
Abstract
Chimeric antigen receptor (CAR) T cell therapy for solid tumors remains challenging. This phase 1, open-label, dose-escalation and expansion study (ClinicalTrials.gov registration: NCT05396300) evaluated the safety and efficacy of PC13, a hypoxia-responsive, carcinoembryonic antigen (CEA)-targeted CAR T cell therapy, in persons with CEA-positive solid tumors. The primary endpoint was safety; secondary endpoints included efficacy, pharmacokinetics and pharmacodynamics. A total of 43 heavily pretreated participants (46.5% with ≥4 prior lines) were assigned to receive PC13 through intraperitoneal (I.P., n = 17) or intravenous (I.V., n = 26) infusion on the basis of predominant metastatic sites. Grade 3 diarrhea occurred in 20.9% of participants and 76.7% experienced grade 1 or 2 cytokine release syndrome. Disease control rates were 82.4% in the I.P. group and 68.0% in the I.V. group, with objective response rates (ORRs) of 23.5% and 8.0%, respectively. In post hoc analyses, ORRs reached 57.1% (4/7) in the I.P. group with peritoneal metastases and 40.0% (2/5) in the I.V. group without liver metastases, both among participants with CEA immunohistochemistry expression ≥ 90%. The predefined safety endpoint was met. PC13 demonstrated manageable toxicity and promising efficacy, supporting further investigations.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$32.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

Data availability
The study protocol is available in Supplementary Information. As this was a clinical trial involving participant data, individual deidentified participant data (including baseline characteristics, safety, efficacy and pharmacokinetic parameters) underlying the results reported in this article are not publicly available to protect participant privacy in accordance with ethical regulations and informed consent agreements. These data can be made available upon request for academic, noncommercial research purposes. The oligonucleotide sequences used in this study are provided within Methods. Any further information regarding reagents or resources is available upon reasonable request.
Requests for data access should be directed to W.F. Proposals will be reviewed by the Department of Medical Oncology (FAHZU) and the study collaborator, Chongqing Precision Biotech, to determine whether any intellectual property or confidentiality obligations apply. Requestors will be asked to sign a data access agreement. A response to requests is typically provided within 30 days. Source data are provided with this paper.
References
Grupp, S. A. et al. Chimeric antigen receptor-modified T cells for acute lymphoid leukemia. N. Engl. J. Med. 368, 1509–1518 (2013).
Schuster, S. J. et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N. Engl. J. Med. 380, 45–56 (2019).
Albelda, S. M. CAR T cell therapy for patients with solid tumours: key lessons to learn and unlearn. Nat. Rev. Clin. Oncol. 21, 47–66 (2024).
Li, D. et al. EpCAM-targeting CAR-T cell immunotherapy is safe and efficacious for epithelial tumors. Sci. Adv. 9, eadg9721 (2023).
Qi, C. et al. Safety and efficacy of CT041 in patients with refractory metastatic pancreatic cancer: a pooled analysis of two early-phase trials. J. Clin. Oncol. 42, 2565–2577 (2024).
Han, Z. W. et al. The old CEACAMs find their new role in tumor immunotherapy. Invest. New Drugs 38, 1888–1898 (2020).
Holzinger, A. & Abken, H. CAR T cells targeting solid tumors: carcinoembryonic antigen (CEA) proves to be a safe target. Cancer Immunol. Immunother. 66, 1505–1507 (2017).
Lakemeyer, L. et al. Diagnostic and prognostic value of CEA and CA19-9 in colorectal cancer. Diseases 9, 21 (2021).
Zhang, C. et al. Phase I escalating-dose trial of CAR-T therapy targeting CEA+ metastatic colorectal cancers. Mol. Ther. 25, 1248–1258 (2017).
Katz, S. C. et al. Phase I hepatic immunotherapy for metastases study of intra-arterial chimeric antigen receptor-modified T-cell therapy for CEA+ liver metastases. Clin. Cancer Res. 21, 3149–3159 (2015).
Thistlethwaite, F. C. et al. The clinical efficacy of first-generation carcinoembryonic antigen (CEACAM5)-specific CAR T cells is limited by poor persistence and transient pre-conditioning-dependent respiratory toxicity. Cancer Immunol. Immunother. 66, 1425–1436 (2017).
Ye, Y. et al. Characterization of hypoxia-associated molecular features to aid hypoxia-targeted therapy. Nat. Metab. 1, 431–444 (2019).
Chen, Z., Han, F., Du, Y., Shi, H. & Zhou, W. Hypoxic microenvironment in cancer: molecular mechanisms and therapeutic interventions. Signal. Transduct. Target. Ther. 8, 70 (2023).
Zhu, X. et al. Hypoxia-responsive CAR-T cells exhibit reduced exhaustion and enhanced efficacy in solid tumors. Cancer Res. 84, 84–100 (2024).
Kosti, P. et al. Hypoxia-sensing CAR T cells provide safety and efficacy in treating solid tumors. Cell Rep. Med. 2, 100227 (2021).
He, H. et al. Conditioned CAR-T cells by hypoxia-inducible transcription amplification (HiTA) system significantly enhances systemic safety and retains antitumor efficacy. J Immunother. Cancer 9, e002755 (2021).
Sagnella, S. M. et al. Locoregional delivery of CAR-T cells in the clinic. Pharmacol. Res. 182, 106329 (2022).
Cherkassky, L., Hou, Z., Amador-Molina, A. & Adusumilli, P. S. Regional CAR T cell therapy: an ignition key for systemic immunity in solid tumors. Cancer Cell 40, 569–574 (2022).
Katz, S. C. et al. Regional CAR-T cell infusions for peritoneal carcinomatosis are superior to systemic delivery. Cancer Gene Ther 23, 142–148 (2016).
Vitanza, N. A. et al. Locoregional infusion of HER2-specific CAR T cells in children and young adults with recurrent or refractory CNS tumors: an interim analysis. Nat. Med. 27, 1544–1552 (2021).
Kepenekian, V. et al. Advances in the management of peritoneal malignancies. Nat. Rev. Clin. Oncol. 19, 698–718 (2022).
Qian, S. et al. Intraperitoneal administration of carcinoembryonic antigen-directed chimeric antigen receptor T cells is a robust delivery route for effective treatment of peritoneal carcinomatosis from colorectal cancer in pre-clinical study. Cytotherapy 26, 113–125 (2024).
Parkhurst, M. R. et al. T cells targeting carcinoembryonic antigen can mediate regression of metastatic colorectal cancer but induce severe transient colitis. Mol. Ther. 19, 620–626 (2011).
Wei, J. et al. The model of cytokine release syndrome in CAR T-cell treatment for B-cell non-Hodgkin lymphoma. Signal. Transduct. Target. Ther. 5, 134 (2020).
Haas, A. R. et al. Two cases of severe pulmonary toxicity from highly active mesothelin-directed CAR T cells. Mol. Ther. 31, 2309–2325 (2023).
Grothey, A. et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 381, 303–312 (2013).
Mayer, R. J. et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N. Engl. J. Med. 372, 1909–1919 (2015).
Dasari, A. et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): an international, multicentre, randomised, double-blind, phase 3 study. Lancet 402, 41–53 (2023).
Li, J. et al. Randomized, double-blind, placebo-controlled phase III trial of apatinib in patients with chemotherapy-refractory advanced or metastatic adenocarcinoma of the stomach or gastroesophageal junction. J. Clin. Oncol. 34, 1448–1454 (2016).
Shitara, K. et al. Trifluridine/tipiracil versus placebo in patients with heavily pretreated metastatic gastric cancer (TAGS): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 19, 1437–1448 (2018).
Fan, A. et al. Immunotherapy in colorectal cancer: current achievements and future perspective. Int. J. Biol. Sci. 17, 3837–3849 (2021).
Katz, S. C. et al. HITM-SIR: phase Ib trial of intraarterial chimeric antigen receptor T-cell therapy and selective internal radiation therapy for CEA+ liver metastases. Cancer Gene Ther. 27, 341–355 (2020).
Katz, S. C. et al. HITM-SURE: hepatic immunotherapy for metastases phase Ib anti-CEA CAR-T study utilizing pressure enabled drug delivery. J. Immunother. Cancer 8, e001097 (2020).
Majzner, R. G. & Mackall, C. L. Tumor antigen escape from CAR T-cell therapy. Cancer Discov 8, 1219–1226 (2018).
Roerden, M. & Spranger, S. Cancer immune evasion, immunoediting and intratumour heterogeneity. Nat. Rev. Immunol. 25, 353–369 (2025).
Goéré, D. et al. The differential response to chemotherapy of ovarian metastases from colorectal carcinoma. Eur. J. Surg. Oncol. 34, 1335–1339 (2008).
Ursem, C. et al. Clinicopathologic characteristics and impact of oophorectomy for ovarian metastases from colorectal cancer. Oncologist 25, 564–571 (2020).
Prager, G. W. et al. Trifluridine–tipiracil and bevacizumab in refractory metastatic colorectal cancer. N. Engl. J. Med. 388, 1657–1667 (2023).
Schulz, K. F., Altman, D. G. & Moher, D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. Brit. Med. J. 340, c332 (2010).
Wolff, A. C. et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline focused update. J. Clin. Oncol. 36, 2105–2122 (2018).
Kalos, M. et al. T cells with chimeric antigen receptors have potent antitumor effects and can establish memory in patients with advanced leukemia. Sci. Transl. Med. 3, 95ra73 (2011).
Acknowledgements
We sincerely thank all participants and their families for their participation in this trial, as well as all colleagues involved. This study was sponsored by Chongqing Precision Biotech. The sponsor provided manufacturing and quality control of the PC13 CAR T cell product used in this study and supplied cellular product-related data. This work was additionally supported by the National Natural Science Foundation of China (NSFC; 82373428 and 52233013, to W.F.), the National Key R&D Program of China (2022YFC3401600, to C.Q.), the Major International (Regional) Joint Research Project of the NSFC (82120108019, to C.Q.), the Special Fund for Clinical Research from Chongqing Precision Biotech (R1801, to C.Q.), the Special Fund for Research on National Major Research Instruments of the NSFC (82127804, to Z.Y.) and the Science and Technology Innovation Key R&D Program of Chongqing (CSTB2021TIAD-KPX0068, to Z.Y.). The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Study design: C.Q., Z.Y., S.Q. and W.F. CAR T cell production: Z.Y., Y.L., L.W., J.S. and Q.Z. Participant enrollment and treatment: Y.G., H.Z., X.Z., L.H., Q.F., X.B., Z.T., B.L., Y. Zheng, L.L., P.Z. and W.F. Data collection: Y.G., J.L., H.Z., Y. Zhang, X.H. and C.Y. Data analysis and interpretation: Y.G., J.L., H.Z., Z.Y., L.H., X.B., B.L. and L.X. Paper drafting: Y.G., J.L., H.Z., Z.Y. and W.F. Y.G., J.L., H.Z., Y. Zhang, S.Q., X.Z., L.H., L.X., Q.F., X.B., Z.T., Y.L., B.L., L.W., J.S., Q.Z., X.H., Y. Zheng, C.Y., L.L., P.Z., P.V.C., Z.Y., C.Q. and W.F. reviewed and revised the paper. All authors approved the final paper and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Competing interests
Z.Y., L.W., Y.L., Y. Zhang, Q.Z., J.S., X.H., C.Y. and C.Q. are employees of Chongqing Precision Biotech. The other authors declare no competing interests.
Peer review
Peer review information
Nature Cancer thanks Iosune Baraibar, Chongyang Duan, Adam Snook and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Structure of the PC13 CAR construct.
The chimeric antigen receptor (CAR) consists of a humanized scFv directed against the A3 domain of CEACAM5, fused to a BBZ signaling domain (4-1BB co-stimulation and CD3ζ activation). Its expression is driven by five upstream hypoxia-responsive elements (HREs). Under normoxic conditions, HIF-1α protein is rapidly degraded, preventing efficient initiation of CAR gene transcription. Consequently, CAR expression might remain minimal in both circulating T cells and those infiltrating healthy tissues. In contrast, under hypoxic conditions within the tumor microenvironment, HIF-1α stabilization might mediate robust CAR upregulation, leading to rapid surface expression and localized cytotoxic activity.
Extended Data Fig. 2 Serum biomarker fold change in relation to CRS occurrence.
Correlation between post-infusion (a) IL-6 and (b) CRP fold change and CRS occurrence in the I.P. and I.V. groups. In each boxplot, the central line represents the median, the box edges represent the interquartile range (IQR, 25th–75th percentile), and the whiskers extend to 1.5 × IQR. Statistical comparisons were performed using two‑sided Wilcoxon rank‑sum tests; no adjustment for multiple comparisons was applied. Abbreviations: CRS, cytokine release syndrome; I.P., intraperitoneal infusion; I.V., intravenous infusion; CRP, C-reactive protein; DL1, dose level 1; DL2, dose level 2; DL3, dose level 3; DL4, dose level 4.
Extended Data Fig. 3 Detection of PC13 CAR T cells in colonic biopsies of patients with immune-mediated colitis.
a, Representative IHC images of colonic biopsy tissues from the I.P. group, stained for CD3 and the PC13 CAR (40× magnification). qPCR analysis of CAR transgene copy numbers in colitis biopsy samples and paired peripheral blood from (b) Patient 028 and (c) Patient 029. Due to the limited size of each clinical biopsy, IHC was performed once per patient. Abbreviations: IHC, immunohistochemistry; I.P., intraperitoneal infusion; qPCR, quantitative real-time polymerase chain reaction.
Extended Data Fig. 4 Clinical management workflow for diarrhea following PC13 CAR T cell infusion.
This workflow guides the assessment and intervention for diarrhea, commencing with a pre-infusion risk evaluation for colitis.
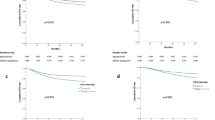
Extended Data Fig. 5 Subgroup analysis of survival outcomes.
Kaplan-Meier curves illustrate PFS and OS stratified by different variables. Survival by the best overall response to therapy in I.P. group (a-b) and I.V. group (g-h). Survival by baseline serum CEA level (high vs. low) (c-d) and primary tumor type (CRC vs. non-CRC) (e-f) in I.P. group. Survival by CEA IHC expression (≥90% vs. <90%) (i-j) and liver metastases (without liver metastases vs. with liver metastases) (k-l) in I.V. group. Between-group survival differences were compared using the log-rank test. For comparisons where Kaplan-Meier curves crossed (indicating non-proportional hazards), the Breslow and Tarone-Ware tests were additionally applied. Abbreviations: I.P., intraperitoneal infusion; I.V., intravenous infusion; PFS, progression-free survival; OS, overall survival; PR, partial response; SD, stable disease; PD, progressive disease; CI, confidence interval; NE, not estimable; CRC, colorectal cancer; IHC, immunohistochemistry.
Extended Data Fig. 6 Survival analysis stratified by RAS mutation status and primary tumor sidedness within the CRC cohort.
Kaplan-Meier curves for PFS and OS stratified by RAS mutation status (mutant vs. wild-type) in the I.P. (a-b) group and I.V. (e-f) group within the CRC cohort. Kaplan-Meier curves for PFS and OS stratified by primary tumor sidedness (left vs. right) in the I.P. (c-d) and I.V. (g-h) groups within the CRC cohort. Between-group survival differences were compared using the log-rank test. For comparisons where Kaplan-Meier curves crossed (indicating non-proportional hazards), the Breslow and Tarone-Ware tests were additionally applied. Abbreviations: CRC, colorectal cancer; I.P., intraperitoneal infusion; I.V., intravenous infusion; PFS, progression-free survival; OS, overall survival; NR, not reached.
Extended Data Fig. 7 Subgroup analyses for ORR and DCR.
ORR and DCR with 95% CIs in I.P. group (a-b) and I.V. group (c-d). In each plot, the point estimate (square) denotes the ORR or DCR for that subgroup, and the horizontal line represents the 95% CI, calculated using the Clopper-Pearson exact method. The vertical dashed line indicates the overall ORR or DCR for the entire I.P. or I.V. group. The selected subgroup in I.P. group was characterized by CEA IHC expression ≥90% and with peritoneal metastases. The selected subgroup in I.V. group was characterized by CEA IHC expression ≥90% and without liver metastases. Abbreviations: ORR, objective response rate; DCR, disease control rate; CI, confidence interval; CRC, colorectal cancer; I.P., intraperitoneal infusion; I.V., intravenous infusion; IHC, immunohistochemistry; FC, fludarabine and cyclophosphamide; DL1, dose level 1; DL2, dose level 2; DL3, dose level 3; DL4, dose level 4; G-CSF, granulocyte colony-stimulating factor.
Extended Data Fig. 8 Flow cytometry analysis of PC13 CAR T cell phenotype.
Phenotypic characterization of the PC13 CAR T cell product was performed using flow cytometry. Panels A–F show representative flow cytometry plots. a, CAR expression analysis by flow cytometry. b, CD4+ and CD8+ subset distribution. c, Memory subset distribution (stem cell memory [scm], central memory [cm], effector [ef], effector memory [em]). Exhaustion marker profiling, including LAG-3 (d), PD-1 (e), and TIM-3(f). Panels G–I present summary statistics. g, Percentage of CAR+ cells within total CD3⁺ T cells, CD4+, and CD8+subsets. h, Quantification of memory subsets, including relative frequencies of Tscm, Tcm, Tef, Tem. i, Percentage of LAG3+, PD-1+, TIM-3+ cells. Exhaustion panel n = 37 due to insufficient samples in 6 patients. In each boxplot, the central line represents the median, the box edges represent the interquartile range (IQR, 25th–75th percentile), and the whiskers extend to 1.5 × IQR. Each dot represents an individual patient’s PC13 CAR T cell product.
Extended Data Fig. 9 Distribution of PC13 CAR T cells and cytokines in body fluids from representative patients.
Tracking of CAR transgene copies and cytokines in peripheral blood and ascites from two representative patients, 003 (a-e) and 040 (f-j), in the I.P. group. Detection of CAR transgene copies in peripheral blood, ascites, and pleural effusion from three patients, 005 (k), 030 (l), and 045 (m) in the I.V. group. CAR transgene levels were quantified by qPCR. Abbreviations: I.P., intraperitoneal infusion; I.V., intravenous infusion; qPCR, quantitative real-time polymerase chain reaction.
Extended Data Fig. 10 Reference examples for CEA immunohistochemistry staining intensity scoring.
Representative micrographs are shown to define the scoring criteria for intense, moderate, and weak CEA staining intensity, as used throughout the study. These images serve as a visual reference and are not derived from a repeated experimental series.
Supplementary information
Supplementary Information (download PDF )
Supplementary Fig. 1 and clinical trial protocol.
Supplementary Tables 1–7 (download XLSX )
Supplementary Tables 1–7.
Supplementary Data (download PDF )
CONSORT 2010 checklist.
Source data
Source Data Figs. 2 and 4 and Extended Data Figs. 2, 3 and 5–9 (download XLSX )
Statistical source data.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gao, Y., Li, J., Zhang, H. et al. Hypoxia-responsive CEA-targeted CAR T cells in CEA-positive solid tumors through intraperitoneal or intravenous infusion: a phase 1 trial. Nat Cancer 7, 608–621 (2026). https://doi.org/10.1038/s43018-026-01124-3
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s43018-026-01124-3
