventions are particularly essential since families exhibiting the Struggling style are likely to have an unfavorable perception of their child and limited confidence in their ability to effectively manage the child’s condition.
Limitations
This study has a few limitations. One notable limitation of this study is that it does not account for potential variations in family management experiences across different age groups of children and adolescents with developmental disabilities. Future research should examine age-related differences to provide more tailored and comprehensive insights.
Two FaMM subscales that exhibited low reliability were omitted from the analysis. Cluster 1 should be interpreted with caution due to its small sample size. To strengthen the robustness of these exploratory findings, future research would benefit from utilizing larger datasets and applying validation techniques, such as cross-validation or bootstrapping, to evaluate the stability and consistency of the identified clusters. Furthermore, the study’s cross-sectional design primarily reflects the perspectives of mothers and individuals with partners. Additional research is necessary to explore the involvement and impact of other family members and single parents.
Conclusion
This study examined and presented three family management styles among families of children and adolescents with developmental disabilities in Korea during challenging times, specifically during the pandemic. The current findings from the typology analysis are critical for understanding the intricate dynamics of family life among families of children and adolescents with developmental disabilities, as well as the relationships between subgroup variables and other factors.
In this study, we found that each cluster correlated with varying levels of children’s and adolescents’ quality of life and family functioning. The Thriving cluster requires ongoing support to enhance strengths while the Struggling cluster needs comprehensive interventions to improve condition management and reduce family challenges. The Somewhat Resilient cluster can benefit from early, proactive support to potentially advance toward the Thriving cluster. Additionally, several crucial family characteristics may influence the formation of family management styles. Healthcare providers should implement tailored interventions that consider specific family styles, particularly during crises. Furthermore, the results offer evidence-based guidance for policymakers to create family-centered policies tailored to the unique needs of families of children and adolescents with developmental disabilities, thereby enhancing support for healthcare providers’ practice.
Traditional educational interventions have predominantly focused on condition-related skills rather than strategies for integrating these skills into daily family life6. Considering the crucial connection between family management styles and child outcomes, future interventions that incorporate condition-specific care into routine family activities can significantly enhance outcomes for children with developmental disabilities and their families.
Data availability
The data supporting the findings of this study are not publicly available due to confidentiality agreements with subjects. However, the data underpinning the conclusions of this study can be made available upon reasonable request from the corresponding author.
References
Olusanya, B. O. et al. Global prevalence of developmental disabilities in children and adolescents: A systematic umbrella review. Front. Public. Health. 11, 1122009. https://doi.org/10.3389/fpubh.2023.1122009 (2023). PMID: 36891340; PMCID: PMC9987263.
Statistics Korea. Status of Persons with Disabilities. (2023). https://www.index.go.kr/unity/potal/main/EachDtlPageDetail.do?idx_cd=2768
Zablotsky, B. et al. Prevalence and trends of developmental disabilities among children in the united States: 2009–2017. Pediatrics 144 (4), e20190811. https://doi.org/10.1542/peds.2019-0811 (2019). PMID: 31558576; PMCID: PMC7076808.
Kokorelias, K. M., Gignac, M. A. M., Naglie, G. & Cameron, J. I. Towards a universal model of family centered care: a scoping review. BMC Health Serv. Res. 19 (1), 564. https://doi.org/10.1186/s12913-019-4394-5 (2019). PMID: 31409347; PMCID: PMC6693264.
Knafl, K. A. & Deatrick, J. A. Family management style: concept analysis and development. J. Pediatr. Nurs. 5 (1), 4–14 (1990). PMID: 2308062.
Deatrick, J. A. et al. Patterns of family management for adolescent and young adult brain tumor survivors. J. Fam Psychol. 32 (3), 321–332. https://doi.org/10.1037/fam0000352 (2018). PMID: 29698006; PMCID: PMC5926795.
Rolland, J. S. Cancer and the family: An integrative model. Cancer 104(11 Suppl), 2584-2595 (2005). https://doi.org/10.1002/cncr.21489. PMID: 16270342.
Knafl, K. A. et al. Patterns of family management of childhood chronic conditions and their relationship to child and family functioning. J. Pediatr. Nurs. 28 (6), 523–535. https://doi.org/10.1016/j.pedn.2013.03.006 (2013) (Epub 2013 Apr 19).
Dückert, S. et al. Multidimensional burden on family caregivers of adults with autism spectrum disorder: A scoping review. Rev. J. Autism Dev. Disord. 1–18. https://doi.org/10.1007/s40489-023-00414-1 (2023).
Schalock, R. L., Keith, K. D., Verdugo, M. A. & Gómez, L. E. Quality of life theory construction and model development in the field of intellectual disabilities. In (ed. Kober, R.) Enhancing Quality of Life for People with Intellectual Disability: from Theory To Practice. 17–32 (Springer, 2010).
Im, Y. & Kim, D. H. Family management style and psychosocial health of children with chronic conditions. J. Child. Fam Stud. 30, 483–492. https://doi.org/10.1007/s10826-020-01870-7 (2021).
Im, Y., Cho, Y. & Kim, D. Family management style as a mediator between parenting stress and quality of life of children with epilepsy. J. Pediatr. Nurs. 45, e73–e78. https://doi.org/10.1016/j.pedn.2018.12.007 (2019) (Epub 2018 Dec 20).
Im, Y. & Jung, S. Family functioning according to clusters of family management styles in Korean families of children with chronic atopic disease: A cross-sectional study. Int. J. Nurs. Stud. 109, 103674. https://doi.org/10.1016/j.ijnurstu.2020.103674 (2020). Epub 2020 Jun 6. PMID: 32590247.
Neece, C., McIntyre, L. L. & Fenning, R. Examining the impact of COVID-19 in ethnically diverse families with young children with intellectual and developmental disabilities. J. Intellect. Disabil. Res. 64 (10), 739–749. https://doi.org/10.1111/jir.12769 (2020). Epub 2020 Aug 18. PMID: 32808424; PMCID: PMC7461180.
Navas, P. et al. Impact of COVID-19 on the burden of care of families of people with intellectual and developmental disabilities. J. Appl. Res. Intellect. Disabil. 35 (2), 577–586. https://doi.org/10.1111/jar.12969 (2022).
Sachs, J. D. et al. The lancet commission on lessons for the future from the COVID-19 pandemic. Lancet 400 (10359), 1224–1280. https://doi.org/10.1016/S0140-6736(22)01585-9 (2022).
Statistics Korea. Household Trend Survey. (2023). https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1L9V054&conn_path=I2
Prata, J., Lawson, W. & Coelho, R. Stress factors in parents of children on the autism spectrum: an integrative model approach. Int. J. Clin. Neurosci. Ment Health. 6 (4), 2. https://doi.org/10.21035/ijcnmh.2019.6.2 (2019).
Kim, D. H. & Im, Y. J. Validity and reliability of Korean version of the Family Management Measure (Korean FaMM) for families with children having chronic illness. J. Korean Acad. Nurs. 43(1), 123–132 (Korean) (2013). https://doi.org/10.4040/jkan.2013.43.1.123.
Knafl, K. et al. Family Management Measure (FaMM) (2011). http://nursing.unc.edu/research/office-of-research-support-consultation/resources/family-management-measure-fa-mm/
Lee, S. K. The Effects of Risk and Protective Factors on Children’s Adaptation: The Theoretical Process Model [Dissertation]. (Sookmyung Women’s University, 1997).
Epstein, N. B., Baldwin, L. M. & Bishop, D. S. The McMaster family assessment device. J. Marital Fam Ther. 9 (2), 171–180. https://doi.org/10.1111/j.1752-0606.1983.tb01497.x (1983).
Gómez, L. E. et al. A new scale for the measurement of quality of life in children with intellectual disability. Res. Dev. Disabil. 53–54, 399–410. https://doi.org/10.1016/j.ridd.2016.03.005 (2016) (Epub 2016 Mar 21).
Sousa, V. D. & Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J. Eval Clin. Pract. 17 (2), 268–274 (2011). Epub 2010 Sep 28. PMID: 20874835.
Lawshe, C. H. A quantitative approach to content validity. Pers. Psychol. 28 (4), 563–575. https://doi.org/10.1111/j.1744-6570.1975.tb01393.x (1975).
Romero-Jeldres, M., Díaz, E. & Nadim, T. A review of Lawshe’s method for calculating content validity in the social sciences. Front. Educ. 8, 1271335. https://doi.org/10.3389/feduc.2023.1271335 (2023).
Gómez, L. E., Morán, M. L., Alcedo, M. Á., Arias, V. B. & Verdugo, M. Á. Addressing quality of life of children with autism spectrum disorder and intellectual disability. Intellect. Dev. Disabil. 58 (5), 393–408. https://doi.org/10.1352/1934-9556-58.5.393 (2020).
Sinha, P., Calfee, C. S. & Delucchi, K. L. Practitioner’s guide to latent class analysis: methodological considerations and common pitfalls. Crit. Care Med. 49 (1), e63–e79. https://doi.org/10.1097/CCM.0000000000004710 (2021). PMID: 33165028; PMCID: PMC7746621.
Weller, B. E., Bowen, N. K. & Faubert, S. J. Latent class analysis: A guide to best practice. J. Black Psychol. 46 (4), 287–311. https://doi.org/10.1177/0095798420930932 (2020).
Gough, K. & Happell, B. Undergraduate nursing students attitude to mental health nursing: a cluster analysis approach. J. Clin. Nurs. 18 (22), 3155–3164. https://doi.org/10.1111/j.1365-2702.2008.02764.x (2009). Epub 2009 Jul 8. PMID: 19619212.
Bruce, P., Bruce, A. & Gedeck, P. Practical Statistics for Data Scientists: 50 + Essential Concepts Using R and Python. 1st Ed. (O’Reilly Media, 2020).
Cohen, J. Statistical Power Analysis for the Behavioral Sciences. 2nd Ed. (Erlbaum, 1988).
Boehm, T. L. & Carter, E. W. Family quality of life and its correlates among parents of children and adults with intellectual disability. Am. J. Intellect. Dev. Disabil. 124(2), 99–115 (2019). https://doi.org/10.1352/1944-7558-124.2.99.
Lee, A., Yeh, V. J., Knafl, K. A. & Van Riper, M. Perceived experiences of Korean immigrant mothers Raising children with disabilities in the united States. J. Transcult Nurs. 33 (2), 219–227 (2022). Epub 2021 Dec 6. PMID: 34872416.
Jansen-van Vuuren, J. et al. Family quality of life for families of children with disabilities in African contexts: a scoping review. Qual. Life Res. 31 (5), 1289–1307. https://doi.org/10.1007/s11136-021-02994-z (2022). Epub 2021 Sep 18. PMID: 34537914.
Anderson, R., Walburn, J. & Morgan, M. Approaches to photoprotection and normalization in highly adherent families of children with xeroderma pigmentosum in the united Kingdom. Qual. Health Res. 30 (8), 1275–1286 (2020). Epub 2019 Feb 9.
Lee, S. H. & Hong, S. J. What are the social care support measures for children with disabilities following COVID-19? Health Welf. 23 (3), 39–63. https://doi.org/10.23948/kshw.2021.9.23.3.39 (2021).
Kim, M. A., Yi, J., Jung, S. M., Hwang, S. & Sung, J. A qualitative study on parents’ concerns about adult children with intellectual disabilities amid the COVID-19 pandemic in South Korea. J. Appl. Res. Intellect. Disabil. 34 (4), 1145–1155. https://doi.org/10.1111/jar.12875 (2021). Epub 2021 Mar 10. PMID: 33694235; PMCID: PMC8237012.
Van Riper, M. et al. Measurement of family management in families of individuals with down syndrome: A Cross-Cultural investigation. J. Fam Nurs. 27 (1), 8–22 (2021). Epub 2020 Dec 4. PMID: 33272069; PMCID: PMC7897787.
Tarzi, G., Mendoza, O., Lunsky, Y. & St John, L. The experiences and attitudes of family caregivers of adults with intellectual and developmental disabilities at different timepoints in the COVID-19 pandemic. Disabil. Health J. 16 (3), 101472. https://doi.org/10.1016/j.dhjo.2023.101472 (2023).
Hsiao, Y. J. Autism spectrum disorders: family demographics, parental stress, and family quality of life. J. Policy Pract. Intellect. Disabil. 15 (1), 70–79. https://doi.org/10.1111/jppi.12232 (2018).
Nikolić, M., Salkić, A. & Vantić-Tanjić, M. Parents’ education and functioning of families of children with intellectual disabilities. Res. Educ. Rehabil. 3(2), 52–61 (2020). https://rer.ba/index.php/rer/article/view/81.
Salomone, E. et al. The association between child and family characteristics and the mental health and wellbeing of caregivers of children with autism in Mid-Childhood. J. Autism Dev. Disord. 48 (4), 1189–1198. https://doi.org/10.1007/s10803-017-3392-x (2018). PMID: 29177606; PMCID: PMC5861164.
Bush, H. H., Cohen, S. R., Eisenhower, A. S. & Blacher, J. Parents’ educational expectations for young children with autism spectrum disorder. Educ. Train Autism Dev. Disabil. 52(4), 357–368 (2017). https://www.researchgate.net/publication/327527753_Parents’_educational_expectations_for_young_children_with_autism_spectrum_disorder.
Crossman, M. K., Parish, S. L., Hauser-Cram, P., Garcia, D. A. & Warfield, M. E. The influence of early intervention, informal support and the family environment on trajectories of competence for fathers Raising children with developmental disabilities. Res. Dev. Disabil. 81, 122–133 (2018). Epub 2018 May 21. PMID: 29798813.
Aishworiya, R. & Kang, Y. Q. Including children with developmental disabilities in the equation during this COVID-19 pandemic. J. Autism Dev. Disord. 51 (6), 2155–2158. https://doi.org/10.1007/s10803-020-04670-6 (2021). PMID: 32816170; PMCID: PMC7438977.
Acknowledgements
This study could not have been undertaken without the support of the families participating in this study. The authors would like to express their deepest appreciation for their contribution to the research.
Author information
Authors and Affiliations
Contributions
Anna Lee: Conceptualization, Methodology, Validation, Investigation, Resources, Data curation, Writing - original draft, Writing - review & editing, Supervision, Project administration, Funding acquisition. Eun Ju Park: Formal analysis, Data curation, Writing - original draft, Writing - review & editing, Visualization. Yeeun Kim: Formal analysis, Writing - original draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lee, A., Park, E.J. & Kim, Y. Family management styles of families of children and adolescents with developmental disabilities during the COVID-19 pandemic: a cross-sectional study. Sci Rep 15, 15260 (2025). https://doi.org/10.1038/s41598-025-99255-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-99255-7
