
Abstract
Aging populations face increasing incidence of neurological disorders, including Alzheimer’s disease (AD) and late-onset epilepsy (LOE), which demonstrate a bidirectional relationship where AD is a risk factor for LOE and LOE is a risk factor for AD. While the APOE gene is a known shared risk factor, comprehensive genetic studies for LOE remain limited. This study employed a multi-task learning framework using Elastic Net modeling to systematically identify shared genetic risk factors between AD and LOE. We analyzed electronic health records from UCLA Health System (N = 416,212; genetic subset N = 16,500) and validated findings in the All of Us dataset (N = 52,493). Longitudinal analyses confirmed strong bidirectional associations between AD and LOE. The multi-task learning approach identified eight shared-risk single nucleotide polymorphisms mapping to key genes including the APOE-TOMM40-APOC1 cluster, BIN1, CLU, PVRL2, and TRAPPC6A. These shared-risk genes were enriched in pathways related to lipid metabolism, amyloid catabolic processes, and tau protein binding. A shared genetic risk score effectively stratified patients into distinct AD-LOE risk groups. This study represents an initial systematic identification of potential shared genetic factors between AD and LOE using multi-task learning. While our findings suggest possible shared genetic contributions, particularly in the APOE region, and highlight tau-mediated mechanisms as potential therapeutic targets, further validation is needed to establish the extent of genetic overlap between these conditions.
Similar content being viewed by others


Introduction
Aging represents a global demographic phenomenon that poses significant challenges to healthcare systems and societies worldwide. As populations age, the incidence of age-related neurological disorders increases substantially, including Alzheimer’s disease (AD) and late-onset epilepsy (LOE). AD is a progressive neurodegenerative disease that impairs memory, cognition, and the ability to perform activities of daily living. It is the leading cause of dementia, accounting for approximately 60–80% of all dementia cases1. Currently, over six million Americans live with AD, and one in three seniors dies with AD or related dementia2. The economic burden of caring for individuals with AD is projected to reach $1 trillion annually in the United States by 20502. LOE, characterized by recurrent unprovoked seizures with onset at age 60 or older, also becomes increasingly prevalent with advancing age, with an incidence estimated at 80 to 102 cases per 100,000 people over 60 years of age3,4,5.
Extensive research from animal models to large epidemiologic studies has established a bidirectional relationship between AD and LOE. Individuals with AD demonstrate a two- to four-fold increased risk of developing epilepsy, with a significant proportion experiencing their first seizure concurrently with, or several years preceding, the onset of cognitive decline6. Conversely, LOE is associated with a two- to three-fold increased risk of developing dementia7. Clinical studies vary widely but report that around 20% of AD patients experience seizures during follow-up periods, with seizure onset occurring at any stage of disease progression8,9. Supporting this clinical evidence, many mouse models of AD develop seizures and epileptiform spiking in early stages of the disease, prior to the deposition of disease-related proteins and onset of cognitive decline10. Moreover, patients with clinical and subclinical epileptiform activity tend to develop AD at younger ages and experience more rapid cognitive decline compared to those without epilepsy11,12. An emerging hypothesis proposes the existence of an epileptic prodromal variant of AD, in which development of LOE represents the first clinical symptom of AD in a subset of patients and serves as a harbinger for subsequent cognitive decline13. While this association may arise from multiple factors including shared pathophysiological mechanisms, neuroinflammation, and structural brain changes14, the present study focuses specifically on the genetic underpinnings of this relationship.
While large-scale genome-wide association studies (GWASs) have successfully identified numerous common genetic risk factors for AD, including the prominent apolipoprotein E (APOE) gene15, there are no GWAS studies for LOE. This gap in the literature limits the ability to examine shared genetic risk factors between AD and LOE using established cross-trait meta-analysis methods such as conjunctional false discovery rate16 or cross-trait linkage disequilibrium score regression (LDSC)17, which are designed to estimate genetic correlations and identify shared loci between related conditions.
To date, shared genetic risk factors between AD and LOE have been identified primarily through observational studies, with APOE serving as the most extensively characterized. Carriers of the APOE-ε4 allele demonstrate a 1.4–2.1-fold increased risk of developing LOE compared to non-carriers18,19. Additionally, APOE-ε4 allele carriers exhibit greater susceptibility to postictal confusion20. However, a comprehensive characterization of the shared genetic architecture between AD and LOE, including both the well-established APOE region and additional genetic factors, remains lacking. The extent to which genetic overlap extends beyond APOE and the biological mechanisms underlying such shared genetic susceptibility require systematic investigation.
This study aims to comprehensively characterize the shared genetic architecture between AD and LOE, including both established factors, such as APOE and novel genetic variants, and to elucidate the biological pathways that may link these genetic variants to the development of both conditions. The findings may enhance our understanding of the disease mechanisms underlying AD and LOE, potentially informing the development of targeted prevention and treatment strategies for these neurological disorders. Furthermore, the methodological approaches employed in this study could be applied to other complex diseases to evaluate shared genetic risks, offering valuable insights into potential causal mechanisms and pathways.
Results
UCLA sample description
Figure 1 provides an overview of the study design and the samples included in the analyses. The primary analytical sample was derived from the electronic health records (EHRs) of the University of California, Los Angeles (UCLA) Health System, specifically from individuals who self-reported as non-Hispanic Whites. Table 1 presents baseline descriptive statistics for our full UCLA sample (N = 416,212). In this cohort, we observed an older age at last visit, a longer span of EHR records, and a higher proportion of deceased patients in LOE or AD cases compared to their corresponding controls. Additionally, there was a higher prevalence of hypertension, diabetes, stroke, and hyperlipidemia among individuals with LOE or AD compared to controls. The proportion of patients with complications related to AD or LOE was also higher compared to controls.

Overview of study design and samples included in the analyses.
The secondary analytical sample was derived from a subset of the primary sample, comprising patients with available genetic data (ATLAS sample, N = 16,500). Compared to patients without genetic data (non-ATLAS sample, N = 399,712), our ATLAS sample exhibited a higher prevalence of AD and LOE, were younger at first visit but older at last visit, had longer EHR record lengths, and a higher rate of deceased patients. The ATLAS sample also presented with worse baseline health conditions, indicated by a higher prevalence of hypertension, diabetes, stroke, and hyperlipidemia (Supplementary Table 1).
Table 2 presents baseline descriptive statistics for our UCLA ATLAS sample. In this sample, similar patterns of distributions were observed across AD/LOE cases, demographics, and health conditions. The proportion of patients with complications related to AD or LOE was higher in cases compared to controls. The distribution of APOE-ε4 allele count and AD polygenic risk score (PRS) without the APOE region also differed significantly between AD cases and controls, with a higher prevalence in AD cases. However, there were no significant differences in APOE-ε4 allele count or AD PRS without the APOE region distributions between LOE cases and controls.
Associations between LOE and AD phenotypes
We employed two longitudinal models to assess the associations between LOE and AD phenotypes in the full UCLA sample (N = 416,212) and the UCLA ATLAS sample (N = 16,500): the Cox proportional hazard model21 and the Fine and Gray model22. The association results are presented in Table 3.
In the full UCLA sample, for the associations between LOE and AD, where incidence of AD was considered the outcome, after adjusting for age at first visit, sex, EHR record length, and health risk factors common to both conditions (including hypertension, diabetes, stroke, and hyperlipidemia), the Cox proportional hazard model demonstrated a strong positive association between LOE and the incidence of AD (Hazard Ratio (HR) = 6.86, 95% confidence interval (CI): 6.02, 7.81). This association still held after accounting for the competing risk of death (HR = 2.54, 95% CI: 2.12, 3.06). Regarding associations between AD and LOE, where LOE was the outcome, a stronger positive association was observed between AD status and the incidence of LOE in the Cox proportional hazard model (HR = 6.31, 95% CI: 5.49, 7.25). This association still held after accounting for the competing risk of death (HR = 2.13, 95% CI: 1.36, 3.34).
In the ATLAS sample, we observed similar increased risks of AD in LOE patients and vice versa, even after accounting for the competing risk of death. When additionally adjusted for AD genetic factors, including the APOE-ε4 allele count and AD polygenic risk score (without the APOE region), these positive associations persisted. Further examination of the effect sizes of these genetic factors (Supplementary Table 2) revealed that only APOE-ε4 allele count was significantly associated with an increased risk of AD when adjusting for LOE status (Cox model: HR = 2.53, 95% CI: 2.10, 3.05; Fine and Gray model: HR = 2.51, 95% CI: 2.07, 3.05). There was a suggestive positive association between APOE-ε4 allele count and the incidence of LOE when adjusting for AD status, but it did not reach statistical significance. No statistically significant association was found between the AD polygenic risk score (without the APOE region) and either AD or LOE.
These association results suggest that APOE may be a significant risk factor for both conditions and could play a role in their co-occurrence or complications. However, a crucial question remains: are there shared risk factors beyond APOE that are not captured by the AD PRS without the APOE region? Investigating their shared genetic risk is essential. Understanding potential genetic overlap could provide insights into underlying biological mechanisms that these models may not fully capture, ultimately contributing to a more comprehensive understanding of the relationship between AD and LOE.
Genetic correlation with LDSC regression.
We initially assessed the genetic correlations between AD and generalized epilepsy using the LDSC regression method with publicly available GWAS summary statistics23,24. Due to the absence of GWAS data specific to LOE, we utilized data from a recent GWAS on generalized epilepsy23. The LDSC analysis revealed no significant genetic correlation between AD and generalized epilepsy (rg = -0.10 ± 0.06, p = 0.10).
Although LDSC regression identified a null association between AD and epilepsy, this result may reflect mechanistic differences in generalized epilepsy and LOE, and certain limitations inherent to the LDSC approach. LDSC is constrained by its reliance on GWAS summary statistics and may lack the power to detect complex genetic relationships or interactions that influence both AD and LOE17. To overcome these limitations, we turned to a multi-task machine learning model, which can simultaneously evaluate multiple outcomes, incorporate more intricate genetic architectures, and potentially uncover shared risk factors that traditional methods might miss25. This approach offers a more nuanced exploration of the genetic underpinnings of AD and LOE.
Shared genetic risks of AD and LOE with multi-task learning.
We applied a multi-task learning framework (Fig. 2, detailed in Methods) to identify shared risk single nucleotide polymorphisms (SNPs) for AD and LOE using a subset of the UCLA ATLAS sample (N = 9,986, including 376 AD cases and 658 LOE cases). In this subsample, we observed similar patterns to the full ATLAS sample that AD and LOE cases had a higher prevalence of condition-specific complications compared to controls. However, distributions of baseline demographics, EHR characteristics, and comorbidity profiles were different from those in the full ATLAS cohort due to stricter control criteria: age at last visit ≥ 70 and a minimum of five years of records. These requirements minimized misclassification bias and improved case–control balance (see Methods, Supplementary Table 3).
After accounting for age at last visit, sex, and ancestry-specific genetic variations (represented by principal components (PCs)), APOE-ε4 was significantly associated with AD (OR = 2.85, 95% CI: 2.34, 3.48) and showed a borderline association with LOE (OR = 1.20, 95% CI: 0.99, 1.45), suggesting a modest shared genetic contribution. The AD polygenic risk score (without the APOE region) was associated with AD (OR = 1.15, 95% CI: 1.04, 1.27) but not with LOE (Table 4).
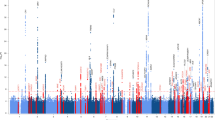
Using a multi-task Elastic Net model, we jointly predicted AD and LOE based on candidate SNPs from recent GWAS of AD24 and generalized epilepsy23 (see Methods) and incorporated offset corrections within a linearized framework. The model identified nine SNPs with non-zero weights for both phenotype prediction tasks. Among these, eight SNPs were identified as shared genetic risk factors for AD and LOE, defined by having coefficients in the same direction for both conditions. Seven of the eight were SNPs from the AD GWAS. The standardized coefficient magnitudes for these shared risk factors are presented in Fig. 3. A detailed list, including related genomic coordinates and functional annotations, were provided in Supplementary Table 4.
A set of shared risk SNPs was identified near the 19q13 region. Among these, chr19:44885243 was the top SNP with the highest coefficient magnitude, particularly in predicting AD. Additionally, SNPs outside the 19q13 region, such as chr2:127133851, chr8:27607412, and chr10:11676714, also contributed significantly to the shared genetic risk for AD and LOE, highlighting the complex genetic interplay between these disorders.

Multi-task elastic net model framework.

Standardized coefficient magnitude of shared risk features identified from the multi-task elastic net models. SNPs identified from the epilepsy GWAS are marked in orange. Colors in the bar plot represent direction of effects (red for ‘+’, blue for ‘-‘).
The eight shared risk SNPs were mapped to 21 genes using positional, expression quantitative trait loci (eQTL), and chromatin interaction mapping techniques. These genes were tested against established gene sets for overrepresentation in terms of positions, biological functions, and pathways (Fig. 4). The APOE region 19q13 (including the overlapping linkage disequilibrium (LD) block with TOMM40 and APOC1 genes), emerged as an essential genomic risk locus among the mapped shared risk genes for AD and LOE (Supplementary Table 5). Other important genes included BIN1, CLU, PVRL2 and TRAPPC6A. The shared risk genes were enriched in gene ontology biological processes related to amyloid catabolic processes and lipid metabolism, cellular components such as protein lipid complex, lipoprotein particles, and chylomicron, and molecular functions including tau protein binding and phosphatidylcholine-sterol O-acyltransferase activity. Notably, the most significantly enriched pathways were primarily associated with AD pathogenesis, with limited evidence for epilepsy-specific pathways.

Enrichment test results for shared risk genes of Alzheimer’s disease and late-onset epilepsy. The set of genes were mapped from shared risk genetic loci from the multi-task Elastic Net model.
Sensitivity analyses
Shared AD-LOE genetic risk score (GRS)
We calculated a shared AD-LOE GRS for each individual in the full UCLA ATLAS sample (N = 16,500) using the shared risk factors identified in the previous analysis. Weights for SNPs were estimated from a logistic regression model in the training set (N = 13,200, N AD = 540, N LOE = 312). The GRS was standardized to reflect per-unit increases in genetic risk. We then assessed the associations between this shared GRS and AD and/or LOE-related phenotypes in the testing set (N = 3,300, N AD = 64, N LOE = 118), comparing these results to the well-documented effect of the APOE gene (Table 5).
In the UCLA ATLAS multi-task modeling testing sample (N = 2,002), a one-standard deviation increase in the shared AD-LOE shared GRS was associated with a 1.42-fold increase in the risk of AD or LOE (95% CI: 1.22, 1.64); a 2.10-fold increase in the risk of AD (95% CI: 1.64, 2.71), and a borderline 1.16-fold increase in the risk of LOE (95% CI: 0.97, 1.38). The effect sizes were stronger when considering the APOE-ε4 allele count in relation to AD or LOE (OR = 1.90, 95% CI: 1.41, 2.53) and AD (OR = 4.31, 95% CI: 2.75, 6.78). However, no association was observed between APOE-ε4 allele count and LOE. While both APOE-ε4 and the shared GRS were associated with the combined AD or LOE phenotype, the associations appeared to be primarily driven by AD cases rather than showing equivalent effects across both conditions individually.
In terms of variation explained by the genetic scores, the APOE-ε4 count explained a higher proportion of variance in AD-related phenotypes compared to the AD-LOE shared GRS. Conversely, the AD-LOE shared GRS explained a greater proportion of the variance in LOE-related phenotypes than the APOE-ε4 count.
To address potential concerns about APOE region dominance in our shared genetic risk score, we conducted additional analyses focusing exclusively on the four shared risk variants located outside the APOE region (chr2:127133851, chr8:27607412, chr10:11676714, and chr2:103489151). These variants map to BIN1, CLU, PVRL2, and TRAPPC6A genes, respectively. The non-APOE shared genetic risk score demonstrated a significant association with the combined AD or LOE phenotype (OR = 1.24, 95% CI: 1.06, 1.45) and LOE-only (OR = 1.21, 95% CI: 1.01, 1.46), and a borderline associations with AD-only (OR = 1.28, 95% CI: 0.99, 1.66). These findings provide evidence for genetic risk sharing beyond the APOE region, with the non-APOE shared genetic risk score demonstrating significant associations with both the combined phenotype and LOE specifically.
Multi-task model performance in AD or LOE prediction
Although the primary aim of our study was to identify shared risk factors rather than to predict AD and LOE, we evaluated the performance of our multi-task Elastic Net model by comparing it with separate Elastic Net models that predicted AD and LOE individually with 1000 iterations (details in Methods). The multi-task Elastic Net model not only identified shared risk factors between AD and LOE but also contributed to the prediction of AD and LOE onset. When compared to the separate Elastic Net models, the multi-task Elastic Net model showed overall improvement in both AD and LOE prediction tasks. Specifically, we observed a significant improvement in the area under the precision-recall curve for AD prediction (0.083 vs. 0.061, Wilcoxon test p-value < 0.001) and a significant improvement for LOE prediction (0.108 vs. 0.078, Wilcoxon test p-value < 0.001).
Validation in all of Us dataset
To further assess robustness, we validated our results in a comparable non-Hispanic White sample extracted from the All of Us database (N = 52,493). Compared to the UCLA ATLAS sample (N = 16,500), the All of Us sample was older at their first visit and younger at their last visit on average, with a higher proportion of females, longer EHR record length, and a lower proportion of deceased patients. The All of Us sample also had a lower prevalence of AD but a higher prevalence of LOE, and better overall health conditions (Supplementary Table 6). Within the All of Us sample, we also observed similar patterns in distributions across AD/LOE cases, demographics, and health conditions. The proportion of patients with complications related to AD or LOE was higher in cases compared to controls (Supplementary Table 7).
First, we repeated the same association tests of AD and LOE with the Cox proportional hazard models and the Fine and Gray models in the All of Us sample. Results were shown in Table 6. After adjusting for age at first visit, sex, EHR record length, hypertension, diabetes, stroke, and hyperlipidemia, we observed a similar positive association between LOE and the incidence of AD (HR = 3.95, 95% CI: 2.77, 5.63). This association still held after accounting for the competing risk of death (HR = 2.47, 95% CI: 1.69, 3.60). Similarly, we also observed a positive association between AD and the incidence of LOE (Cox model: HR = 2.96, 95% CI: 1.89, 4.61; Fine and Gray model: HR = 1.98, 95% CI: 1.22, 3.30). After additionally adjusting for APOE-ε4 count, the positive associations still held.
We then applied the shared GRS weights, derived from the UCLA ATLAS training sample, to a subset of participants in the All of Us cohort with available genetic data. To ensure comparability, we restricted this evaluation sample using the same inclusion criteria as those applied to the UCLA genetic dataset. An individual-level AD–LOE shared GRS was subsequently computed for each participant in the All of Us subset (N = 23,037). We tested the associations between the AD-LOE shared GRS and both AD and LOE in this sample and compared them to the APOE-ε4 model (Table 7). The positive associations still held between AD-LOE shared GRS and AD or LOE (OR = 1.09, 95% CI: 1.04, 1.14) and AD (OR = 1.54, 95% CI: 1.40, 1.69). However, the effect sizes were not as large as those in the UCLA ATLAS sample, where those weights were trained. The APOE-ε4 allele count was associated with AD or LOE (OR = 1.16, 95% CI: 1.01, 1.32) and AD (OR = 1.98, 95% CI: 1.42, 2.84), with smaller effect sizes observed as well. The variation explained by the genetic scores was also lower for both variables compared to the UCLA ATLAS sample. However, the non-APOE shared genetic risk score did not show a statistically significant association with any of the tested phenotypes, including the combined AD or LOE outcome, AD-only, or LOE-only.
Discussion
Using a multi-task Elastic Net method, we identified eight shared risk SNPs between AD and LOE, which were then mapped to genes for further biological function analysis. Our findings highlight the APOE region, including the overlapping LD block with TOMM40 and APOC1 genes, as a significant genomic risk locus for both conditions. Additionally, genes such as BIN1, CLU, PVRL2, and TRAPPC6A were identified as key shared risk factors. These genes are enriched in pathways related to lipid metabolism, amyloid catabolic processes, and tau protein binding. This approach enabled the discovery of common genetic factors, providing valuable insights into shared disease mechanisms that could inform prevention, targeted treatments, and drug development for both AD and LOE.
Few studies have evaluated LOE and AD associations with longitudinal models26,27, and none have further included genetic risk factors, such as the APOE gene and AD PRS, as covariates to control for genetic factors that could contribute to both conditions. To further explore the complex associations between LOE and AD, we employed two different longitudinal models (Cox proportional hazard and Fine and Gray models) in two different populations (UCLA Health and All of Us). Our findings suggest an independent bidirectional relationship between AD and LOE, even when accounting for the influence of mortality.
In the UCLA ATLAS genetic subsample, we further evaluated the role of AD-related genetic risk in both conditions. APOE was significantly associated with AD and showed a modest, borderline association with LOE, suggesting it may contribute to both outcomes. However, this association with LOE was not replicated in the All of Us validation cohort, providing limited evidence for its generalizability and likely reflecting limited power to detect small effect sizes, differences in sample size, ancestry composition, or EHR-derived phenotype accuracy between the UCLA and All of Us cohorts. These results highlight the need for further validation in well-powered, ancestrally representative datasets.
Initially, we attempted to estimate the genetic correlation between these conditions using the established LDSC tool17. However, results indicated no significant genetic correlation between AD and generalized epilepsy. One possible explanation is that we used a generalized epilepsy23 GWAS due to the lack of GWAS data specific to LOE, and the genetic risk factors may differ between these conditions. Another limitation of LDSC is that it averages the genetic effects across the entire genome17. When only a few loci are shared and these loci, such as the APOE gene, have strong effects, the signal from these specific SNPs may be diluted by the large number of non-shared SNPs with little or no effect. As a result, the overall estimate of genetic correlation may appear weaker than it actually is.
Despite the null results from LDSC, we hypothesized the existence of underlying genetic predispositions and overlapping biological pathways between AD and LOE. This led us to develop a multi-task Elastic Net model to identify these shared genetic risk factors. When selecting candidate SNPs for the multi-task Elastic Net model, we moved beyond the typical reliance on GWAS p-values and the closest gene, opting instead to prioritize Combined Annotation-Dependent Depletion (CADD) scores and functional mapping results. This strategy not only enhanced model interpretability by targeting variants with functional consequences and pinpointing likely causal loci, but also yielded significantly higher predictive accuracy compared to conventional p-value filtering28, allowing us to frame our findings in the broader context of genes and molecular pathways underlying shared AD and LOE risk.
Our findings provide initial evidence for potential shared genetic architecture between AD and LOE within a European population, though the extent and independence of this shared architecture require further investigation. Our multi-task Elastic Net model selected multiple shared-risk SNPs mapping to the APOE region, reinforcing the hypothesis that shared genetic risks exist between AD and LOE, particularly in the APOE region. These findings align with previous studies18,19,29. APOE, as the primary lipid carrier in the brain, is crucial for maintaining neuronal and synaptic function and repair mechanisms in the central nervous system. Dysregulation of APOE function, especially in the context of the APOE-ε4 allele, may contribute to altered amyloid-beta metabolism30,31, neuronal hyperexcitability32, and neuroinflammation33, potentially leading to both the cognitive decline seen in AD and the increased susceptibility to seizures in LOE.
However, the identification of shared-risk SNPs outside the APOE region by the multi-task Elastic Net model suggests that other genetic risk factors also contribute to the shared genetics of AD and LOE. Of particular interest is the identification of the BIN1 and CLU genes. BIN1 (Bridging Integrator 1) is a major genetic risk factor for AD, known to regulate calcium homeostasis, electrical activity, and gene expression in glutamatergic neurons34,35. Its involvement in membrane dynamics, endocytosis, and neurotransmitter vesicle release36 suggests a role in synaptic function and neuronal health, which are critical for both AD pathology and seizure susceptibility. CLU (Clusterin), also known as apolipoprotein J, is another significant genetic risk factor for AD37. It is involved in amyloid-beta clearance and aggregation38, inflammation, and oxidative stress39. Given its role in maintaining neuronal integrity and responding to cellular stress, CLU may contribute to the shared pathogenic mechanisms underlying both AD and LOE40. The identification of these genes reinforces the complex genetic interplay beyond APOE in the shared etiology of AD and LOE.
Enrichment analysis of the identified genes enhances our understanding of the pathogenesis underlying the interconnection between these two diseases. Our analysis revealed a notable enrichment in tau protein binding with identified genes such as BIN1, CLU, and APOE. Tau protein, a critical microtubule-associated protein, has been implicated in the pathophysiology of epilepsy and AD, signifying its potential as a therapeutic target35,41. Remarkably, tau reduction has been identified as a viable therapeutic strategy for AD and other related disorders characterized by epileptic activity. In a mouse model of AD, genetic reduction of tau levels was found to prevent learning and memory disruption, epileptic activity, and other AD-related deficits42. Furthermore, biomarkers associated with tau, such as total tau and p-tau levels in cerebrospinal fluid41,43,44 or plasma45, are used to diagnose AD and may hold promise for LOE. This evidence, along with our results, suggests that tau-mediated mechanisms may provide a novel opportunity for the development of disease-modifying therapies for both LOE and AD.
In addition, we conducted secondary analyses to explore the utility of the predicted value derived from the multi-task Elastic Net model and validated all our findings in an independent cohort—the All of Us dataset. Our findings demonstrated the shared GRS’s capability to effectively stratify patients into distinct AD-LOE risk groups, allowing for better risk assessment and management. The consistent results across these distinct datasets underscore the reliability of our identified shared genetic risks and their potential applicability to broader populations.
On the other hand, several findings warrant careful interpretation. First, pathway enrichment analyses primarily highlighted AD-related biological processes, with minimal evidence supporting epilepsy-specific pathways, suggesting a more limited genetic overlap than initially hypothesized. Second, we observed no significant association between APOE-ε4 and LOE in the All of Us cohort, a finding that diverges from some prior reports and calls into question the strength of APOE’s contribution to LOE susceptibility. Finally, associations with the shared genetic risk score appeared to be driven predominantly by AD cases, rather than showing comparable effects across both conditions. Collectively, these findings provide only limited evidence for shared genetic architecture and suggest that although some genetic overlap exists, the extent of shared genetic architecture between AD and LOE appears limited and requires further validation in larger, more diverse cohorts. Future studies should aim to replicate these findings in larger, independent cohorts and explore the functional consequences of the identified variants to better understand their role in the shared pathophysiology of AD and LOE.
While this study advances our understanding of potential shared genetic risk between AD and LOE, several limitations must be acknowledged. The prevalences of AD and LOE were lower in both our discovery and validation datasets, likely reflecting the under-diagnosis of both conditions in EHRs. Participant samples in our study were selected based on ICD-10 diagnosis codes retrieved from EHRs, which could be subject to misclassifications. For example, individuals classified with LOE could also have undiagnosed mild cognitive impairment or AD. Similarly, some diagnosed with AD could exhibit subclinical seizures. Another limitation is the study’s applicability to individuals of European ancestry only. Due to the small sample sizes of other ancestry groups in our dataset, we did not perform modeling for these populations. As a result, the generalizability of our findings to other ancestries is limited. Future studies should consider the impact of sample heterogeneity during model development. Training with larger sample sizes, collecting data from multiple institutions, and focusing on additional populations may help enhance the generalizability.
In conclusion, our study provides evidence for potential shared genetic risks of AD and LOE in the European population by deploying a multi-task learning method. While our results confirmed the importance of the APOE gene region and identified novel genes that may contribute to both diseases, future studies with larger sample sizes, more diverse populations, and LOE-specific GWAS data will be essential to definitively establish the extent of genetic overlap between these conditions. By highlighting these novel genes, our study contributes to a deeper understanding of the molecular mechanisms that govern the complex interplay between neurodegenerative diseases. These findings can inform future research to improve disease prevention, diagnosis, treatments, and drug development for both conditions.
Methods
Data source
Our primary samples were derived from the electronic health records (EHRs) of the UCLA Health System. The UCLA Health System encompasses two hospitals and 210 primary and specialty outpatient sites across greater Los Angeles. Since March 2, 2013, the UCLA Data Discovery Repository (DDR) has collected de-identified EHRs under the auspices of the UCLA Health Office of Health Informatics Analytics and the UCLA Institute for Precision Health. The DDR includes longitudinal records of demographics, vital signs, diagnoses, laboratory tests, encounters, provider metadata, prescriptions, and hospital admissions46. Mortality data were ascertained via in-hospital records, family reports, and California Department of Public Health death registries.
Sample selection
To focus on longitudinal patient records, our analyses were restricted to patients with complete demographic information (age and sex) who self-reported as non-Hispanic White and had at least two medical encounters after the age of 60. An age range of 60 to 90 years was applied based on two considerations: (1) to ensure patients were old enough to meet the criteria for LOE, defined as onset after age 60; and (2) to address limitations in EHR data, where patients aged 90 or older are recorded as 90 in the UCLA de-identified EHR to maintain privacy. The final analytical sample from the full UCLA cohort comprised N = 416,212 patients. For the UCLA ATLAS sample, which included available genetic data, we further ensured that self-reported non-Hispanic White patients also had European American genetically inferred ancestry to enhance precision in ancestry reporting. This resulted in N = 16,500 patients in the UCLA ATLAS sample.
Phenotype definition
To identify individuals with LOE or AD, we utilized a previously validated set of phecodes. Phecodes are groupings of International Classification of Diseases, Tenth Revision (ICD-10) codes that correspond to specific clinical phenotypes47. For LOE, the phecodes used in this study included “345” (Epilepsy, recurrent seizures, convulsions), “345.1” (Epilepsy), “345.11” (Generalized convulsive epilepsy), “345.12” (Partial epilepsy), and “345.3” (Convulsions). Individuals were classified as LOE cases if they met two criteria: (1) at least one encounter with any of these phecodes, and (2) the first LOE diagnosis occurred after age 60, with at least one encounter before age 60.
For AD, the phecode “290.11” was used, and AD cases were defined as individuals with at least one encounter with this code.
Non-LOE or non-AD controls were defined as individuals who: (1) had no diagnosis of LOE or AD, and (2) had no diagnosis of phecodes within the “exclude ranges” for each corresponding phecode. These exclude ranges were employed to mitigate inaccuracies in ICD coding, where less specific codes are sometimes applied to certain medical conditions48. These exclusion criteria ensured the selection of controls without related conditions, thereby providing more accurate and reliable data for EHR-based case-control analysis. For instance, phecodes “290.12” (Dementia with cerebral degenerations) and “290.16” (Vascular dementia) were excluded from the AD control group. Supplementary Table 8 provides detailed descriptions of the phecodes, exclude ranges, and mapped ICD-10 codes used in our phenotype definition.
We also collected data on other health conditions potentially associated with LOE and/or AD, including hypertension (phecode “401.1”), diabetes (phecode “250.2”), stroke (phecodes “433”), and hyperlipidemia (phecode “272.1”). All ICD-phecodes mappings were performed using the R package “PheWAS”49. Baseline characteristics were compared across LOE and AD status. χ2 test and analysis of variance were used as appropriate to assess homogeneity across groups.
Genetic data pre-processing
Quality control
A subsample of UCLA Health patients participates in the UCLA ATLAS Community Health Initiative (ATLAS), which provides biosamples linked to their de-identified EHRs. All procedures adhered to UCLA Institutional Review Board (IRB)-approved protocols; informed consent was obtained prior to enrollment, and comprehensive biobanking details are described previously50,51. This study was classified as exempt human-subjects research (UCLA IRB #21–000435). For the UCLA ATLAS sample, stringent quality control (QC) measures and genotype imputation procedures were implemented to ensure the robustness and reliability of subsequent analyses. QC was conducted using PLINK v1.952, following established guidelines46. Samples with a missingness rate exceeding 5% were excluded. Low-quality SNPs, including those with more than 5% missingness, monomorphic SNPs, and strand-ambiguous SNPs, were removed. Following QC, genotype imputation was performed using the Michigan Imputation Server53 to enhance the coverage of genetic variants and facilitate comparisons across different genotyping platforms. SNPs with an imputation r² below 0.90 or a minor allele frequency of less than 1% were pruned. After these procedures, approximately 8 million genotyped SNPs were retained across the 54,935 individuals.
Inferring genetic ancestry
Genetic ancestry refers to the most recent geographic origins of an individual’s genome, which is independent from an individual’s cultural identity54. Genetically inferred ancestry utilizes genetic data, reference populations, and inference methods to characterize individuals within a group who likely share recent geographical ancestors55. For the UCLA ATLAS sample, we employed principal component analysis (PCA)56 to infer patients’ genetic ancestry, using the reference panel from the 1000 Genomes Project57. This panel includes genotypes from individuals of known European, African, Admixed American, East Asian, and South Asian descent. For instance, “European American genetically inferred ancestry " refers to individuals in the United States whose recent biological ancestors were inferred to be of European descent. Ancestry-specific principal components (PCs) were subsequently recalculated using PCA to identify population structures within each ancestry group.
APOE-ε4 count and AD polygenic risk score
The APOE gene has two key variants, rs7412 and rs429358, which determine the three common isoforms of the apolipoprotein E (apoE) protein: E2, E3, and E4, encoded by the ε2, ε3, and ε4 alleles, respectively58. To quantify the APOE genotype in our study, we created a numerical variable, “APOE-ε4 count”, representing the number of ε4 alleles (0, 1, or 2) carried by each individual.
We computed the AD PRS as the sum of an individual’s risk allele dosages, each weighted by its corresponding risk allele effect size from the AD genome-wide association study (GWAS) summary statistics15, as shown in the PRS equation: \(\:{PRS}_{i}={\sum\:}_{j}^{M}{\widehat{\beta\:}}_{j}\times\:{dosage}_{ij}\). To isolate the effect of APOE gene from other genetic factors, we constructed the PRS without including the APOE region. Specifically, for our scores with the APOE gene region removed, we excluded all variants from the summary statistics on chromosome 19 near APOE (44,891,220 to 44,919,349, GRCh38). This region spans from 10 kilobases upstream of the start position of TOMM40 (44,891,220) to 10 kilobases downstream of the stop position of APOC1 (44,919,349). This entire region was removed due to the dense LD block observed in European ancestries, which overlaps these three genes (TOMM40, APOE, APOC1).
Candidate single nucleotide polymorphisms (SNPs) identification and annotation
To identify shared genetic risk SNPs, we initially selected a set of genome-wide significant and potentially causal SNPs from recent GWAS on AD24 and epilepsy23. As there is currently no GWAS specifically focused on LOE, a generalized epilepsy GWAS was used as a substitute. We utilized FUMA59, a comprehensive tool that integrates information from various biological data repositories and resources, to annotate and prioritize these SNPs.
FUMA first identifies SNPs that have reached a genome-wide significant P-value (< 5e-8). Then it implements a sophisticated LD-based approach to identify and annotate genetic variants that extend beyond the SNPs directly tested in the original GWAS. Specifically, FUMA incorporates “proxy variants” from its reference LD panel (1000 Genomes Project by default) to comprehensively define and annotate each genomic locus57. The mapping from SNPs to genes was subsequently performed using ANNOVAR60 (“gene-based annotation”) with Ensembl genes (build 85). SNPs were mapped to genes through three distinct methods: (i) positional mapping, based on physical location on the genome; (ii) eQTL associations, through eQTL mapping; and (iii) 3D chromatin interactions, via chromatin interaction mapping. The Combined Annotation-Dependent Depletion (CADD) score61 was also applied to select potential causal SNPs, with higher scores indicating a greater likelihood of the variant being deleterious. SNPs with at least one positional, eQTL, or chromatin interaction mapped gene, or with a CADD score above the suggestive threshold (≥12.37), were considered deleterious.
A total of 4,454 SNPs were identified as genome-wide significant and potentially causal SNPs from the two GWAS summary statistics. These SNPs were subsequently used as candidate features for identifying shared genetic risk loci for AD and LOE.
Statistical modeling
Associations between LOE and AD phenotypes
We first compared baseline demographic, comorbidities, and AD genetics measures (where applicable) across LOE and AD status in our analytical samples. Continuous variables (e.g., age) were analyzed using the Wilcoxon rank-sum test (Mann–Whitney U test), whereas categorical variables (e.g., sex) were assessed with Pearson’s chi-squared test. We then examined the associations between LOE and AD phenotypes in our analytic samples, which included both the full UCLA patient cohort (N = 416,212) and the ATLAS sample with available genetic data (N = 16,500). First, we employed Cox proportional hazard models to assess the association between the presence of LOE and the incidence of AD, and vice versa, thereby indicating the cause-specific hazard of one condition on the other. Second, we applied the Fine and Gray proportional subdistribution hazards model. This model accounts for competing risks, such as death, by retaining them in the risk set indefinitely22. The Fine and Gray model focuses on the cumulative incidence function, which reflects the probability of the outcome occurring over time while considering the possibility that death could preclude the occurrence of the outcome.
For all association models, demographic adjustments included age at first visit, sex, and EHR record length. Additional adjustments accounted for health risk factors associated with both conditions, including hypertension, diabetes, stroke, and hyperlipidemia status. For the genetic sample, we also adjusted for APOE-ε4 count and AD PRS without the APOE region to examine the effect of genetic variables on the associations. We calculated the follow-up time for each patient, considering both the time to event and censoring. Patients with the outcome prior to the onset of exposure were excluded from the analysis. We reported hazard ratios (HR) from Cox and Fine and Gray models, along with their 95% confidence intervals (CIs).
Genetic correlation with linkage disequilibrium score (LDSC) regression
We evaluated the genetic correlations between AD and generalized epilepsy using the linkage disequilibrium score (LDSC) regression method with publicly available GWAS summary statistics. We utilized GWAS summary data from studies on AD24 and generalized epilepsy23, and performed genetic correlation estimation using LDSC software62. Briefly, LDSC software estimates the genetic correlation between two phenotypes by comparing the strength and direction of association signals at each locus while adjusting for the correlation expected due to genetic linkage62. We adjusted for linkage between SNPs (i.e., covariance due to genomic proximity) using LD scores based on the European sample from the 1000 Genomes Project63. Additional SNP QC procedures followed the defaults in the LDSC ‘munge_sumstats.py’ function, ensuring that alleles matched those in the HapMap3 reference panel64. The genetic correlation was assessed using the intersection of QC-positive SNPs, and results were reported as the correlation coefficient ± standard error.
Identification of shared risk genetic loci of AD and LOE with multi-task learning
We employed a multi-task learning framework to identify shared genetic risk loci of AD and LOE in a separate UCLA ATLAS sample. The modeling sample (N = 9,986) was further restricted by applying stricter inclusion criteria to controls: age at last visit ≥ 70 and a minimum of five years of records. These criteria reduced the potential bias from misdiagnosis. Given the limited number of cases for both phenotypes (658 cases for LOE and 376 cases for AD), reducing the number of controls also helped mitigate bias due to the imbalanced dataset65.
To distinctly assess genetic influences, we began by mitigating the impact of demographic factors, including age, sex, and ancestry-specific PCs. We first employed a logistic regression model using these variables to predict AD or LOE status, deriving predicted values for each patient. Using a logit inverse link function, we subtracted these predicted values from the observed outcomes (AD or LOE status), generating “offset” values. These offsets represented the AD or LOE status after regressing out the effects of demographic variables and genetic population structure.
Next, we trained a multi-task Elastic Net model to predict AD and LOE status, applying offset corrections in the linearized space, expressed as: \(\:{\widehat{y}}_{i}={g}^{-1}({\beta\:}_{0}+{\beta\:}_{1}{x}_{i1}+\dots\:+{\beta\:}_{p}{x}_{ip}+{offset}_{i})\), where \(\:{\widehat{y}}_{i}\) represents the predicted dementia status, and \(\:{g}^{-1}\left(\right)\) is the inverse of the link function66.
Figure 2 illustrates the multi-task Elastic Net model. In general, a multi-task learning model is trained simultaneously on multiple related tasks, leveraging shared information to improve performance across all tasks. The multi-task Elastic Net model consists of a linear model trained with a mixed ℓ1 ℓ2-norm and ℓ2-norm for regularization, using coordinate descent to fit the coefficients67.
The multi-task Elastic Net model also employs Elastic Net regularization, which combines the advantages of both Lasso (L1) and Ridge (L2) regression methods. This approach enhances model stability and variance handling, aiding in variable selection by reducing the coefficients of less relevant variables to zero, thereby simplifying the model and improving its ability to manage multicollinearity—particularly useful given the many SNP features in linkage disequilibrium (LD)68. The hyperparameter α, which controls the strength of L1 regularization, and \(\:\rho\:\), which balances L1 and L2 regularization, were optimized using a grid search to maximize the penalized likelihood within the training set.
To enhance the robustness of our findings, we repeated the modeling process 1,000 times with different random seeds to determine feature importance and establish statistical significance. Model performance and features selected by the multi-task Elastic Net model in each iteration were recorded. SNPs identified in at least 25% of the 1,000 iterations were retained. Shared genetic risk loci for AD and LOE were defined as features with average coefficients in the same direction for both tasks across all iterations.
For biological interpretations, we mapped identified risk SNPs to genes using FUMA’s positional, eQTL, and chromatin interaction mapping59. Specifically, we used: (1) positional mapping based on genomic coordinates from the GRCh38 reference genome, mapping SNPs to genes within ± 100 kb windows; (2) eQTL mapping using data from the GTEx v8 database, focusing on brain-relevant tissues including cortex, hippocampus, and other neural tissues; and (3) chromatin interaction mapping using Hi-C data from the 3D Genome Browser and published chromatin conformation capture studies in neural cell types. Functional consequences of each variant were predicted using the Ensembl Variant Effect Predictor (VEP) database, which integrates multiple prediction algorithms including SIFT, PolyPhen-2, and CADD scores69. Genes of interest (e.g., mapped shared risk genes of AD and LOE) were tested for enrichment of biological functions using hypergeometric tests against gene sets from MsigDB. Gene sets with an adjusted P-value ≤ 0.05 and more than one overlapping gene were reported and visualized using heatmaps.
Sensitivity analyses
Shared AD-LOE genetic risk score on AD and LOE diagnosis
We constructed an AD-LOE shared genetic risk score (GRS) for each patient using the shared risk factors identified in prior analyses. The full UCLA ATLAS sample was randomly split into a training set (80%) and a testing set (20%). For each individual \(\:i\), the shared GRS was calculated as: \(\:shared\_GR{S}_{i}=\sum\:_{j}^{M}{\widehat{\beta\:}}_{j}\times\:dosag{e}_{ij}\), where \(\:M\) represents the total number of shared SNPs, and \(\:{\widehat{\beta\:}}_{j}\) represents the estimated weight for a given shared risk SNP \(\:j\). The \(\:{\widehat{\beta\:}}_{j}\) for each SNP was determined by fitting a logistic regression model on the training set (N = 13,200), using all identified shared risk SNPs as predictors and AD or LOE as the outcome. Consistent with earlier modeling steps, we first regressed out the effects of demographic variables and genetic population structure. We standardized the final shared GRS to a mean of 0 and a standard deviation of 1 (defined by the training set) to reflect per-unit increases in the score.
The resulting shared GRS was standardized (mean = 0, SD = 1) based on the training set to facilitate interpretation per unit increase. Associations between the standardized shared GRS and AD or LOE status were subsequently evaluated in the independent testing set (N = 3,300) using logistic regression models, adjusting for sex and the first five ancestry-specific PCs. ORs and their 95% CIs were reported.
Based on the logistic regression models, we also calculated the variance explained by the AD-LOE shared GRS for each phenotype. A reduced logistic regression model was fitted with sex and the first five ancestry-specific PCs only. The percentage of variation explained by the AD-LOE shared GRS was calculated using the formula:
Given that the APOE gene is a well-studied shared risk factor between AD and LOE, we also compared the variance explained by our AD-LOE shared GRS to that explained by the APOE-ε4 allele.
To address potential concerns about the dominance of APOE region variants in our shared genetic risk score and to evaluate the independent contribution of non-APOE variants to shared genetic risk, we conducted a sensitivity analysis using only the four shared risk variants located outside the APOE region. These variants included chr2:127133851 (BIN1), chr8:27607412 (CLU), chr10:11676714 (PVRL2), and chr2:103489151 (TRAPPC6A). The non-APOE shared genetic risk score was constructed using identical methodology as the full shared GRS described above.
Model evaluation for AD or LOE prediction
As part of our sensitivity analysis, we evaluated the performance of our multi-task Elastic Net model in predicting AD and LOE phenotypes by comparing it with a separate Elastic Net model that predicts AD and LOE individually. The primary assessment criterion was the Area Under the Precision-Recall Curve, chosen for its effectiveness in scenarios involving imbalanced datasets, where the number of cases significantly outnumbers the controls70. The same 1,000 iteration steps were applied, and results were reported on the testing set of each iteration. To compare the models, we used the paired Wilcoxon signed-rank test71, as this test is suitable for comparing two metrics derived from the same observations.
Validation in All of Us dataset
To further assess robustness, we validated our results in the All of Us Research Program, a geographically and demographically diverse U.S. cohort of over 500,000 participants72. We employed Data Release v8, which contains longitudinal clinical data for 393,596 individuals through October 1, 2023. All analyses were performed within the All of Us Researcher Workbench under approved data-use protocols, and we derived a comparable subset from the All of Us Research Hub using the same inclusion criteria.
First, we repeated the same association tests of AD and LOE with the Cox proportional hazard models and the Fine and Gray models in the All of Us sample. The same variables were adjusted in these models. Next, we applied the GRS weights trained from the UCLA ATLAS sample to the All of Us sample and constructed an AD-LOE shared GRS for each patient in the All of Us cohort. Similarly, we tested the associations between the shared AD-LOE GRS and both AD and LOE in this sample and compared them to the APOE-ε4 model.
We considered p-values < 0.05 as statistically significant unless otherwise specified. Codes used to produce all analyses in this manuscript are available online (https://github.com/TSChang-Lab/AD_LOE_shared_genetics).
Data availability
Individual electronic health record data are not publicly available due to patient confidentiality and security concerns. Collaboration with the study authors who have been approved by UCLA Health for Institutional Review Board-qualified studies are possible and encouraged. Code is available on GitHub: https://github.com/TSChang-Lab/AD_LOE_shared_genetics.
References
Alzheimer’s and Dementia. Alzheimer’s Disease and Dementia https://alz.org/alzheimer_s_dementia. (2023).
Alzheimer’s Association. Alzheimer’s Association 2024 Alzheimer’s Disease Facts and Figures. (2024).
Stephen, L. J. & Brodie, M. J. Epilepsy in elderly people. Lancet 355, 1441–1446 (2000).
Werhahn, K. J. Epilepsy in the elderly. Dtsch. Arztebl Int. 106, 135–142 (2009).
Faught, E. et al. Incidence and prevalence of epilepsy among older US medicare beneficiaries. Neurology 78, 448–453 (2012).
Stewart, D. & Johnson, E. L. The bidirectional relationship between epilepsy and alzheimer’s disease. Curr. Neurol. Neurosci. Rep. 25, 18 (2025).
Lam, A. D. Linking Late-Onset epilepsy with alzheimer disease. Neurology 101, 551–552 (2023).
Friedman, D., Honig, L. S. & Scarmeas, N. Seizures and epilepsy in alzheimer’s disease. CNS Neurosci. Ther. 18, 285–294 (2012).
Vossel, K. A. et al. Seizures and epileptiform activity in the early stages of alzheimer disease. JAMA Neurol. 70, 1158–1166 (2013).
Kazim, S. F. et al. Early-Onset network hyperexcitability in presymptomatic alzheimer’s disease Transgenic mice is suppressed by passive immunization with Anti-Human APP/Aβ antibody and by mGluR5 Blockade. Front. Aging Neurosci. 9, 71 (2017).
Vossel, K. A. et al. Incidence and impact of subclinical epileptiform activity in alzheimer’s disease. Ann. Neurol. 80, 858–870 (2016).
Vossel, K. A., Tartaglia, M. C., Nygaard, H. B., Zeman, A. Z. & Miller, B. L. Epileptic activity in alzheimer’s disease: causes and clinical relevance. Lancet Neurol. 16, 311–322 (2017).
Romoli, M., Sen, A., Parnetti, L., Calabresi, P. & Costa, C. Amyloid-β: a potential link between epilepsy and cognitive decline. Nat. Rev. Neurol. 17, 469–485 (2021).
Larner, A. J. Epileptic seizures in AD patients. Neuromol Med. 12, 71–77 (2010).
Kunkle, B. W. et al. Genetic meta-analysis of diagnosed alzheimer’s disease identifies new risk loci and implicates Aβ, tau, immunity and lipid processing. Nat. Genet. 51, 414–430 (2019).
Smeland, O. B. et al. Discovery of shared genomic loci using the conditional false discovery rate approach. Hum. Genet. 139, 85–94 (2020).
Bulik-Sullivan, B. K. et al. LD score regression distinguishes confounding from polygenicity in genome-wide association studies. Nat. Genet. 47, 291–295 (2015).
Ramsay, R. E., Rowan, A. J. & Pryor, F. M. Special considerations in treating the elderly patient with epilepsy. Neurology 62, S24–29 (2004).
Johnson, E. L. et al. Association between midlife risk factors and Late-Onset epilepsy: results from the atherosclerosis risk in communities study. JAMA Neurol. 75, 1375–1382 (2018).
Chapin, J. S. et al. APOE epsilon4 is associated with postictal confusion in patients with medically refractory Temporal lobe epilepsy. Epilepsy Res. 81, 220–224 (2008).
Lin, D. Y. & Wei, L. J. The robust inference for the Cox proportional hazards model. J. Am. Stat. Assoc. 84, 1074–1078 (1989).
Fine, J. P. & Gray, R. J. A proportional hazards model for the subdistribution of a competing risk. J. Am. Stat. Assoc. 94, 496–509 (1999).
Stevelink, R. et al. GWAS meta-analysis of over 29,000 people with epilepsy identifies 26 risk loci and subtype-specific genetic architecture. Nat. Genet. 55, 1471–1482 (2023).
Wightman, D. P. et al. A genome-wide association study with 1,126,563 individuals identifies new risk loci for alzheimer’s disease. Nat. Genet. 53, 1276–1282 (2021).
Zhang, Y. & Yang, Q. An overview of multi-task learning. Natl. Sci. Rev. 5, 30–43 (2018).
Tsai, Z. R. et al. Late-onset epilepsy and subsequent increased risk of dementia. Aging (Albany NY). 13, 3573–3587 (2021).
Romanelli, M. F., Morris, J. C., Ashkin, K. & Coben, L. A. Advanced alzheimer’s disease is a risk factor for Late-Onset seizures. Arch. Neurol. 47, 847–850 (1990).
Fu, M. et al. Improving genetic risk modeling of dementia from real-world data in underrepresented populations. Commun. Biol. 7, 1–12 (2024).
Altuna, M., Olmedo-Saura, G., Carmona-Iragui, M. & Fortea, J. Mechanisms involved in epileptogenesis in alzheimer’s disease and their therapeutic implications. Int. J. Mol. Sci. 23, 4307 (2022).
Holtzman, D. M. Role of apoe/Abeta interactions in the pathogenesis of alzheimer’s disease and cerebral amyloid angiopathy. J. Mol. Neurosci. 17, 147–155 (2001).
Kulminski, A. M., Philipp, I., Shu, L. & Culminskaya, I. Definitive roles of TOMM40-APOE-APOC1 variants in the alzheimer’s risk. Neurobiol. Aging. 110, 122–131 (2022).
Hunter, J. M. et al. Emergence of a seizure phenotype in aged Apolipoprotein epsilon 4 targeted replacement mice. Brain Res. 1467, 120–132 (2012).
Soltani Khaboushan, A., Yazdanpanah, N. & Rezaei, N. Neuroinflammation and Proinflammatory cytokines in epileptogenesis. Mol. Neurobiol. 59, 1724–1743 (2022).
Saha, O. et al. The alzheimer’s disease risk gene BIN1 regulates activity-dependent gene expression in human-induced glutamatergic neurons. Mol. Psychiatry. 29, 2634–2646 (2024).
Voskobiynyk, Y. et al. Alzheimer’s disease risk gene BIN1 induces Tau-dependent network hyperexcitability. eLife 9, e57354 (2020).
Ponnusamy, M. et al. Loss of forebrain BIN1 attenuates hippocampal pathology and neuroinflammation in a tauopathy model. Brain 146, 1561–1579 (2023).
Herring, S. K., Moon, H. J., Rawal, P., Chhibber, A. & Zhao, L. Brain clusterin protein isoforms and mitochondrial localization. eLife 8, e48255 (2019).
Milinkeviciute, G. & Green, K. N. Clusterin/apolipoprotein J, its isoforms and alzheimer’s disease. Front. Aging Neurosci. 15, 1167886 (2023).
Zhao, L. & Woody, S. Clusterin (APOJ) in alzheimer’s disease: an old molecule with a new role. in Update on Dementia (ed Moretti, D. V.) (IntechOpen, Rijeka, https://doi.org/10.5772/64233. (2016).
Kalyvas, A. C., Dimitriou, M., Ioannidis, P., Grigoriadis, N. & Afrantou, T. Alzheimer’s disease and epilepsy: exploring shared pathways and promising biomarkers for future treatments. J. Clin. Med. 13, 3879 (2024).
Paudel, Y. N. et al. Tau related pathways as a connecting link between epilepsy and alzheimer’s disease. ACS Chem. Neurosci. 10, 4199–4212 (2019).
Roberson, E. D. et al. Reducing endogenous Tau ameliorates amyloid beta-induced deficits in an alzheimer’s disease mouse model. Science 316, 750–754 (2007).
Blennow, K. & Zetterberg, H. Biomarkers for alzheimer’s disease: current status and prospects for the future. J. Intern. Med. 284, 643–663 (2018).
Ossenkoppele, R., van der Kant, R. & Hansson, O. Tau biomarkers in alzheimer’s disease: towards implementation in clinical practice and trials. Lancet Neurol. 21, 726–734 (2022).
Jack, C. R. Jr et al. Revised criteria for diagnosis and staging of alzheimer’s disease: alzheimer’s association workgroup. Alzheimer’s Dement. 20, 5143–5169 (2024).
Johnson, R. et al. The UCLA ATLAS community health initiative: promoting precision health research in a diverse biobank. Cell. Genomics. 3, 100243 (2023).
Wei, W. Q. et al. Evaluating phecodes, clinical classification software, and ICD-9-CM codes for phenome-wide association studies in the electronic health record. PLOS ONE. 12, e0175508 (2017).
Bastarache, L. Using phecodes for research with the electronic health record: from PheWAS to phers. Annu. Rev. Biomed. Data Sci. 4, 1–19 (2021).
Carroll, R. J., Bastarache, L. & Denny, J. C. R phewas: data analysis and plotting tools for phenome-wide association studies in the R environment. Bioinformatics 30, 2375–2376 (2014).
Lajonchere, C. et al. An Integrated, Scalable, electronic video consent process to power precision health research: Large, Population-Based, cohort implementation and scalability study. J. Med. Internet. Res. 23, e31121 (2021).
Naeim, A. et al. Electronic video consent to power precision health research: A pilot cohort study. JMIR Formative Res. 5, e29123 (2021).
Shaun, P. & Christopher Chang. PLINK 1.9.
Das, S. et al. Next-generation genotype imputation service and methods. Nat. Genet. 48, 1284–1287 (2016).
Wagner, J. K. et al. Anthropologists’ views on race, ancestry, and genetics. Am. J. Phys. Anthropol. 162, 318–327 (2017).
Johnson, R. et al. Leveraging genomic diversity for discovery in an electronic health record linked biobank: the UCLA ATLAS community health initiative. Genome Med. 14, 104 (2022).
Abdi, H. & Williams, L. J. Principal component analysis. WIRE Comput. Stat. 2, 433–459 (2010).
1000 Genomes Project Consortium. 1000 Genomes (20181203_biallelic_SNV). http://ftp.1000genomes.ebi.ac.uk/vol1/ftp/data_collections/1000_genomes_project/release/20181203_biallelic_SNV/.
Belloy, M. E., Napolioni, V. & Greicius, M. D. A quarter century of APOE and alzheimer’s disease: progress to date and the path forward. Neuron 101, 820–838 (2019).
Watanabe, K., Taskesen, E., van Bochoven, A. & Posthuma, D. Functional mapping and annotation of genetic associations with FUMA. Nat. Commun. 8, 1826 (2017).
Wang, K., Li, M. & Hakonarson, H. ANNOVAR: functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 38, e164 (2010).
Kircher, M. et al. A general framework for estimating the relative pathogenicity of human genetic variants. Nat. Genet. 46, 310–315 (2014).
Bulik-Sullivan, B. et al. An atlas of genetic correlations across human diseases and traits. Nat. Genet. 47, 1236–1241 (2015).
Gazal, S. S-LDSC reference files. Zenodo https://doi.org/10.5281/zenodo.7768714 (2017).
HapMap 3. https://www.sanger.ac.uk/data/hapmap-3/.
Tyagi, S. & Mittal, S. Sampling Approaches for Imbalanced Data Classification Problem in Machine Learning. In Proceedings of ICRIC 2019 (eds Singh, P. K., Kar, A. K., Singh, Y., Kolekar, M. H. & Tanwar, S.) 209–221Springer International Publishing, Cham, (2020). https://doi.org/10.1007/978-3-030-29407-6_17.
Generalized Linear Model. (GLM) — H2O 3.28.0.2 Documentation. https://h2o-release.s3.amazonaws.com/h2o/rel-yu/2/docs-website/h2o-docs/data-science/glm.html.
1.1. Linear Models. scikit-learn https://scikit-learn/stable/modules/linear_model.html.
Zou, H. & Hastie, T. Regularization and variable selection via the elastic net. J. Royal Stat. Soc. Ser. B (Statistical Methodology). 67, 301–320 (2005).
McLaren, W. et al. The ensembl variant effect predictor. Genome Biol. 17, 122 (2016).
Davis, J. & Goadrich, M. The relationship between Precision-Recall and ROC curves. in Proceedings of the 23rd international conference on Machine learning - ICML ’06 233–240ACM Press, Pittsburgh, Pennsylvania, (2006). https://doi.org/10.1145/1143844.1143874.
Conover, W. Practical Nonparametric Statistics (3rd Ed.). (John Wiley & Sons, Inc., (1999).
The All of Us Research Program. Curated Data Repository (CDR) version 8 Release Notes. (2025). https://support.researchallofus.org/hc/en-us/articles/30294451486356-Curated-Data-Repository-CDR-version-8-Release-Notes.
Acknowledgements
We gratefully acknowledge the resources provided by the Institute for Precision Health (IPH) and participating UCLA ATLAS Community Health Initiative patients. The UCLA ATLAS Community Health Initiative in collaboration with UCLA ATLAS Precision Health Biobank, is a program of IPH, which directs and supports the biobanking and genotyping of biospecimen samples from participating UCLA patients in collaboration with the David Geffen School of Medicine, UCLA CTSI and UCLA Health.
Funding
MF, TT and TSC was supported by the National Institutes of Health (NIH) National Institute of Aging (NIA) grant K08AG065519-01A1, UH2AG083254, and the Fineberg Foundation. TSC was supported by U54NS123746 and the California Department of Public Health. KV was supported by NIH grants R01 NS033310, R01 AG058820, R01 AG075955, R56 AG074473, and UH2 AG083254. BP was supported by NIH grants R01HG009120, R01MH115676, and R01HG006399.
Author information
Authors and Affiliations
Contributions
MF, TT, KV and TSC contributed to conception and design of the study. MF and TT performed the statistical analysis. MF wrote the first draft of the manuscript. TT wrote sections of the manuscript. MF, TT, BP, KV, and TSC contributed to manuscript revision, read, and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fu, M., Tran, T., Pasaniuc, B. et al. Multi-task learning identifies shared genetic risk for late-onset epilepsy and alzheimer’s disease. Sci Rep 16, 2517 (2026). https://doi.org/10.1038/s41598-025-32329-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-32329-8
