
Abstract
Alternative regulatory pathways for vaccine licensure without traditional Phase III efficacy trials are of increasing priority for epidemic pathogens. Using IXCHIQ, a chikungunya virus vaccine licensed through an accelerated pathway, we demonstrate that prior understanding of disease risk from infection can inform risk–benefit assessments for new vaccines. The mass deployment of IXCHIQ during an outbreak in La Réunion was suspended in those aged over 65 years following three deaths in vaccine recipients, although two appear unlikely to have been vaccine-linked. For individuals aged 18–64 years, we find the vaccine benefits outweigh risks across epidemiological settings. In those aged over 65 years, we estimate a net benefit in large outbreaks, including the La Réunion outbreak, and endemic settings over ten years. There is insufficient evidence of a net benefit in smaller outbreaks or in travellers. We also identify the level of vaccine-associated severe adverse events that would nevertheless still result in a net benefit for a set of endemic and epidemic pathogens. Our generalizable approach can help guide trial recruitment, inform vaccine implementation, and provide a foundation for weighing potential benefits against vaccine-associated risks.
Similar content being viewed by others
Main
Most vaccines are licensed based on the results of Phase III randomized placebo-controlled trials (RCTs), which assess vaccine safety and efficacy in reducing infection, morbidity and mortality. Planning such trials generally requires a predictable and detectable level of disease incidence. Alternative licensure pathways may therefore be needed for candidate vaccines against epidemic pathogens. For such pathogens, outbreaks can be sporadic, short-lived and associated with broader public health emergencies—circumstances that each pose challenges for trial planning and implementation1. The US Food & Drug Administration (FDA) and European Medicines Agency (EMA) therefore allow the use of immune correlates as a trial endpoint, where an immune marker is significantly associated with protection from a clinical endpoint2. These Phase III RCTs typically require fewer participants to determine immunogenicity than would be needed to detect clinical efficacy, as they instead measure the proportion of trial participants who mount a pre-specified immune response. Although such trials are still designed to detect safety outcomes, including serious adverse events (SAEs), their smaller size limits the power to detect rare SAEs (<1 in 1,000). Additionally, they may not capture safety signals in underrepresented subpopulations. The evidence generated may therefore be insufficient for robust quantitative assessments of benefits and risks.
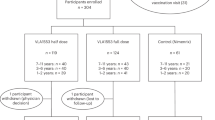
The recent licensure and rollout of the chikungunya vaccine IXCHIQ illustrates these challenges. IXCHIQ is a single-dose live attenuated vaccine developed by Valneva for preventing chikungunya disease3. Chikungunya virus (CHIKV) is a major public health threat across global tropical and subtropical regions, causing disease manifestations ranging from acute febrile disease to encephalitis, long-term disabling arthralgia or arthritis, and death4,5,6. Age and comorbidities are risk factors for severe and fatal CHIKV infections4,5. There are an estimated 34 million CHIKV infections and over 3,000 deaths each year, but CHIKV outbreaks are unpredictable, explosive and often short-lived, making Phase III efficacy RCTs difficult or even impossible to implement6,7. Instead, the FDA and EMA licensed IXCHIQ in 2023/2024 based on a correlate of protection identified through passive transfer studies in non-human primates and confirmed in human seroepidemiological cohort studies8. In the Phase III safety and immunogenicity RCT (VLA1553-301), 263 of 266 vaccine recipients (98.9%) in the immunogenicity subset developed neutralizing antibodies within 28 days, with responses sustained through three years of follow-up3,8,9,10. Among 3,082 IXCHIQ recipients followed for safety outcomes, two vaccine-associated SAEs were reported in individuals aged 58 and 66 years. The trial reported no age-related differences in immunogenicity or safety, although only 11% of individuals were aged 65+ (n = 463). The trial had a 94% probability of detecting at least one rare vaccine-associated SAE among the 3,000 vaccinated participants, but it was not powered to detect such events specifically in the higher-risk 65+ age group.
The first mass vaccination with IXCHIQ began in April 2025 in response to a CHIKV outbreak in La Réunion that started in August 2024, with 54,500 cases and 40 confirmed deaths as of September 202511. Mathematical modelling supporting the outbreak response estimated an attack rate (the proportion of an at-risk population that is infected) of 18–32% (S. Cauchemez, personal communication). As part of epidemic control efforts, elderly individuals with comorbidities were initially prioritized for vaccination. An estimated 5,600 doses were administered to those aged 65+ years before the EMA suspended IXCHIQ vaccination in this age group due to three deaths in vaccinated male individuals aged 77, 84 and 88 years, all of whom had multiple chronic comorbid conditions12 (Valneva, personal communication). Only one death is likely to be associated with the IXCHIQ vaccine; however, the limited representation of individuals aged 65+ years in the Phase III trial meant that there was insufficient evidence to confirm that the benefits of vaccination outweigh risks in this age group. In July 2025, the EMA’s safety committee lifted the age restrictions but recommended evaluation of IXCHIQ risks and benefits before use. Conversely, in August 2025, the FDA permanently suspended IXCHIQ’s licence, citing serious safety concerns and uncertainty in the clinical efficacy of IXCHIQ in the absence of Phase III efficacy trials.
The incidence of cardiovascular complications and blood clots from COVID-19 vaccines has motivated previous analytical exercises to quantify risk–benefit trade-offs13,14,15. However, these studies focused exclusively on COVID-19 vaccines and did not assess the strength of the evidence for vaccine benefits. In this Article we present a generalizable pathogen- and vaccine-agnostic framework for evaluating vaccine risk–benefit profiles that account for age-related variation in disease severity and vaccine-associated SAEs, as well as uncertainty in SAE risk estimates when alternative licensure pathways are used. We then apply this model to IXCHIQ, as well as a set of endemic (SARS-CoV-2) and other epidemic (measles, Ebola) pathogens to help guide future vaccine implementation.
Results
Quantifying the risks and benefit of vaccines
We consider four factors when comparing a vaccine’s risks and benefits: the risk of infection (defined as the attack rate), the risk of a clinical outcome (morbidity or mortality) given infection, vaccine efficacy against clinical outcomes, and risk of vaccine-associated SAEs, including death. We define a vaccine-associated SAE as any untoward medical occurrence that results in death, is life-threatening, requires or prolongs hospitalization, or results in persistent or substantial disability or incapacity following immunization16. Specific population strata may experience differing adverse outcome risks from either infection or vaccination, for example, by age, sex, pregnancy status and presence of comorbidities, meaning that risk–benefit assessments differ across subgroups. For example, if the risk of severe outcomes following infection is U-shaped by age (Extended Data Fig. 1a), as is common for many pathogens, but the risk of SAEs is age-independent, vaccine benefits will be greatest in infants and the elderly (Extended Data Fig. 1b). If, by contrast, the risk of SAEs also increases with age, greater benefits may shift to younger age groups (Extended Data Fig. 1c). Vaccine net benefit also scales with attack rate and vaccine efficacy (Extended Data Fig. 1d,e).
Here we present a generalized framework that quantifies severe outcomes averted by vaccination (Fig. 1), the maximum acceptable risk of vaccine-associated SAEs (Fig. 2) and the probability that vaccine benefits outweigh risks (Extended Data Fig. 2), across varying levels of infection severity, attack rates and vaccine efficacy. We characterize the attack rate through four epidemiological scenarios—a small outbreak (5% attack rate), a large outbreak (30% attack rate), an endemic setting (average annual infection of 2.4% over ten years6) and a traveller (ten days exposure risk during a large outbreak). We do not consider indirect vaccination impacts such as the acquisition of herd immunity or changes in transmission dynamics, as our aim is to assess an individual’s risk–benefit profile, rather than considering population benefits. Considerations of indirect effects also require dynamic models and strong assumptions about the infection-blocking nature of the vaccine, vaccine uptake, pre-existing immunity from natural infection, and population mixing patterns, which may differ across settings, limiting their generalizability.

Positive and negative cases averted (per 10,000 in each age group) are coloured in orange and pink, respectively. The dashed diagonal line indicates the threshold of zero net benefit. The risks associated with chikungunya infection and vaccination for each age group (per 10,000) are denoted by the shapes.

Maximum acceptable probability of severe outcome following vaccination (colour scale) to ensure that vaccine benefits outweigh the risks, as a function of the attack rate (x axis) and the probability of severe outcome following infection (y axis). Data points represent disease–age group combinations: CHIKV (purple), COVID-19 in 2020 (dark pink) and 2022 (light pink), EV (green), MeV in the current era (light blue) and pre-vaccination era (dark blue). Symbols indicate age groups: open squares (25–44 years), open triangles (18–64 years), filled triangles (65+ years) and filled squares (75+ years). Estimates are shown assuming 50% or 95% vaccine efficacy (VE) against severe outcomes. Severe outcomes following infection are medically attended disease (CHIKV), hospitalization (COVID-19, MeV) or death (EV). See Extended Data Table 1 for a full overview of parameters. EV, ebola virus; MeV, measles virus; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
For each epidemiological scenario, we estimate the number of severe outcomes averted by a vaccine with 50% or 95% efficacy. The boundary between net benefit and net harm (dashed line) highlights the trade-off between the risks of adverse outcomes from infection versus vaccination (Fig. 1). As the risk of severe outcomes following infection increases (y axis), net benefits persist (orange areas), even for vaccines associated with greater SAE risk (x axis). We also assess the strength of evidence for vaccine benefit by estimating the probability that benefits outweigh risks (Extended Data Fig. 2). To incorporate uncertainty in infection and vaccine risk estimates, we use a Bayesian approach that models both as random variables. The probability of vaccine benefit increases nonlinearly as the risk of severe outcomes given infection increases (Extended Data Fig. 2). Additionally, even when no SAEs are observed among 1,000 vaccinated individuals, the probability of net benefit may still be <0.95 when the infection attack rate or risk of severe outcomes given infection is low. Increasing the number vaccinated to 10,000 with no observed SAEs increases the probability of vaccine benefit.
Using the same framework, we next identify upper bounds of acceptable vaccine risk that still support a conclusion of net benefit for any disease, based on its attack rate and the probability of severe outcomes given infection (Fig. 2 and Extended Data Table 1). For instance, if the severe outcome under consideration is hospitalization, we calculate the maximum tolerable probability of vaccine-associated hospitalization while still concluding overall vaccine benefit. For a highly lethal pathogen like the Ebola virus (60% infection fatality rate, IFR), a 95% efficacious vaccine provides net benefit with vaccine-associated mortality risks as high as 4%. Equally, for a virus with a very high attack rate like measles in the pre-vaccination era, a vaccine-associated hospitalization risk of up to 17% would still be acceptable. Our framework also highlights how acceptable vaccine-associated risk can vary across age groups and over time (Fig. 2). For example, widespread measles vaccination greatly reduced the attack rate, lowering the acceptable vaccine risk threshold. Conversely, although the Omicron variant of SARS-CoV-2 in 2022 was associated with a lower probability of hospitalization compared to earlier variants, the higher attack rate meant that, regardless of age, the acceptable level of vaccine-associated risk remained similar to that earlier in the pandemic (Fig. 2).
IXCHIQ vaccine as a case study
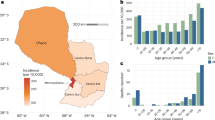
Due to the suspension of vaccination for individuals aged 65+ years during the CHIKV outbreak in La Réunion, we next applied our modelling framework to the IXCHIQ vaccine as a detailed case study. During the Phase III immunogenicity trial, two non-fatal vaccine-linked SAEs were reported, one in the 18–64-year age group (n = 2,736 vaccinated individuals) and one in the 65+ age group (n = 346)3. As of 15 August 2025, ~51,400 IXCHIQ doses had been administered globally, including ~18,000 doses in individuals aged 65+ years (Extended Data Fig. 3a) (Valneva, personal communication). Among vaccinated individuals, 29 non-fatal SAEs (seven aged 18–64 years and 22 aged 65+ years) and three fatal SAEs (all aged 65+ years) were reported. Only one fatality was linked to vaccination (encephalitis with vaccine strain CHIKV-positive blood and cerebrospinal fluid), with most of the non-fatal SAEs also consistent with chikungunya-like illness (Extended Data Fig. 3b). We therefore include the 29 non-fatal and one fatal SAE in the main analysis, with a sensitivity analysis on the number of fatal SAEs. This corresponds to 2.1 (95% confidence interval (CI): 0.9–4.4) and 11.9 (95% CI: 7.5–18.1) non-fatal SAEs per 10,000 individuals aged 18–64 and 65+ years, respectively. The estimated death rates are 0.0 (95% CI: 0.0–1.1) and 0.5 (95% CI: 0.0–3.0) per 10,000 in the same two age groups (Extended Data Fig. 3c), indicating that the probability of SAEs and death following IXCHIQ vaccination increases with age. Similarly, the risk of disease and death from CHIKV infection increases with age4,5,6. A study in Paraguay estimated an IFR more than 20-fold higher in individuals aged 65+ years compared with those aged 18–64, with corresponding estimates of 1,300.9 (95% CI: 1,283.5–1,318.3) and 631.4 (95% CI: 627.3–635.5) medically attended cases per 10,000 in these groups, respectively (Extended Data Fig. 3c)4.
Using our risk–benefit framework, we model the expected number of clinical chikungunya cases, deaths and disability-adjusted life years (DALYs), by age group and epidemiological scenario, both with and without vaccination (Fig. 3). We consider only direct impacts and assume 100% coverage of IXCHIQ with 95% efficacy against clinical outcomes, and that vaccine SAEs are equivalent to medically attended chikungunya. We account for uncertainty in the risk of severe outcomes associated with both infection and vaccination. In all epidemiological scenarios, we find that vaccinating individuals aged 18–64 years reduces the number of medically attended chikungunya cases/SAEs, deaths and DALYs (Fig. 3). Conversely, for those aged 65+ years, net benefit or risk depends on the epidemiological scenario. There is a clear benefit in endemic settings and large outbreaks, with up to 359 (95% CI: 352–366) cases, three (95% CI: 2–4) deaths and 47 (95% CI: 35–55) DALYs averted per 10,000 vaccinated. Vaccinating individuals aged 65+ years is also beneficial when comparing chikungunya cases and non-fatal SAEs in small outbreaks and among travellers (Fig. 3d). However, in these settings, vaccination may also increase the risk of death, and the lower bound of DALYs averted crosses zero, indicating that excess DALYs are possible (Fig. 3e,f). Overall, an attack rate >5% confers net mortality benefits regardless of age group (Extended Data Fig. 4). As the attack rate in La Réunion is estimated to be 18–32%, our analysis suggests that vaccination remains beneficial in reducing disease and mortality in both age groups in this setting.

a–c, Expected number of medically attended chikungunya cases and SAEs (a), deaths (b) and DALYs (c) per 10,000 individuals in each age group in the presence or absence of vaccination across different epidemiological scenarios. d–f, Medically attended chikungunya cases and SAEs (d), deaths (e) and DALYs (f) averted across different epidemiological scenarios and age groups. Positive and negative cases averted (per 10,000 in each age group) are coloured in blue and red, respectively. Bars represent mean estimates and error bars represent 95% uncertainty intervals derived from n = 100,000 binomial samples. See Methods for full details of assumptions.
Next, we evaluate the strength of the evidence that the benefits of IXCHIQ outweigh its potential risks. Considering non-fatal SAEs first, we calculate the probability that the number of medically attended chikungunya cases averted by vaccination is greater than vaccine-associated SAEs, using both the data available at the end of the Phase III immunogenicity trial and all the data available today (that is, post-licensure surveillance including SAEs identified during mass vaccination in La Réunion; Fig. 4). Assuming 95% vaccine efficacy, we find that at the end of the trial, there was a >0.95 probability that the vaccine’s benefit outweighed the risk of SAEs in all epidemiological scenarios for the 18–64-year age group and in the large outbreak and endemic settings for the 65+ age group. Using all the data available today, all age groups and epidemiological scenarios show that the vaccine benefit outweighs the risk of non-fatal SAEs (Fig. 4).

Open diamonds show the evidence available at the end of the trial, and filled circles show all evidence currently available. Vertical dashed lines denote 95% probability (n = 100,000 posterior samples).
Next, considering deaths, we find that at the end of the Phase III trial, there was insufficient evidence that the vaccine benefits outweigh the risks across all scenarios considered (Fig. 4). Despite the detection of one vaccine-associated death during mass vaccination, the additional doses administered increase the probability of vaccine benefit against death for all scenarios. Consequently, there is now a ≥0.95 probability that the vaccine reduces deaths in the 65+ year age group in large outbreaks and endemic settings. The lower evidence for net mortality benefit in the 18–64 year age group reflects the low IFR (Extended Data Fig. 3). We estimate that demonstrating net mortality benefit in this age group during a large outbreak would require observing no deaths in >100,000 vaccinated individuals (Extended Data Fig. 5). This highlights that, for some pathogens or subpopulations, clinical trials may never generate sufficient evidence to conclusively show that benefits outweigh risks, despite the absolute risk remaining very low. Comparatively, for the Ebola virus, even at a low attack rate (5%), no deaths in 67 vaccinated individuals are sufficient to conclude that the mortality benefits outweigh the risks (Extended Data Fig. 5). For SARS-CoV-2 in previously unexposed individuals, observing no deaths in 3,400 vaccinated individuals would provide similar comfort.
We conducted several sensitivity analyses on the assumptions made during the main analysis. First, we assumed 95% IXCHIQ efficacy, although this was not measured directly during the clinical trial. Assuming 50% efficacy, there is still >0.95 probability of benefit in all age groups and epidemiological scenarios comparing SAEs to medically attended chikungunya (Extended Data Fig. 6a). Overall, ensuring net benefit against medically attended chikungunya, regardless of age or epidemiological context, requires an efficacy of >24% (Extended Data Fig. 6b). Net mortality benefit in those aged 65+ years requires efficacies of >16%, >22% and >88% in large outbreaks, endemic settings and small outbreaks, respectively. In contrast, even a perfect vaccine does not provide net mortality benefit for travellers. Second, there is not strict comparability between vaccine SAEs and medically attended chikungunya cases. If 50% of medically attended CHIKV infections are equivalent in health burden to SAEs (consistent with chronic sequelae in half of medically attended cases17), the vaccine still provides a net benefit across all age groups and epidemiological scenarios (Extended Data Fig. 7). Alternatively, if fewer SAEs are ultimately linked to vaccination, the absolute net benefit would be greater than estimated here. Finally, if all three deaths observed in the 65+ year age group were linked to vaccination, we would only estimate net reductions in DALYs in large outbreaks and endemic settings, and with lower probabilities of benefit (0.89 and 0.67, respectively; Extended Data Figs. 8 and 9).
Discussion
We have presented a generalizable pathogen- and vaccine-agnostic framework to critically assess the risk–benefit trade-offs of vaccines licensed through alternative pathways, where risks are incompletely characterized due to the absence of large Phase III safety and efficacy RCTs or underrepresentation of high-risk populations. This framework allows us to characterize both the absolute risk–benefits (cases averted) as well as the strength of the evidence (probability of benefit). We show that both the underlying infection risk and subgroup risk of severe outcomes are key to identifying settings where vaccine benefits reliably outweigh the risks. We identify thresholds of vaccine-associated SAEs that still result in a net benefit for multiple endemic and epidemic pathogens, showing how acceptable risk thresholds for measles and SARS-CoV-2 vary over time with changing disease dynamics. These findings highlight how vaccine policy can be guided by both pathogen characteristics and evolving epidemiological context. For CHIKV, we show that the benefits of IXCHIQ outweigh SAE risks across all age groups and epidemiological scenarios when compared to medically attended or chronic chikungunya, consistent with the aim of CHIKV vaccines to reduce long-term morbidity, especially arthralgia.
Conversely, the evidence for IXCHIQ’s benefit against mortality depends on age and epidemiological context. We estimate that the vaccine reduces the risk of deaths in the 18–64 year age group in all epidemiological scenarios. However, the low IFR in this population means there is currently insufficient evidence to conclude that the mortality reduction outweighs the risks. It is only after observing no deaths in over 100,000 vaccinated individuals that we can conclude benefit against mortality. In this context of very low absolute risk in the 18–64 year age group, the clear net benefit of the vaccine in preventing severe disease and DALYs should guide decision-making. In older individuals, where the absolute risk of mortality from both vaccine and infection is higher, our findings suggest that, despite one vaccine-linked death, IXCHIQ remains beneficial in large outbreaks and endemic settings. Given the high attack rate estimated in the recent La Réunion outbreak, vaccination remained beneficial in those aged 65+ years. If all three deaths among vaccine recipients were vaccine-related, we still estimate a net reduction in DALYs from vaccination in large outbreaks and endemic settings, although the evidence for benefit is weaker. Critically, we did not account for comorbidities, which are strongly linked to the incidence of SAEs and were part of the vaccination campaign strategy developed by the authorities in La Réunion. Also, there have been more SAEs in males than in females. With detailed disease and SAE data by comorbidity and sex, risk–benefit estimates could be refined to more specific subpopulations.
Our findings show that using the existing understanding of the age-specific risks from CHIKV infection, it would have been possible to conclude at the end of the Phase III trial (~3,000 vaccinated individuals) that vaccine benefits against clinical disease outweighed SAE risks in the 18–64 year age group across all epidemiological scenarios, and in older age groups under higher attack rates. Accounting for age and other factors associated with the risk of severe infection outcomes during participant recruitment in vaccine trials can improve the ability to generate an evidence base of a vaccine’s risks and benefits. In the case of IXCHIQ, this would have involved recruiting more participants aged 65+ years, who comprised only 11% of trial participants, despite being the population at greatest risk of severe CHIKV disease. Specifically, assuming a rare SAE (1/1,000) and 95% efficacy, enroling 4,000 individuals aged 18–64 years and 1,000 aged 65+ years in the vaccine arm would have demonstrated net benefit across all epidemiological scenarios and age groups, when compared to medically attended chikungunya.
The attack rate is a critical component in assessing a vaccine’s net benefit. In a new outbreak, this means decision-making must be supported by epidemic forecasting, anticipating the likely size of the epidemic18. Typically, a public health response assumes a high attack rate to support aggressive vaccination; however, this may cause vaccine-associated harm if transmission is unexpectedly low. Conversely, a cautious approach to risk–benefit assessments, assuming a small outbreak, may underuse an effective vaccine if the outbreak escalates. Estimating pre-existing immunity through serosurveys and evaluating the likely impact of other control measures (for example, vector control for CHIKV) is therefore essential. As CHIKV outbreaks become more frequent and vaccine-induced antibodies are broadly neutralizing and expected to persist for years, vaccinated individuals are likely to remain protected in future outbreaks6,19.
True efficacy estimates are unavailable for vaccines licensed through accelerated pathways without RCTs with clinical endpoints. Additionally, efficacy may be lower in older age groups or those with comorbidities. Our model can be used to identify the minimum vaccine efficacy necessary for the benefits of a vaccine to outweigh its risks in specific subgroups. In the case of IXCHIQ, we demonstrate that 25% vaccine efficacy would lead to a net benefit for medically attended chikungunya across all scenarios. However, even with 100% vaccine efficacy, travellers aged 65+ years do not show a net mortality benefit. This is in line with the FDA’s decision to suspend IXCHIQ’s licence, based on a risk–benefit analysis for travellers. Conversely, our finding that IXCHIQ is beneficial regardless of age in endemic settings over ten years and large outbreaks is also consistent with the EMAs’ recommendation to use IXCHIQ when the risk of infection is high. Risk–benefit analyses in endemic settings, looking at shorter-term impacts, may find less benefit. These differences in recommendations highlight the importance of clear communication of post-marketing safety data, as well as transparent risk–benefit analyses and the epidemiological context they relate to, to maintain public trust and support evidence-based decision-making.
The underlying probability of CHIKV death has only recently been quantified using a combination of death registry data and a seroprevalence study following a major outbreak in Paraguay4. Assuming an attack rate of 25% for the current outbreak in La Réunion, consistent with mathematical modelling estimates supporting the outbreak response, we estimate ~225,000 infections in a population of 900,000. Based on the 40 deaths currently reported, this corresponds to an IFR of 18 deaths per 100,000 infections11—consistent with the ~13 deaths per 100,000 estimated in Paraguay4. Planned seroprevalence studies in La Réunion will help quantify the true infection burden in the territory, supporting a comparison of IFRs in different populations, which we have shown is vital for quantifying vaccine risks and benefits.
Our approach relies on necessary simplifications and assumptions. We did not account for indirect vaccine effects. An infection-blocking vaccine could confer herd immunity, benefiting unvaccinated individuals, including those ineligible, such as pregnant or immunocompromised people. Our estimates relied on IFRs from a single population and outbreak, and we assumed that medically attended CHIKV disease was approximately equivalent in disease burden to non-fatal vaccine-associated SAEs. Both vaccine-associated SAEs and medically attended CHIKV cases probably encompass substantial variability in symptom severity and healthcare-seeking behaviour. Nonetheless, varying the probability of severe disease from vaccination or infection consistently showed substantial vaccine benefit across age groups in high-transmission settings. We assume that the morbidity and mortality associated with vaccination are equivalent to those resulting from infection. However, vaccine-related risks are often perceived as less acceptable, and such perceptions can influence behaviour as strongly as empirical evidence20. Addressing vaccine hesitancy requires clear communication of vaccine benefits, alongside transparent acknowledgement of uncertainties and a recognition of contexts or subpopulations in which individual risks may outweigh potential benefits. We did not consider severe CHIKV infection outcomes such as encephalitis, a poorly understood disease manifestation, especially in younger age groups21,22. Protection from encephalitis, arthralgia and other chronic sequelae will be a further benefit from the vaccine not considered here, including economic impacts. Finally, we assume that a traveller is exposed to a high incidence outbreak for ten days; however, an individual’s risk will depend strongly on their activities and use of protective measures.
Accelerated pathways are an increasingly important avenue for licensing vaccines where it is not feasible or practical to conduct randomized placebo-controlled Phase III safety and efficacy trials. In addition, it is faster, cost-effective and logistically/operationally preferable to do an immunogenicity study when possible, including for many non-epidemic pathogens, such as pneumococcal vaccines23. There must exist high confidence in vaccines approved through these mechanisms. We have shown that even when the safety of a vaccine is not fully characterized during licensure, we can identify upper bounds of acceptable vaccine risk, quantify the strength of the evidence that the benefits of a candidate vaccine outweigh the risks, and identify specific epidemiological scenarios and subpopulations that benefit from vaccination.
Methods
Our analysis employs a risk–benefit framework to evaluate vaccine safety by comparing the expected harm prevented through vaccination against the potential harm caused by vaccine-associated SAEs. We first establish a simple model that calculates the number of severe outcomes expected in vaccinated versus unvaccinated populations under different epidemic scenarios, accounting for vaccine efficacy and baseline disease risk. From this, we derive a safety threshold—the maximum acceptable vaccine risk that still provides net benefit. We then implement this framework probabilistically using Bayesian inference to incorporate uncertainty in both disease and vaccine risk estimates, allowing us to calculate the probability that vaccination provides a net benefit for different risk groups and outcomes.
Quantifying the risks and benefits of vaccines
To understand the risks and benefits of a vaccine, we first estimate the risk of severe outcomes for vaccinated and unvaccinated individuals, given the underlying risk of infection, the risk of severe outcomes following infection, vaccine efficacy and the risk of vaccine-associated SAEs. We assume that the probability of severe outcomes following infection and vaccine-associated SAEs vary by risk group (for example, age). We characterize the underlying risk of infection through four scenarios: a small outbreak (5% attack rate), a large outbreak (30% attack rate), endemic transmission over ten years (2.4% annual infection risk6) and short-term exposure (ten days) of a traveller during a large outbreak.
The number of severe outcomes (S) by vaccination status (v = vaccination, nv = no vaccination) by risk group a is calculated as
where i is the epidemiological scenario index, λi is the attack rate for scenario i, αa is the age-specific probability of severe outcome given infection, δa is the age-specific probability of vaccine-linked SAEs, v is the vaccine efficacy against severe outcome, and N is the population size.
The number of severe outcomes averted by vaccination is therefore
Vaccine safety threshold
We evaluate a vaccine’s safety by comparing the observed risk of SAEs after vaccination to the expected background risk of severe outcomes given infection without vaccination. Using the same notation as above, to conclude vaccine benefit, we require that the total risk with vaccination does not exceed the risk without vaccination:
Rearranging, we obtain the maximum acceptable vaccine risk probability δmax:
For vaccination to provide net benefit, we require δa ≤ δmax.
Probabilistic framework that benefits outweigh risks
To account for uncertainty in the infection and vaccine risk estimates, we adopt a Bayesian approach that treats both infection and vaccine risks as random variables. Specifically, we calculate the probability that the vaccine benefit threshold (\({\delta }_{max}={\alpha }_{a}\times {\lambda }_{i}\times \nu\)) exceeds the actual vaccine risk (δa).
For each adverse outcome (vaccine or infection) we use conjugate Bayesian inference. We assume non-informative uniform priors for the risks of severe outcomes given infection and vaccination:
We assume that the number of adverse outcomes x in n total exposures (doses or infection) follows a binomial distribution:
where p = αa when x corresponds to adverse outcomes given infection, and p = δa when x corresponds to vaccine-linked SAEs.
The posterior distribution of adverse infection or vaccine-linked outcomes therefore follow a beta distribution:
Drawing 100,000 samples from the posterior distributions of both αa (adverse infection outcomes) and δa (vaccine-linked SAEs), we calculate the probability of vaccine benefit as the proportion of samples where δa ≤ δmax. This represents the probability that vaccination provides net benefit given the observed data.
Power to detect at least one death from vaccination
Finally, we extended the safety threshold δmax = αa × λi × ν to determine the minimum sample size required to conclude that the benefits of a vaccine in preventing death outweigh the risks, when no vaccine-associated deaths have been observed. Specifically, we calculate the sample size required to detect at least one vaccine-associated death with 80% power, assuming a one-sided exact binomial test and that the true vaccine risk is equal to the safety threshold δmax:
where \(x \sim \mathrm{Binomial}(n,\,{\delta }_{\max })\).
Application to the IXCHIQ vaccine
Next, we apply the framework described above to evaluate the IXCHIQ vaccine, analysing two distinct severe outcomes: medically attended CHIKV cases and death. For each outcome, we estimate separate risk parameters for infection and vaccination by age group (18–64 and 65+ years).
Data
IXCHIQ vaccine benefits are defined as the prevention of medically attended CHIKV cases (that is, severe cases requiring hospitalization or medical care) or deaths following infection. Estimates of the proportion of infections leading to medically attended cases and deaths were based on data from a large chikungunya outbreak in Paraguay (2022–2023), where a post-outbreak seroprevalence study was conducted (298 deaths, 142,412 medically attended cases and 2.3 million infections)4. The limited prior circulation of chikungunya allowed for a more accurate estimation of the IFR, as post-outbreak seroprevalence more closely reflected recent infections rather than background immunity. Medically attended cases were defined using national surveillance data and included symptomatic individuals who sought care and met the clinical case definition (sudden onset of fever and arthralgia or disabling arthritis not explained by another condition)4. In the 18–64 year age group, there were 65 deaths, 80,342 cases and 1,272,530 infections. In the 65+ year age group, there were 178 deaths, 18,747 cases and 144,113 infections.
IXCHIQ vaccine risk outcomes include SAEs (both non-fatal and fatal). To compare vaccine risks and benefits, we assume that medically attended CHIKV cases are equivalent to a non-fatal SAE, but vary this in a sensitivity analysis. We calculated the proportion of vaccine-associated SAEs stratified by age group (18–64 and 65+ years) from data on the number of vaccine doses administered and the number of vaccine-associated SAEs12 (Valneva communication). In the 18–64 year age group, there were seven non-fatal SAEs and zero fatal SAEs out of 32,949 vaccinated individuals. In the 65+ year age group, there were 22 non-fatal SAEs and one fatal SAE out of 18,445 vaccinated individuals.
Statistical analysis
We estimated the risks and benefits of the IXCHIQ vaccine by calculating the net number of severe outcomes averted using equation (3). To incorporate uncertainty in the observed data, we sampled 100,000 times from binomial distributions representing the number of observed events (medically attended cases and deaths given infection, and fatal and non-fatal SAEs) given the total exposures (infections or vaccine doses). From these samples, we estimated the distribution of outcomes averted for each age group and epidemic scenario.
We also evaluated the risks and benefits of IXCHIQ using DALYs, which represent the total number of healthy years lost due to illness, disability and premature death. DALYs are defined as the sum of years of life lost (YLLs) and years lived with disability (YLDs). YLLs were calculated using the average life expectancy of individuals in La Réunion and the probability of death associated with infection or vaccination described above. To calculate YLDs, we assumed that 50% of infections are symptomatic6. Among symptomatic infections, 13% (ages 18–64 years) and 26% (ages 65+ years) require medical attention4, while the remaining 87% and 74%, respectively, are mild cases. We assumed that 50% of medically attended chikungunya cases develop chronic arthralgia4. Mild and medically attended acute cases were assumed to last seven days, with disability weights of 0.006 and 0.133, respectively24. Chronic chikungunya was assumed to last six months with a disability weight of 0.233 (refs. 25,26). As above, we assumed that SAEs are equivalent to medically attended chikungunya, with a duration of seven days and a disability weight of 0.133.
Additionally, we estimated the probability that vaccination provides net benefit for each outcome and age group separately. Using the posterior sampling approach (equations (6)–(9)), we drew 100,000 samples from the Beta distributions of infection risks (αa for deaths and cases) and vaccine risks (δa for SAEs), then calculated the proportion of samples where δa ≤ δmax for each combination of outcome (deaths or medically attended cases) and age group (18–64 or 65+ years).
We initially assumed a fixed vaccine efficacy of 95% for all age groups3. We included sensitivity analyses where we assumed vaccine efficacies ranging from 0 to 100%, attack rates of 0–50%, more or no vaccine-associated deaths, and that SAEs are instead comparable to chronic chikungunya cases17.
All analysis was conducted in R version 4.4.3 (28 February 2025).
Reporting Summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this Article.
Data availability
All data are available at https://github.com/bnc19/vaccine_risk_benefits. Data on IXCHIQ SAEs and doses administered are from personal communications with Valneva.
Code availability
Code is available at https://github.com/bnc19/vaccine_risk_benefits.
References
Openshaw, P. J. M. Using correlates to accelerate vaccinology. Science 375, 22–23 (2022).
Liberti, L. et al. FDA facilitated regulatory pathways: visualizing their characteristics, development and authorization timelines. Front. Pharmacol. 8, 161 (2017).
Schneider, M. et al. Safety and immunogenicity of a single-shot live-attenuated chikungunya vaccine: a double-blind, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 401, 2138–2147 (2023).
Pérez-Estigarribia, P. E. et al. Modeling the impact of vaccine campaigns on the epidemic transmission dynamics of chikungunya virus outbreaks. Nat. Med. 31, 2335–2341 (2025).
de Souza, W. M. et al. Spatiotemporal dynamics and recurrence of chikungunya virus in Brazil: an epidemiological study. Lancet Microbe 4, e319–e329 (2023).
Ribeiro Dos Santos, G. et al. Global burden of chikungunya virus infections and the potential benefit of vaccination campaigns. Nat. Med. 31, 2342–2349 (2025).
Rezza, G. & Weaver, S. C. Chikungunya as a paradigm for emerging viral diseases: evaluating disease impact and hurdles to vaccine development. PLoS Negl. Trop. Dis. 13, e0006919 (2019).
Roques, P. et al. Effectiveness of CHIKV vaccine VLA1553 demonstrated by passive transfer of human sera. JCI Insight 7, e160173 (2022).
Valneva Reports Positive Three-Year Antibody Persistence Data for its Single-Shot Chikungunya Vaccine IXCHIQ® (Valneva, 2024); https://valneva.com/press-release/valneva-reports-positive-three-year-antibody-persistence-data-for-its-single-shot-chikungunya-vaccine-ixchiq
Yoon, I.-K. et al. Pre-existing chikungunya virus neutralizing antibodies correlate with risk of symptomatic infection and subclinical seroconversion in a Philippine cohort. Int. J. Infect. Dis. 95, 167–173 (2020).
Chikungunya à La Réunion: Semaine du 01 au 07 Septembre 2025. Chikungunya in Reunion: Week of September 1 to 7, 2025 (Santé Publique France, 2025); https://www.lareunion.ars.sante.fr/chikungunya-la-reunion-point-de-situation
Campagne Vaccinale Contre le chikungunya: Point de Situation sur la Surveillance du Vvaccin Ixchiq (Chikungunya Vaccination Campaign: Update on Ixchiq Vaccine Monitoring) (ANSM, 2025); https://ansm.sante.fr/actualites/lansm-accompagne-la-campagne-vaccinale-contre-le-chikungunya-vaccin-ixchiq
Lau, C. L. et al. Risk-benefit analysis of the AstraZeneca COVID-19 vaccine in Australia using a Bayesian network modelling framework. Vaccine 39, 7429–7440 (2021).
Lewis, G. & Bonsall, M. Risk-benefit analysis of emergency vaccine use. Sci. Rep. 12, 7444 (2022).
Tran Kiem, C. et al. Benefits and risks associated with different uses of the COVID-19 vaccine Vaxzevria: a modelling study, France, May to September 2021. Euro Surveill 26, 2100533 (2021).
Serious AEFI (WHO, 2018); https://www.who.int/groups/global-advisory-committee-on-vaccine-safety/topics/aefi/serious-aefi
Kang, H. et al. Chikungunya seroprevalence, force of infection, and prevalence of chronic disability after infection in endemic and epidemic settings: a systematic review, meta-analysis and modelling study. Lancet Infect. Dis. 24, 488–503 (2024).
Andronico, A. et al. Comparing the performance of three models incorporating weather data to forecast dengue epidemics in Reunion Island, 2018–2019. J. Infect. Dis. 229, 10–18 (2024).
Weber, W. C. et al. The approved live-attenuated chikungunya virus vaccine (IXCHIQ®) elicits cross-neutralizing antibody breadth extending to multiple arthritogenic alphaviruses similar to the antibody breadth following natural infection. Vaccines 12, 893 (2024).
Wilson, C. B. & Marcuse, E. K. Vaccine safety–vaccine benefits: science and the public’s perception. Nat. Rev. Immunol. 1, 160–165 (2001).
Sampaio, M. P. et al. Detection of encephalitis-causing viruses reveals predominance of chikungunya virus in the state of Bahia, Brazil. Int. J. Infect. Dis. 145, 107090 (2024).
Bhardwaj, N., Kumar, V., Singh, P. & Kaur, J. Chikungunya encephalitis: a case report. J. Acute Dis. 13, 157–160 (2024).
King, D. F. et al. Realising the potential of correlates of protection for vaccine development, licensure and use: short summary. npj Vaccines 9, 82 (2024).
Salomon, J. A. et al. Disability weights for the Global Burden of Disease 2013 study. Lancet Glob. Health 3, e712–e723 (2015).
Krishnamoorthy, K., Harichandrakumar, K. T., Krishna Kumari, A. & Das, L. K. Burden of chikungunya in India: estimates of disability adjusted life years (DALY) lost in 2006 epidemic. J. Vector Borne Dis. 46, 26–35 (2009).
Nash, R. K. et al. Ebola virus disease mathematical models and epidemiological parameters: a systematic review. Lancet Infect. Dis. 24, e762–e773 (2024).
Timothy, J. W. S. et al. Early transmission and case fatality of Ebola virus at the index site of the 2013-16 West African Ebola outbreak: a cross-sectional seroprevalence survey. Lancet Infect. Dis. 19, 429–438 (2019).
Ward, T. et al. The real-time infection hospitalisation and fatality risk across the COVID-19 pandemic in England. Nat. Commun. 15, 4633 (2024).
Coronavirus (COVID-19) Infection Survey: England (Office for National Statistics (ONS), 2023); https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/coronaviruscovid19infectionsurveydata
What to Know About Measles and Vaccines (Johns Hopkins Bloomberg School of Public Health, 2025); https://publichealth.jhu.edu/2025/what-to-know-about-measles-and-vaccines
Acknowledgements
We acknowledge funding from the Coalition of Epidemic Preparedness Innovation (CEPI; H.S., B.C.D.). T.E., J.L.d.F., J.G.B., A.P., R.E.C. and N.L. are paid employees of CEPI. CEPI has supported the technology transfer of IXCHIQ to Institut Butantan in Brazil. S.C. acknowledges support from the European Commission under the EU4Health programme 2021–2027, grant agreement project: 101102733–DURABLE, the Laboratoire d’Excellence Integrative Biology of Emerging Infectious Diseases program (grant no. ANR-10-LABX-62-IBEID), ANRS-MIE, DGOS, ARS Réunion and the INCEPTION project (PIA/ANR16-CONV-0005).
Author information
Authors and Affiliations
Contributions
B.C.D., T.E. and H.S. conceptualized the analysis. B.C.D. conducted the formal analysis and visualization. B.C.D. and H.S. developed methods and wrote the initial draft. T.E., J.L., J.L.d.F., O.C.-A., J.G.B., S.C., A.P., A.K., R.E.C., S.J.T. and N.L. reviewed and edited the paper. H.S. supervised the project.
Corresponding authors
Ethics declarations
Competing interests
H.S. and O.C.-A. are consultants for Valneva regarding phase IV trial design. H.S. has been a consultant for Gavi Alliance. H.S. and B.C.D. are consultants for CEPI. T.E., J.L.d.F., J.G.B., A.P., R.E.C. and N.L. are paid employees of CEPI. CEPI has supported the technology transfer of IXCHIQ to Institut Butantan in Brazil. The other authors declare no competing interests.
Peer review
Peer review information
Nature Health thanks the anonymous reviewers for their contribution to the peer review of this work. Primary Handling Editor: Lorenzo Righetto, in collaboration with the Nature Health team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Factors affecting the risks and benefits of vaccination.
(a) Age-specific probabilities of adverse age-dependent infection outcomes (blue), age-dependent adverse vaccine outcomes (orange), and age-independent adverse vaccine outcomes (purple). (b) Net adverse outcomes averted per 10,000 individuals by age under the two vaccine risk scenarios. (c) Adverse outcomes averted as a function of vaccine efficacy for individuals at different ages (1, 20, 60, 80 years), assuming a 30% attack rate. (d) Adverse outcomes averted as a function of the infection attack rate for individuals at the same four ages assuming 95% vaccine efficacy. The dashed horizontal line indicates the threshold of zero net benefit. Negative values (shaded region) indicate net harm.
Extended Data Fig. 2 Evidence that benefits from vaccination outweigh risks.
Probability that vaccine benefits outweigh the risks of vaccine SAEs assuming different probabilities of severe outcomes following infection, probabilities of SAEs and either 1,000 or 10,000 individuals vaccinated (cohort size). Estimates are shown for different epidemiological scenarios (columns), assuming 50% or 95% vaccine efficacy (rows). n = 100,000 posterior samples. SAE: serious adverse event.
Extended Data Fig. 3 Risk of disease and death associated with chikungunya infection or IXCHIQ vaccination, stratified by age group.
(a) Chikungunya vaccine doses administered as of August 2025 by location. (b) Number of reported vaccine-associated SAEs and deaths. (c) Mean (bars) and 95% exact binomial confidence intervals (error bars) for the probability of medically attended chikungunya/SAEs and death associated with chikungunya infection (blue) or vaccination (yellow). SAE: serious adverse event.
Extended Data Fig. 4 Impact of changes in the attack rate on cases averted by IXCHIQ vaccination.
Number of medically attended chikungunya cases or deaths averted per 10,000 vaccinated in each age group (colors). The dashed horizontal line indicates the threshold of zero net benefit. Negative values (shaded region) indicate net harm. Arrows indicate epidemiological scenarios used in the main analysis, from left to right: traveller, small outbreak, endemic transmission, large outbreak. Solid line represents mean estimates and shaded region represent 95% uncertainty intervals derived from n = 100,000 binomial samples. SAE: serious adverse event.
Extended Data Fig. 5 Power to detect at least one death from vaccination.
(a) Sample size needed to achieve 80% power to detect at least one death as a function of attack rate and probability of death from infection, assuming 95% vaccine efficacy. From left to right, the black arrows indicate the probability of death for CHIKV in the 18-64 age group (0.00005), SARS-CoV-2 (0.01), and EV (0.6). Sample sizes >20,000 are shown as 20,000. (b) Minimum population size required (vertical dashed line) for detecting that vaccine mortality risks do not exceed benefits with 80% power given a 5% attack rate (horizontal line), shown for the infection fatality rates (brackets) of CHIKV, SARS-CoV-2, and EV. CHIKV: Chikungunya virus. SARS-CoV-2: Severe acute respiratory syndrome coronavirus 2. EV: Ebola virus. SAE: serious adverse event.
Extended Data Fig. 6 Impact of vaccine efficacy on IXCHIQ risks and benefits.
(a) Probability that the IXCHIQ vaccine benefits outweigh the risks of vaccine SAEs and vaccine deaths by age group and epidemiological scenario, assuming a vaccine efficacy of 50%. Open diamonds show the evidence available at the end of the trial and solid circles show all evidence currently available. Vertical dashed line denotes 95% probability (n = 100,000 posterior samples). (b) Impact of changes in vaccine efficacy on cases averted by IXCHIQ vaccination. Number of medically attended chikungunya cases / SAEs or deaths averted per 10,000 vaccinated in each age group (colors) by epidemiological scenario (columns). The dashed horizontal line indicates the threshold of zero net benefit. Negative values (shaded region) indicate net harm. Solid line represents mean estimates and shaded region represent 95% uncertainty intervals derived from n = 100,000 binomial samples. Dashed vertical line indicates baseline efficacy of 95%. SAE: serious adverse event.
Extended Data Fig. 7 Probability that the IXCHIQ vaccine benefits outweigh the risks of vaccine SAEs by age group and epidemiological scenario, assuming that 50% of medically attended CHIKV infections are equivalent in health burden to SAEs.
Open diamonds show the evidence available at the end of the trial and solid circles show all evidence currently available. Vertical dashed line denotes 95% probability (n = 100,000 posterior samples). SAE: serious adverse event.
Extended Data Fig. 8 Probability that the IXCHIQ vaccine benefits outweigh the risks of vaccine deaths by epidemiological scenario, using all the evidence currently available and assuming zero, one or three vaccine-linked deaths in the 65+ age group.
Vertical dashed line denotes 95% probability (n = 100,000 posterior samples).
Extended Data Fig. 9 DALYs averted per 10,000 individuals vaccinated with IXCHIQ by age group and epidemiological scenario, assuming three vaccine-linked deaths in the 65+ age group.
Positive and negative cases averted (per 10,000 in each age group) are coloured in blue and red, respectively. Bars represent mean estimates and error bars represent 95% uncertainty intervals derived from 100,000 binomial samples. DALY: Disability-Adjusted Life Year. SAE: serious adverse event.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cracknell Daniels, B., Endy, T., Lewnard, J. et al. A framework for risk–benefit analysis of vaccines approved through accelerated pathways. Nat. Health 1, 120–128 (2026). https://doi.org/10.1038/s44360-025-00027-4
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s44360-025-00027-4
