
Abstract
Congenital cytomegalovirus (cCMV) is the leading infectious cause of birth defects worldwide, yet immune determinants of protection to inform maternal vaccine design remain elusive due to the lack of a translational animal model. Here, we characterized the outcome of primary rhesus CMV (RhCMV) infection in pregnant, immunocompetent, RhCMV-naïve rhesus macaques. RhCMV DNA was detected in amniotic fluid and/or fetal tissues in six of 12 (50% placental transmission) dams following early second trimester gestation RhCMV inoculation. Widespread tissue dissemination dominated by one of two inoculated RhCMV strains was present in one fetus (8.3% cCMV disease). RhCMV DNA detection in the amniotic fluid was associated with elevated fetal and maternal plasma TNF-alpha and reduced maternal brain-derived neurotrophic factor and IL-10 levels. Maternal RhCMV exposure during pregnancy had a broad impact on the placenta and fetus even in the absence of congenital infection, as evidenced by ubiquitous maternal-fetal interface infection, and reduced placental efficiency and small-for-gestation age fetuses compared to control pregnancies. This model provides new insights into the complexity of CMV vertical transmission and can be used to evaluate immune and viral determinants of protection against cCMV.
Similar content being viewed by others


Introduction
Congenital cytomegalovirus (cCMV), the leading cause of in utero infections, impacts ~1 in 200 births each year worldwide1,2. Following intrauterine transmission, cCMV can cause teratogenic effects such as microcephaly, intrauterine growth restriction (IUGR), developmental delays, and sensorineural hearing loss (SNHL)2,3,4. Despite its global impact, there are currently no available efficacious preventatives for cCMV.
One barrier to developing a successful maternal CMV vaccine is our limited understanding of immune determinants necessary for preventing intrauterine transmission5,6. Primary infection of CMV-seronegative women during pregnancy has a higher risk of intrauterine transmission (30–70%) compared to reinfection or reactivation in CMV-seropositive women (1–4% transmission risk), suggesting pre-existing maternal immunity can partially protect against cCMV5,7. Yet it is well-established that a robust CMV-specific humoral and cellular immune response induced by natural infection is not sufficient to prevent reinfection or cCMV8,9,10. Protection against congenital infection may require adequate immunity at the tissue level, in this instance at the maternal-fetal (M-F) interface to prevent CMV from crossing the placental barrier and infecting the fetus. Tissue immunity is difficult to assess in clinical settings due to ethical limitations and limited sample availability, so establishing a translational animal model of cCMV is critical for better defining immune determinants of protection.
Rhesus macaques have been used for studies on human CMV (HCMV) pathogenesis in the context of AIDS and transplant settings11. This model is also ideal for studying the maternal immune system and outcomes of cCMV infection because of biologic and genetic similarities between rhesus CMV (RhCMV) and HCMV, and the physiologic and immunologic similarities between macaque and human placenta12,13,14. Historical studies showed intraperitoneal, intracranial, and intraamniotic RhCMV inoculation in rhesus macaques results in fetal pathology consistent with human cCMV infection11,15. More recently, we established the placental transmission model of cCMV in rhesus macaques and demonstrated the ability of RhCMV to cross the placenta and cause fetal infection after intravenous inoculation in RhCMV-seronegative rhesus macaques that were either immunocompetent or CD4+ T cell-depleted prior to RhCMV infection. In the CD4+ T cell-depleted group, six of six dams (100%) transmitted RhCMV across the placenta and five (83%) experienced spontaneous abortion16,17. In the immunocompetent group, two of three dams transmitted RhCMV across the placenta, but did not exhibit RhCMV-associated fetal sequelae16. Due to the small size of the immunocompetent cohort, we were unable to fully characterize intrauterine transmission in the setting of an intact immune system. We therefore set out to define a robust translational model of primary cCMV transmission using a larger immunocompetent cohort of rhesus macaques.
Here, we report the outcome of primary infection in 12 immunocompetent rhesus macaque dams inoculated intravenously with two RhCMV strains during early second trimester gestation and show that vertical transmission and cCMV disease rates in this model are like primary HCMV infection. Using whole-genome deep sequencing, we characterized the dominant RhCMV strain crossing the placenta in one fetus with extensive cCMV disease. We also define virologic and pathologic responses to primary RhCMV infection in pregnancy and show its impact on the placenta and fetus even in the absence of congenital infection. Finally, we identified several analytes associated with RhCMV vertical transmission in our model. Our results corroborate published evidence that rhesus macaques recapitulate human cCMV pathogenesis and provide new insights into the complexity of RhCMV vertical transmission.
Results
Viremia and viral shedding kinetics
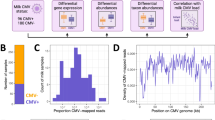
To model primary human cCMV infection, we enrolled 12 pregnant RhCMV-seronegative rhesus macaque dams that were intravenously inoculated at late first trimester/early second trimester gestation with equal proportions of the wild-type-like RhCMV strain UCD52 and a bacterial artificial chromosome-clone (BAC) with repaired full length (FL)-RhCMV and monitored RhCMV DNAemia in maternal blood, urine, saliva and amniotic fluid obtained by ultrasound-guided amniocentesis until elective Cesarean section (C-section) near term gestation, at which point placenta and fetal tissues were harvested (Fig. 1A, Supplementary Table 1).

A Twelve RhCMV-seronegative, immunocompetent rhesus macaque dams were intravenously inoculated with two RhCMV strains during early second trimester gestation. Blood, amniotic fluid (AF), urine, and saliva were collected weekly until elective C-section. Fetal and placental tissues were harvested at C-section. These samples were used in downstream analyses. Created in BioRender. Manuel, T. (2025) (https://BioRender.com/la7dz86). B RhCMV DNA copy numbers in plasma, saliva, and urine in individual animals. Mean of three to six technical PCR replicates for each data point shown. Viral loads expressed as mean copies of input RhCMV DNA per mL of plasma, and per µg of input DNA in saliva or urine.
RhCMV DNAemia was detected in all dams, peaking at day 7 through day 14 post-infection (PI), and thereafter resolving with variable kinetics (Fig. 1B and Supplementary Fig. 1). Beginning at 6 weeks PI, eight of 12 (75%) dams became intermittently aviremic. Viral shedding in saliva and urine appeared within 3 weeks PI with variable kinetics among the dams. By week 4 PI, all dams were consistently shedding RhCMV in saliva and urine at levels ranging between 106 and 108 RhCMV DNA copies per µg input DNA that persisted for the duration of the study (Fig. 1B and Supplementary Fig. 1). This is consistent with prior studies showing naturally-infected immunocompetent rhesus macaques are aviremic, yet persistently shed virus in saliva and urine18.
RhCMV intrauterine transmission
In clinical settings, the “gold standard” method for detection of cCMV includes amniocentesis followed by PCR analysis of the amniotic fluid (AF)19,20. We replicated this method in our previous studies, as well as in the current study. Consistent with our prior study, AF positivity was defined by PCR detection of RhCMV DNA in at least two of 12 individual replicates of AF per time-point21. Based on this criterion, we determined five dams were amniotic fluid positive (AF+), and the remaining seven dams were amniotic fluid negative (AF–) (Fig. 2A). RhCMV DNA in one of 12 replicates was detected in the AF of dam 001-102; however, this did not meet our criterion for AF positivity.

A RhCMV DNA detection in amniotic fluid (AF) of five AF+ dams. Viral loads expressed as mean RhCMV DNA copies per mL of AF. Data on mean of 12 PCR replicates per time-point. B Schematic diagram of rhesus macaque M-F interface tissues. Created in BioRender. Manuel, T. (2025) (https://BioRender.com/501tyz9). C Heatmap illustrating mean RhCMV DNA copies per µg of input DNA within tissues of the M-F interface of each dam within AF+ and AF– group. Mean copy number of 12 PCR replicates shown. Gray boxes (ND) indicate no sample collected. White boxes (0) indicate no viral DNA was detected in the sample. D Heatmap showing number of RhCMV-positive cells per cm2 by in situ hybridization (ISH) in full-thickness placental cross-sections of individual AF+ and AF– dams.
The kinetics of RhCMV DNA detection in the AF varied among the dams. It was detected transiently within 7 weeks PI in four of five AF+ dams. Dam 001-106 showed the earliest detectable RhCMV DNA in the AF at three time-points (days 7, 14, and 21 PI), whereas dams 001-109, 001-107, and 001-103 had detectable RhCMV DNA at a single time-point between day 28 and day 49 PI (Fig. 2A). In contrast, RhCMV DNA in the AF of dam 001-101 was detected on days 77 and 82 PI and showed the highest RhCMV DNA copy numbers (Fig. 2A).
We also evaluated the M-F interface for RhCMV infection. Each component of the M-F interface (amniochorion, fetal and maternal surfaces of both the primary and secondary placental discs, and maternal decidua) was dissected and RhCMV DNA quantitated by quantitative real-time PCR (Fig. 2B, C). In situ hybridization (ISH) was performed on a full thickness section (decidua through amniochorion) of the primary placental disc to confirm placental RhCMV infection (Supplementary Fig. 2A, B). Based on our PCR positive criteria outlined in the methods, 11 of 12 dams were RhCMV DNA-positive at the M-F interface (Fig. 2C). 11 of 12 dams had RhCMV ISH-positive cells at the M-F interface (Fig. 2D). PCR and ISH quantitation of RhCMV infection at the M-F interface did not correlate and were sometimes discordant, as demonstrated by dams 001-101 and 001-107 (Fig. 2C, D). We did not detect RhCMV DNA in the umbilical cord of any dam.
Taken together, all 12 dams met our criteria for being RhCMV-positive at the M-F interface. Discordance between quantitative PCR and ISH data is likely due to differences in sampling and the random multifocal distribution of RhCMV throughout the placenta. Our PCR and ISH results paint a complex picture that highlights the high frequency of detection of RhCMV at the M-F interface even in the absence of evidence of AF positivity and emphasizes the need for multimodal diagnostics to assess placental transmission risk.
cCMV outcomes
All placental lesions identified were of mild severity. Lesions included acute to subacute placentitis in four dams; chorioamnionitis in one dam; and placental infarction in two dams (Supplementary Table 2). Additional histopathologic changes in placentas included scattered placental fibrinoid, mineralization, and syncytial knot formation. However, these changes can be seen with variable frequency in normal, late term placentas, and therefore were not interpreted as pathologic.
One of 12 fetuses (fetus of dam 001-101) had widespread RhCMV infection based on multiple tissues with detectable RhCMV DNA by PCR (Fig. 3A). The highest RhCMV DNA copy numbers within this fetus were found in the parietal cortex, basal ganglion, and lung, with lower copy numbers in the cochlea, kidney, spleen, liver, submandibular salivary gland, parotid salivary gland, hippocampus, cerebellum, frontal cortex, occipital cortex, thalamus, and hypothalamus (Fig. 3A). RhCMV DNA was also detected in the plasma and cord blood of this fetus, but not in the urine which was collected by cystocentesis (Fig. 3A).

A RhCMV DNA copies in fetal tissues of dams 001-101, 001-107, and 001-110. Mean copy number of 12 PCR replicates shown and expressed per µg of input DNA for urine and tissues, or per mL of sample for fetal plasma and cord blood. Gray boxes and ND indicate no sample collected. Tissues in which no viral DNA was detected are denoted with “0” and a white box. Representative RhCMV ISH of fetal tissues from dam 001-101. Rare RhCMV RNA positive cells (green, arrows) were detected in inflamed sections of hypothalamus (B) and lung (C) with RNAscope. Bar = 50 μm. D Heatmap showing number of RhCMV-positive cells per fetal tissue sample from dam 001-101. Histopathology of fetal tissues from dam 001-101 showing E Glial nodules in brainstem; F Hypothalamus lesions included cerebral vessels with mononuclear perivascular cuffs; G Lung, alveolar septa were thickened by inflammatory cells with rafts of neutrophils (inset) within alveoli. Bar = 100μm.
Two additional fetuses were RhCMV DNA positive in one organ (Fig. 3A). The fetus of dam 001-107 had two of 12 positive replicates in the fetal urinary bladder, while the fetus of dam 001-110 had two of six positive replicates in the cochlea. Four other fetuses (001-102, 001-104, 001-105, and 001-109) had detectable levels of RhCMV DNA in one of 12 replicates in a single organ, but did not meet our criterion for PCR positivity. These included the fetal urinary bladder of 001-104, the fetal cochlea of 001-102, the parietal cortex of 001-109, and the auditory ganglion of 001-105.
To confirm the widespread infection found in the 001-101 fetus, we performed ISH on the same tissues used in our PCR analysis (Fig. 3B–D). Similar to the analyses of the M-F interface, RhCMV quantitation in fetal tissues by ISH and PCR did not correlate, likely due to sampling differences and random multifocal distribution of RhCMV (Supplementary Fig. 2C). However, both methods indicated widespread RhCMV infection. Viral intranuclear inclusions, which are characteristic of CMV infection, were not observed, but the presence of RhCMV was confirmed by ISH in lesions found during histopathological examination (Fig. 3B–D). Lesions consistent with cCMV were identified in multiple organs of the fetus of dam 001-101 (Fig. 3E–G) and included mild lymphocytic perivascular cuffing and multifocal glial nodules within the hypothalamus and brainstem, interstitial pneumonia, and rare panniculitis. Two other fetuses had histopathologic lesions- the fetus of dam 001-102 had a focus of cerebral hemorrhage in the frontal lobe, and the fetus of dam 001-106 had mild histiocytic infiltration of the thymus.
It is generally thought that the source of CMV in the AF is fetal urine. We were able to collect urine by cystocentesis from seven of 12 fetuses at fetal necropsy including four AF+ dams (001-101, 001-103, 001-107, 001-106) and three AF– dams (001-110, 001-105, 001-108). All fetal urine samples were RhCMV-negative by PCR. Fetal plasma IgM serology performed on IgG-depleted samples was also inconclusive of fetal infection (Supplementary Fig. 3A, B).
Compared to our previous studies of primary RhCMV infection in the setting of CD4+ T lymphocyte depletion16,17, all dams in this cohort had reduced risk of RhCMV DNA detection in amniotic fluid (41.6% AF+ vs 100% AF+ in CD4-depleted dams) and carried to elective C-section with no incidence of spontaneous abortion (100% vs 16.7% fetal survival in CD4-depleted dams) (Supplementary Fig. 4A, B).
Fetal and placental morphometrics
cCMV can cause delayed fetal growth and IUGR. Therefore, we performed weekly ultrasound measurements of the fetal hand, foot, humerus, femur, occipito-frontal diameter, biparietal diameter (BPD), head circumference, abdominal circumference, and chest circumference. We limited our statistical analyses to the BPD and femur length, as these are the most reliable and clinically relevant measurements, and compared them to reference sonographic values across gestation age in normal pregnant rhesus macaques22. No statistically significant differences were noted in the BPD or femur growth rate compared to the reference. Minor variations were noted among fetuses in our cohort between gestation days 108–136, with some of the fetuses exhibiting a shorter average femur length, and in one fetus, 001-111, a narrower BPD, but these differences were not significant (Fig. 4A). There were no statistically significant differences between the fetal growth rates of AF+ and AF– dams.

A Fetal growth curves of biparietal diameter (BPD) and femur length. AF+ dams denoted by red icons, AF– dams shown in black, and referent population indicated by blue icons. Shaded region and dotted line indicate range of gestation days that dams were inoculated with RhCMV. B Box and whisker plot demonstrating CRL and fetal weight z-scores of placenta PCRhi and PCRlo dams. C Summary of morphometric parameter z-scores below population median and small for gestational age (SGA) by placenta PCRhi/lo burden and overall. D Bar graph illustrating placental efficiency ratios of the study dams in gray and the referent population from Roberts et al. in blue. Significance determined by Wilcoxon rank sum test. Error bars denote minimum and maximum measurements.
At C-section, the fetus and placenta were weighed, and fetal measurements were taken and compared to published reference values for fetal morphometrics based on gestation day23 (Supplementary Table 3A). All parameters were centered and scaled by gestational age specific reference mean and standard deviation, respectively, to define z-scores based on the published values. We then assessed the z-score characteristics of crown-rump length (CRL) and fetal weight (Fig. 4B, C). Six of 12 fetuses (50%) had CRL z-scores values below the expected 10th percentile (i.e., z-score < −1.28) considered small for gestation age (SGA). Two of 12 (16.7%) fetuses had fetal weight z-scores in the SGA range (Fig. 4B). Our cohort had a discernably greater proportion of fetuses with SGA CRLs than expected (p < 0.001; Fig. 4C). For CRL and fetal weight, nine out of 12 (75%) fetus z-scores were below zero (Fig. 4C). The observation that two-thirds of the cohort had z-scores below zero could suggest potential IUGR in primary RhCMV-infected dams.
Next, we grouped fetuses based on PCR results to determine whether detectable RhCMV DNA in the AF (n = 7 AF– vs n = 5 AF+), or fetal tissue (n = 9 Fetus PCR– vs n = 3 Fetus PCR+) correlated with fetal morphometrics measured at C-section (Supplementary Table 3A). Additionally, we grouped fetuses based on a scoring metric we developed for placental RhCMV spread at the M-F interface as Placental PCRlo (n = 6) and PCRhi (n = 6) (described in methods) (Supplementary Table 3A). We did not observe significant differences in morphometrics between groups based on AF-positivity or fetal infection (Supplementary Table 3B). However, the CRL and fetal weight parameters showed a consistent separation of z-scores between the Placental PCRlo and PCRhi groups (Supplementary Table 3A). The PCRhi dams displayed a smaller CRL compared to the PCRlo group (p = 0.092; Supplementary Table 3B). The proportion of fetuses with CRL z-scores below the 10th percentile was higher in the Placenta PCRhi (66.7%) compared to the Placenta PCRlo (33.3%) group. This suggests a potential association between SGA and RhCMV burden at the M-F interface (Fig. 4B, C).
Placental efficiency (PE) is a measure of how well the placenta supports fetal nutrition, growth, waste management, and oxygen transfer. PE, thus, is an important measurement to consider when drawing conclusions about fetal and placental health following primary RhCMV infection. For each dam, we collected the weight in grams of the fetus and placenta at C-section. Total placental weight includes primary and secondary placental discs, as well as the umbilical cord. We then calculated the fetal: placental weight ratio to use as a proxy of PE23. We compared the PE of our dams to that of similar gestational age controls from Roberts et al.23. The fetus of dam 001-109 was not weighed, so this dam’s PE was unable to be calculated. The PE of dams in our cohort (n = 11) ranged from 2.71 to 3.89 (median = 3.33). Comparatively, the gestation-comparable controls (n = 28) taken from Roberts et al. had PE measurements ranging from 1.9 to 5.6 (median = 4.11). Exact Wilcoxon rank sum test showed statistically significantly lower PE measurements in our cohort compared to these controls (Fig. 4D; p = 0.0002).
Viral sequencing
We used whole genome sequencing to understand in vivo dynamics of the two inoculating strains over the course of infection in 001-101, the only dam to exhibit widespread fetal infection. We performed amplicon-based Illumina deep sequencing of RhCMV from maternal plasma during acute infection (4, 7, 14 days PI), plasma and AF at the timepoints when AF was positive for RhCMV (77 and 82 days PI), and five fetal tissues at the time of delivery that had high viral loads (82 days PI; heart, lung, kidney, parietal cortex, basal ganglion). Three samples (plasma 77 and 82 days PI, and AF 82 days PI) had fewer than 1000 input copies and we observed a corresponding decrease in genome coverage in these samples.
Inferred strain frequency in each sample was determined by identifying genomic positions where the two reference strains differed and applying several filters to those positions to account for strain-specific mapping biases (Supplementary Fig. 5). The total number of remaining single nucleotide variants (SNVs) used for each sample ranged from 14 to 862 (median 710) and are specified in Supplementary Table 4. For each sample, we then calculated the mean proportion of aligned bases per position that had the nucleotide corresponding to either strain (number of reads with UCD52 or FL nucleotide/total reads) to estimate the relative abundance of each strain in the sample. To ensure our method was robust to the reference genome used for mapping, we performed these calculations using mapping outputs with either RhCMV-FL and RhCMV UCD52 as the mapping reference and found consistent inferred strain frequencies (within 1.5%) between the two mapping references (Fig. 5, Supplementary Fig. 6A–M, Supplementary Table 4). Furthermore, when performing our strain frequency analysis on the sequenced stock virus, the inferred strain frequency was >99.8% for both viruses (Supplementary Table 4, Supplementary Fig. 5E, F). Across all samples, mean inferred strain frequency for “other strain” was <0.03%, highlighting a low level of other variants resulting from de novo mutations or sequencing error.

For each sample, inferred strain frequency of RhCMV UCD52 (blue) or FL-RhCMV (orange) was determined by taking mean of the percent of reads with the nucleotide corresponding to each strain at positions where the two inoculating strains differ. Sample IDs are denoted with “P” = plasma, “AF” = amniotic fluid, # = days post infection, “M” = maternal, and “F” = fetal. Mean indicated by open circle with error bars corresponding to standard error. Black dots represent frequencies at a single SNV.
At acute plasma timepoints (4, 7, 14 days PI), FL-RhCMV virus is the dominant replicating strain early in infection (90-91% at 4 days PI), but by 14 days PI, the strains appear to be present in a mixed population (39–40% FL, 60–61% UCD52; Fig. 5). Although we sequenced virus from plasma at 77 days PI, the overall genome coverage was low due to limited input virus, and only 14 SNVs were retained after filtering for determining inferred strain frequency (Supplementary Fig. 6E). Therefore, we omitted this sample from our inferred strain frequency calculations. AF from 77 days PI and the paired AF and plasma samples from 82 days PI, despite an apparently mixed population of virus in the plasma at 82 days PI, FL-RhCMV appears to be at nearly 100% frequency in the AF (Supplementary Fig. 6F–H). Of note, there was limited virus present in the plasma at 82 days PI, so the inferred strain frequency is based on 273-275 SNVs. We sequenced five fetal tissues, also collected at 82 days PI, and these tissues appear to have nearly 100% FL-RhCMV, consistent with the AF (Fig. 5, Supplementary Fig. 6I, M).
Acute host response association with cCMV transmission
We evaluated the early host response as a predictor of RhCMV infection outcome. White blood cell (WBC) counts revealed a transient decline in leukocytes (p = 0.001; padj = 0.0029) by day seven PI due to a decline in neutrophil counts (Fig. 6A). This was followed by an increase in lymphocyte counts that persisted up to day 84 PI (Fig. 6A). The mean absolute monocyte counts significantly increased by the 3rd week PI (p = 0.0005; padj = 0.0015), then returned to baseline levels by week 6 PI (Fig. 6A). We observed no discernable differences between cell counts of AF+ and AF– dams.

A Mean absolute counts of circulating total white blood cells (WBC), neutrophils, lymphocytes, and monocytes from day 0 to day 98 post-infection (PI). Gray lines denote AF– dams (n = 7), while red lines denote AF+ dams (n = 5). B Heatmap illustrating rank values of median maternal plasma concentrations of cytokines between 0 and 14 days PI. Cytokines measured by a 33-plex NHP Luminex assay. C Box and whisker plot illustrating area under the curve (AUC) of maternal plasma TNF-alpha concentrations during first 2 weeks PI. Red icons denote AF+ dams (n = 5) and black icons refer to AF– dams (n = 7). The open red circle denotes dam 001-101. Significance determined by Wilcoxon rank sum test.
Using a 33-plex NHP Luminex assay, we evaluated concentrations of cytokines within the maternal plasma in the first 2 weeks PI. Of the 30 analytes which passed our quality control requirements, 16 demonstrated highest median concentrations on day four PI, three at day seven PI, and three at day 14 PI (Fig. 6B). Multiple analytes showed changes over time with several showing a significant post-hoc difference against baseline (Supplementary Table 5). Several pro-inflammatory and anti-viral analytes showing a statistically significant transient increase at day 4 PI included GM-CSF, IFN-alpha, IP-10, IL-6, and VEGF (Supplementary Table 5). When comparing the area under the curve of analyte concentrations in maternal plasma during the first 2 weeks post-infection, one analyte, TNF-alpha, was higher in AF+ dams compared to AF– dams (p = 0.0139; padj: 0.417 Fig. 6C).
Analytes associated with RhCMV amniotic fluid transmission
PCR analyses showed a significant increase in cumulative viral load (via AUC) within the urine of AF– dams compared to AF+ dams during the first 2 weeks PI (p = 0.0177, padj: 0.053, Supplementary Fig. 7A). There was no association between AF status and the AUC of viral loads in plasma or saliva during the study. When we examined cumulative viral load over the remainder of the study, we no longer observed the statistically significant association in urine (Supplementary Fig. 7B, C).
We then evaluated analytes within maternal plasma, AF, and fetal plasma collected at C-section for differences between AF+ and AF– dams. In the maternal plasma, AF+ dams had lower concentrations of brain-derived neurotrophic factor (BDNF) (p = 0.048, padj: 0.502) and IL-10 (p = 0.0455, padj: 0.502) compared to AF– dams (Fig. 7A and Supplementary Table 6). In contrast, IFN-alpha (p = 0.0265; padj: 0.342) and IL-21 (p = 0.0467; padj: 0.342) were higher in the AF of AF+ dams (Fig. 7B and Supplementary Table 7). Fetal plasma TNF-alpha concentrations were significantly higher in AF+ dams compared to AF– dams, and this remained statistically significant after multiple testing correction (Fig. 7C; p = 0.00126; padj: 0.0379; Supplementary Table 8). This difference was not observed in cord blood plasma (Supplementary Table 9). We also measured chemerin levels in amniotic fluid as it has been reported as a biomarker of severe cCMV infection in humans24, but in our model, we observed no difference between AF+ and AF– dams (Supplementary Fig. 8).

A Concentrations of BDNF and IL-10 in maternal plasma at time of C-section for AF+ dams (red) and AF– dams (black). B Plots showing concentrations of IFN-alpha and IL-21 in the amniotic fluid at C-section in AF+ dams (red) and AF– dams (black). C Plot displaying TNF-alpha concentrations in fetal plasma of AF+ dams (red) and AF– dams (black). Open circle in A-C denotes dam 001-101. D Principal Components Analysis (PCA) visualization shows clear separation of AF+ (red) and AF– dams (gray) in PC3 axis when evaluating analytes in fetal plasma. E Biplot reflecting importance of each variable with regards to the principal components. Bar graph illustrates the importance of each analyte in regard to the principal components. Significance determined by Wilcoxon rank sum test. Statistical analyses in (A–E) include five AF+ dams and seven AF– dams. Error bars denote minimum and maximum measurements.
While not statistically significant, other notable findings included higher concentrations of IFN-beta, IFN-gamma, and VEGF (p = 0.0732; padj: 0.342) in the AF of AF+ dams (Supplementary Table 7). As in the maternal plasma at C-section, levels of BDNF in the AF were lower in AF+ dams compared to AF– dams (p = 0.0732; padj: 0.342; Supplementary Table 7). We observed higher granzyme B concentrations in cord blood of AF+ dams compared to AF– dams (p = 0.0568; padj: 0.795; Supplementary Table 9).
We then performed exploratory principal component analysis (PCA) on maternal plasma, cord blood, fetal plasma, and AF cytokine data. Only the PCA of fetal plasma showed separate clusters for AF+ and AF– dams evident in the PC3 axis (Fig. 7D). This difference was primarily driven by TNF-alpha, followed by IL-7 and CXCL2 (Fig. 7E).
Discussion
In this study, we established the outcomes of primary RhCMV infection during pregnancy in immunocompetent rhesus macaques with a longitudinal systemic and tissue-level analysis of events leading to congenital transmission. Our results show differences and similarities to human cCMV infection. We demonstrate placental RhCMV transmission in immune competent rhesus macaques after early second trimester primary infection, with the profile of fetal tissues infected in utero, and detection of disseminated CMV disease in the newborn occurring at a frequency akin to symptomatic cCMV in humans. We also report a broad outcome of maternal RhCMV exposure during pregnancy with ubiquitous M-F interface infection and deleterious effect on fetal growth even in the absence of vertical transmission, which has not been reported in human cases.
Using the criteria of RhCMV DNA detection in AF, our cohort showed a 42% (5/12) placental transmission rate in immunocompetent dams. Of these five dams, one exhibited the typical virologic pattern described in human cCMV cases, with high copy numbers of RhCMV DNA detected in the AF late in gestation associated with disseminated fetal infection. In the other four dams, RhCMV DNA was detected transiently in the AF in the first 6 weeks post RhCMV inoculation at early- to mid-second trimester gestation, an observation not reported in human cCMV cases. One reason for this discrepancy may be the intravenous route of inoculation in the rhesus macaque model, accounting for the early detection of RhCMV DNA in AF. Another reason may be the absence of longitudinal AF sampling data in humans. Because amniocentesis for suspected cCMV in pregnant women is typically performed at a single time-point after 20-weeks gestation and at least 6–8 weeks after a suspected maternal CMV infection, it is unclear whether the observation of early transient AF positivity in our model reflects a biological difference between humans and rhesus macaques, or if the phenomenon is under-recognized in clinical settings due to limited opportunities for longitudinal sampling of the AF.
We also identified an 8% rate of widespread fetal infection- similar to the rate at which symptomatic cCMV is reported in humans2. Dam 001-101 exhibited a distribution of virus within fetal tissues consistent with reports in human cCMV cases25. One of the RhCMV-positive tissues was the cochlea, which corroborates findings from murine studies showing CMV migrates to the inner ear after inoculation of the cerebral cortex26. This may be indicative of inner ear pathology that leads to SNHL—a common outcome of human cCMV26,27. RhCMV DNA was also detected in tissues consistent with CMV natural history (urinary bladder) and other organs involved in cCMV symptomatology (brain and auditory ganglion). The fetus of dam 001-101 also exhibited encephalitis, pneumonia, and panniculitis- consistent with CMV-associated sequelae in humans. However, our observations in this fetus were not as severe as outcomes reported in human infants25,28,29. This discrepancy may be due to much of the current understanding of human cCMV pathology being limited to cases with severe outcomes, such as those with spontaneous abortion or birth defects, which did not occur in our study25,29,30,31,32. On the other hand, this discrepancy may stem from differences in fetal development in humans and rhesus macaques.
Another difference from humans was that the PCR of fetal urine collected by cystocentesis was consistently negative for RhCMV DNA, including in the fetus of dam 001-101 despite widespread fetal tissue infection in several organs including the kidney. Because CMV is a slow replicating virus, successful replication within the fetal kidney and subsequent virus excretion may not occur until up to 3 weeks post-infection of the fetus. If this fetus became infected near the time of C-section, the virus may not have undergone sufficient replication for shedding in the urine. Moreover, the replicating virus may be more present in the lower urinary tract which is not fully assessed by urine collected by cystocentesis. Although fetal urine is thought to be the major source of CMV in AF, it is not the only source that has been described. The fetus of dam 001-101 did have detectable levels of RhCMV DNA in the lungs and salivary glands. Thus, fetal saliva and pulmonary secretions may be the alternative source of RhCMV in the AF of this dam, consistent with the current understanding of AF contents33,34,35.
When performing in-depth interrogations of the M-F interface, AF, and fetal tissues by PCR and ISH, we identified a broad range of outcomes, which has previously not been reported (Fig. 8A). These additional outcomes ranged from ubiquitous RhCMV detection at the M-F interface without AF positivity or fetal infection, to AF positivity with undetectable, limited, or disseminated fetal infection, implying potential transmission bottlenecks. These additional outcomes paint a more complicated picture of cCMV transmission, with potential for unrecognized clinical impacts on the developing fetus. Of note, reports of detection of CMV DNA in late gestation human placenta from normal deliveries36,37,38,39 suggests that non-clinically recognized CMV infection at the M-F interface may not be unique to the rhesus macaque model.

A Schematic summarizing PCR and ISH results in Amniotic Fluid (AF), M-F interface, and fetal tissues. Pink cell/plus sign indicate RhCMV nucleic acid detection in the respective tissues. Below schematic is a description of our proposed spectrum of congenital RhCMV intrauterine transmission. B Diagram of possible routes of cCMV vertical transmission. Dotted lines represent new proposed modes of vertical transmission found in our cohort. Created in BioRender. Manuel, T. (2025) (https://BioRender.com/8e36npq).
The route by which CMV crosses the placenta is not fully understood, but placental HCMV infection in the absence of fetal infection suggests the placental barrier is critical for protection40. Similarly, our cohort has shown M-F interface positivity in the absence of fetal tissue or AF positivity. This may highlight the importance of AF, or the fetal immune system, in protecting against fetal cCMV infection. Concurrent with this finding, one study containing 68 pregnant women with primary CMV infections reported false positive results from CMV PCR of AF. Within this group, 52 infants were CMV negative by urine culture, but 17 (33%) of the 52 had detectable CMV in the AF. The authors suggest that these results indicate virus transfer to the AF without fetal infection41. The source of early and transient detection of RhCMV DNA in the AF in four dams in our study is unclear (Figs. 2A and 8A). It is possible that RhCMV entry into the AF occurred during the viremic phase via intramembranous absorption, as has been described in rhesus macaques33. Subsequently, successful establishment of fetal infection may rely on several factors. Overall, the heterogenous spectrum of cCMV vertical transmission in our model suggests that RhCMV crosses a series of bottlenecks before accomplishing transmission or establishing fetal infection (Fig. 8B). These bottlenecks could be imposed by viral or tissue barriers, as well as by circulating and tissue-resident maternal and fetal immune cell subsets that can be studied systematically in our model.
We were also able to uncover the dominance of the clonal BAC-derived FL-RhCMV in the AF and fetal tissues of dam 001-101, despite apparently mixed populations in maternal plasma. Although it appears that FL-RhCMV was the dominant virus to cross the placenta and lead to widespread fetal infection in this dam, the clinical isolate RhCMV UCD52 did cross the placenta and lead to fetal infection in a previous study16. We speculate that either FL-RhCMV has a competitive fitness advantage or, perhaps the placenta functions as a narrow bottleneck and FL-RhCMV established the initial infection in the fetal compartment. The latter contrasts with a previous estimate of bottleneck size at the M-F interface using only two genes, which suggested a wide bottleneck at the M-F interface42. This method for inferring sample-level strain frequencies is subject to several limitations. We used many SNV positions across the viral strain genomes to infer strain frequencies, but our approach was still limited by the need to select SNVs without strain bias and with sufficient sequencing coverage. Of note, our method for inferring strain frequency highlights variable nucleotide frequencies for each strain across this genome. Frequent recombination with multi-strain infections of HCMV is well-documented. We hypothesize that recombination between the two inoculating isolates may happen in vivo; however, assessing haplotypes and determining the extent to which recombination is occurring is outside the scope of this manuscript.
Despite normal fetal ultrasound measurements during pregnancy, CRL and fetal weight measurements taken at fetal necropsy indicated that the presence of RhCMV at the M-F interface alone has an impact on fetal growth. Dams with higher PCR scores at the M-F interface had fetuses with smaller CRLs, compared to dams with lower PCR scores and compared to reference controls. Dams with high PCR scores also tended to have fetuses of lower weights at C-section. Surprisingly, fetal growth was not significantly impacted by AF DNA positivity or fetal tissue DNA positivity. In summary, abundance of RhCMV virus particles detected at the M-F interface negatively correlates with fetal weight and CRL in our cohort. This indicates that even when RhCMV is undetectable in AF or fetal tissues, the presence of RhCMV at the M-F interface can have an impact on fetal outcomes of this model.
Several analytes were associated with RhCMV transmission to the amniotic fluid. Fetal plasma TNF-alpha concentration was the strongest prognostic indicator differentiating AF+ and AF– dams. Our study also revealed lower levels of circulating BDNF in maternal plasma of AF+ dams. Maternal BDNF is involved in placentation and placental health43,44, and clinical studies have shown that low maternal serum BDNF levels correlate with higher risk of low birth weight45. Thus, sustained low levels of BDNF in AF+ dams may be predictive of placental or fetal pathology. Additionally, lower IL-10 in the maternal plasma and higher IL-21 and IFN-alpha in the AF at term gestation point to an increased inflammatory profile in the AF+ dams. This is corroborated by clinical studies demonstrating that CMV infection can lead to a bias of pro-inflammatory cytokines in the AF46. These findings indicate the presence of increased pro-inflammatory and anti-viral responses within the fetuses exposed to CMV infection in utero.
This study has several limitations. The small sample size could have impacted our statistical findings, resulting in decreased probability of detecting differences among groups, and increasing susceptibility to random variation. Larger studies will be needed to validate the predictive value of the biomarkers elucidated in this study for amniotic fluid transmission. For fetal and placental morphometric analyses, we compared the study dams to published data from a large cohort of healthy controls at the Oregon National Primate Research Center. While these controls were healthy and gestation-matched, we cannot exclude the possibility that differences in housing or population genetics contributed to the differences we observed between the cohorts. Another limitation is related to the sequencing analysis for inferring sample-level RhCMV strain frequencies and recombination events in maternal and fetal compartments. This analysis was restricted to one dam whose fetus had disseminated RhCMV infection. Future studies of viral sequences across dam and fetal anatomic compartments will enable in-depth studies of viral dynamics at the M-F interface. Lastly, the i.v. route of inoculation may lead to higher plasma viral loads compared to oral challenge or mucosal inoculation. The latter more closely mimics the natural route of CMV infection and may yield different virological and immunological outcomes.
Overall, this model of primary cCMV infection revealed new insights into the complexity of CMV vertical transmission, suggesting a larger population of newborns may be impacted by maternal primary CMV infection than previously appreciated. Given the widespread use of rhesus macaques in preclinical trials and translational research projects, our findings support their promise as a model of primary congenital CMV infection. While small animal models play a significant role in advancing cCMV research, a large animal model with more comparable immunology, placental architecture, fetal developmental stages, and AF components offers important translational advantages. The ability to longitudinally sample maternal fluids and collect M-F interface and fetal tissues provides a unique opportunity to investigate cCMV pathogenesis, identify biomarkers, and elucidate immune correlates of protection. In the future, this model could test the safety of CMV vaccine candidates, as well as their ability to protect against fetal CMV transmission and disease.
Materials and methods
Experimental design
Animals in this study are RhCMV-seronegative, immunocompetent female rhesus macaques (Macaca Mulatta) breeding dams of Indian origin housed in the expanded specific pathogen-free colony at the Tulane National Biomedical Research Center (TNBRC, Covington, La). At the start of breeding season, outdoor colony-housed dams underwent periodic screening for pregnancy by abdominal ultrasound. Upon detection of pregnancy, 12 dams (aged 2.8–9.6 years) were enrolled in the study. All animal procedures were approved by the Institutional Animal Care and Use Committee at TNBRC. Animals were cared for in accordance with the NRC Guide for the Care and Use of Laboratory Animals and the Animal Welfare Act. We have complied with all relevant ethical regulations for animal use.
Between gestation days 55–69 (mean = 61.6 days), enrolled dams were inoculated intravenously with two RhCMV strains. Pregnancies were monitored until ~21 weeks of gestation (11–12 weeks post-infection), at which point elective C-section was performed. Maternal blood was collected in EDTA vacutainer on days 0, 1, 4, 7, and then weekly until C-section. C-sections were performed at 19–22 weeks gestation (near term gestation). Saliva, urine, and AF were collected at assignment and thereafter weekly from day 0 pre-infection until C-section. Weekly ultrasounds were performed to monitor fetal biometrics. Animals were anesthetized with either intramuscular ketamine hydrochloride (10 mg/kg) or tiletamine-zolazepam (3–6 mg/kg) to facilitate physical examination and sample collection. For C-sections, dams were induced via ketamine hydrochloride then maintained on isoflurane gas inhalant anesthesia.
At C-section, maternal blood, saliva, urine and AF were collected, fetus and placenta were removed from uterus, and decidua parietalis was swabbed from the uterus with surgical gauze. The cord was clamped on both sides and severed. Cord blood was collected from the umbilical vein into EDTA vacutainer from the placental facing cord to mimic procedure in humans. After C-section, fetal blood was collected by cardiac puncture and the fetus was euthanized with ketamine via intracardiac injection immediately after. At fetal necropsy, fetal and placental morphometrics were recorded and all fetal tissues were collected for histopathological and virologic evaluation. Additionally, fetal urine was collected by cystocentesis.
Virus inoculations
Dams were intravenously inoculated with a single dose of 1 × 106 pfu RhCMV UCD52 and a single dose of 1 × 106 pfu of Full length RhCMV (FL-RhCMV) diluted in one mL of sterile PBS and administered on opposite sides of the body. RhCMV UCD52 is a low-passage clinical isolate chosen because it was previously found to be the dominant variant detected in plasma and AF following inoculation with a panel of three RhCMV variants16. The FL-RhCMV strain is a BAC-derived full-length wild-type-like RhCMV clone that was first tested for replication competency in RhCMV-seronegative male rhesus macaques and displayed in vivo characteristics of wild-type virus47. Challenge with both viruses mirrors a mix of RhCMV variants similar to natural infection with a virus swarm and allows us to address questions regarding placental transmission bottlenecks.
Sample collection and processing
Saliva, urine, AF, and PBMCs were collected weekly from each dam enrolled in the study as previously described16,17. Saliva was collected by oral saline wash, concentrated using Ultracel YM-30 (Amicon/Milipore), then aliquoted for storage at −20 °C. Urine samples were collected by clean pan catch, cellular material and debris was pelleted, and the supernatant was concentrated using Ultracel YM-30 (Amicon/Milipore), then aliquoted for storage at −20 °C. AF was collected by amniocentesis, centrifuged to remove debris, and supernatant was aliquoted for storage at −20 °C. Following plasma collection, PBMCs were isolated by ficoll separation using Lymphocyte Separation Media (LSM) (MP Biomedicals). All PBMCs were cryopreserved using serum-free freezing media Bambanker BB01 (Bulldog-Bio).
While working under sterile practice, placental tissues were harvested at C-section into cold PBS and at fetal necropsy into cold R10 media. The placenta was first processed at necropsy for top-down pictures of maternal and fetal side. In addition, sections of full-thickness placenta, cord and amniotic membrane were placed in zinc-formalin fixative and paraffin-embedded for preservation for H&E and ISH. Remaining placenta was cold transported to research lab for further processing. The primary and, if present, the secondary placenta were washed in a petri dish which was placed over wet ice with saline solution to remove maternal blood and visible blood clots. After extensive cleaning (~1 h), tissues were dissected as follows for snap freezing with liquid nitrogen. The extensive cleaning is important for both viability and to ensure tissue-bound cells are not investigated. Cord was cut in 1 cm pieces, amniotic membrane was cut in 1–2 cm2 squares from a location far from the placenta discs. The decidua layer of placenta was removed using forceps to pull of the tissue layer of decidua basalis from the maternal side of the placenta(s). Care was taken to not pull off the epithelial layer of the placenta (too deep). Sterile gauze used to wipe the uterus of both decidua parietalis and basalis at surgery was moved one by one into the lid of a petri dish and screened for decidua tissue which was moved to a separate petri dish with R10 media on wet ice. After cleaning and decidua collection, each placental disc was cut with a scalpel into a 2 × 2 cm2 away from the margin and moved to a separate round petri dish with 1X PBS. This full thickness (excluding decidua) of placenta was cut into 0.5 cm wide strips and flipped on its side. The maternal side and fetal side were dissected apart and placed in a 1.5 mL snap cap tube for snap freezing of maternal and fetal side. This was repeated for both the primary and if present also for the secondary placenta. The zone between maternal and fetal size was excluded to not risk cross-contamination. The decidua was further cleaned for any small remaining blood clots in a petri dish and media was replaced with 1X PBS to easily spot any tiny blood clots. Clean decidua pieces of about 0.5–1 cm in size were snap frozen. The remaining tissue was washed in 50 mL conical with ~40 mL of saline into a coarse metal strainer. Washed tissue was transferred with a backward rinse from the metal strainer via a funnel back into a clean 50 mL conical. This process was repeated 4X to prepare washed decidua tissue. Washed decidua was transferred back to a petri dish and resuspended with 1X PBS to cover the tissue for further dissection. Using a scalpel 3–4 mm pieces of decidua was prepared and then transferred into a 25 cm2 cell culture flask for enzymatic digestion.
Complete fetal necropsies were also performed and included sampling of 42 tissues per fetus. Collection focused on tissues with known CMV-tropism (brain, lung, kidney, cochlea). Tissues were processed for lymphocyte isolation, snap frozen for DNA extraction, and placed in zinc-formalin and processed routinely for paraffin blocks. Tissues sections were cut into 4 μm sections and mounted on charged slides prior to staining (H&E or ISH). DNA was extracted from 1–25 mg of snap-frozen tissue using DNeasy Blood and Tissue kit (Qiagen).
DNA extraction and measurement of RhCMV DNA by real-time qPCR
Qiagen Kit QIAamp DNA Blood Mini Kit (catalog# 55106) was used to extract DNA from plasma, saliva, and AF. Qiagen Kit QIAamp Viral RNA Mini Kit (catalog# 52906) was used to extract DNA from 140 μL of urine. DNA was extracted from 200 μL of plasma, then each plasma sample was eluted in 150 μL of elution buffer. DNA from AF, saliva, or urine was extracted and eluted in 100 μL of elution buffer. DNA was extracted from maternal and fetal tissues using Qiagen QIAamp Fast DNA Tissue Kit (catalog# 51404). Snap-frozen tissues were kept chilled with dry ice and dissected in a petri dish. DNA was extracted from 1 to 25 mg of snap-frozen tissue using DNeasy Blood and Tissue kit (Qiagen).
Absolute quantification of RhCMV DNA in tissues and fluids was determined by quantitative real-time PCR as previously described21,48. The Forward Primer 5′-GTTTAGGGAACCGCCATTCTG-3′, Reverse primer 5′-GTATCCGCGTTCCAATGCA-3′, and Probe 5′-FAM-TCCAGCCTCCATAGCCGGGAAGG-TAMRA-3′ added to a 25 μL reaction with Supermix Platinum Quantitative PCR SuperMix-UDG (Invitrogen). Primers and probes target conserved noncoding exon 1 region of the immediate early gene and have been used to amplify different RhCMV strains47. Reaction was performed on a 96-well plate using QuantStudio6 (ThermoFisher Scientific). To control for non-target sequence lowering efficiency of reaction, a screened cohort of RhCMV-seronegative animals PBMC’s were DNA extracted and used as seronegative rhesus genomic DNA. This DNA is screened by the same assay to confirm genomic DNA as negative. Standard curve target sequence is diluted in 3 ng/μL seronegative genomic DNA. The lower limit of detection of this assay is between one to ten RhCMV DNA copies in the PCR reaction.
Maternal plasma, urine, and saliva samples, as well as maternal or fetal tissue samples were run in six technical replicates, while AF and fetal urine samples were run in 12 technical replicates. RhCMV DNA PCR on fetal or M-F interface tissue samples showing one of six replicates positive were repeated for another six technical replicates. At least two of 12 PCR replicates scoring positive at one or more copies in the PCR reaction were required to consider RhCMV DNA positivity in AF, M-F interface tissue and fetal tissue. RhCMV DNA in plasma and AF was reported as DNA copies per mL of sample, whereas PCR data on saliva, urine and tissues was reported as DNA copies per microgram of input DNA.
Placental RhCMV burden
Following real-time qPCR of individual components of the M-F interface tissues (Fig. 2C), we calculated one PCR score for the entire M-F interface of each dam as a metric of placental RhCMV burden. To generate this score, the mean number of positive PCR reads of all M-F interface tissues were added together and divided by the number of M-F interface tissues collected from that dam. We then calculated the average PCR score of the cohort (avg PCR score = 4). By comparing individual PCR scores to the average PCR score of the cohort, six dams were categorized as PCRlo (score < 4), and six were categorized as PCRhi (score > 4). This metric was used as one of the grouping parameters to compare the effect of high vs low placental RhCMV burden on fetal crown-rump length and weight (Fig. 4B-C).
RNAscope in situ hybridization tissue pretreatment
Four um tissue sections were mounted on Superfrost Plus Microscope slides, baked for 2 h at 60 °C and passed through three changes of Xylene and three changes of 100% ethanol to remove paraffin. Slides were air dried, labeled, and loaded onto the Ventana Discovery Ultra autostainer. The assay was run using ACD RNAScope VS Universal Sample Prep and HRP Detection Reagents (Catalog# 323740 and 323210). Tissue pretreatments include Target Retrieval at 97 °C for 16 or 24 min, depending on the tissue, and protease at 37 °C for 16 min. The RhCMV and DapB probes (Catalog# 435299 and 320759) were incubated for 2 h at 43 °C. Green color development was done at the recommended time of 20 min, followed by counterstaining with hematoxylin II and bluing reagent at 16 min each. Upon completion, slides were removed and put through alternating manual washes of deionized water containing 0.1% Dawn dish soap and plain deionized water for a total of five cycles. Slides were then cleared in ethanol (80%, 95%, 100%, 100%) and three xylene changes before being permanently mounted with StatLab Acrymount mounting media. Slides were then dried overnight.
RNAScope in situ hybridization
The assay was run using ACD RNAScope VS Universal Sample Prep and HRP Detection Reagents (Catalog# 323740 and 323210) using RhCMV and DapB probes (Catalog# 435299 and 320759). The RhCMV Probe targets the ORF for rh38, rh39, and rh55. Slides were digitally imaged at 40X with a Hamamatsu NanoZoomer360. CMV ISH positive cells were counted using a deep learning algorithm (HALO AI, Indica Labs) trained and then manually checked for accuracy by a pathologist. The deep learning algorithm was trained on training set of positive and negative control slides. Annotation regions were then drawn around entire tissue sections. The deep learning algorithm identified CMV positive events, and the pathologist visually confirmed or rejected based on location, size, and staining intensity. The number of CMV positive cells were reported over the total tissue examined and expressed as CMV+ cells per cm2.
IgM serology of fetal plasma
Fetal IgM responses were assessed using fetal plasma collected at C-section. Fetal plasma was chosen over cord blood due to potential contribution of maternal blood in cord blood samples. Plasma was diluted 1:5 with sterile PBS (25 μL plasma plus 225 μL PBS) and incubated overnight in a Protein A trap plate (Cytiva Cat# 28903133) supplemented with 100 μL of Protein G agarose resin (Pierce) at 4 °C with constant agitation to remove IgG from the plasma to reduce potential background and competition for antigen binding with IgM in our assay. The trap plate was spun at 200 × g for 1 min with a 96 well round bottom plate (Corning) attached to collect the flow-through containing IgG-depleted plasma, and each well was washed once more with an equivalent volume (250 μL) of PBS. IgG-depletion was confirmed using a total IgG sandwich ELISA, using unlabeled and HRP-conjugated mouse anti-monkey IgG (Clone SB108a, Southern Biotech) for coating and detection, respectively. For detection of RhCMV-specific IgM in IgG-depleted plasma, we performed a whole virion ELISA as previously described17. Briefly, high binding 384-well clear plates (Corning) were coated overnight at 4 °C with 2000 TCID50/mL UCD52 or 8000 TCID50/mL FL- RhCMV diluted in 0.1 M sodium bicarbonate buffer (pH = 9.55). After blocking for 1–2 h at ambient temperature, we added serially diluted plasma samples and incubated for 1–2 h at ambient temperature. IgM binding was detected using a goat anti-monkey IgM mu chain-HRP antibody (Rockland cat. 617-101-007) incubated for 1 h at 1:8000. TMB substrate (TMB SureBlue, KPL) was used to develop plates for 7 min, followed by 0.1% HCl (TMB Stop, KPL) to stop the reaction, and plates were read at 450 nm on a spectrophotometer (BioTek Synergy). Results are reported as the OD450 of undiluted IgG-depleted plasma (1:10 from original plasma sample), and a positivity cutoff was established at 2 standard deviations above the mean OD450 of two control animals with RhCMV-seronegative plasma samples.
Fetal and placental measurements
Ultrasounds were performed weekly to monitor BPD and femur length using Edan Acclarix X8. Biometrics were recorded in duplicate and reported as mean mm. Gestational age was determined by sonographic measurements of the gestational sac diameter, as well as the crown-rump length. At C-section, ultrasound was performed to screen for characteristic cCMV abnormalities in brain and calcification in different organs, including brain and liver. These include periventricular calcifications, ventricular dilation, white matter gliosis, cerebral atrophy, cyst formations, abnormal sulcation, and cerebellum abnormalities. Fetal and placental weights were recorded postmortem. Fetal morphometric measures were performed with a caliper and measuring tape of the following metrics: abdominal circumference, crown rump length, head circumference, right foot, right hand, thoracic circumference, and transtemporal circumference.
Ultradeep sequencing of RhCMV
Based on viral load, we used minimum 1000 input copies for amplification and library preparation, where available. AF at 82 days PI had ~300 input copies, while plasma at 77 and 82 days PI had fewer than 100 input copies. Sample DNA was non-specifically amplified using multiple displacement amplification (MDA, Repli-g, Qiagen #150025), then purified and concentrated using Zymo Genomic DNA Clean and Concentrate kit (Zymo Research, D4011). Sample DNA was equally split across 96 wells, each containing a single primer pair to span the entire genome and PCR amplified using the pure PfuUltra II Fusion HS DNA Polymerase (Agilent #600674). Primer sequences are listed in the Supplementary Data excel file. Amplicons were pooled together then purified using QIAprep spin mini prep kit (Qiagen #27106). Using 500 ng of purified DNA, library prep was performed using NEB FS DNA library prep kit (E7805) and dual-index Illumina adapters. Libraries were run on Illumina Nextseq 2000 platform using a 200-cycle cartridge.
De-multiplexed reads with adapter sequences removed were loaded into CLC Genomics workbench and processed using a modified version of Qiagen’s SARS-CoV-2 ARTIC V3 analysis pipeline. Reads were trimmed by base quality and separately mapped to either FL-RhCMV (GCA_027929765.1) or RhCMV UCD52 (GCA_027930255.1) reference genomes. Due to limited consensus-level differences (two SNVs or indels in each reference) in the inoculation stock compared to the respective reference genomes, the published reference genomes were used as reference sequences in downstream analyses. Read mapping was refined by removing ligation artifacts, performing local realignment based on structural variant calls, removing reads with unaligned ends, and trimming bases aligning to the primer sequences at the ends of reads. Output BAM files for each sample were used in downstream analyses.
To infer strain frequencies, read depths were calculated for all samples using samtools v1.19.249 function mpileup with additional flags to filter low quality bases and allow for character parsing: --min-BQ 20, --max-depth 0, --no-output-ends, --no-output-ins, and --no-output-del. Next, each reference genome was aligned to the other, and differing positions were extracted using NucDiff v2.0.250. Outputs (ref_snps.gff) were subset to only include SNVs. Insertions, deletions, and multiple nucleotide variants (MNVs) were not considered. Filter schema is shown in Supplementary Fig. 5 and total number of remaining SNVs used for each sample-level strain frequency calculation can be found in Supplementary Table 4. Finally, strain frequencies at each remaining SNV position for each sample were calculated by dividing the number of reads with a nucleotide matching the reference genome (i.e., RhCMV UCD52 or FL-RhCMV) by total read depth at that position. Mean frequencies across all positions were also calculated for each sample. We performed the above procedure using both reference genomes.
Hypervariable regions were identified by calculating the number of SNVs within 100 bp windows across each reference genome. SNVs within regions that had >5 mean differences within 100 bps were removed to reduce the impact of reference genome mapping bias. SNVs with low coverage (<250 reads) in the non-reference, sequenced inoculum sample (e.g., sequenced FL-RhCMV inoculum mapped to RhCMV UCD52 reference genome) were also removed. To account for heterogeneity in the stocks, particularly in the passaged RhCMV UCD52 isolate, positions in each stock that had >1% frequency of the alternate stock were filtered out. In total, the filters removed 2015 of 2865 SNVs identified as differing between the two reference genomes with RhCMV UCD52 as the reference and 2000 of 2862 SNVs with FL-RhCMV as the reference. At the sample level, SNVs with coverage of <100 reads were also removed to avoid estimating strain frequencies in genomic positions with few aligned reads.
Custom scripts were generated in R Statistical Environment51 with extension packages from Comprehensive R Archive Network (CRAN; https://cran.r-project.org/), including tidyverse v2.0.052, and knitr v1.4553 to summarize the allele depth corresponding to each strain at each position, apply reference strain SNV filters to account for mapping bias, and calculate inferred strain frequencies based on the mean frequency of alleles corresponding to each reference strain at each resulting SNV position. The code for replicating these analyses is available through a public source code repository54.
Complete blood count
For each dam, whole blood was collected on days 0, 1, 7, and weekly PI until time of C-section. A pre timepoint was also collected when possible, considering colony logistics, housing acclimation period, and timing of pregnancy detected. The TNPRC clinical lab assessed the whole blood samples using a Sysmex XXN-1000v analyzer, which allows for determination of complete blood counts (CBC). This provides absolute counts of granulocytes, lymphocytes, and monocytes. Abnormal counts are reviewed by a manual differential.
Luminex
Luminex assay was used to determine cytokine levels in the maternal plasma, fetal plasma, cord blood, and AF. We used the R&D Systems NHP XL Cytokine Premixed 33-plex Panel (Cat# FCSTM21-33). EDTA plasma and AF samples were analyzed in two replicates and were prepared using a 1:2 dilution. To optimize sample dilution needed for linearity, serial dilutions was performed and 1:2 dilution in PBS was determined. Reactions were read using the Bio-Plex® 200 System (Bio-Rad Laboratories, Hercules, CA), and results were calculated on the Bio-Plex Manager™ Software (Bio-Rad) at the TNPRC Pathogen Detection and Quantification Core. Mean concentrations of replicates were plotted. We included values which were estimated based on extrapolation from the standard curve. We excluded values from wells that had a low bead count (below 50 beads) or a high %CV (above 30%).
Chemerin immunoassay
Amniotic fluid chemerin levels were measured using the quantitative sandwich enzyme immunoassay (Quantikine ELISA) by R&D Systems (Catalog# DCHM00). Before conducting the assay, we used NCBI Blast to confirm that human and Rhesus macaque chemerin (NCBI reference genome Mmul_10) have 100% homology to ensure the assay is appropriate for our model. The assay was conducted according to the manufacturer’s instructions. All samples were run in duplicate and read on a Synergy 2 (BioTek) microplate reader at 450 nm wavelength.
Statistics and reproducibility
Functional mean trajectory of each CBC panel component was smoothed via a Gaussian kernel using fdapace package in R55. Durbin test within coin package was used to test for association of time with CBC, and separately with Luminex maternal plasma data during acute phase. Statistical significance was determined via Monte-Carlo (10000 permutations). Multiple testing correction was done using FDR56 with significance set at an adjusted p value less than 0.2. For markers and analytes that demonstrated significant difference by time, we performed three and four follow up tests, respectively. CBC markers compared day 7, 21, and 84 to day zero, while analytes compared day 2, 4, 7, and 14 back to day 0 via exact Wilcoxon signed rank test using coin package in R57. Due to inconsistent timing of CBC measures at week 12, values recorded between day 81 and 84 were used for change from baseline at day 84. In these post-hoc tests, multiple testing correction was done via Holm procedure.
Global differences in fetal morphometric parameter z-scores between groups were assessed via non-parametric MANOVA (multivariate analysis of variance) using npmv package in R58. Fetal morphometric parameter z-scores were derived as gestational age-specific mean-centered and standard deviation-scaled values using published population estimates23. Missing z-scores were imputed with animal specific median z-score of observed z-score parameters. Exact Wilcoxon rank-sum tests were conducted to determine differences between groups in each morphometric parameter and for comparing PE in our cohort to gestation-comparable controls57. Binomial tests on proportions determined whether median z-scores and proportion below small for gestational age (10th percentile) of the population of macaques under study differed from the referent population for crown-rump length and fetal weight.
AUC was calculated using the standard trapezoid rule for analyzing viral loads in maternal plasma, urine, and saliva calculating cumulative viral load over different time frames. If an animal lacked a day 0 observation, they were dropped from analysis. If they lacked a day 14 observation, we carried forward the last observation. We performed a similar procedure for calculating AUC over the acute plasma Luminex data (first 14 days). We tested for differences in these AUC values as well as other Luminex data (C-section, fetal plasma, etc) by AF status via exact Wilcoxon rank sum test due to the small sample size. Multiple testing correction was done separately within each sample source/analysis (i.e., VL and acute plasma were separate corrections) with significance set at adjusted p value less than 0.2. We set data below the limit of detection to the lower limit divided by 2.
We performed PCA separately on data from fetal plasma, AUC of the maternal acute plasma, C-section, cord blood, and maternal plasma. For PCA visualization, missing values were replaced with the mean value for that analyte. Values below limit of detection were again set to the lower limit divided by 2. We scaled and centered the data prior to calculating principal components. Survival analyses comparing either placental transmission or fetal survival between immunocompetent and CD4 depleted animals was done via log-rank test using R package survival. We tested whether Spearman correlation between ISH and PCR data within animal 001-101. Exact Wilcoxon rank sum tests were performed for PE and chemerin analyses.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Source data can be obtained from supplementary data file “Supplementary Data.xlsx”. Raw sequence reads can be accessed via NCBI BioProject (Weill Cornell Medicine, Rhesus cytomegalovirus infection in pregnant rhesus macaques, NCBI BioProject, 2025, Accession: PRJNA1331192, ID: 1331192). All other data are available from the corresponding author upon reasonable request.
Code availability
Our code base is publicly available on Zenodo.org (https://doi.org/10.5281/zenodo.17193504).
References
Cannon, M. J., Schmid, D. S. & Hyde, T. B. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev. Med. Virol. 20, 202–213 (2010).
Kenneson, A. & Cannon, M. J. Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Rev. Med. Virol. 17, 253–276 (2007).
Cheeran, M. C., Lokensgard, J. R. & Schleiss, M. R. Neuropathogenesis of congenital cytomegalovirus infection: disease mechanisms and prospects for intervention. Clin. Microbiol. Rev. 22, 99–126 (2009).
Manicklal, S., Emery, V. C., Lazzarotto, T., Boppana, S. B. & Gupta, R. K. The “silent” global burden of congenital cytomegalovirus. Clin. Microbiol. Rev. 26, 86–102 (2013).
Permar, S. R., Schleiss, M. R. & Plotkin, S. A. Advancing our understanding of protective maternal immunity as a guide for development of vaccines to reduce congenital cytomegalovirus infections. J. Virol. 92, https://doi.org/10.1128/JVI.00030-18.(2018).
Scarpini, S. et al. Development of a vaccine against human cytomegalovirus: advances, barriers, and implications for the clinical practice. Vaccines 9, https://doi.org/10.3390/vaccines9060551 (2021).
Britt, W. J. Congenital human cytomegalovirus infection and the enigma of maternal immunity. J. Virol. 91, https://doi.org/10.1128/JVI.02392-16 (2017).
Boppana, S. B., Rivera, L. B., Fowler, K. B., Mach, M. & Britt, W. J. Intrauterine transmission of cytomegalovirus to infants of women with preconceptional immunity. N. Engl. J. Med. 344, 1366–1371 (2001).
Hansen, S. G. et al. Evasion of CD8+ T cells is critical for superinfection by cytomegalovirus. Science 328, 102–106 (2010).
Meyer-Konig, U., Ebert, K., Schrage, B., Pollak, S. & Hufert, F. T. Simultaneous infection of healthy people with multiple human cytomegalovirus strains. Lancet 352, 1280–1281 (1998).
Barry, P. A. et al. Nonhuman primate models of intrauterine cytomegalovirus infection. ILAR J. 47, 49–64 (2006).
de Rijk, E. P. C. T. & Van Esch, E. The macaque placenta-a mini-review. Toxicol. Pathol. 36, 108s–118s (2008).
Mostrom, M. J. et al. Immune profile of the normal maternal-fetal interface in rhesus macaques and its alteration following zika virus infection. Front. Immunol. 12, 719810 (2021).
Powers, C. & Fruh, K. Rhesus CMV: an emerging animal model for human CMV. Med. Microbiol. Immunol. 197, 109–115 (2008).
London, W. T. et al. Experimental congenital disease with simian cytomegalovirus in rhesus monkeys. Teratology 33, 323–331 (1986).
Bialas, K. M. et al. Maternal CD4+ T cells protect against severe congenital cytomegalovirus disease in a novel nonhuman primate model of placental cytomegalovirus transmission. Proc. Natl. Acad. Sci. USA 112, 13645–13650 (2015).
Nelson, C. S. et al. Preexisting antibodies can protect against congenital cytomegalovirus infection in monkeys. JCI Insight 2, https://doi.org/10.1172/jci.insight.94002 (2017).
Antoine, P. et al. Postnatal acquisition of primary rhesus cytomegalovirus infection is associated with prolonged virus shedding and impaired CD4+ T lymphocyte function. J. Infect. Dis. 210, 1090–1099 (2014).
Rawlinson, W. D. et al. Congenital cytomegalovirus infection in pregnancy and the neonate: consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect. Dis. 17, e177–e188 (2017).
Leber, A. L. Maternal and congenital human cytomegalovirus infection: laboratory testing for detection and diagnosis. J. Clin. Microbiol. 62, e0031323 (2024).
Mostrom, M. J. et al. Protective effect of pre-existing natural immunity in a nonhuman primate reinfection model of congenital cytomegalovirus infection. PLoS Pathog. 19, e1011646 (2023).
Tarantal, A. F. Ultrasound imaging in rhesus (Macaca mulatta) and long-tailed (Macaca fascicularis) macaques: reproductive and research applications. in The Laboratory Primate (Academic Press, 2005).
Roberts, V. H. J. et al. Rhesus macaque fetal and placental growth demographics: a resource for laboratory animal researchers. Am. J. Primatol. 85, e23526 (2023).
Vorontsov, O. et al. Amniotic fluid biomarkers predict the severity of congenital cytomegalovirus infection. J. Clin. Investig. 132, https://doi.org/10.1172/JCI157415 (2022).
Gabrielli, L. et al. Congenital cytomegalovirus infection: patterns of fetal brain damage. Clin. Microbiol. Infect. 18, E419–E427 (2012).
Carraro, M. et al. Cytomegalovirus (CMV) infection causes degeneration of cochlear vasculature and hearing loss in a mouse model. J. Assoc. Res. Otolaryngol. 18, 263–273 (2017).
Keithley, E. M., Woolf, N. K. & Harris, J. P. Development of morphological and physiological changes in the cochlea induced by cytomegalovirus. Laryngoscope 99, 409–414 (1989).
Fernandez-Alarcon, C. et al. Impairment in neurocognitive function following experimental neonatal guinea pig cytomegalovirus infection. Pediatr. Res. 89, 838–845 (2021).
Piccirilli, G. et al. Fetal brain damage in human fetuses with congenital cytomegalovirus infection: histological features and viral tropism. Cell Mol. Neurobiol. 43, 1385–1399 (2023).
Dreher, A. M. et al. Spectrum of disease and outcome in children with symptomatic congenital cytomegalovirus infection. J. Pediatr. 164, 855–859 (2014).
Lipitz, S. et al. Outcome of pregnancies with vertical transmission of primary cytomegalovirus infection. Obstet. Gynecol. 100, 428–433 (2002).
Malinger, G. et al. Fetal cytomegalovirus infection of the brain: the spectrum of sonographic findings. Am. J. Neuroradiol. 24, 28–32 (2003).
Gilbert, W. M., Eby-Wilkens, E. & Tarantal, A. F. The missing link in rhesus monkey amniotic fluid volume regulation: intramembranous absorption. Obstet. Gynecol. 89, 462–465 (1997).
Ruellan-Eugene, G. et al. Evaluation of virological procedures to detect fetal human cytomegalovirus infection: avidity of IgG antibodies, virus detection in amniotic fluid and maternal serum. J. Med. Virol. 50, 9–15 (1996).
Underwood, M. A., Gilbert, W. M. & Sherman, M. P. Amniotic fluid: not just fetal urine anymore. J. Perinatol. 25, 341–348 (2005).
Kumazaki, K. et al. Detection of cytomegalovirus DNA in human placenta. J. Med. Virol. 68, 363–369 (2002).
McDonagh, S., Maidji, E., Chang, H. T. & Pereira, L. Patterns of human cytomegalovirus infection in term placentas: a preliminary analysis. J. Clin. Virol. 35, 210–215 (2006).
McDonagh, S. et al. Viral and bacterial pathogens at the maternal-fetal interface. J. Infect. Dis. 190, 826–834 (2004).
Paradowska, E. et al. Detection of cytomegalovirus in human placental cells by polymerase chain reaction. APMIS 114, 764–771 (2006).
Yinon, Y., Farine, D. & Yudin, M. H. Screening, diagnosis, and management of cytomegalovirus infection in pregnancy. Obstet. Gynecol. Surv. 65, 736–743 (2010).
Guerra, B. et al. Prenatal diagnosis of symptomatic congenital cytomegalovirus infection. Am. J. Obstet. Gynecol. 183, 476–482 (2000).
Vera Cruz, D. et al. Intrahost cytomegalovirus population genetics following antibody pretreatment in a monkey model of congenital transmission. PLoS Pathog. 16, e1007968 (2020).
Kawamura, K. et al. Brain-derived neurotrophic factor promotes implantation and subsequent placental development by stimulating trophoblast cell growth and survival. Endocrinology 150, 3774–3782 (2009).
Mayeur, S. et al. Do neurotrophins regulate the feto-placental development?. Med. Hypotheses 76, 726–728 (2011).
Christian, L. M., Mitchell, A. M., Gillespie, S. L. & Palettas, M. Serum brain-derived neurotrophic factor (BDNF) across pregnancy and postpartum: associations with race, depressive symptoms, and low birth weight. Psychoneuroendocrinology 74, 69–76 (2016).
Scott, G. M. et al. Cytomegalovirus infection during pregnancy with maternofetal transmission induces a proinflammatory cytokine bias in placenta and amniotic fluid. J. Infect. Dis. 205, 1305–1310 (2012).
Taher, H. et al. In vitro and in vivo characterization of a recombinant rhesus cytomegalovirus containing a complete genome. PLoS Pathog. 16, e1008666 (2020).
Kaur, A. et al. Direct relationship between suppression of virus-specific immunity and emergence of cytomegalovirus disease in simian AIDS. J. Virol. 77, 5749–5758 (2003).
Danecek, P. et al. Twelve years of SAMtools and BCFtools. Gigascience 10, https://doi.org/10.1093/gigascience/giab008 (2021).
Khelik, K., Lagesen, K., Sandve, G. K., Rognes, T. & Nederbragt, A. J. NucDiff: in-depth characterization and annotation of differences between two sets of DNA sequences. BMC Bioinform. 18, 338 (2017).
RC, T. R.: A Language and Environment for Statistical Computing, R Foundation for Statistical Computing https://www.R-project.org/ (2023).
Wickham, H. et al. Welcome to the tidyverse. J. Open Source Softw. https://doi.org/10.21105/joss.01686 (2019).
Y, X. knitr: A General-Purpose Package for Dynamic Report Generation in R, vR package version 1.45. https://yihui.org/knitr/ (2023).
“A rhesus macaque model of congenital cytomegalovirus infection reveals a spectrum of vertical transmission outcomes” Manuel et al. Communications Biology (git commit 891b9b3). (Zenodo, 2025). https://doi.org/10.5281/zenodo.17193504 (2025).
Zhou, Y. et al. fdapace: functional data analysis and empirical dynamics. R package version 0.5.9. https://CRAN.R-project.org/package=fdapace (2022).
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. 57, 289–300 (1995).
Hothorn, T., Hornik, K., van de Wiel, M. A. & Zeileis, A. A Lego system for conditional inference. Am. Stat. 60, 257–263 (2006).
Woodrow Burchett, W., Amanda Ellis, R., Solomon Harrar, W. & Arne Bathke, C. Nonparametric inference for multivariate data: the R package npmv. J. Stat. Softw. 76, 1–18 (2017).
Acknowledgements
The authors acknowledge the Veterinary Medicine staff at the Tulane National Biomedical Research Center (TNBRC) for their expert care of the animals, and the following TNBRC Core services: Clinical Pathology Core (RRID:SCR_024609) for complete blood count analysis; Anatomic Pathology Core (RRID:SCR_024606) and Confocal Microscopy and Molecular Pathology Core (RRID:SCR_024613) for histopathology, image analysis and RNAScope services; and the Pathogen Detection and Quantification Core for performing and reading Luminex assays (RRID:SCR_024614). This study was funded by National Institutes of Health grant P01 AI129859, TNBRC Base Grant P51OD011104 (RRID: SCR_008167), and National Institutes of Health grant S10 OD026800.
Author information
Authors and Affiliations
Contributions
T.D.M. and M.J.M. developed the experimental model and performed experiments. Conceptualization: T.D.M., M.J.M., D.M., K.F., S.R.P., R.V.B., A.K. Methodology: T.D.M., M.J.M., C.M.C., R.V.B., A.K. Validation: T.D.M., M.J.M., E.A.S., C.M.C., M.R.L., L.W.R., A.M., T.F.K., R.B., A.D. Formal analysis and interpretation: T.D.M., M.J.M., E.A.S., R.V.B., R.B., A.D., C.C., M.R.L., L.W.R., J.G., S.L., C.E.O. Investigation: T.D.M., M.J.M., E.A.S., S.K., M.E.T., F.A.B., L.M.S., L.M., C.E.O., C.C.M., A.M., R.V.B. Data Curation: T.D.M., M.J.M., S.K., E.A.S., R.V.B., R.B., A.D., C.M.C., A.M. Writing—original draft preparation: T.D.M., R.V.B., A.K. Writing—review and editing: All authors. Visualization: T.D.M., M.J.M., C.M.C., C.E.O., A.D., R.B., R.V.B. Resources: M.N.S., V.W.D., L.A.D.M., D.M., K.F., R.B., A.D., C.C., C.M.C., M.R.L., L.W.R., J.G., K.O., S.L. Supervision: K.F., T.F.K., C.C., S.R.P., A.K. Project Administration: T.D.M., M.J.M., E.A.S., A.K. Funding Acquisition: K.F., S.R.P., A.K.
Corresponding author
Ethics declarations
Competing interests
The authors declare the following competing interests: S.R.P. provides individual consulting services to Moderna, Merck, Dynavax, Pfizer, GlaxoSmithKline, and Imunon, (for vaccines). Dynavax, Pfizer, and Moderna have provided grants for her Institutional sponsored programs. OHSU and K Früh have a financial interest in Vir Biotechnology, Inc., a company that may have a commercial interest in the results of this research and technology. This potential conflict of interest has been reviewed and managed by OHSU. All other authors declare no competing interests.
Peer review
Peer review information
Communications Biology thanks the anonymous reviewers for their contribution to the peer review of this work. Primary Handling Editor: Dario Ummarino. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Manuel, T.D., Moström, M.J., Crooks, C.M. et al. A rhesus macaque model of congenital cytomegalovirus infection reveals a spectrum of vertical transmission outcomes. Commun Biol 8, 1647 (2025). https://doi.org/10.1038/s42003-025-09033-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s42003-025-09033-4
